
Abstract

Epidemiology, comorbidity, outcomes and classification including big data
MTV20-OR-001
Migraine headache frequency and attack triggers during the coronavirus disease 2019 (COVID‐19) pandemic
Faraidoon Haghdoost1,*, Candice Delcourt2, Cheryl Carcel2, Deepak Chandrasekhar3, Weijie Poh3, François Cadiou3 and Anthony Rodgers1
1The George Institute for Global Health, University of New South Wales, Sydney, Australia
2The George institute for Global Health, The University of NSW, Royal Prince Alfred Hospital, The University of Sydney., Sydney, Australia
3Healint Pte Ltd, Singapore., Singapore, Singapore
Introduction
Chronic diseases have been shown to be at great risk for worsening during the Coronavirus disease 2019 (COVID‐19) pandemic. However, there is little data on the effect of COVID-19 on migraine frequency.
Objectives
To evaluate the effect of COVID‐19 on migraine headache frequency and most reported triggers for the headache attacks.
Methods
Self-reported data in the migraine tracking smartphone app Migraine Buddy (MB) for January, February, March and April in 2018, 2019 and 2020 were collected. Users who had recorded at least one attack in the respective months were included in analysis. Demographic data such as age, sex and country were collected, where available. Headache frequency per month and four most reported triggers were collected. Data was self-reported, and user data was de-identified. Online t-test was used to compare the means.
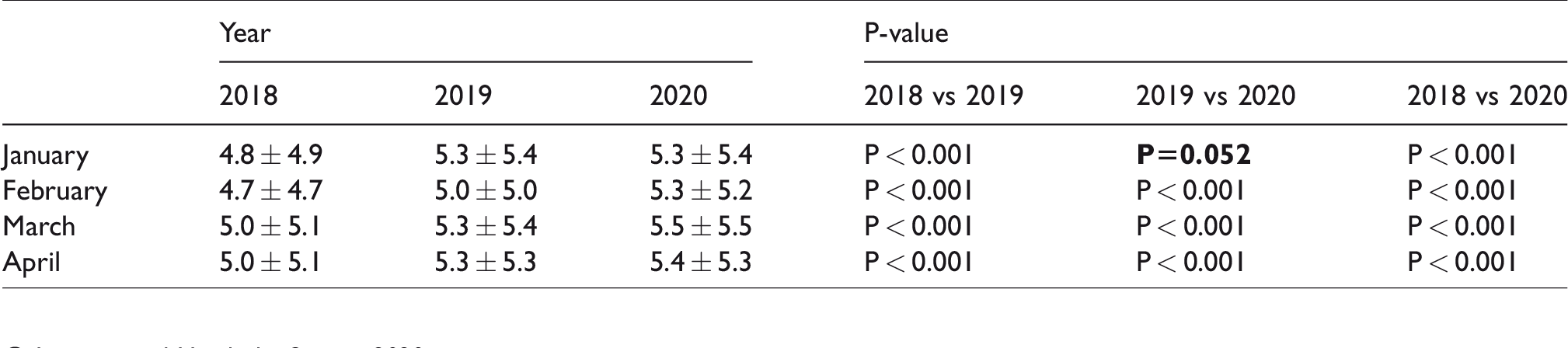
Mean (±SD) reported headache frequency per month.
Results
Data from an average of 124,717 users per month was collected. Among those with data on age and sex, mean age was 36.3 ± 10.9 years and 89% were female. The largest group of users were from the United States (average 47%).
Mean migraine headache frequency is reported in table 1. The four most commonly reported triggers for migraine attacks were stress, lack of sleep, neck pain and anxiety. For 2018, 2019 and 2020, the reported triggers for a migraine attack were stress in 39.7%, 38.4% and 36.1%, lack of sleep in 25%, 25% and 22.8%, neck pain, 20%, 20.4% and 19.3% and anxiety in 19%, 18.4% and 18.4%, respectively.
Conclusion
Among MB users, there has been a small increase in self-reported migraine frequency over last 3 years. This could reflect a real increase, change in reporting habits, or change in makeup of MB users. There was no evidence that frequency changed substantially in March and April 2020 from previous years or from records in January and February. In addition, the proportion of most common triggers including stress, lack of sleep, neck pain and anxiety decreased in a small degree in corresponding months of 2020 compare to 2019 and 2018.
Epidemiology, comorbidity, outcomes and classification including big data
MTV20-OR-003
THE USE OF IMAGING IN THE DIAGNOSIS OF HEADACHE- A RETROSPECTIVE ANALYSIS
William E. Alton1,* and David Watson2
1University of Aberdeen
2Hamilton Medical Group, Aberdeen, United Kingdom
Introduction
The use of imaging to investigate headaches is commonplace, but little data are available documenting the outcomes in a secondary care setting. We undertook a 5 year retrospective analysis to understand the appropriateness of neuroimaging to detect the headache aetiology in this setting.
Objectives
1) Identify the demographics of patients presenting with headache
2) Quantify the detection rate, using different modalities of imaging, of headache-causing pathology
3) Quantify the incidental findings unearthed through imaging
4) Contribute to understanding of the appropriateness of neuroimaging in the work-up of headache aetiology
Methods
Data were retrospectively collected from 233 patients between the years 2015–2019 inclusive from a secondary care headache clinic in Aberdeen Royal Infirmary. Parameters recorded included sex, age on the day of scan, headache type/concerning neurological symptoms, reason for imaging, imaging modality and both headache-causing pathology and incidental findings noted on the scan.
Results
1214 new patients were seen of which 233 (19.2%) underwent neuroimaging. Of the 223 patients scanned using either CT or MRI, 53.4% (n = 119) were female. The commonest age band of patients (19.3%, n = 43) were in the age range of 50–59. The most common diagnosis pre-imaging was ‘New Daily Persistent Headache’ (n = 76, 34.1%). The most common reasons for scanning were a) new symptoms b) change of symptoms c) change in headache pattern and d) doctor uncertainty, which together represented 50.2% of cases (n = 112). Out of the 223 patients scanned, 3 yielded secondary headache-causing pathology (1.3%) including a vascular loop, pituitary adenoma and Chiari malformation with descent of cerebellar tonsils, kinking and compression of brain stem and syrinx. Incidental findings were noted in 105 of the 223 patients (47.1%). Incidental findings differed with imaging modality, occurring in 37.9% of CT and 60.4% of MRI scans (p < 0.01).
