
Abstract
Background
Definitions of medication overuse headache have changed over time.
Objective
To evaluate the clinical characteristics of medication overuse headache patients admitted for inpatient withdrawal therapy over a period of 32 years.
Methods
We included all patients with medication overuse headache treated from 1 January 1984 to 31 December 2015. We obtained all data from the medical reports and defined three periods, P1 (1984–1993), P2 (1994–2003), and P3 (2004–2015). The p-value adjusted for multiple comparisons was set to 0.005.
Results
Within 32 years, a total of 787 patients accounted for 904 admissions for MOH. From P1 to P3, the proportion of patients with preexisting migraine increased from 44.3% to 53.3% (chi2 = 9.0, p = 0.01) and that with preexisting tension-type headache decreased from 47.9% to 34.6% (chi2 = 9.3, p < 0.01). The median time since onset of headache and medication overuse headache decreased from 20 to 15 years (p < 0.001) and from 3 to 2 years (p < 0.001). The median cumulative number of single doses decreased from 120 to 90 per month (p = 0.002). Overuse of triptans, non-opioid analgesics, and opioids increased, whereas overuse of ergotamines decreased over time (p < 0.001 for all tests). The use of prophylactic medication before admission increased from 8.3% to 29.9% (chi2 = 89.5, p < 0.001).
Conclusion
This retrospective study in a large number of patients with medication overuse headache admitted for inpatient withdrawal therapy over a period of 32 years shows a trend towards changes in the preexisting headache type, a decrease in the time since onset of headache and medication overuse headache, a decrease in the number of drug doses used per month, changes in the type of drugs overused, and an increase in, but still low rate, of prophylactic medication prior to admission.
Keywords
Introduction
Medication overuse headache (MOH) affects about 2% of the general population and is most commonly related to chronic migraine (CM) or chronic tension-type headache (TTH) (1). The first classification of headache disorders published in 1988 included “headache induced by chronic substance use or exposure” and differentiated “ergotamine-induced headache” and “analgesics abuse headache” (2). The diagnosis required daily intake of a substance for three or more months, a minimum monthly dose, headache on 15 or more days per month, and headache resolution within 1 month after withdrawal. The second edition of the International Classification of Headache Disorders (ICHD-2) published in 2004 (3) introduced the term “medication overuse headache”, did not define any minimum doses, set the cut-off for overuse at 15 days per month for simple analgesics and at 10 days for any medication over a period of 3 months, and required that headache both worsens during overuse and reverts to its previous pattern within 2 months after discontinuation of the overused medication. ICHD-2 (3) differentiated the overuse of ergotamines, triptans, analgesics, opioids, combination-medication overuse, other medication overuse, and probable MOH. Revised criteria published in 2006 discarded the requirement that headache improves after withdrawal (4) and allowed diagnosis of MOH immediately, not only after follow-up. In ICHD-3 beta (5), the requirement that headache worsens during overuse was also discarded, “analgesic-overuse headache” was replaced by “simple analgesic-overuse headache”, two further types of overuse; that is, overuse of multiple drug classes not individually overused and unverified overuse of multiple drug classes, were added, and probable MOH was discarded. In ICHD-3 (6), the criteria remained unchanged apart from replacing “simple analgesic-overuse headache” by “non-opioid-analgesic-overuse headache” and specifying that “all non-opioid analgesics are regarded as a single class”. Consequently, the use of more than one non-opioid analgesic with every single drug being used on less than 15 days per month is classified as non-opioid analgesic-overuse headache (6).
This change in definitions and the long tradition in the management of MOH at our clinic dating back to 1989 (7) prompted us to examine changes in the characteristics of patients admitted for inpatient treatment of MOH over a period of 32 years.
Methods
The study was approved by the ethics committee of the Medical University of Vienna. We screened the diagnoses at the discharge of all patients admitted to the Department of Neurology of the Medical University of Vienna from 1 January 1984 to 31 December 2015 and identified all subjects with a diagnosis of MOH or corresponding previously used terms such as “drug-abuse headache” or “drug-induced headache”. For assessing the change in the patients' characteristics over time, we defined three periods ranging from 1984–1993 (P1), 1994–2003 (P2), and 2004–2015 (P3). These periods were commensurate with each other and reflected the years before and just after the publication of ICHD-1 (2), the subsequent era of ICHD-1 (2), and the time of ICHD-2 (3) and ICHD-3 beta (5).
