
Abstract
Objective
A meta-analysis was conducted to analyze the incidence of typical and atypical headaches and outcomes following various treatments in patients with Chiari I malformation.
Background
Headache is the most common symptom of Chiari malformation, which can be divided into typical and atypical subgroups to facilitate management. Much controversy surrounds the etiology, prevalence and optimal therapeutic approach for both types of headaches.
Method
We identified relevant studies published before 30 July 2022, with an electronic search of numerous literature databases. The results of this study were reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.
Result
A total of 1913 Chiari malformation type I CIM patients were identified, 78% of whom presented with headache, within this group cephalgia was typical in 48% and atypical in 29% of patients, and migraine was the most common type of atypical headache. The ratio of typical/atypical headaches with international classification of headache disorders diagnosis was 1.53, and without international classification of headache disorders diagnosis was 1.56, respectively. The pooled improvement rates of typical headaches following conservative treatment, extradural decompression and intradural decompression were 69%, 88%, and 92%, respectively. The corresponding improvement rates for atypical headaches were 70%, 57.47%, and 69%, respectively. The complication rate in extradural decompression group was significantly lower than in intradural decompression group (RR, 0.31; 95% CI: 0.06–1.59, I2 = 50%, P = 0.14). Low reoperation rates were observed for refractory headaches in extradural decompression and intradural decompression groups (1%).
Conclusion
The International Classification of Headache Disorders can assist in screening atypical headaches. extradural decompression is preferred for typical headaches, while conservative therapy is optimal for atypical headaches. A definite correlation exists between atypical headaches and Chiari Malformation Type I patients with higher prevalence than in the general population. Importantly, decompression is effective in relieving headaches in this particular patient population.
Keywords
Introduction
Chiari malformations (CM) were first described by the Austrian pathologist Hans Chiari in 1891 and further classified into four types (1), with type I (CIM) being the most common. Although a constellation of symptoms has been documented in CIM patients, headaches are often the most severe and common (2).
The sub-occipital Valsalva headache has been considered a hallmark symptom of CIMs and is defined as the typical headache (2,3). However, before the International Classification of Headache Disorders (ICHD)-III diagnosis was proposed (4), significant heterogeneity surrounded the prevalence and diagnostic criteria of the typical headache of CIM in the literature.
Recently, many scholars have identified many atypical headaches in CIMs, such as migraine, tension-type headaches, cluster headaches, trigeminal neuralgia, etc. (2,5,6). However, in general, scholars still consider CIM headaches as an integral symptom rather than dividing them into typical and atypical headaches for diagnosis, treatment and measurement (7,8). This tends to lead to the wrong treatment plan for CIMs headache and biases the efficiency assessment.
No consensus has been reached on the pathophysiology, prognostic factors and treatment protocol of CIM headaches. It is widely thought that the typical headache constitutes a common indication of posterior fossa decompression (PFD); however, highly heterogeneous outcomes have been reported in the literature. It remains unclear whether conservative treatment, including multidisciplinary (9), physiotherapy (10) or pharmacological therapy (11,12–14), is the initial treatment of choice for typical headaches. Besides, the efficacy of different PFD procedures, including extradural decompression (EDD) and intradural decompression (IDD), is controversial for typical and atypical headaches.
The incidence of atypical headaches in CIMs has long been thought to be comparable to the general population and is usually incidental. Accordingly, they should be treated with conservative treatment alone (15,16). However, contrasting studies revealed an increased prevalence of atypical headaches in CIMs compared with the general population and significant improvement is experienced after PFD, suggesting that atypical headaches can be considered part of the pathological spectrum of symptoms of CIMs (9,17).
However, these long-standing controversies have not yet been evaluated in either a meta-analysis or a review. Therefore, we conducted a systematic review and meta-analysis to compare the differences in rates of improvement, complication and reoperation between typical and atypical headaches using different managements, screening for the optimal methods for typical and atypical headaches. Moreover, we assessed the correlation between atypical headaches and CIM pathophysiology by reviewing the proportion of atypical headaches and the post-surgical remission rates in CIMs.
Patients and methods
Ethic approval and patient consent
As the study only analyzed pooled data from previously published articles and all patient data were anonymized, ethics approval and informed patient consent were waived by the ethics committee at our institution.
Search strategy
The senior author (YH) conducted the initial literature search by reading titles and abstracts. All search strategies were developed according to PRISMA guidelines with guidance from the Cochrane Handbook for Systematic Reviews of Interventions, National Academies Standards for Systematic Reviews, and Peer Review of Electronic Search Strategies. Studies on the prevalence of typical and atypical headaches and the rates of improvement, complication, and reoperation of various management strategies for CIMs headaches were retrieved from the literature. The author (YH) created search strategies using the following keywords (including different spellings of “Chiari malformation type I” and “typical headache” OR “atypical headache” OR “type headache” OR “chiari headache” OR “non-chiari headache” OR “characteristic headache” OR “Valsalva headache” OR “non-Valsalva headache” OR “cough headache” OR “non-cough headache” OR “tussive headache” OR “non-tussive headache” OR “specific headache” OR “unspecific headache” OR “non-specific headache” OR “migraine” OR “tension-type headache”) in PubMed, Embase, the Cochrane Library and Google Scholar, then manually searched relevant conference abstracts and examined the reference lists in identified studies and other reviews.