Conclusion
In the context of secondary care, neuroimaging provides a low diagnostic yield for determining the aetiology of headaches. Our data are consistent with the literature suggesting the chance of identifying headache causing pathology using neuroimaging is <10%. Whilst guidelines are in place to assist with decisions regarding who should be scanned, the scan requestor’s experience and other factors, such as possibility of litigation, play a role. Incidental findings were present in approximately 50% of patients, depending on imaging modality. A larger proportion of incidental findings related to soft tissues, for example small vessel disease, explaining the greater preponderance with MRI. Additional investigations are needed to improve the positive detection rate and cost-effectiveness of neuroimaging for headache.
Experimental research
MTV20-OR-004
INVESTIGATION OF SEX-BASED CHARACTERISTICS OF BEHAVIORAL RESPONSES, ABSOLUTE CEREBRAL BLOOD FLOW, AND RESTING-STATE FUNCTIONAL NETWORKS IN A SURROGATE RODENT MODEL OF MIGRAINE
Mareike Hörnschemeyer1,*, Parisa Gazerani2 and Zhifeng Liang3
1Neuroscience & Neuroimaging, Sino-Danish-Center for Education and Research, Aarhus C
2Department of Health Science and Technology, Faculty of Medicine, Aalborg University, Aalborg, Denmark
3Laboratory of Comparative Neuroimaging, Institute of Neuroscience, Shanghai, China
Introduction
Migraine is manifested by recurrent headache attacks, sensory, and transient motor disturbances. The current consensus states a potential contribution of neuronal, non-neuronal, and vascular components of the trigeminovascular system in the pathophysiology of migraine. Despite the higher prevalence in women and multiple lines of evidence highlighting migraine as a sexually dimorphic disorder, preclinical studies have largely excluded females in surrogate models of migraine.
Objectives
This study investigated sex-based behavioral characteristics and potential underlying mechanisms in a surrogate rodent model of migraine with the aid of awake rodent functional magnetic resonance imaging (fMRI).
Methods
Adult male and female (normal cycling) Sprague-Dawley rats (n = 32) received supradural injections of inflammatory soup (IS) and were evaluated for cephalic and extracephalic sensitivity to mechanical stimuli with von Frey, light aversive behavior with a light-dark-box, and facial expression with the rat grimace scale. We also performed awake rodent arterio-spin-labeling and resting-state fMRI to investigate sex-related differences in absolute cerebral blood flow (CBF) and resting-state functional networks (rsfN) in IS-treated animals compared with saline-treated controls.
Results
Data demonstrated significant behavioral changes following IS, including nocifensive response and migraine-like symptoms, with overall stronger manifestations in females. A sex-treatment interaction was found in cortical and subcortical areas, in the limbic, visual, and auditory systems. Higher mechanical sensitivity observed in females could be related to the higher activity of cortical areas and stronger light-aversive behavior might be due to higher activity in superior colliculus and cerebellum involved in avoidance behavior. Higher perfusion and increased rsfN of limbic structures could also explain higher nociception and anxiety seen in females. Activation of the pretectal region and rsfN of the caudate putamen could explain stronger anti-nociceptive responses in males.
Conclusion
This study provided the first evidence that the IS model can be used for investigation of sex-based characteristics of migraine, and potentially testing of sex-specific migraine therapeutics. It also highlighted that the awake rodent imaging approach with the possibility of fMRI scans shortly after the IS injection, could mimic the ictal phase of the migraine while overcoming a need for anesthesia.
General aspects of headache care
MTV20-OR-005
CLINICAL CHARACTERISTICS AND PERFUSION CT ALTERATIONS IN A SERIES OF MIGRAINE WITH AURA ATTENDED AS STROKE CODE
Alicia Gonzalez-Martinez1,*, Santiago Trillo2, Carmen Benavides Bernaldo de Queirós3, Laura Casado Fernández4, Ana B. Gago Veiga5, María De Toledo6, Antonio Barbosa del Olmo7, Rafael Manzanares Soler8 and José Vivancos9
1Department of Neurology, Hospital Universitario de La Princesa & Instituto de Investigación Sanitaria de La Princesa
2Stroke Unit, Department of Neurology, Hospital Universitario de La Princesa
3Department of Neuroradiology, Hospital Universitario de la Princesa & Instituto de Investigación Sanitaria de la Princesa
4Department of Neurology
5Headache Unit, Department of Neurology
6Epilepsy Unit, Department of Neurology
7Department of Neuroradiology
8Departmen of Neuroradiology
9Head of Department, Stroke Unit, Department of Neurology, Hospital Universitario de La Princesa & Instituto de Investigación Sanitaria La Princesa, Madrid, Spain
Introduction
Migraine with aura is one of the most frequent stroke mimics (SM) after epileptic seizures, since the focal neurological symptoms associated with migraine with aura (MA) can be confused with stroke when they have an abrupt onset.
Objectives
The aim of our study is to analyze perfusion CT (PCT) alterations in patients treated as a stroke code with a final diagnosis of MA.
Methods
We carried out a retrospective study including patients with a final diagnosis of MA at discharge who were treated as code stroke with complete multimodal CT (baseline CT, angio CT and perfusion CT) between January 2015 and March 2018.
Results
Of a total of 1761 patients treated as stroke code, 284 were SM with complete multimodal CT, of which 25 were MA (7.3%). Among MA patients, 14/25 (56%) were women, the average age was 39 years (SD 13.15) and 12/25 (50%) had previous history of migraine. The most frequent aura was of the sensitive type. Time elapsed between the onset of symptoms and the performance of CT was 194 minutes on average. We found alterations in PCT in 3/25 (12.5%), with a lower frequency than that observed in other SM such as epileptic seizures (x2; p < 0.001) or status epilepticus (x2; p < 0.001). The PCT pattern found in MA was hypoperfusion pattern not restricted to a vascular territory. All the three patients had aphasia as the presenting symptom.
Conclusion
In our study, MA was a frequent cause of MS. Patients with MA presented a lower frequency of alteration in PTC compared to other SM such as seizures or epileptic status. Aphasia was a focal symptom common to all patients with MA and an alteration in PTC. Further research on PCT patterns and clinical characteristics of patients with MA presenting as SM would be useful in order to help clinicians diagnose MA among patients with aphasia attended stroke code.