We gathered biographic data, smoking status, body mass index (BMI), the time since headache onset, the headache diagnoses, and the details of the use of acute and prophylactic medication from the medical reports. We recorded the use of dihydroergotamine, ergotamine mono- and combination- preparations, almotriptan, eletriptan, frovatriptan, naratriptan, rizatriptan, sumatriptan, zolmitriptan, acetylsalicylic acid, diclofenac, ibuprofen, dexibuprofen, ketoprofen, mefenaminic acid, metamizole, naproxen, paracetamol, other non-opioid mono-preparations, tramadol, other opioids, and combination analgesics. Following ICHD-3 (6), we categorized these drugs as ergotamines, triptans, non-opioid analgesics, opioids, and combination analgesics. Also, we recorded the use of benzodiazepines and other tranquilizers. For each drug, we recorded the number of single doses used per month and the number of days per month the drug was taken. Besides, we calculated cumulative doses for all drugs and in each drug category. We defined use and overuse for every single drug and every drug category according to ICHD-3 (6).
Statistics
We analyzed all data with SPSS for Windows 24.0. Categorial data are shown as numbers and percentages and continuous variables as means and standard deviations (SD) or medians, lower and upper quartiles (Q1, Q3). For comparing P1, P2, and P3, we used chi-square tests for categorical variables, t-tests for normally and Kruskal-Wallis tests for non-normally distributed variables. To adjust for multiple comparisons, Bonferroni correction was performed online using SISA online statistical analysis following the suggestions of Sankoh et al. (8). Considering correlations between the variables, the adjusted p-value was set to 0.005.
Results
Admissions
Screening the diagnoses at discharge revealed 1028 admissions for possible MOH. Reviewing the medical reports did not confirm a diagnosis of MOH in 124 admissions. Accordingly, we included 904 hospital admissions of 787 patients. The number of admissions was 192 in P1, 348 in P2, and 364 in P3. The vast majority of patients (n = 699, 88.8%) was admitted once, 68 patients (8.6%) were admitted twice, and 20 (2.6%) three to five times.
Biographic data
Biographic characteristics of 787 patients with MOH in P1 (1984–1993), P2 (1994–2003), and P3 (2004–2015). Data presented refer to the first admission.

BMI and smoking
Among all admissions, the BMI was 26.0 ± 5.4 (women: 25.7 ± 5.6, men: 27.0 ± 4.5) and the proportion of smokers was 41.1% (women: 39.3%, men: 47.8%). In P1, P2, and P3, there was neither difference for the BMI (25.1 ± 5.1, 26.2 ± 5.6, and 26.1 ± 5.2), nor for the proportion of smokers (45.1%, 39.7%, and 40.9%, chi2 = 1.2; p = 0.6).
Headache
Headache diagnoses in 904 admissions for MOH in P1 (1984–1993), P2 (1994–2003), and P3 (2004–2015).