Study selection
The authors HY and MZ assessed each article for eligibility. The inclusion and exclusion criteria are listed in Table 1. Figure 1 displays the detailed article selection process. The authors screened titles and abstracts to exclude articles that did not satisfy inclusion/exclusion criteria. Full texts were subsequently evaluated. No patients were excluded based on patient age or presence or absence of syringomyelia.
Inclusion and exclusion criteria.

There were no exclusion criteria based on age, sex, race and BMI.

Flow diagram detailing the study selection process.
Data extraction
Two authors HY and CH independently extracted data from each study into a Microsoft Excel data form, and the extracted data are listed in Table 2.
Characteristics of the 24 studies (all had 30 data sets) that met inclusion criteria.

Six papers were split into “Author 1” and “Author 2” based on the “Management” and “Pediatric/Adult”. AHA, atypical headache; Both T/AHA, Cases presenting both atypical and typical headaches; CH/O, cluster headache and others; EDD, extradural decompression; Fe, female; ICHD, International Classification of Headache Disorders; IDD, intradural decompression; Ma, male; mi, migraine; NA, not available; THA, typical headache; T-T = tension-type headache.
Assessment of quality and risk of bias within studies
Two authors independently assessed the quality of evidence for each article according to the Methodological Index for Non-randomized Studies (MINORS). Reviewers were not blinded to the article’s authors, institutions, or manuscript journals. Disagreements between authors were resolved through discussions.
Statistical analysis
All statistical analyses were performed using statistical software R version 4.1.1. Pooled results were expressed as Odds Ratio (OR) and proportions. The heterogeneity among studies was estimated using Cochran’s Q test and I2 index. A random effects model was employed to estimate the pooled effects when significant heterogeneity was found (P-value from Cochran’s Q test ≤ 0.05 and I2 index < 50%); otherwise, a fixed-effects model was used (18). Publication bias was estimated using Egger’s test (19); a P-value < 0.1 was statistically significant. Significant differences between subgroups were determined by pooled effect sizes with 95% Cis.
Results
Study selection and characteristics
A total of 2207 articles were initially retrieved from the electronic databases and manual search, and the retrieval strategy is depicted in Figure 1. After excluding 1594 duplicates and 599 articles that did not meet the inclusion criteria, 24 studies were included in the present analysis (Table 2).
Included studies and patients
Six out of 24 included studies stratified patients according to their age (pediatric, adult) (13) and management methods (conservation, EDD, and IDD) (14,20–23), then quantified the incidence of typical and atypical headaches. This part of literature was expressed as “Author 1/Author 2” (Table 2). Finally, 24 studies (30 datasets) were analyzed.
All studies were published in English in peer‐reviewed journals between 1992 to 2022, except for two meeting abstracts with unavailable details. Three papers were case series, and 21 were cohort studies. All included studies were observational, including retrospective (n = 21) and prospective (n = 3) studies.
Basic data of included studies
Twelve studies included only pediatric patients, 17 studies included only adults, and one study evaluated both. The average cohort age was 25.08 years (0.42–79), with 14.29 years (range: 0.42–18) and 35.99 years (range: 18–79) for pediatric and adult patients. The gender ratio (male/female) was 1.73 (1200/693) with 1.4 (541/384) and 2.20 (621/282) for pediatric and adult patients. The median follow-up period was 34 months (0.31–258 months).
Typically, 1430 out of 1913 patients with CIMs included in the present investigation complained of headaches, and each study’s sample size ranged from 7 to 141. Typical, atypical and both types of headaches were observed in 912, 453, and 65 cases, respectively. Five datasets (n = 184 cases) were treated with conservative treatment, and 26 datasets (n = 1249 cases) were treated with surgery. In the surgical group, 6 (n = 186), 13 (n = 759) and 6 (n = 304) datasets adopted EDD, IDD, and PFD (mix EED and IDD) (Table 2). The proportion of patients for each subgroup of headaches is illustrated in Figure 2.

The prevalence of headache symptoms. (a–c) The prevalence of headache in all cases, pediatric and adult cases, respectively. (d–f) The prevalence of typical and atypical headaches in all cases, pediatric and adult cases, respectively and (g–i) The prevalence of various types of atypical headaches in all cases, pediatric and adult cases, respectively.