General aspects of headache care
MTV20-OR-006
ASSESSMENT OF ATTENTION, VIGILANCE, AND EXECUTIVE FUNCTIONS IN MIGRAINE: A CLINIC-BASED STUDY FROM NORTH INDIA
Debabrata Datta* and Debashish Chowdhury1; G B Pant headache group
1Neurology, G B Pant Institute of Post Graduate Medical Education and Research, NEW DELHI, India
Introduction
Migraine patients often report ictal and inter-ictal cognitive symptoms related to deficits in attention, executive function, and memory. However, several clinic and population-based studies that assessed cognitive dysfunctions in migraine patients have shown conflicting results.
Objectives
To study the cognitive function in terms of attention, vigilance and executive functions in migraine patients during the inter-ictal phase and compare them with healthy controls.
Methods
Consecutive patients of migraine attending the headache clinic aged ≥18 years and who were able to read, write & have elementary school education of at least 5th standard were included. Only preventive drug naïve patients were included. Episodic migraine (EM) patients were assessed at least after 72 hours of the last headache episode and chronic migraine (CM) patients were ≥assessed during non-migraine or headache-free days or at least after 72 hours of the last migraine episode. An equal number of matched normal healthy volunteers without any history of headache served as controls. Mini-mental state examination (MMSE), frontal assessment battery (FAB), digit span forward and backward (DSF, DSB), Stroop word (SW), Stroop color (SC) and Stroop word & color interference tests (SI), trail making test A (TMT-A) and B (TMT-B) scores were generated and compared between patients and controls.
Results
A total of 150 patients (122 EM and 28 CM) were studied. There were 30 males and 120 females and the mean age of onset of migraine was 28.9 ± 8.3 years. The average migraine days per month in EM and CM were 5.4 ± 2.7 and 14.0 ± 4.2 respectively. The mean headache severity by visual analog scale (VAS) was 7.1 ± 1.4 and headache impact by HIT-6 and 61.4 ± 5.9 respectively. MMSE score was not significantly different between migraine patients (27.6 ± 2.0) and controls (27.8 ± 1.9). Migraine patients as compared to controls fared worse in FAB (14.5 ± 2.0 vs 16.1 ± 1.4; p =<0.0001), DSF (6.3 ± 1.8 vs 6.7 ± 1.5; p = 0.0206), DSB (61.4 ± 5.9 vs 4.8 ± 1.3; p =<0.0001), SW (47.3 ± 10.8 sec vs 40.6 ± 7.6 sec; p =<0.0001); SC (76.9 ± 16.1sec vs 69.8 ± 12.3 sec; p =<0.0001); SI (139.3 ± 25.6sec vs 130.8 ± 23.6 sec; p = 0.0022), TMT-A (39.3 ± 13.5sec vs 32.4 ± 8.5 sec; p =<0.0001)and TMT-B (90.8 ± 36.2sec vs 72.4 ± 27.0 sec; p =<0.0001).
Conclusion
Migraine patients showed significant cognitive dysfunctions in terms of attention, vigilance, and executive functions involving mental processing speed, mental flexibility, inhibitory control & monitoring, and working memory. They also had significantly poorer performances in overall frontal lobe functions. Contrarily, MMSE did not discriminate between migraine patients and controls.
Headache pathophysiology: basic science
MTV20-OR-007
OREXINERGIC NETWORKS REGULATING MIGRAINE INITIATION
Paula Sureda Gibert1,*, Lauren C. Strother1, Peter J. Goadsby1, Maurice Vincent2, Keith A. Wafford2, Gary Gilmour2 and Philip R. Holland1
1Basic and Clinical Neuroscience, King’s College London, London
2Lilly Centre for Cognitive Neuroscience, Eli Lilly and Company, Windlesham, United Kingdom
Introduction
Migraine patients commonly report head pain and marked fatigue as hallmarks of their attacks. Given the key role of orexinergic regulation in modulating central nervous system (CNS) homeostasis (i.e. sleep or appetite) and its ability to modulate trigeminal pain processing, we sought to determine the impact of orexinergic ablation on orofacial sensory processing in orexin-cre+ transgenic mice.
Objectives
We aimed to determine the role of orexin-mediated hypothalamic networks on orofacial sensory processing, and establish the potential efficacy of intranasal orexin A to reverse induced migraine-like phenotypes.
Methods
Sixteen adult mice (7 orexin Cre+, 9 Wild-type) underwent targeted ablation of hypothalamic orexinergic neurons via stereotaxic injection of a cre-dependent diphtheria toxin (dtA) into the lateral hypothalamus. Orofacial mechanical withdrawal thresholds were assessed longitudinally through the up-down method, as a marker of allodynia. These were assessed between groups using independent t-tests corrected for multiple comparisons. To determine the impact of intranasal orexin A, orexin ablated and wild-type mice were subsequently administered orexin A (10ng/ul) twice a day for five days.
Results
Ablation of hypothalamic orexinergic neurons induced orofacial hypersensitivity (P = 0.016), as a preclinical readout of migraine-related cephalic allodynia. Subsequent chronic administration of intranasal orexin A for 5 days, fully reversed the orexin ablation-induced orofacial hypersensitivity (P = 0.08) when compared to control mice.
Conclusion
Our data highlights that orexinergic circuits play key roles in the regulation of head pain and dysfunctional orexinergic signalling may link abnormal sensory processing in migraine patients. In addition, we identify orexin A, and potentially orexin 1 receptor activation as a potential therapeutic intervention to treat migraine-related pain.
Headache pathophysiology: basic science
MTV20-OR-008
MECHANISMS OF ACTION OF VERAPAMIL IN A PRECLINICAL MODEL OF CLUSTER HEADACHE
Marta Vila-Pueyo1,*, Zuzanna Bojarowska1, Peter J. Goadsby1 and Philip R. Holland1
1Basic and clinical neurosciences, King’s College London, London, United Kingdom
Introduction
Verapamil, the preferred preventive treatment for cluster headache (CH), has an unknown mechanism of action. The high doses required for clinical efficacy can result in significant cardiovascular side effects.
Objectives
In order to develop more effective, well-tolerated therapies, we explored the potential mechanisms of action of verapamil in a preclinical model of CH.
Methods
Male Sprague-Dawley rats (n = 48) were anesthetized and surgically prepared to permit placement of a stimulating electrode in the superior salivatory nucleus (SSN), to evoke cranial parasympathetic activation. To record SSN-evoked changes in choroidal blood flow a laser Doppler probe was placed on the anterior choroid. Alternatively, to record SSN-evoked trigeminovascular nociceptive activation a recording electrode was positioned in the trigeminocervical complex. Following baseline responses to SSN stimulation, animals were intravenously infused with verapamil, specific agonists/antagonists and appropriate vehicle controls, with responses recorded for 90 minutes.
