
Abstract
Background
Chiari I malformation typically presents with cough headache. However, migraine-like or tension-type-like headaches may also occur. There are limited publications on Chiari I malformation-associated headache semiologies and the effect of foramen magnum decompression on different headache types.
Methods
A retrospective analysis complemented by structured phone interviews was performed on 65 patients with Chiari I malformation, treated at our hospital between 2010 and 2021. Headache semiology (according to ICHD-3), frequency, intensity, and radiological characteristics were evaluated pre- and postoperatively.
Results
We included 65 patients. 38 patients were female and 27 male. Mean age was 43.9 ± 15.7 years. Headache was predominant in 41 patients (63.0%). Twenty-one patients had cough headache and 20 had atypical headache (12 migrainous, eight tension-type headache-like). Thirty-five patients with headache underwent surgery. Frequency, intensity, and analgesic use was significantly reduced in cough headache (p < 0.001). Atypical headaches improved less (p = 0.004 to 0.176). Exploratory analysis suggested that larger preoperative tonsillar descent correlated with larger postoperative headache intensity relief (p = 0.025).
Conclusion
Decompression was effective in Chiari I malformation-related cough headache. Atypical headache responded less well, and the causal relation with Chiari I malformation remains uncertain. For atypical headache, decompression should only be considered after failed appropriate preventive therapy and within an interdisciplinary approach involving a neurologist.
Introduction
The diagnosis of Chiari I malformation (CIM) is made not clinically but by magnetic resonance imaging (MRI) and is defined by a downward herniation of the cerebellar tonsils ≥5 mm through the foramen magnum. This type of cerebellar tonsillar descent occurs in approximately 0.1% of adults, predominantly affects women and is often associated with syringomyelia, and in some cases, scoliosis (1–4).
Symptoms tend to begin in adulthood with typical paroxysmal ‘cough headache’ – induced or exacerbated by laughing, coughing, or Valsalva manoeuvre and lasting seconds to a few minutes (5). However, migrainous headache with classical accompanying symptoms, such as sensory phobia or nausea, and tension-type-like (TTH) headache have also been described to be associated with CIM (3,6,7). In addition, not all patients with CIM present with headache, and symptoms like vertigo, dizziness and gait disturbances have also been described (8). Less frequently, patients have neurological signs or oculomotor disturbances such as downbeat nystagmus (1). Diagnostically, MRI of the craniocervical junction is the method of choice, showing a descent of one or both cerebellar tonsils from the McRae (basion-opisthion) line, with or without accompanying syringomyelia (1,9).
The following theories on the pathophysiology of the typical CIM-related headache have emerged: The Oldfield’s theory, which describes pulsatile pressure effect caudally with mechanical impact to the spinal cord (10) and the William’s theory, which implies increasing the abdominal pressure results in a higher craniocaudal pressure gradient that cannot be dissipated via the subarachnoid space. This would result in transient symptomatic intracranial pressure elevation with consecutive affection of trigeminal afferents of the meninges, resulting in headache. (11–13)
Foramen magnum decompression is the treatment of choice for patients with debilitating symptoms and/or pronounced syringomyelia. In case of mild symptoms or incipient syringomyelia, a surgical approach may be discussed, whereas asymptomatic patients do not require further therapy (14). The standard surgical approach is the foramen magnum decompression in combination with C1 laminectomy (15,16). In several trials, foramen magnum decompression had a favourable effect on symptom relief – especially on headache (6,17,18). However, previous studies have examined headache semiology alone without a precise description of the postoperative course (6,19) or the outcome of headache without detailed headache semiology (20). Therefore, a detailed description of headache semiology and characteristics pre- and postoperatively and the postoperative outcome of different headache types (including typical cough headache and other headache semiologies) in CIM is still lacking.
The aim of our project was to provide such a description of headache characteristics and attempt a correlation of radiological characteristics with headache outcome to further promote the understanding of the relation between CIM and headache.
Methods
We retrospectively included 65 adult patients of the Department of Neurology and the Department of Neurosurgery with conservative or surgical therapy for CIM from 2010 until 2021. Inclusion criteria were: Adult (≥18 years) patients with radiologically (MRI) proven CIM, defined by a tonsillar descent of >5 mm. Exclusion criteria were: Other secondary headache disorders (e.g. idiopathic intracranial hypertension) or intracranial abnormalities (e.g. subdural haematoma, tumour, abscess) or missing written informed consent.