The proportion of each type of headache
The overall pooled incidence of headache
The overall pooled prevalence of headache in all 24 studies (30 datasets) was 78% (95% CI: 0.70–0.85, I2 = 93%, P < 0.01), including 72% (95% CI: 0.57–0.85, I2 = 94%, P < 0.01) and 82% (95% CI: 0.72–0.90, I2 = 92%, P < 0.01) in pediatric and adult patients (Figures 3a-c).

Forest plot of each type of headache. (a-c) The overall pooled incidence of headache in all cases, pediatric and adult cases, respectively. (d-f) The pooled incidence of typical headache in all cases, pediatric and adult cases, respectively. (g-i) The pooled incidence of atypical headache in all cases, pediatric and adult cases, respectively. (j-l) The pooled incidence of migraine in all cases, pediatric and adult cases, respectively and (m-o) The pooled incidence of tension-type headache in all cases, pediatric and adult cases, respectively.

Continued.
The pooled incidence of typical headache
In total, 21 studies (26 datasets) classified headaches into typical and atypical, and three studies (four datasets) included only typical headache cases. Pooled analysis of the 21 studies yielded a headache incidence of 48% (95% CI: 0.39–0.57, I2 = 92%, P < 0.01), with 37% (95% CI: 0.25–0.51, I2 = 91%, P < 0.01) and 55% (95% CI: 0.45–0.66, I2 = 90%, P < 0.01) for pediatric and adult patients (Figures 3d-f).
The pooled incidence of atypical headache
The pooled atypical headache rate was 29% (95% CI: 0.23–0.35, I2 = 83%, P < 0.01) in 21 studies (26 datasets), with 27% (95% CI: 0.19–0.36, I2 = 79%, P < 0.01) and 30% (95% CI: 0.22–0.38, I2 = 86%, P < 0.01) in pediatric and adult patients. In eight studies (ten datasets), the atypical headaches were further divided into migraine, tension-type headaches, and others (Figures 3g-i).
The pooled incidence of migraine
The pooled analysis of eight studies showed an overall incidence of migraine of 31% (95% CI: 0.13–0.52, I2 = 94%, P < 0.01) (the corresponding incidence of atypical headache was 38%), with 20% (95% CI: 0.01–0.51, I2 = 89%, P < 0.01) and 38% (95% CI: 0.17–0.62, I2 = 94%, P < 0.01) in pediatric and adult patients (Figures 3j-l)
The pooled incidence of tension-type headache
The pooled incidence of tension-type headache was 8% (95% CI: 0.01–0.18, I2 = 79%, P < 0.01) in eight studies, with 2% (2/102) in pediatric (reported by only one study) and 12% (95% CI: 0.07–0.19, I2 = 0%, P < 0.98) in adult patients (Figure 3m-o).
ICHD for headache identification
Only six out of 21 studies adopted ICHD diagnosis recommended by the International Headache Society (IHS) to classify headaches. The ratio of typical/atypical headaches with and without ICHD was 1.53 (545/357) and 1.56 (571/365), respectively. Consequently, the ratio of atypical headaches increased significantly with ICHD.
Efficiency of headache treatment with three methods
Typical headache
A total of 24 publications (30 datasets) with 944 patients reported typical CIM headaches and treatment efficiency (Table 2). Patients were divided into conservative treatment, EDD and IDD groups (EDD and IDD belong to the surgery group). Concurrently, the four studies were excluded since the efficiency of surgical methods (mixed EDD and IDD) was not described separately. Only two of the papers directly compared the improvement rates of the conservative group with the surgical group: 35.71% vs. 85.74% (conservative vs. EDD) and 40% vs. 94.62% (conservative vs. IDD), all of which were significantly lower in the conservative group than in the surgical groups.
For the remaining 18 papers pooled separately for the improvement rate, the pooled improvement rate after conservative treatment was 69% (95% CI: 0.18–1.00, I2 = 91%, P < 0.01). EDD yielded a pooled improvement rate of 88% (95% CI: 0.70–0.99, I2 = 67%, P = 0.03), while IDD was associated with an improvement of 92% (95% CI: 0.85–0.97, I2 = 81%, P < 0.01) (Figures 4a-c).

Forest plots of headache improvement rates between conservation, EDD and IDD groups. (a-c) The improvement rates of typical headaches and (d-f) The improvement rates of atypical headache.
The conservative groups exhibited significantly lower efficacy against typical headaches than the surgical groups with non-overlapping 95% CIs, consistent with studies by Chavez et al. (14) (40.00% vs. 94.62%) and Pascual et al. (20) (35.71% vs. 85.74%).
Atypical headache
In total, 18 studies (19 datasets with 500 CIMs) reported data on atypical headaches and treatment efficiency (Table 2). They were divided into three treatment groups (conservative treatment, EDD, and IDD). The remaining four studies included patients that underwent surgery mixed EDD and IDD and were excluded.