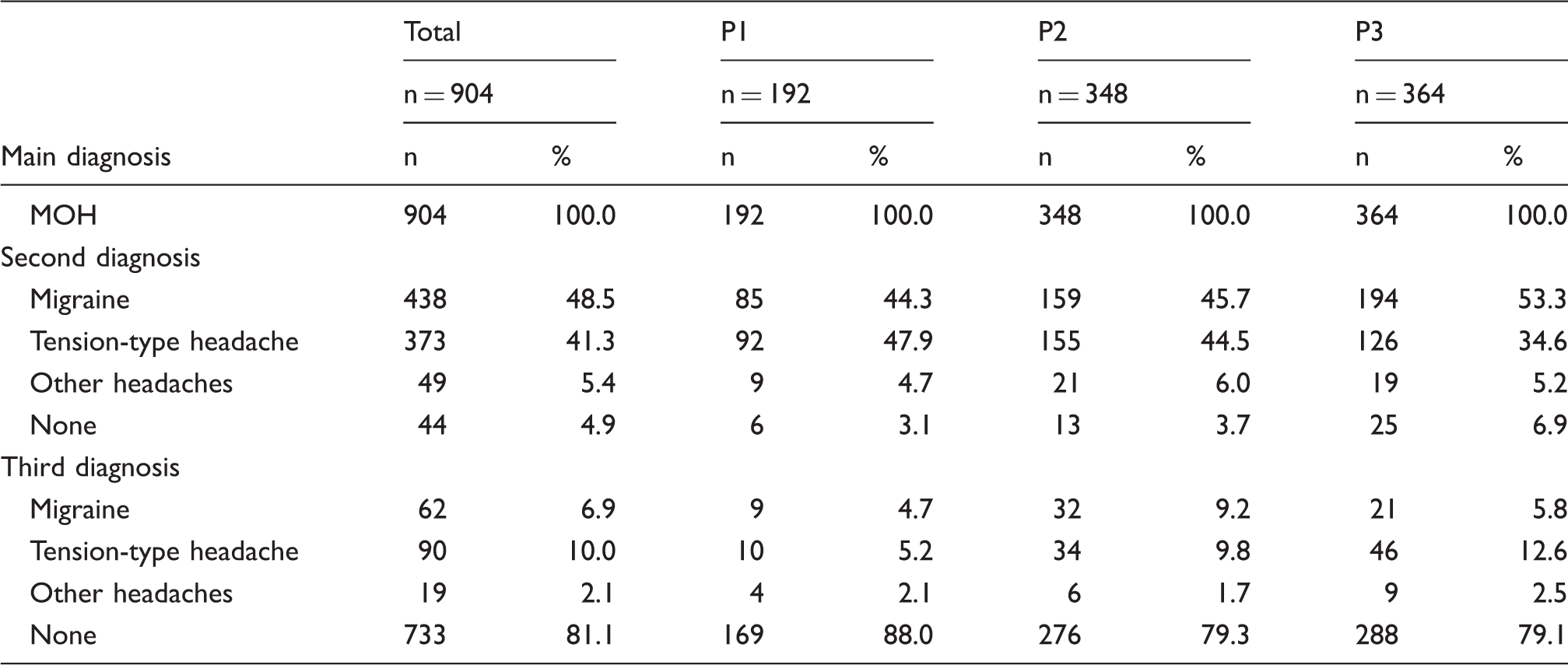
Among all admissions, the primary pre-existing headache was migraine, TTH, and other headaches in 48.2%, 41.7%, and 5.3%. From P1 to P3, the proportion of migraine increased from 44.3% to 53.3% (chi2 = 9.0, p = 0.01) and that of TTH decreased from 47.9% to 34.6% (chi2 = 9.3, p < 0.01). Both results did not remain statistically significant after correction for multiple testing.
Years since onset of the main pre-existing headache (i.e. second diagnosis in Table 2) and years since onset of MOH in 904 admissions for MOH in P1 (1984–1993), P2 (1994–2003), and P3 (2004–2015).

Kruskal Wallis Test.
Acute medication
Overuse of ergotamines, triptans, non-opioid analgesics, combination analgesics, and opioids was found in 27.9, 18.9, 45.6, 37.5, and 10.6% of the admissions. Overuse of two or more drug classes was present in 47%, whereas overuse of two or more drug classes not individually overused was rare (0.7%). The overuse of more than one non-opioid analgesic was mentioned in 13.5% of all medical reports and 28.2% of the reports referring to the use or overuse of non-opioid analgesics.
Medication overuse in 904 admissions for MOH in P1 (1984–1993), P2 (1994–2003), and P3 (2004–2015). Data are given for all drug classes and for the most common compounds within each class.