Clinical and neurosurgical data as given in Tables 1–4 were extracted from the patients’ charts and complemented by a structured phone interview conducted with all patients in May 2021. Mostly, patient charts contained information about the initial (preoperative) presence of cough headache vs. other headache vs. no headache, and of headache intensity and frequency, while more detailed headache characteristics and accompanying symptoms had to be assessed retrospectively in many cases. Postoperative headache was assessed as the state at the time point of the phone interview. The phone interview was conducted personally by one of the authors using a structured questionnaire including pre- and postoperative headache characteristics, frequency, intensity (maximum and minimum intensity on a numerical rating scale from 0 = no headache to 10 = most intense headache imaginable) and frequency and type of acute headache medication intake. In addition, retrospective, subjective change of headache in the weeks after foramen magnum decompression was obtained (as improved, unchanged or worsened). Headache semiology was determined according to the International Classification of Headache Disorders 3rd edition (ICHD-3) (5). Typical headache attributed to CIM was defined (according to the ICHD-3 diagnostic criteria, chapter 7.7) as a (sub-)occipital headache evoked by coughing, laughing or other Valsalva-type manoeuvres, lasting for seconds to a maximum of 5 min.
Characteristics of the study population.
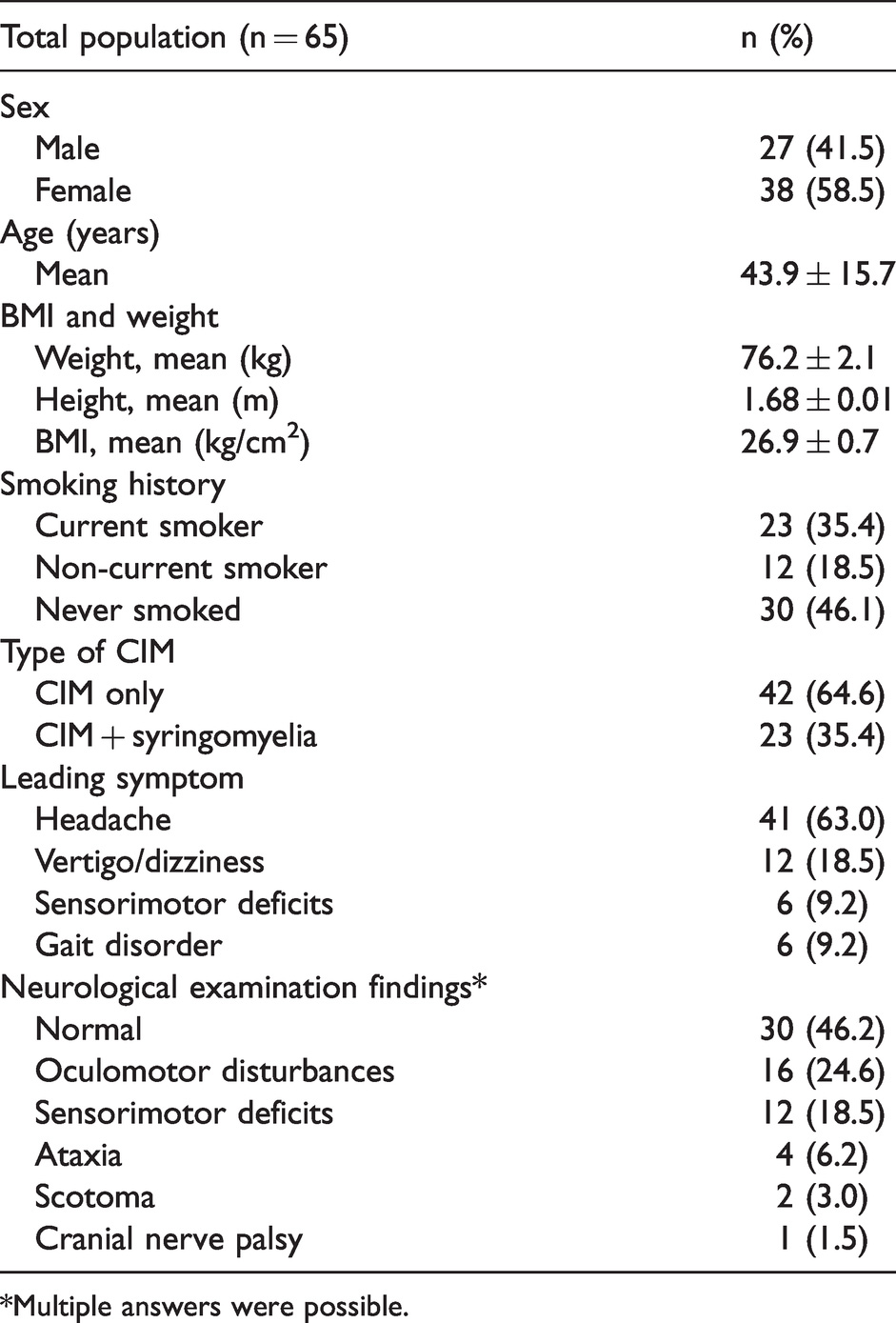
*Multiple answers were possible.