Only one study compared the effect of conservative therapy vs. IDD for atypical headaches (61.54% vs. 92.86%) (14). Two studies (3 data sets) documented the efficacy of conservation treatment for atypical headache with a pooled improvement rate of 70% (95% CI: 0.19–1.00, I2 = 94%, P < 0.01) (Figure 4D). Fourteen studies reported a pooled improvement rate of 61% (95% CI: 0.47–0.74, I2 = 81%, P < 0.01) after surgery for atypical headache (Figure 4e).
Furthermore, we compared the difference in the improvement rate of atypical headaches between EDD and IDD. Only one study compared the efficacy of EDD with IDD, and both showed full remission (2/2 vs. 2/2) (23). A study reported efficacy of 57.47% (50/87) for EDD against atypical headaches (24). Eight studies described the efficacy of IDD in atypical headache with a pooled improvement rate of 69% (95% CI: 0.49–0.86, I2 = 84%, P < 0.01) (Figure 4f).
There were no significant differences in the improvement rate for atypical headaches between conservative and surgery groups, as indicated by overlapping CIs.
Complications
In the surgical groups, twelve studies reported the complication rate of EDD or IDD, and four directly compared the complication rate between EDD and IDD (RR: 0.31; 95% CI: 0.06–1.59, I2 = 50%, P = 0.14). Two papers documented the complication rate of EDD alone with a pooled rate of 1% (95% CI: 0.00–0.04, I2 = 0%, P = 0.42); the remaining six papers documented the complication rate of IDD alone with a pooled rate of 8% (95% CI: 0.04–0.13, I2 = 73%, P < 0.01) (Figures 5a-c).

Forest plots of complications and reoperations between EDD and IDD groups. (a-c) Complications and (d-f) Re-operations.
EDD was associated with a significantly lower complication rate than IDD, as shown by non-overlapping CIs and consistent with the pooled results of double-arm studies.
Reoperation of headache
Eleven studies analyzed the reoperation rate due to refractory headaches after the initial operation. Three studies found the reoperation rate was comparable between EDD and IDD (RR, 0.71; 95% CI: 0.02–22.57, I2 = 60%, P = 0.11) (Figure 5d). Two studies documented the reoperation rate following EDD with a pooled rate of 1% (95% CI: 0.00–0.04, I2 = 0, P = 0.42) (Figure 5e), while the six remaining studies assessed the reoperation rate of IDD alone with a pooled rate of 1% (95% CI: 0.00–0.04, I2 = 63%, P = 0.02) (Figure 5f).
There were no significant differences in reoperation rate due to the refractory headaches between EDD and IDD groups, as indicated by the overlapping CIs.
Publication bias and evidence quality
Per MINORS assessment of all studies, the quality of evidence and strength of the data are shown in Table 3. Funnel plots created for all outcomes of interest show no significant asymmetry (Figure 6). There was thus no evidence of publication bias.
The Quality Assessment of the Studies According to the Methodological Index for Non-Randomized Studies (MINORS).

The items are scored 0 (not reported), 1 (reported but inadequate) or 2 (reported and adequate). The global ideal score being 16 for non-comparative studies and 24 for comparative studies.