Results
Verapamil decreased choroidal blood flow responses to SSN stimulation when compared to the vehicle-treated rats (F2.7,55 = 4.5, P = 0.009). These responses were inhibited by blockade of hyperpolarization-activated cyclic nucleotide-gated (HCN) channels, but not L-type calcium channels. Verapamil also inhibited trigeminocervical complex neuronal responses to SSN stimulation when compared to vehicle-treated rats (F4.7,47 = 3.27, P = 0.014), an effect that was also blocked by HCN antagonism.
Conclusion
The results demonstrate a clear translational effect of verapamil in a preclinical model of CH that contrary to the accepted mechanism, was not L-type calcium channel-dependent. Instead, responses were HCN-dependent suggesting neural HCN channels as a potential novel therapeutic target for CH.
Headache pathophysiology: clinical
MTV20-OR-009
MIGRAINE WITH AURA IN WOMEN IS NOT ASSOCIATED WITH STRUCTURAL THALAMIC ABNORMALITIES
Anders Hougaard*, Silas H. Nielsen, David Gaist, Oula Puonti, Ellen Garde, Nina L. Reislev, Pernille Iversen, Camilla G. Madsen, Morten Blaabjerg, Helle H. Nielsen, Thomas Krøigaard, Kamilla Østergaard, Kirsten O. Kyvik, Kristoffer H. Madsen, Hartwig R. Siebner and Messoud Ashina
Introduction
Migraine with aura is a highly prevalent disorder involving transient neurological disturbances associated with migraine headache. While the pathophysiology is incompletely understood, findings from clinical and basic science studies indicate a potential key role of the thalamus in the mechanisms underlying migraine with and without aura. Two recent, clinic-based MRI studies investigated the volumes of individual thalamic nuclei in migraine patients with and without aura using two different data analysis methods. Both studies found differences of thalamic nuclei volumes between patients and healthy controls, but the results of the studies were not consistent.
Objectives
To investigate whether migraine with aura is associated with changes in thalamic volume
Methods
We analyzed MRI data obtained from a large, cross-sectional population-based study which specifically included women with migraine with aura (N = 156), unrelated migraine-free matched controls (N = 126), and migraine aura-free co-twins (N = 29) identified from the Danish Twin Registry. We used two advanced, validated analysis methods to assess the volume of the thalamus and its nuclei; the MAGeT Brain Algorithm and a recently developed FreeSurfer-based method based on a probabilistic atlas of the thalamic nuclei combining ex vivo MRI and histology. These approaches were very similar to the methods used in each of the two previous studies. Between-group comparisons were corrected for potential effects of age, educational level, BMI, smoking, alcohol, and hypertension using a linear mixed model. Further, we used linear mixed models and visual inspection of data to assess relations between migraine aura frequency and thalamic nuclei volumes in patients. In addition, we performed paired t-tests to compare volumes of twin pairs (N = 29) discordant for migraine with aura.
Results
None of our analyses showed any between-group differences in volume of the thalamus or of individual thalamic nuclei.
Conclusion
Our results indicate that the pathophysiology of migraine with aura does not involve alteration of thalamic volume.
Headache pathophysiology: clinical
MTV20-OR-010
RESTING STATE FUNCTIONAL CONNECTIVITY CHANGES OF THE HYPOTHALAMUS IN MIGRAINE PATIENTS: A CROSS-SECTIONAL AND LONGITUDINAL STUDY
Roberta Messina1,*, Paola Valsasina1, Paolo Misci1, Maria Assunta Rocca1 and Massimo Filippi1
1IRCCS San Raffaele Scientific Institute, Milan, Italy
Introduction
Previous studies support the role of the hypothalamus in the early and interictal phase of the migraine attack.
Objectives
The aim of our study was to explore cross-sectional and longitudinal resting state functional connectivity (RS FC) changes of the hypothalamus in patients with migraine.
Methods
Using a 3.0 Tesla scanner, RS functional magnetic resonance imaging (MRI) and 3D T1-weighted scans were acquired from 91 headache-free episodic migraine patients and 73 controls. Twenty-three migraine patients and 23 controls were reexamined after 4 years.
Maps of hypothalamic RS FC were obtained for each subject using a seed-region correlation approach. A whole-brain voxel-wise analysis was performed to assess hypothalamic RS FC abnormalities between groups using the general linear model and theory of gaussian fields, as implemented in SPM12. The correlation between functional MRI abnormalities and patients’ clinical characteristics was also investigated.
Results
At baseline, compared to controls, migraine patients showed a decreased RS FC between the right and left hypothalamus and the right cerebellum, left parahippocampus and bilateral orbitofrontal cortex (OFC). The left hypothalamus had also a decreased RS FC with the left middle frontal gyrus. While, the right hypothalamus had a decreased RS FC with the right inferior temporal gyrus, lingual gyrus and left calcarine cortex. At baseline, the decreased RS FC between the right hypothalamus and the ipsilateral lingual gyrus correlated with higher migraine attack frequency (r = –0.4, p < 0.05, FWE corrected). After 4 years, migraine patients developed an increased FC between the hypothalamus and the OFC, bilaterally, while RS FC between the right hypothalamus and the ipsilateral lingual gyrus decreased. RS FC between the right hypothalamus and the ipsilateral OFC correlated with lower migraine attack frequency at year 4 (r = –0.6, p < 0.001, uncorrected).
Conclusion
RS FC of the hypothalamus changes dynamically in migraine patients. During the interictal phase, the hypothalamus modulates the activity of pain and visual processing areas in migraine patients. The recurrent experience of migraine attacks might disrupt the functional interaction between the hypothalamus and high-order visual processing areas. An increased RS FC between the hypothalamus and brain areas belonging to the descending pain-inhibitory pathway might reduce migraine attack frequency over time.