Baseline headache characteristics (n = 41).

*Multiple answers allowed as defined in ICHD-3 (5).
Radiological findings at baseline and after surgery.

Mean ± SD, range.
Headache outcome.

Mean ± SD [range], significant changes are marked in bold.
Imaging data
Diagnosis of CIM was based on MR imaging in all cases. However, part of the MR images was performed outside our hospital and had not been retained for documentation. The analysis of imaging data is based on 49 subjects at baseline and on 37 subjects after foramen magnum decompression. The following measures were obtained from cranial and spinal MR imaging by a radiologist (MPF): i) Distance between the anterior and posterior margins of the foramen magnum (basion to opisthion), called the McRae line (mm) preoperatively and midsagittal foramen magnum diameter postoperatively, ii) extent of tonsillar descent (measured from the McRae line) (mm), and iii) maximum median anterior-posterior (a.p.) diameter of the fourth ventricle (mm). These measurements are shown in Figure 1. In those patients where syringomyelia was detected, maximum a.p. diameter (mm) and longitudinal extent (number of segments) of the syrinx were assessed further.

Distance measurements. Yellow: McRae line (distance between the anterior and posterior margins of the foramen magnum); red: extent of tonsillar descent; green: maximum median diameter of the fourth ventricle.
Statistical analysis
SPSS (SPSS version 26, IBM, Armonk/NY, USA) was used for statistical analysis. A two-sided p-value of <0.05 was considered statistically significant.
Descriptive statistics were performed to analyse frequencies, means and standard deviations. Metric data were analysed for normal distribution using the Shapiro–Wilk test. Wilcoxon’s test was used for comparison of pre- and postoperative data, and the Mann–Whitney U test, or Chi-square test were used for comparisons between groups. Dichotomous variables were compared pre- and postoperatively using the McNemar test. Effect sizes (Cohen’s d) were measured via paired t-tests. By way of an exploratory analysis, Pearson’s correlation was used to test for correlations between preoperative radiological findings and clinical outcomes.
Results
Patient characteristics
We included 65 patients (27 males and 38 females), with a mean age of 43.9 ± 15.7 years (range 21–79 years), with radiologically confirmed CIM. Baseline characteristics are listed in Table 1. Comorbidities were present in 33 patients, with hypertension, asthma, diabetes, epilepsy and vertebral disc protrusion being the most frequent. Eight patients had psychological comorbidities, mostly depression or anxiety disorders.
Clinical data and neurological findings
Of the 65 patients, 41 (63.0%) experienced headache as the predominant symptom. Other leading symptoms were vertigo and dizziness in 12 patients and sensorimotor deficits or gait disorder in 12 patients. Results of the neurological examination presented abnormalities in 53.8% (mostly oculomotor disturbances and sensorimotor deficits, as listed in Table 1).
Headache semiology (according to ICHD-3) and acute and prophylactic headache therapy
Baseline headache characteristics of the 41 patients suffering from headache are listed in Table 2. Mean time between headache onset and diagnosis of CIM was 56.4 ± 11.3 months (range 0 months to 50 years). Headache was predominantly occipital or nuchal (80.5%) and bilateral (80.5%), and headache quality was mostly pressing (68.3%). The most frequent accompanying symptom was nausea with 43.9%. The average minimum headache intensity was 4.7 ± 1.4 on the NRS and the average maximum intensity was 7.8 ± 1.6. Monthly headache days were 22.4 ± 10.1 (range 1–31 days) and monthly days with acute medication use were 11.2 ± 9.9 (range 0–31 days).