Funnel plots for all outcomes. The abscissa is OR value and the ordinate is standard error. It can be observed that most significant results have no significant asymmetry, and the few asymmetries are due to the small amount of available data.
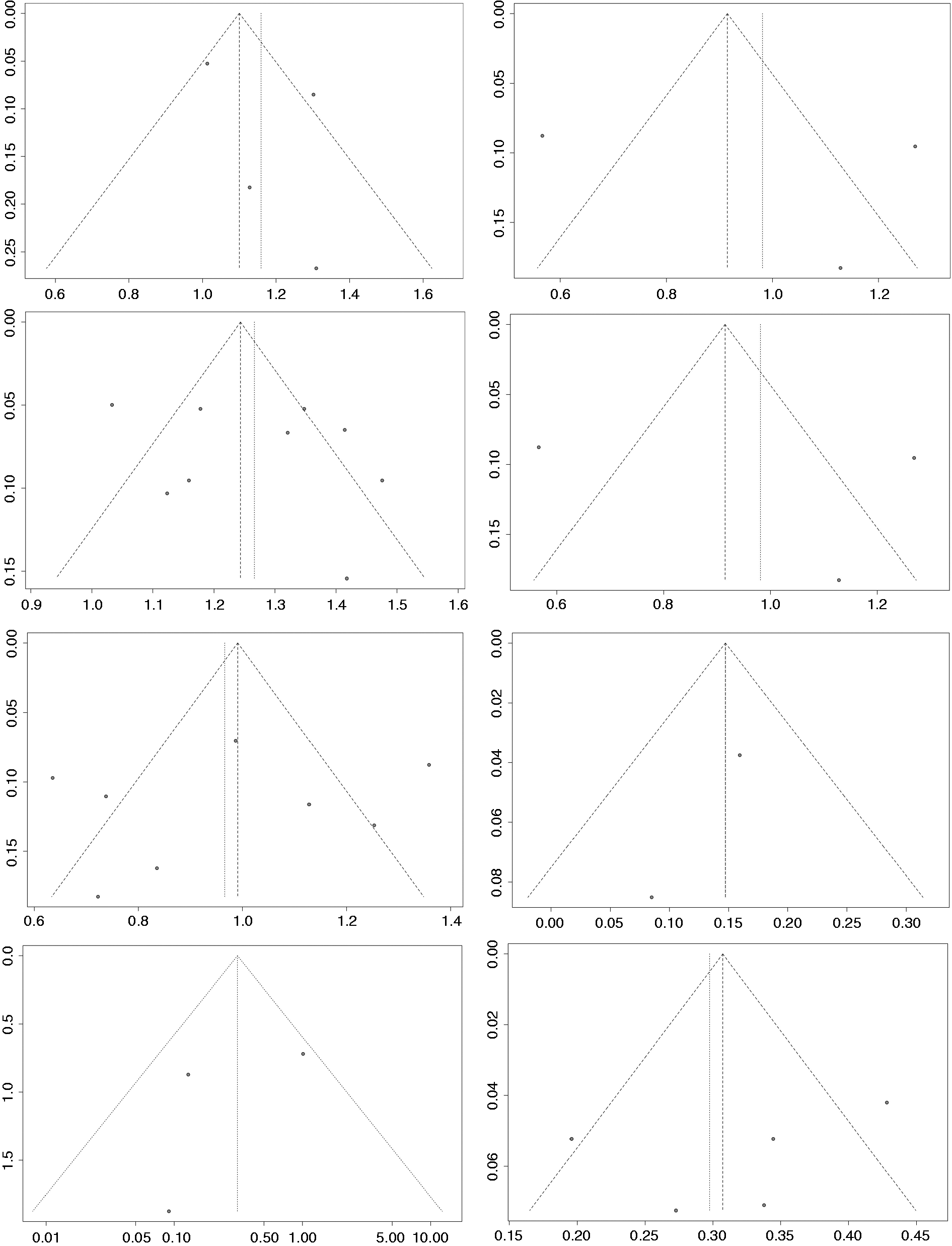
Continued.
Discussion
The prevalence of headache
It is well-established that although CIM patients report various symptoms, headache remains the chief complaint. Plenty of evidence suggests that the prevalence of headaches ranges from 50% to 93.1% (25,26). In the seminal studies by Milhorat and colleagues (27), the headache rate was as high as 81%, whereas, in the recent study by Dawes et al. (25), the rate was only 50%. Consequently, there are considerable differences in the prevalence of headaches reported in previous literature.
In our meta-analysis, CIM patients with headaches accounted for roughly 75% of all included patients and were divided into atypical (approximately 25%) and typical (approximately 50%) headaches (Figure 1), consistent to a certain extent with the reported prevalence of CIM headaches (50%–80%) in the literature. The discrepancy may be attributed to the different proportions of patients with mixed typical and atypical headaches. In the study by Milhorat et al., typical and atypical headaches were not distinguished (27), while headaches reported by Dawes et al. were all Valsalva headaches (25), which caused a huge difference in the percentage of headaches.
The typical headache of CIM
The definition of a typical headache of CIM
Before CIM typical headache was formally defined, the typical headache attributed to CIM was regarded as occipital cough headache (3,9,20,28–31). However, identifying it in clinical practice can be challenging given its significant heterogeneity. For example, Gundag et al. (32) defined it as coughing or exertional headache in the occipital and palatal regions, while it was described by Mueller et al. (33) as pressure or explosive headache that originates in the posterior occipital region, radiating to one or both eyes and moving to the vertex or both temporal regions. Interestingly, Bezuidenhout et al. (2) concluded that short bouts of Valsalva headaches are the most typical manifestation of CIMs, but it does not mean that these symptoms and CIM-associated headaches are the same. In contrast, Pascual et al. (20,34) found that all cases of cough headache were associated with CIM, which has led to some scholars equating Valsalva headache to CIM typical headache (14,35–37). Interestingly, another group of scholars characterized a typical headache of CIM as a posterior occipital headache (38).
Identification of CIM headache with ICHD-III
The third edition of the International Classification of Headache Disorders (ICHD-III beta) proposed diagnostic criteria for CIM typical headaches in 2013 (39). Recently, based on this classification, some studies identified the headache attributed to CIMs as typical and atypical and provided different treatment options. However, only a few included studies (n = 6) used ICHD in the current meta-analysis (Table 1).