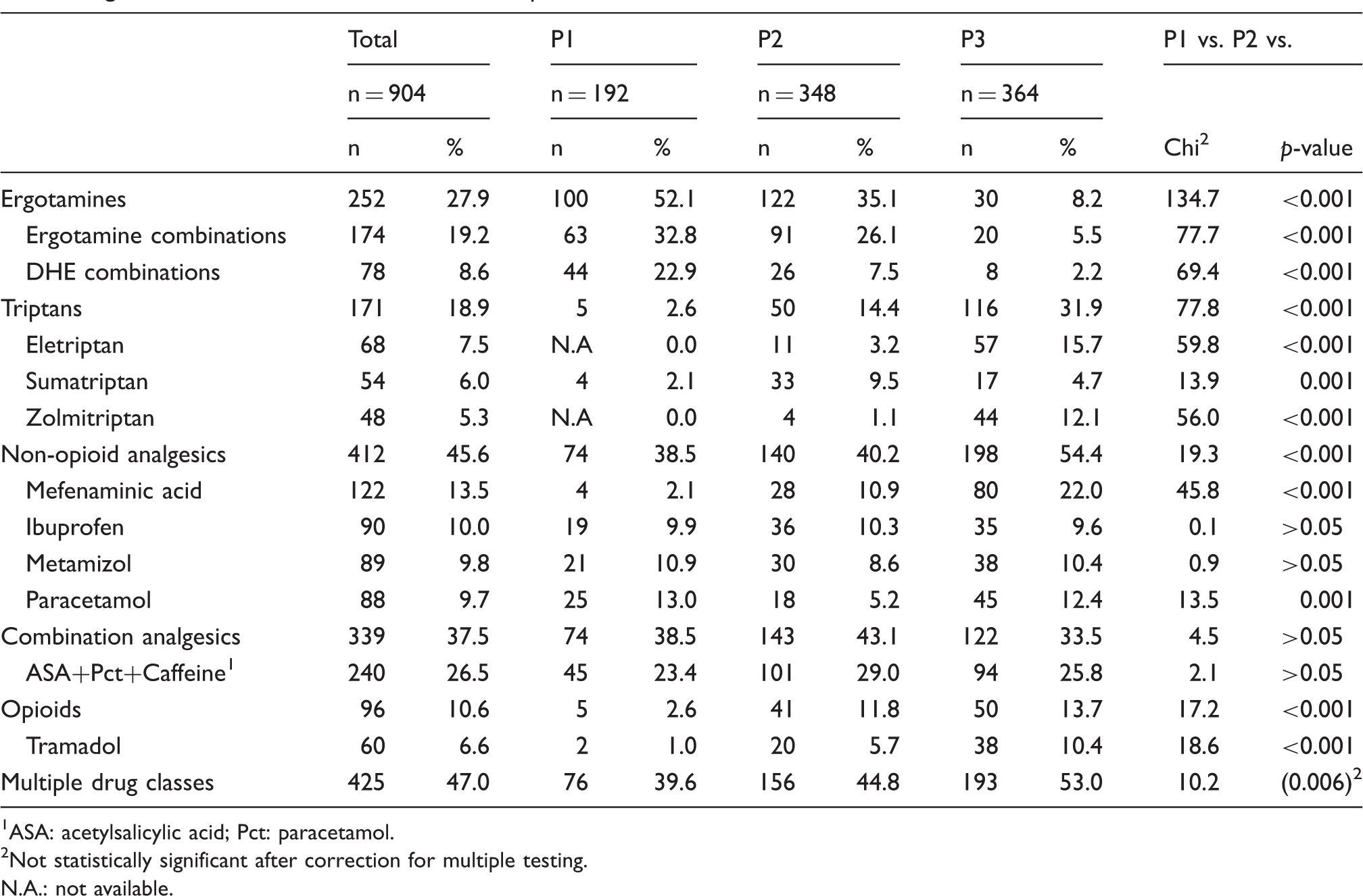
ASA: acetylsalicylic acid; Pct: paracetamol.
Not statistically significant after correction for multiple testing.
N.A.: not available.
Comparing medication overuse in patients with and without other pain disorders at the time of the first admission showed more frequent overuse of non-opioid analgesics (58.4% vs. 43.7%; chi2 = 8.6, p = 0.002) and a trend towards more frequent overuse of opioids (17.7% vs. 9.6%; chi2 = 86.8, p = 0.01), whereas overuse of triptans, ergotamines, and combination analgesics did not differ in the two groups.