Regarding semiology according to the ICHD-3, typical cough headache was seen in 21 patients (51.2%). Headache with other (‘atypical’) semiology was present in 20 patients (48.8%). Of note, all patients with typical cough headache also experienced pain evoked by Valsalva manoeuvre and laughing. Of the 20 individuals with atypical headache, semiology corresponded to chronic migraine (CM) in 10 cases (50.0%), episodic migraine (EM) in two (5.0%), chronic TTH (CTTH) in five (25.0%) and episodic TTH (ETTH) in three (15.0%) (see Table 2). No patient fulfilled the ICHD-3 criteria of more than one of the headache semiologies mentioned above. Medication overuse (defined as nonsteroidal anti-inflammatory drug (NSAR) or simple analgesic use ≥15 days per month or opioid or triptan use ≥10 days per month for at least 3 months consecutively) was seen in 10 patients. NSAR were used by 39%, metamizole or paracetamol by 24.4%, both by 14.6%, and one patients used opioids. In all, 19.5% did not use any acute medication. Only seven patients (17.0%) were on prophylactic headache medication (mostly amitriptyline, topiramate or pregabaline).
Baseline radiological data
Baseline radiological data were available for 49 patients (Table 3). Tonsillar descent was 12.2 ± 6.1 mm (range 5–27 mm), the McRae line was 37.5 ± 3.7 mm (range 31–46 mm). Spinal MRI detected syringomyelia in 23 cases (35.4% of all patients, 39.0% of the headache patients). Incidence of syringomyelia was not significantly different between non-headache patients (30.5%), typical (34.7%, p = 0.170), and atypical headache patients (34.7%, p = 0.271). Furthermore, there were no significant correlations between radiological characteristics and headache intensity or frequency (Supplemental Table 1).
Surgery
Foramen magnum decompression was performed in 49 patients (75.4%). This included 35 of the 41 patients with headache (18 of the 21 patients with typical cough headache, 10 patients of the 12 patients with a migraine semiology [eight CM, two EM], and seven out of eight patients with a TTH semiology [five CTTH, two ETTH]). 14 surgical interventions were performed due to non-headache symptoms. Mean operation time was 217 ± 54 min (range 133–331 min). C1-laminectomy was performed in all cases, durotomy with arachnoidal dissection and duraplasty in 42 patients, and tonsillectomy in 35 patients. The average ICU time was 1.0 ± 0.5 days (range 0–3 days). Four patients (8.1%) experienced postoperative complications (two wound healing disorder, one hydrocephalus, one meningitis). There were no severe residual neurological deficits. Surgery was not performed in 16 patients (including six headache patients) because of patient decision, mild symptoms, or contraindications.
Headache outcome
Thirty five of the 41 headache patients underwent foramen magnum decompression. After surgery, subjective headache relief was indicated by 30 patients (87.7%), whereas headache remained unchanged in two cases (4.9%) and worsened in three patients (7.3%).
Headache outcome data are summarised in Table 4. After foramen magnum decompression, maximum and minimum headache intensity, headache days per month and acute medication days per month were significantly reduced. When patients with cough headache and atypical headache were considered separately, headache improvement was present in both groups. Improvement was markedly more pronounced in the cough headache group (Table 4). This was true when considering statistical significance, which was achieved for all 4 outcomes in cough headache with very large effects sizes (Cohen’s d 1.10 to 1.85). In contrast, significance for atypical headache was only achieved for maximum intensity and monthly headache days with medium to large effects (Cohen’s d 0.42–0.82) (see Table 4). Headache outcomes of the different semiologies within the atypical headache group are listed in Supplementary Table 2, showing a significant improvement of headache intensity in patients with CM semiology and a significant improvement of headache frequency in patients with a CTTH phenotype. However, these groups were small and results have to be interpreted with caution. For comparison, we also analysed the outcome in the group of six headache patients who did not undergo surgery (three cough headache, one ETTH-like, two CM-like). These patients did not improve meaningfully regarding headache days per month: initial versus present: 21.0 ± 14.3 to 20.5 ± 13.7, z = −0.707, p = 0.480, n = 6, d = 0.58). Analgesics use per month did not change in this cohort (9.8 ± 9.6 to 10.3 ± 8.1, z = −647, p = 0.518, n = 6), had only minor changes in intensity regarding minimum NRS (4.6 ± 2.4 to 5.3 ± 1.6, z = −0.333, p = 0.739, n = 6) and mild improvement in maximum headache intensity (8.6 ± 1.5 vs. 7.67 ± 1.9, z = −1.730, p = 0.084, n = 6). However, because of the small number in this group, these data must also be interpreted with caution.