Post-traumatic headache
MTV20-OR-011
CGRP MONOCLONAL ANTIBODY (MAB) PREVENTS DYSREGULATION OF CENTRAL PAIN MODULATION AND POST-TRAUMATIC HEADACHE FOLLOWING MILD TRAUMATIC BRAIN INJURY IN MICE
Caroline M. Kopruszinski1,*, Joelle M. Turnes2, Todd J. Schwedt3, David W. Dodick3, Trent Anderson4, Edita Navratilova1 and Frank Porreca1
1Pharmacology, University of Arizona, Tucson, United States
2Pharmacology, Federal University of Parana, Curitiba, Brazil
3Neurology, Mayo Clinic
4Biomedical Sciences, University of Arizona, Phoenix, United States
Introduction
The “pain inhibits pain” phenomenon is a dynamic measure of net descending inhibition form central pain modulatory circuits. The efficiency of descending inhibition is evaluated as conditioned pain modulation (CPM) in humans and is referred to as diffuse noxious inhibitory controls (DNIC) in preclinical studies. Loss of CPM has been demonstrated in patients with different chronic pain and headache disorders, including post-traumatic headache (PTH) induced by mild traumatic brain injury (mTBI), and is a mechanism that is likely to promote pain progression and/or persistence. PTH often presents with a migraine-like phenotype. Calcitonin-gene related peptide (CGRP) plays a pivotal role in migraine and preclinical studies have also revealed its involvement in mTBI-related PTH.
Objectives
Determination of the role of CGRP in promoting PTH and dysregulation of central pain modulation induced by mTBI in mice.
Methods
Male, C57BL/6J mice received light anesthesia alone (sham) or in combination with a mTBI. The mTBI was induced by a weight drop onto a closed and unfixed skull, which allowed free head rotation after impact. DNIC was assessed as the latency to a thermally-induced tail-flick that served as the test stimulus in the presence of right forepaw capsaicin injection that provided the conditioning stimulus. DNIC was assessed between naïve mice or 2 days after sham or mTBI, with or without intraperitoneal treatment with the anti-CGRP monoclonal antibody, fremanezumab or vehicle 2 hours after the injury. Periorbital and hindpaw cutaneous allodynia (CA) was determined by the assessment of the frequency of response to tactile stimulation.
Results
Capsaicin injection into the forepaw of naïve and sham mice elevated the latency to tail-flick, reflecting the antinociceptive DNIC response. CA, as well as loss of DNIC was observed in mice with mTBI. Systemic treatment with fremanezumab blocked mTBI-induced CA and prevented the loss of DNIC.
Conclusion
Sequestration of CGRP in the initial stages of mTBI, abolished the development of acute CA that may reflect mTBI-related PTH and additionally, prevented the loss of net descending inhibition within central pain modulation pathways. As loss of CPM/DNIC has been linked to multiple chronic pain conditions, these findings suggest an opportunity for early anti-CGRP intervention for the treatment of mTBI-induced PTH and for inhibiting mechanisms that may promote the persistence of PTH.
Psychological and behaviour factors
MTV20-OR-012
EFFECT OF LOCKDOWN DURING COVID-19 ON MIGRAINE: A COHORT STUDY
Iris E. Verhagen*, Daphne S. van Casteren1, Simone de Vries Lentsch1 and Gisela M. Terwindt1
1Neurology, LUMC, Leiden, Netherlands
Introduction
The recent Coronavirus outbreak (COVID-19) and associated lockdown measures have enormous impact on individuals. Lockdown could potentially positively impact migraine patients as migraine patients may benefit from a life with less time-locked outdoor work- and social obligations.
Objectives
The objective of this study was to asses if Dutch intelligent lockdown measures during COVID-19 impact migraine-related outcomes.
Methods

Results
Intelligent lockdown led to a decrease in monthly number of migraine days (−0.48; 95%CI: −0.79 to −0.18, P = 0.002) and acute medication intake (−0.48; 95%CI: −0.76 to −0.20, P < 0.001), and an increase in general well-being (0.11; 95%CI: 0.06 to 0.17, P < 0.001). No differences in monthly number of non-migrainous headache days and pain coping were observed.
Conclusion
Our findings imply that intelligent lockdown measures can improve migraine disability despite of the stress COVID-19 presumably causes. We assume that this effect is a combined result of working from home, scaling down demanding social lives, and freedom to choose how to organize one’s own time to better reconcile suffering from migraine and work- and social obligations.
Secondary headaches
MTV20-OR-002
CLINICAL CHARACTERIZATION OF HEADACHE ATTRIBUTED TO COVID-19: A SERIES OF 457 CASES.
Álvaro Sierra1, David Garcia-Azorin2,*, Javier Trigo3, Ana Alberdi4, Ana Cornejo4, Ana Gil4, Ana Guiomar Lozano4, Carol Montilla4, Carolina Perez4, Cristina García4, Cristina Martinez Vadillo4, Gabriela Nuñez4, Ismael Calcerrada4, María Blanco4, Marina Paniagua4, Marta Mora4, Miguel Cubero4, Leticia Sierra4, Luisa Hurtado4 and Ángel L. Guerrero2
1Hospital Clinico Universitario Valladolid
2Headache Unit, Hospital Clínico Universitario de Valladolid
3Headache Unit, Hospital Clínico Universitario Valladolid
4Primary Care, Valladolid East Primary Care Area, Valladolid, Spain
Introduction
Headache is one of the most frequent symptoms of coronavirus disease 2019 (Covid-19). Most of the published series and cases described hospitalized patients, which could bias the results because of a more severe Covid-19.
Objectives
In the present study we aim to describe the clinical phenotype of headache attributed to Covid-19 (HAC-19) including the full spectrum of patients, including cases managed both in primary care and hospital care.
Methods
We screened the presence of headache all consecutive patients with a confirmed diagnosis of Covid-19, since the first hospitalized patient (March 8th, 2020) until April 11th. Patients with headache and capability to describe the headache phenotype were invited to participate. Diagnosis was confirmed by polymerase chain reaction test in all patients. A physician conducted a structured interview including demographic and clinical variables. Local ethics review board approved the study (PI 20-1738).
Results
A total of 138/576 (26.0%) hospitalized patients and 408/1690 (24.1%) primary care patients described headache, being included in the study 105 and 352 of them. Mean age was 52.1 ± 15.6 years, being 329 (72.0%) female, and 151 (33.0%) had pneumonia. Prior history of headache was described by 223 (48.8%) of patients, being migraine in 83 (18.2%). Headache was the first Covid-19 symptom in 126 (27.6%) patients and the mean duration of headache was 12.8 (16.1) days.