The prevalence of typical headache in CIM patients
The pooled prevalence of typical headaches in this meta-analysis was 48%, while a significantly lower proportion of typical headaches and a higher proportion of atypical headaches were found using ICHD (Table 3). Therefore, we recommend the classification of headaches according to ICHD criteria, which can facilitate the identification of typical/atypical headaches of CIMs, consistent with the literature (28,40).
The management of typical headache
Conservative treatment
Typical headache has been long considered the first indication for PFD in CIMs (13,14,37,41,48). Current evidence suggests that decompression is often effective for typical headaches but is not indicated for CIMs with mild symptoms or good response to conservative management (28). Meanwhile, some studies have attempted conservative treatment of the typical headache attributed to CIMs, but the reported efficacy was inconsistent.
It is widely thought that although different approaches can resolve most symptoms of CIMs, PFD is the most preferred in terms of efficacy for typical headaches (13,14,20). Importantly, in the pioneering study by Abdallah et al., (10) a novel conservative treatment algorithm including prescriptive medications, physical therapy, Pilates, and swimming was applied in 31 CIM patients with typical headaches, and relief was observed in 29 patients. Therefore, these authors proposed that this “novel conservative treatment” can be useful in selected CIMs, and surgery is not necessary.
It has been reported that the efficacy of conservative treatment is lower than surgical intervention for typical headaches, which is also consistent with the conclusion of our meta-analysis. Nonetheless, the conservative treatment proposed by Abdallah et al. might be a good alternative for patients who are contraindicated or unwilling to undergo surgery.
Surgery for typical headache
Decompression methods with or without dural opening have been debated for CIM patients. Interestingly, some scholars believe that IDD yields a more robust decompressive effect than EDD, resulting in better relief of typical headaches and lower reoperation rates (14,28,36,41,43). For instance, Hidalgo et al. (38) performed IDD on 28 CIMs with typical headaches, and 57% of cases experienced complete relief before discharge, and typical headaches disappeared completely in all cases within six months, substantiating its strong and effective decompressive effect.
In contrast, EDD provided a similar therapeutic effect to IDD against typical headaches (20–22,24,43) but lower rates of complications (6,21,44).
In this meta-analysis, EDD and IDD yielded excellent outcomes for typical headaches. No significant difference was observed between the two methods in pooled rates of improvement and reoperation, consistent with recent double-arm observational studies conducted by Seaman et al. (22) and Mozaffari et al. (21).
Meanwhile, in our meta-analysis, EDD was associated with significantly lower complication rates than IDD (1% vs. 8%), consistent with the literature (45,46).
Accordingly, EDD should be considered the optimal treatment option for typical headaches of CIMs. Additionally, Massimi et al. (44) recommended EDD with the removal of the outer layer of the dura to achieve a better decompressive effect. For patients with residual or recurrent headaches after EDD, the “novel conservation” proposed by Abdallah et al. may be a good choice. Only a small number of patients required secondary IDD due to refractory headaches.
Atypical headaches of CIM
The definition of atypical headache of CIM
Although different forms of atypical headaches have been screened from CIM patients recently (including migraine, tension-type headache, cluster headache and trigeminal neuralgia), there is a lack of an official definition of atypical headache.
Some scholars identified atypical headaches based on the site of onset, such as Abdallah et al. (10) who defined the headache as poorly localized frontal temporal or nonspecific headaches. Krucoff et al. (29) directly employed the diagnostic criteria of primary headaches to identify atypical headaches of CIMs. Meanwhile, some use the exclusion method that divided all headaches that did not fulfill the criteria for typical headaches were defined as by Beretta et al. (9) and Galan et al. (31).
We believe that using the exclusion method is the simplest and most effective approach, but the possibility of secondary headache due to other etiologies should also be ruled out when the typical headache is excluded, as suggested by Galan et al. (31).
Nevertheless, much controversy surrounds these atypical headaches observed in CIM patients. Next, we elaborate on these divergences according to our meta-analysis results.
Atypical headache was not correlated with CIM
We found that approximately 8% of pediatric/adolescent (47) and 14.2% of adult (48) cases reported migraines, suggesting that the risk in CIM patients and patients with primary headache is comparable and atypical headache is often an incidental finding. Therefore, some scholars conclude that the presence of atypical headaches may be coincidental and mechanistically distinct from the specific symptoms of CIM (15,16). Consequently, conservative treatment is recommended (2,6,37).
Although relief of atypical headaches is achieved in many cases of CIMs after PFD, Thunstedt et al. (15) noted the effect was smaller than a typical headache, which cannot be ruled out as a result of the natural course of primary headache as well as the placebo effect of surgery. Notably, Thunstedt pointed out that the relationship between atypical headache and CIM remains unclear and requires further study. Moreover, Davidson et al. (49) reported 66.67% relief of atypical headache cases after PFD in a CIM cohort. It was thought that most atypical headaches were not associated with CIM because typical headaches exhibited a significantly better response to PFD than atypical headaches in their cohort.