Cumulative monthly single doses of 24 compounds or groups of compounds in five drug classes in 904 admissions for MOH in P1 (1984–1993), P2 (1994–2003), and P3 (2004–2015).
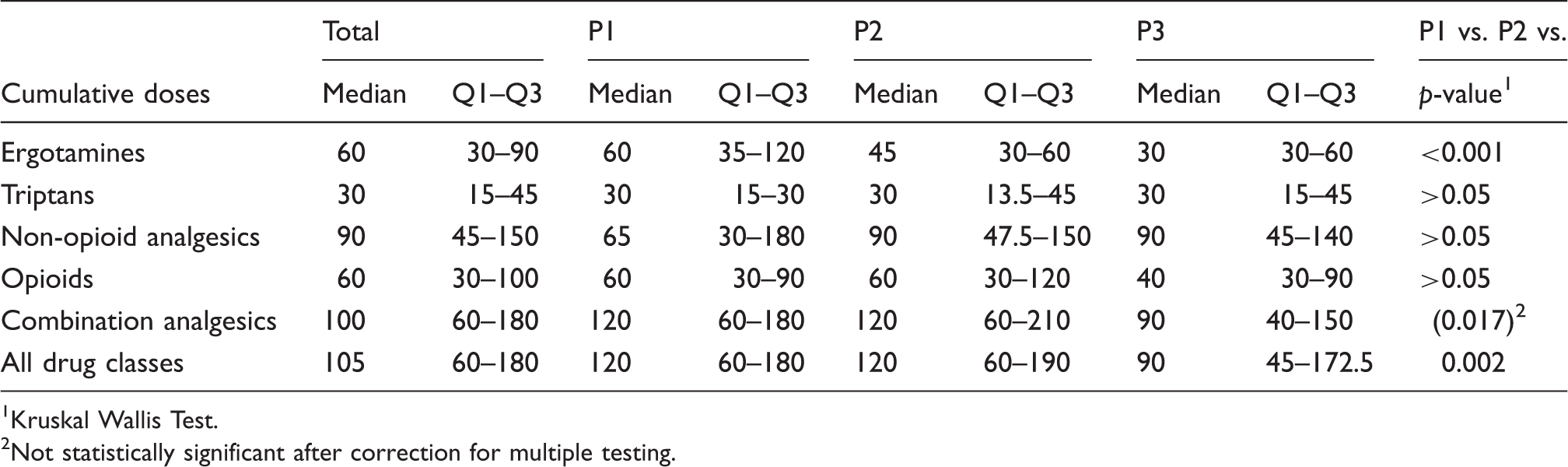
Kruskal Wallis Test.
Not statistically significant after correction for multiple testing.
Regular use of benzodiazepines and other tranquilizers was recorded in 7.2% of all admissions and was similar in the three study periods.
Prophylactic medication
Use of prophylactic headache medication prior to or at the time of admission in P1, 1984–1993), P2 (1994–2003), and P3 (2004–2015).

Besides, there was a marked increase in the use of other antidepressants. The prescription rate was 3.6% in P1, 13.2% in P2, and 34.9% in P3. In contrast, a diagnosis of depression or anxiety was similar in the three study periods and ranged between 31.3% and 33.5%. Antidepressants apart from amitriptyline were used more often in patients with depression/anxiety (36.9%) than in those without (11.6%), whereas the use of amitriptyline was similar in the two groups (10.8% vs. 7.8%).
Finally, the number of patients who had used more than one class of medication (including other antidepressants) increased markedly from 1.6% in P1, to 10.6% in P2, and 26.1% in P3.
Discussion
We retrospectively collected data of 787 patients with MOH, who accounted for a total of 904 admissions for inpatient detoxification over a period of 32 years. Thus, this represents one of the largest retrospective samples of MOH patients ever published covering a period of more than three decades. In 2004, Bigal et al. reported the characteristics of 456 patients with transformed migraine and compared patients treated in 1995 or before to those treated thereafter (9). Mesukunas et al. reported on 1200 patients with probable MOH from a tertiary headache center, but, unlike our study, diagnoses of MOH were based on ICHD-2 (10).