The most frequent concomitant symptoms were olfactory disorders in 268 (58.6%) cases, followed by asthenia 335 (73.3%), cough 296 (64.8%), fever 259 (56.7%), and myalgia 223 (48.8%). Headache was the most bothersome Covid-19 symptom in 69 (15.1%) cases, being the mean intensity 6.9 ± 1.7. Patients estimated that headache allowed them to do 49.1 ± 32.6% of their planned activities because of it. The headache was holocranial in 335 (73.3%), with frontal topography in 244 (53.4%), followed by temporal (121 (26.5%) and periocular in 97 (21.2%). Quality of pain was oppressive in 323 (70.7%) and throbbing in 66 (14.1%). Patients described avoidance of routine physical activity in 288 (63.0%) cases, photophobia in 150 (32.8%) cases, phonophobia in 146 (31.9%), and nausea in 69 (15.1%). The most frequently used symptomatic medication was paracetamol in 379 (82.9%), followed by ibuprofen in 70 (15.3%) and metamizole in 48 (10.5%).
Conclusion
Headache is a frequent symptom in Covid-19 disease. The clinical phenotype combines features from both tension-type headache and migraine, with moderate intensity and significant disability. A quarter of patients described headache as the first Covid-19 symptom.
INDUSTRY ORAL PRESENTATIONS Epidemiology, comorbidity, outcomes and classification including big data
MTV20-OR-014
INCIDENCE OF INPATIENT CONSTIPATION AMONG MIGRAINE PATIENTS TREATED WITH ERENUMAB: A RETROSPECTIVE COHORT STUDY IN A US ELECTRONIC HEALTH RECORD DATABASE
Veena Hoffman1,*, Karminder S. Gill2, Christine A. Szekely2, Gally Reznor1, Stephen M. Ezzy1, Andrew S. Park2, Robert Urman2, Rohini K. Hernandez2, Marco Navetta2, Sandra Lopez-Leon3, Denise E. Chou2, Fei Xue2 and Florence T. Wang1
1Optum, Boston, MA
2Amgen, Thousand Oaks
3Novartis Inc., East Hanover, NJ, United States
Introduction
Erenumab was approved in the US in May 2018 as a first in class treatment for migraine prevention in adults. Constipation with serious complications has been observed among erenumab users in the post-marketing setting.
Objectives
This study describes the incidence of inpatient (IP) constipation among new erenumab users, overall and by baseline characteristics.
Methods
New erenumab users age ≥18 years were identified using prescription orders from May 2018 – March 2019 in the Optum Electronic Health Record Database. Patients were required to have at least 1 migraine diagnosis (ICD-10-CM G43.-) or prescription for a triptan/ergot in the prior year, and at least 1 outpatient (OP) visit at least 1 year prior to erenumab start to establish a 1-year period for assessing baseline characteristics. IP constipation events were identified with ICD-10-CM K59.0- in an emergency department (ED) or IP visit, and the 90-day incidence proportion (95% CI) was calculated.
Image:
Results
The study included 9,994 new erenumab users (87% female; mean age [standard deviation]: 46.6 (12.7) years). Fifty-five IP constipation events were identified (incidence: 0.6%, 95% confidence interval [CI]: 0.4–0.7%). The incidence was 0.6% (95% CI:0.4–0.8%) in females, 0.3% (95% CI:0.1–0.8%) in males, 0.5% (95% CI:0.4–0.7%) in patients 18–64 years, and 1.0% (95% CI:0.5–2.0%) in patients ≥65 years. In patients with prescription drug use to treat constipation during baseline, incidence was 2.7% (95% CI:1.6–4.6) and for over-the-counter drugs was 2.8% (95% CI:1.8–4.3). Incidence by select baseline characteristics ranged from 1.0% to 11.5% (Table).
Conclusion
The overall 90-day incidence of IP constipation among new erenumab users (0.6%) was similar to the rate observed in migraine patients in real-world settings. The incidence increased with older age and with baseline constipation factors. Further research on the incidence in non-erenumab users with migraine and older age or baseline constipation risk factors may be helpful to contextualize these findings.
Disclosure of Interest: V. Hoffman Conflict with: full-time employee of Optum and own shares/stock options in the parent company of Optum (United HealthGroup, Inc.), K. Gill Conflict with: Employment by Amgen Inc, along with Stock Options, C. Szekely Conflict with: Employment & Stock Ownership with Amgen Inc, G. Reznor Conflict with: full-time employee of Optum and own shares/stock options in the parent company of Optum (United HealthGroup, Inc.), S. Ezzy Conflict with: full-time employee of Optum, A. Park Conflict with: Employment & Stock Ownership with Amgen Inc, R. Urman Conflict with: Employment & Stock Ownership with Amgen Inc, R. Hernandez Conflict with: Employment & Stock Ownership with Amgen Inc, M. Navetta Conflict with: Employment & Stock Ownership with Amgen Inc, S. Lopez-Leon Conflict with: Employment by Novartis Inc. with Stock Options, D. Chou Conflict with: Employment & Stock Ownership with Amgen Inc, F. Xue Conflict with: Employment & Stock Ownership with Amgen Inc, F. Wang Conflict with: full-time employee of Optum and own shares/stock options in the parent company of Optum (United HealthGroup, Inc.)

Migraine – acute therapy
MTV20-OR-015
A LONG TERM, OPEN LABEL STUDY OF SAFETY AND TOLERABILITY OF PRECISION OLFACTORY DELIVERY OF DHE IN ACUTE MIGRAINE (STOP 301): CLINICAL RESULTS
Sheena Aurora1,*, Maria Jeleva1, Jasna Hocevar-Trnka1, John Hoekman1 and Stephen Shrewsbury1
1Impel NeuroPharma, Seattle, United States
Introduction
Migraine is a common neurological disease impacting at least 12% of the US population. Despite several recent approvals, high unmet need and patient dissatisfaction remains for early and sustained efficacy with reduced recurrence. Intravenous dihydroergotamine (DHE) mesylate has a rapid onset and sustained effect. Similar plasma levels of DHE from 20 minutes with INP104, a novel drug-device combination product that delivers DHE to the upper nasal space, using a Precision Olfactory Delivery (POD®) device have been reported.
Objectives
To report the long term safety, tolerability, patient acceptability and exploratory efficacy of INP104.
Methods
STOP 301 was a multicenter, open-label, 24-week study, with a subset extending treatment to 52-weeks; (NCT0355733). Patients completed a daily diary and a migraine diary with every attack during a 28-day screening (on “best usual care”) and then on treatment. Patients were allowed to self administer up to 3 doses/week of INP104 nasally with migraine attacks (1.45 mg). The primary safety focus was on change in nasal mucosa and olfactory function. Exploratory objectives included efficacy measures compared to best usual care, patient acceptability by a questionnaire (PAQ), and heathcare utilization and quality of life measures (MIDAS and HIT-6).