Atypical headache is correlated with CIM
In contrast, some researchers believe that atypical headache, especially migraine is strongly involved in CIM physiopathology, and the conventional surgical approach remains helpful.
It has been established that the prevalence of atypical headache (primary headache) among CIM patients was higher than in the general population (5,50,51). Besides, the coexistence rate of typical and atypical headaches was 74% in CIM cases reported by Beretta et al. (9). Moreover, the surgical remission rate of atypical headaches reached an astonishing 85% in Beretta et al.'s cohort. Therefore, Beretta et al. advocated that atypical headaches are closely related to CIM and promote the progression of symptoms. Additionally, in a study by Kaplan et al. (17), although the frequency of total migraine in CIM patients and healthy controls was comparable, the incidence of chronic migraine was threefold higher in CIMs. Therefore, it was concluded that CIM is associated with chronic atypical headaches.
The present meta-analysis showed that the pooled prevalence of atypical headaches was 29% based on 21 studies and 38% in the subgroup of adults. Nine studies further stratified atypical headache; migraine was the most predominant subgroup with a pooled rate of 31% (the corresponding total atypical headache was as high as 36%). Compared with healthy controls (48,49), a significantly higher rate of atypical headache has been reported in CIM, inconsistent with the previous literature. Furthermore, the high pooled remission rate (61%) in atypical headaches makes it unlikely that our results could be explained by the “natural course” and “placebo effect”. Consistent with the literature, we found that atypical headache in CIMs was not a coincidental finding. However, the specific mechanism between atypical headaches and CIM must be further elucidated.
The management of atypical headaches
Lavorato et al. (43) recommend IDD for atypical headaches, while other studies recommend conservative management (12,13). In the present meta-analysis, the pooled relief rate with conservative management and surgery was 70% (95% CI: 0.19–1.00, I2 = 94%, P < 0.01) and 61% (95% CI: 0.47–0.74, I2 = 81%, P < 0.01), respectively. Our findings suggest that conservative and surgical treatment exhibit comparable efficacy for atypical headaches. Therefore, for CIMs with atypical headaches, conservative treatment may be indicated, especially the “novel conservative” therapy reported by Abdallah et al., which leads to a satisfactory control rate. However, CIM cases with atypical headaches combined with other CIM symptoms or imaging manifestations can also be treated surgically, with a remission rate of about 61%.
Limitations
Our present meta-analysis included only English language publications, which may lead to the potential omission of relevant studies.
Although our meta-analysis focused only on the primary symptoms of headaches in CIM patients, these symptoms are rarely isolated. Accordingly, emphasis should be placed on co-occurring symptoms when designing treatment strategies for CIMs.
Most publications included in this study (21/24) were retrospective observational studies, which exhibit very low-quality evidence (Table 3), limiting the generalizability of the findings of this analysis.
The sample size was low, and studies with a one-arm design lacked a control group.
The studies included in our meta-analysis were conducted over a wide temporal period and were influenced by changes in the surgical management of CIMs.
The clinical outcomes are difficult to interpret due to the heterogeneity of the same treatment modality.
Strengths
This is the first meta-analysis to settle the debate regarding typical/atypical headaches in CIMs.
The quantitative analysis performed in this meta-analysis increased the reliability of the results of our study.
Headache is one of the most common complaints and a characteristic symptom of CIMs.
Although the overall quality of the included papers was poor, the pooled results of single-arm trials tended to be consistent with the double-arm trials included, substantiating the credibility of the findings of our meta-analysis.
Conclusion
The present study undertook a comprehensive review and meta-analysis of the literature to assess the prevalence, classification and treatment effect of headache in CIMs. A total of 78% of CIMs presented headaches, of which 48% were typical, 29% were atypical, and migraine was the most common type of atypical headache. The binary classification of typical and atypical headaches based on ICHD was useful for CIMs to facilitate clinical management.
EDD, especially outer dura splitting, should be considered the optimal treatment option for typical headaches. For patients with residual or recurrent headaches after EDD, the “novel conservation” proposed by Abdallah et al. (10) might be a good choice. Only a very small number of patients require further decompression of IDD due to refractory headaches.
There is an inevitable correlation between atypical headaches and CIMs, given the higher prevalence than the general population and the non-negligible efficiency of PFD. For atypical headaches, conservative treatment is preferred, which may achieve a comparable effect to surgery. Refractory cases or headaches combined with other symptoms can also be treated surgically. The recommended management regimen based on our results is shown in Figure 7.