Biographic characteristics
The biographic characteristics were stable over a period of 32 years and similar to previously published data (10,11). Basically, MOH always was and still is a disorder mainly affecting middle-aged women with a long headache history.
BMI and smoking
While in the general population of Austria overweight (BMI 25–30) decreased over the last decades (12), the mean BMI was within the overweight range and did not change over time in our population. Several studies already showed an association between MOH and obesity (13–15). This association could be explained by central and peripheral pathophysiological mechanisms shared by migraine and obesity, whose emerging players are adipocytokines and a generally pro-inflammatory state (16). Notably, obesity was not the only unhealthy condition reported to be common in MOH. Obesity and daily smoking were associated with MOH independently and in combination (14).
The proportion of smokers in our study was higher than in the general population of Austria (12). Epidemiological studies have repeatedly shown an association between MOH and smoking (13–15,17). The question arises whether the high proportion of smokers among patients with MOH simply reflects a population prone to addictive behaviors, or if the association goes beyond that. Experimental data on capsaicin-induced pain highlight the role of nicotine deprivation resulting in increased pain sensitivity (18). Pain could, therefore, be a withdrawal-related symptom with deprivation-induced amplification of pain, thus leading patients to retain their smoking habits. However, these considerations are speculative, we could not find any data on the role of nicotine or nicotine withdrawal in MOH. Overall, harmful health behaviors seem to cumulate in MOH patients as well as in those with CM frequently associated with MOH (14).
Headache
The diagnostic category of the primary pre-existing headache tended to shift from TTH to migraine. This development may result from a growing awareness of migraine whereas TTH, even though the most common headache, fell behind. Previously published data already underlined the importance of migraine followed by TTH in MOH aetiology (1,19), but in our population, 20.1% of patients had a third or even fourth pre-existing additional headache type. We did not further classify these additional headache types and could not find any information in the literature regarding this MOH subclass with multiple pre-existing headache types.
The time since the first manifestation of both pre-existing headache and MOH decreased over time both in all patients and in non-triptan over-users, suggesting more awareness towards MOH and improved education of health care providers. However, considering that only a small minority of patients was ever advised to limit the intake frequency of acute headache medications (20), every effort has to be made to enhance educational work on MOH. Even though the debate is still going on about whether or not chronic headache can truly be induced by medication overuse, the perceived importance of MOH in Europe overcomes the importance observed in Northern America (21). Anyway, the European emphasis on MOH may not be completely wrong, considering that the uncritical use of opioids caused an epidemic in the US.
Treatment strategies shifted from an inpatient detoxification program as a standard- setting to outpatient programs. Nowadays, we offer inpatient detoxification preferably to those patients presenting with complicating factors such as co-morbid psychiatric disorders, opioid-overuse, or with difficult social conditions (22).
Acute medication
Interestingly, the median cumulative single doses continuously decreased over the past three decades. Usage of multiple over-the-counter medications, better information on possible side effects and complications, or the change in medication overuse pattern could partly explain this phenomenon. When analysed separately for substance classes, only the intake of median ergotamine single doses decreased.
While ergotamines were major players in migraine treatment in the past, they gradually lost their importance (9,13,23,24) owing to changes in European treatment guidelines (25). In parallel, triptan overuse significantly increased, reaching a proportion of up to 31% in our analysis. Several studies confirmed the importance of triptans in contemporary medication-overuse patterns (11,13,24). Triptan overuse headache typically develops faster and the amount of triptans needed to induce MOH is smaller than for analgesics (26). A survey based on nationwide healthcare claims data estimated that the proportion of migraine patients using a triptan was less than 6% in Austria and 5.9% of them were triptan over-users (27).
In a recent longitudinal study, triptan users showed high treatment efficacy and had better outcomes at one-year follow-up compared to those with poor acute treatment efficacy (as seen with non-opioid analgesics), who had an increased risk for new-onset CM (28). However, it remains speculative whether the early prescription of triptans to migraine patients could prevent chronification and overuse at least in those with high treatment efficacy. As triptan overuse generally becomes more frequent, the goal should be to identify patients with frequent migraine attacks, poor triptan response, and rebound headache to offer them timely prophylactic treatment, before overuse develops.