Results
360 patients entered the 24-week treatment period, with 185 and 354 patients in the Primary and Full Safety Sets (PSS and FSS) respectively, while 55 and 73 patients composed the respective 52-week data sets. 36.7% of patients reported AEs, with 6.8% of patients discontinuing due to AEs (FSS). No significant olfactory mucosal integrity issues or functional disturbance was found by upper nasal endoscopy, nasal related TEAEs, or University of Pennsylvania Smell Identification Test (UPSIT) scores. Most common TEAEs were nasal congestion (15.0%), nausea (6.8%), nasal discomfort and unpleasant taste (5.1% each) with all other TEAEs being reported by < 3%. There were no treatment related Serious AEs, cardiac TEAEs or deaths. 4,515 migraines were treated with INP104 over 24-weeks (FSS). Pain- and most bothersome symptom-freedom were reported by 33.1% and 49.1% of patients at 2 hours post-INP104 (Weeks 21–24, PSS) compared to 26.2% and 43.9% on best usual care at baseline, respectively. Sustained pain freedom through 24 hours was reported by 98.4% of patients (Weeks 21–24). The PAQ demonstrated that the majority of patients agreed or strongly agreed that INP104 was easy to use (∼84%) and preferred over current therapy (FSS).
Conclusion
INP104 provides well tolerated, rapid and effective symptom relief, predictably and consistently, without injection. No new safety signals were observed following delivery to the upper nasal space. These data suggest INP104 may be a promising acute treatment for patients suffering from migraine.
Migraine – acute therapy
MTV20-OR-016
UBROGEPANT IS EFFECTIVE IN THE ACUTE TREATMENT OF MIGRAINE WITH MILD PAIN
Richard B. Lipton1,*, David W. Dodick2, Peter J. Goadsby3, Rami Burstein4, Aubrey M. Adams5, Jeff Lai6, Sung Y. Yu6, Michelle Finnegan6 and Joel M. Trugman6
1Albert Einstein College of Medicine and Montefiore Headache Center, Bronx
2Mayo Clinic, Phoenix, United States
3NIHR-Wellcome Trust King’s Clinical Research Facility, London, United Kingdom
4Havard Medical School, Beth Israel Deaconess Medical Center, Boston
5AbbVie Inc., Irvine
6AbbVie Inc., Madison, United States
Introduction
Ubrogepant, approved for the acute treatment of migraine in adults with/without aura, demonstrated efficacy in treating migraine with moderate/severe pain in two phase-3 trials. Clinical guidance recommends treatment of migraine when pain is mild, a strategy studied herein for ubrogepant.
Objectives
The goal of this analysis was to evaluate the efficacy of ubrogepant in the treatment of migraine with mild pain.
Methods
This was a phase-3, open-label, 52-week extension trial (NCT02873221). Adults with migraine with/without aura, randomized 1:1:1 to usual care, or in blinded fashion to ubrogepant-50mg or ubrogepant-100mg, were allowed to treat up to 8 migraine attacks of mild, moderate, or severe pain severity every 4 weeks. Efficacy measures included 2-hour pain freedom and absence of migraine-associated symptoms and were only collected for the ubrogepant treatment groups. Data were analyzed for the first treated attack and all treated attacks (averaged for each participant and then across participants, weighting individuals equally).
Results
Participants’ (n = 808) mean age was 42 years; most were white and female. This analysis includes data for 21,454 attacks treated during the trial. Pain free rates were higher for the treatment of mild pain than moderate/severe pain for ubrogepant 50 mg (39% vs 19%; p < 0.0001), and ubrogepant 100 mg (43% vs. 21%; p < 0.0001). Absence of photophobia was achieved in an average of 55% (both doses; p < 0.0001) of attacks treated with mild pain versus 34% (both doses) with moderate/severe pain. Absence of phonophobia was achieved in an average of 64% (ubrogepant-50 mg; p < 0.0001) and 70% (ubrogepant-100mg; p < 0.0001) of attacks treated with mild pain versus 42% (ubrogepant-50 mg) and 45% (ubrogepant-100 mg) with moderate/severe pain. Absence of nausea was achieved in an average of 83% (ubrogepant-50 mg; p < 0.0001) and 82% (ubrogepant-100 mg; p < 0.0001) of attacks treated with mild pain versus 67% (ubrogepant-50 mg) and 68% (ubrogepant-100 mg) with moderate/severe pain. First treated attack data trended similarly. Overall, 10% of participants reported treatment-related adverse events; one was considered serious (exacerbation of sinus tachycardia).
Conclusion
Treating migraine patients with ubrogepant when headaches are mild rather than moderate/severe increases the likelihood of rendering them free of pain and associated symptoms.
Migraine – acute therapy
MTV20-OR-017
RANDOMIZED, CONTROLLED TRIAL OF LASMIDITAN OVER FOUR MIGRAINE ATTACKS: CONSISTENCY FINDINGS
Messoud Ashina1,*, Judith Krikke-Workel2, John Krege2, Timothy SmithQun Lin2, Suzanne Klise2, Sonja Bragg2, Erin Doty2, Sherie Dowsett2 and Uwe Reuter3
1Danish Headache Center and Dept Neurology, University of Copenhagen, Copenhagen, Denmark
2ELI LILLY AND COMPANY, Indianapolis, United States
3Neurology, Charité-Universitätsmedizin Berlin, Berlin, Germany
Introduction
Lasmiditan (LTN) is a selective 5-HT1F receptor agonist for the acute treatment of migraine in adults.
Objectives
We present findings from the multicenter, placebo (PBO)-controlled, double-blind Phase 3 study, CENTURION, designed to assess the efficacy, including consistency of response, of lasmiditan for the acute treatment of migraine.
Methods
Patients were randomized 1:1:1 to lasmiditan 200 mg (LTN 200); LTN 100; or a control group which received PBO for 3 attacks and LTN 50 for either the 3rd or 4th attack. This modified parallel design enabled comparisons of the consistency for LTN vs PBO. Patients were asked to treat 4 migraine attacks, preferably consecutively. The primary endpoints were pain freedom at 2h (first attack) and pain freedom at 2h in ≥ 2/3 attacks. Statistical testing used a logistic regression model and graphical multiplicity methodology to preserve overall type I error. Here, we present the consistency findings for the intention-to-treat (ITT) population and a predefined subset of patients who were triptan insufficient responders (TIR).