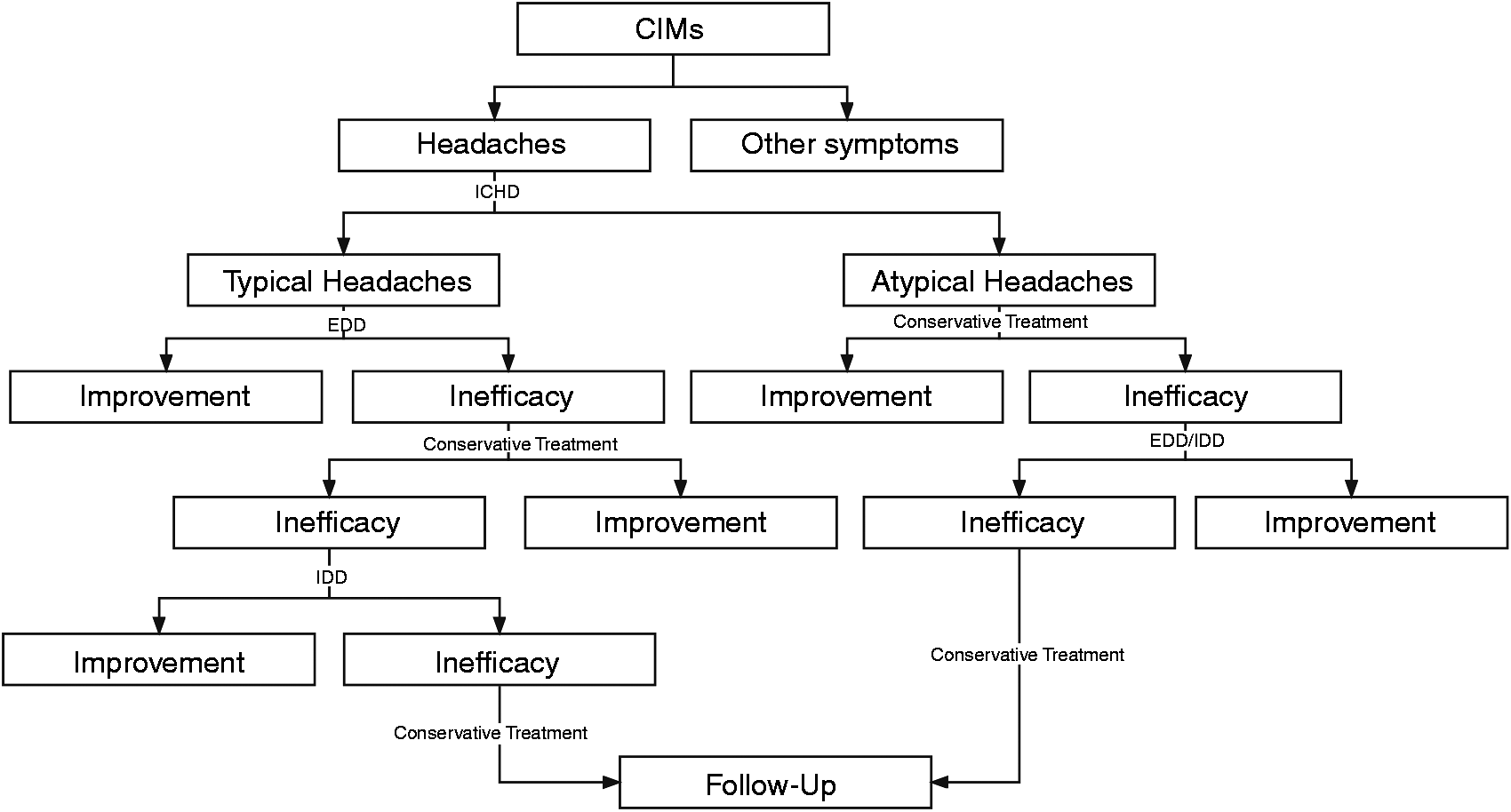
The recommended management regimen for CIMs headache is based on the present meta-analysis results.
Due to the low-quality evidence of our meta-analysis, further research, including larger, randomized, double-blinded, placebo-controlled, multicenter trials with long-term follow-up of high quality, is warranted to substantiate our conclusions.
Clinical implications
A total of 78% of CIMs presented headaches, of which 48% were typical, 29% were atypical, and migraine was the most common type of atypical headache. Chiari headache was a heterogeneous symptom, and the binary classification of typical and atypical headaches based on ICHD was useful for CIMs to facilitate clinical management. Extradural decompression should be considered the optimal treatment option for Chiari typical headaches. For atypical headaches, conservative treatment is preferred, which may achieve a comparable effect to surgery. There is an inevitable correlation between atypical headaches and CIMs, given the higher prevalence than the general population and the non-negligible efficiency of PFD.
Footnotes
Acknowledgments
We thank Qing Pan of Medical Statistics, for advice on statistical methods and comments on the manuscript. We also thank Home for Researchers editorial team for language editing service.
Author statement
All authors contributed substantially to the study design, data collection, methodology, software, original draft, critical revision, and final approval of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.