In 13 of the 18 cough headache patients, cough headache completely resolved after surgery, but some type of headache remained in all: Nine had infrequent TTH-like or migrainous headaches (ETTH or EM semiologies) after surgery, while four continued to have frequent headaches (≥15 days/month), corresponding to CTTH or CM semiologies. The other five cough headache patients continued to have cough headache after surgery, but with much reduced frequency and intensity. None of the atypical headache patients started to have cough headache after surgery.
Radiological outcome after foramen magnum decompression
Postoperative radiological data were available for 37 patients. The McRae line (after foramen magnum decompression: Midsagittal foramen magnum diameter) increased significantly (from 37.1 ± 3.7 mm to 54.8 ± 6.3 mm, z = −4.786, p < 0.001, n = 31), but the maximum a.p.-diameter of the fourth ventricle did not change significantly (z = −1.178, p = 0.239, n = 28). Although the maximum a.p.-diameter of the syrinx was significantly reduced after foramen magnum decompression (z = −2.032, p = 0.042, n = 7), the number of segments affected by syringomyelia did not change significantly (z = −1.000, p = 0.317, n = 4).
Correlation of radiological characteristics with headache improvement
We performed explorative correlations between preoperative radiological data with postoperative improvement in headache intensity and monthly headache days (Supplemental Table 3). Larger preoperative tonsillar descent was correlated significantly with larger improvement of minimum headache intensity after foramen magnum decompression (r = −0.42, p = 0.025, n = 28, Figure 2); however, there was no correlation with improvement of maximum headache intensity or headache frequency.

Association of preoperative tonsillar descent (mm) and difference between pre- and post-operative headache severity (NRS).
Discussion
Main results of the present study were: Almost half of the CIM patients with headache presented not with typical cough headache but with migrainous (29.3%) or TTH (19.5%) phenotypes. After foramen magnum decompression, headache improved especially in patients with typical cough headache, and less in migrainous and TTH-like headaches.
Patient characteristics were similar to those found in previous studies, with the exception of age, which was higher in our total population (43.9 years) (3,21). Similar to Batzdorf's work, vertigo and dizziness were the second-most prevalent symptoms, despite sensorimotor deficits being the second-most common in earlier research (21,22).
Typical cough headache was seen in 51.2% of our headache sample, compared to 63% in Berretta et al. (n = 135) and 87% in Curone et al. (n = 201) (6,20). Curone et al. investigated headache semiology in 201 patients with CIM revealing 28.8% with migraine criteria (6). In our study, 29% of headache patients met migraine criteria. Interestingly, 61% of our patients with headache exhibited at least one possibly migraine-related symptom (sensory phobias, nausea, or vomiting), compared to 38% (n = 201) in the work of Curone et al. (6). However, other studies reported lower frequency of migraine phenotype in CIM patients; for example, Kaplan et al. found that 15.1% of 73 CIM patients had migraine headaches (23). Furthermore, TTH was seen in 19.5% in our headache population, similar to 12.0% in a former study by Pascual et al. (7) With regard to medication overuse, in our study 24% of the headache patients met the criteria of medication overuse whereas former studies reported frequencies of 10% in CIM patients (6). Mean time from onset of symptoms to diagnosis was 56.4 ± 11.3 months, which was comparable to other studies (21).
Concerning surgical data, C1-laminectomy and tonsillar resection were typically performed in foramen magnum decompression at our centre. Durotomy with resection of the arachnoidea following duraplasty was done in 85.7%, comparable to previous data (21). Postoperative complications were rare. There were no persisting neurological deficits due to surgery, which is consistent with the findings of previous literature (20,22). However, careful inclusion of patients is a possible selection bias.
In our study, foramen magnum decompression reduced headache frequency, intensity, and acute medication use significantly. Subjective improvement was seen in most patients, which is similar to Grangeon et al., who reported headache relief in 57% of the patients (17). Other authors indicated a postoperative improvement in up to 81% of the patients, but without clarifying exact semiology of the patients (22,24).