Image:
Results
1613 patients were randomized, and 1471 (mean age 41 years; 84% female; 76% from Europe, 12% N. America, 12% Asia; MIDAS mean score 31.6) treated ≥1 migraine attack with study drug. All primary and gated secondary endpoints were met (active drug vs placebo comparisons all p < 0.001). Both LTN doses were significantly superior to PBO for pain freedom and pain relief at 2h in ≥2/3 attacks, for the ITT and TIR populations (table). The most frequent treatment emergent adverse events with LTN were dizziness, paresthesia, fatigue, nausea, vertigo, somnolence, hypoesthesia, muscle weakness, asthenia, and feeling abnormal; the incidence of TEAEs was highest during the 1st attack.
Conclusion
LTN was superior to PBO for all gated endpoints. Intra-patient consistency of response was superior with LTN compared with PBO, both overall and in the TIR subset.

Migraine – preventive therapy
MTV20-OR-018
ATOGEPANT SIGNIFICANTLY REDUCES MEAN MONTHLY MIGRAINE DAYS IN THE PHASE 3 TRIAL (ADVANCE) FOR THE PREVENTION OF MIGRAINE
Jessica Ailani1,*, Richard B. Lipton2, Peter J. Goadsby3, Hua Guo4, Rosa Miceli4, Lawrence Severt4, Michelle Finnegan4 and Joel M. Trugman4
1Georgetown University, Washington, DC
2Albert Einstein College of Medicine and Montefiore Headache Center, Bronx, United States
3NIHR-Wellcome Trust King’s Clinical Research Facility, London, United Kingdom
4AbbVie Inc., Madison, United States
Introduction
Atogepant is an oral, small molecule, calcitonin gene-related peptide receptor antagonist in development for the prevention of migraine.
Objectives
To evaluate the efficacy, safety, and tolerability of atogepant for the prevention of migraine.
Methods
Phase 3, multicenter, randomized, double-blind, placebo-controlled parallel-group trial (NCT03777059). Adults with 4 to 14 migraine days per month were randomized 1:1:1:1 to atogepant 10 mg, atogepant 30 mg, atogepant 60 mg, or placebo taken once daily for 12 weeks. The primary efficacy endpoint was a change from baseline in mean monthly migraine days (MMDs) across the 12-week treatment period. A key secondary endpoint was the proportion of participants with ≥50% reduction in their 3-month average of MMDs. Adverse events (AEs) were collected throughout the trial; severity and causality were assigned by the investigator.
Results
The trial included 910 randomized participants, 902 in the safety population, and 873 in the efficacy analysis population (modified intent-to-treat population); >87% of participants completed the double-blind treatment period across all treatment groups. Participants were on average 42 years old, 89% female, and 83% white, with a mean BMI of 31 kg/m2. Mean change from baseline in MMDs were −3.69 atogepant 10 mg, −3.86 atogepant 30 mg, −4.20 atogepant 60 mg versus −2.48 placebo (p < 0.0001 all dose groups). The percentage of participants who achieved a ≥50% reduction in their 3-month average of MMDs were 56% atogepant 10 mg, 59% atogepant 30 mg, 61% atogepant 60 mg versus 29% placebo (p < 0.0001 all dose groups). AEs were reported by 52%>54% of participants in atogepant treatment groups and 57% in the placebo group. The most commonly reported AEs were constipation (7%>8% across doses vs 0.5% placebo) and nausea (4%>6% across doses vs 2% placebo); none were considered serious. Serious AEs were reported by 0.9% in both atogepant 10 mg and placebo groups; none were reported for 30 mg or 60 mg. Discontinuations due to AEs were 2%>4% in atogepant groups, and 3% in placebo. No hepatic safety issues were identified following daily dosing with atogepant.
Conclusion
Atogepant provided statistically significant and clinically meaningful reductions in migraine days in the ADVANCE trial. Atogepant was safe and well-tolerated.
Migraine – preventive therapy
MTV20-OR-019
INTERICTAL BURDEN OF MIGRAINE: CORRELATIONS WITH OTHER MEASURES OF MIGRAINE BURDEN AND EFFECTS OF GALCANEZUMAB MIGRAINE-PREVENTIVE TREATMENT
Holland Detke1, Dawn Buse2,*, Janet Ford1, Austin Hand3, Jakub Jedynak1, Richard Lipton4, Martha Port1 and Claire Sandoe5
1Eli Lilly and Company, Indianapolis
2Albert Einstein College of Medicine, Bronx
3IQVIA, Durham
4Albert Einstein College of Medicine, Bronx, United States
5Centre for Headache/Neurology, Women’s College Hospital, Toronto, Canada
Introduction
Typical migraine clinical trial endpoints assess only ictal burden.
Objectives
Assess the nature of interictal burden in migraine, and whether treatment with galcanezumab (GMB) can reduce it?
Methods
Correlation of baseline MIBS-4 score with those of other baseline measures

*Absolute value of rho for Spearman’s correlation coefficient
Abbreviations: GAD-7=Generalized Anxiety Disorder Scale; MIBS-4=Migraine Interictal Burden Scale-4; MIDAS=Migraine Disability Assessment; MSQ=Migraine-Specific Quality of Life Questionnaire v.2;
PGI-S= Patient Global Impression of Severity; PHQ-9= Patient Health Questionaire-9.
Results
At baseline, MIBS-4 was moderately correlated with PHQ-9 (r = .55) and MSQ total (r = −.53) but showed low correlation (|r| = .3 to < .5) with GAD-7, MIDAS, and PGI-S, and negligible correlation (|r| < .3) with monthly migraine headache days.
After 3 months, from a mean baseline of 13.2 monthly migraine headache days, GMB patients improved by 4.4 days vs 1.3 days for PBO (p < .0001). From mean baseline MIBS-4 score of 5.5, GMB patients improved by 1.8 points vs 0.8 points for PBO (p < .0001).
Conclusion
In addition to reducing ictal burden, GMB treatment significantly reduces interictal burden of migraine as measured by MIBS-4. The lack of strong correlation between MIBS-4 and other trial outcomes supports previous validation work and suggests that interictal burden in migraine is a distinct effect of the disease that is not fully captured by other constructs.