When headache outcomes of different headache semiologies were considered, cough headache had the largest improvements. This is similar to Grangreon et al., where short attacks with duration <5 min, strong intensity, occipital accentuation, and Valsalva manoeuvre-induced headache had been prognostically favourable factors after decompression (17). In contrast, patients with other headache phenotypes improved less. It must be considered that primary headaches such as migraine and TTH have a high prevalence. Cranial imaging is sometimes performed in patients with a primary headache phenotype, e.g. in therapy refractory cases, or in cases with features deemed atypical (e.g. prolonged aura). Therefore, in patients with primary headache phenotypes, CIM might have been an incidental finding, without causal relation to the headache. In these cases, improvement over time might be due to the natural course, as primary headache disorders often improve with age (25). On the other hand, most patients indicated subjective headache relief shortly following the surgery. However, this might also have been reinforced by the strong placebo effect usually associated with a surgical treatment. Unfortunately, the cohort of CIM patients with headache that did not undergo surgery was rather small, precluding its use as a valid control group. However, all things considered, the present results suggest that in patients with CIM and headache fulfilling migraine or TTH criteria, a neurologist should be involved and classical preventive headache therapy should be tried before considering foramen magnum decompression for headache relief. This would also be true for patients suffering from both, cough headache and a primary headache phenotype, if cough headache is not clearly the leading headache type.
In terms of radiological findings, mean preoperative tonsillar descent was 12.2 ± 6.1 mm, which is more than in other publications (26) with 6.4 ± 2.2 mm. Furthermore, syringomyelia was seen in 35.4% of our total population, compared to 65% to 75.8% in other studies (24,27). Syringomyelia was not related to headache in our study, in line with prior studies (7). Our trial as well as others did not show a significant correlation between headache symptoms and extent of tonsillar descent. However, in the present study, larger tonsillar descent was related to an improvement of minimum headache intensity. This had not been shown in previous literature (17,18). Restrictively, it must be emphasised that improvement of maximum headache intensity and headache frequency were not significantly correlated with tonsillar descent, and this finding was the result of an explorative analysis without correction for multiple testing. It therefore must be regarded with caution.
Limitations
Main limitation is the retrospective study design, as it introduces an unavoidable recall bias. Some patients who had foramen magnum decompression more than 10 years ago had to recall missing data from a headache symptom that had not been recorded in the charts. Another limitation is the relatively small absolute number of CIM patients with headache who underwent surgery (n = 35). In addition, the group of CIM patients with headache who did not undergo surgery was very small (n = 6), precluding its use as a proper control group for the natural course of headache in CIM patients.
Conclusion
Typical cough-induced headache remains the mainstay of the clinical manifestation in CIM, but atypical headaches accounted for almost half of our CIM cohort. Incidental findings in imaging studies performed in primary headache patients might contribute to this. In cases with a typical cough headache, surgical decompression is effective for CIM-related headache treatment. Although migrainous and TTH-like headaches also improved after surgery, the effect was smaller, and should be compared to the natural course of primary headache disorders in future studies. The present results may be useful for counselling patients with CIM regarding surgery according to their headache type and emphasise that careful history taking and, where appropriate, involvement of a neurologist, are important to determine the best therapy for a given patient with CIM.
Clinical implications
Migrainous and TTH-like headaches can be found in Chiari 1 malformation, but causality remains unclear. Occipital decompression is effective for headache relief, particularly in patients with typical cough headache. Migrainous and TTH-like headaches respond less well to surgery.
Supplemental Material
sj-pdf-1-cep-10.1177_03331024221079296 - Supplemental material for Headache characteristics and postoperative course in Chiari I malformation
Supplemental material, sj-pdf-1-cep-10.1177_03331024221079296 for Headache characteristics and postoperative course in Chiari I malformation by Dennis C Thunstedt, Michael Schmutzer, Matthias P Fabritius, Jun Thorsteinsdottir, Mathias Kunz, Ruth Ruscheweyh and Andreas Straube in Cephalalgia
Footnotes
Acknowledgements
Conceptualisation: DCT, AS; methodology: DCT, RR, MPF, JT, MK, MS, AS; formal analysis and investigation: DCT, JT, MK, MPF, MS; writing – original draft preparation: DCT; writing – review and editing: DCT, MS, RR, AS, JT, MK, MPF; supervision: AS, RR, JT, MK.
Ethical approval
This retrospective non-interventional monocentric study was approved by the ethics committee of the Ludwig Maximilian University (LMU), Munich, Germany (project number 21-0300) and prospectively registered in the German Clinical Trials Register (DRKS) (DRKS00025285).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All patients provided written informed consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.