Non-opioid analgesics and combination analgesics were the top two drug classes overused in our study population, accounting for 45.6 and 37.5% of MOH, respectively. Both are main representatives of over-the-counter medications, often purchased without the need for prescription and thus easily available. Caffeine-containing substances in particular were blamed for inducing MOH (24), but in a population sample of adults with episodic and chronic daily headache their use was at least not associated with an increased risk of chronification in the adjusted analysis (29). According to epidemiological studies, almost all MOH patients purchased non-opioid analgesics and among patients from Europe and Latin America combination analgesics were frequently overused (11,23). The substance most frequently overused in our population, although not recommended in any guidelines, was mefenaminic acid followed by paracetamol, metamizole, and ibuprofen. The widespread use of mefenaminic acid seems to be specific for Austria, but we cannot provide an adequate explanation for this continuing popularity. In contrast, indomethacin and ibuprofen were most frequently overused in Italy (24). In Denmark, paracetamol and ibuprofen were among the most commonly purchased analgesics and the amounts purchased for MOH patients were four to 11-fold higher than the amounts dispensed to chronic headache patients without MOH (23,24). Differences in prescription habits, divergent insurance systems, and methodological issues could lead to this marked variation.
Overuse of multiple substance classes
More than half of the patients in our study reported the overuse of more than one substance class. Compared to this result the percentages reported in other studies were lower, ranging from 1.5–36.8% (9,11). This difference could relate to the fact that our study was conducted at a tertiary headache centre, whose patients were certainly severely affected. A possible relation between the MOH severity and overuse of multiple substance classes is supported by another study reporting this type of overuse in 50% of patients with previous withdrawal experience (24).
Notably, ICHD-3 beta (and ICHD-3) include criteria for overuse of multiple drug classes not individually overused, which was found in only 0.7% in our and 2.2% in another study, respectively (11). More information on this type of newly defined MOH is needed.
Opioids
In Europe, opioids are generally not recommended for headache treatment owing to their limited potential for relief from headache and their dependency potential (25,30). Therefore, it is surprising that the frequency of opioid overuse, expected to be no issue, varies from 1.5–33.3% (9,11,13,23), data not deriving solely from American studies, but rather also from Europe observing opioid overuse in up to 32% (23). Our current data show opioid overuse in 10.6% and, contradicting European treatment guidelines, it even increased over time and therefore well reflects the trend of non-critical opioid prescription for non-cancer pain (31). The question arises of why doctors would prescribe opioids to their headache patients. Maybe they are prescribed for other pain disorders in the first place, and then patients start self-administration to treat their headaches. Supporting this hypothesis, the overuse of opioids in our study tended to be more common in patients with other pain disorders than in those without. In a US-based survey, 17.7% of patients with chronic headache used opioids to treat not only a headache but also other pain conditions (29). An association of back pain, osteoarthritis, and rheumatoid arthritis with chronic migraine was also described in a Danish study (23), and in another recently published study MOH patients used analgesics for other pain conditions, muscle/joint pain and back pain in 23.9%, 22.6% and 21.5%, respectively (32). Besides, lacking familiarity with current treatment guidelines could contribute to generous opioid prescription policy. Also, the prescription of opioids together with antidepressants for co-morbid psychiatric disorders may be associated with the risk of serotonin toxicity (33). Educational campaigns warning of opioid-induced side effects may raise the awareness for uncritical opioid use.
Prophylactic treatment
A striking result of our study is the rare use of prophylactic medication prior to or at the time of admission. Prophylactic treatment was recorded in not more than 21% of the patients during the entire study period, though the proportion increased from 8% in P1 to (still low) 30% in P3. We wonder why the majority of our patients with a long headache history and alarming medication overuse did not receive prophylactic medication. Previously published data already described the under-treatment of CM and showed that prophylactic medication was rather the exception than the norm (9,20,34), raising concerns about insufficient treatment in primary care and neurological offices. Probably, physicians indeed do not recommend or inform patients about prophylactic medication or they do, but patients are not willing to take it. The monoclonal antibodies against calcitonin gene-related peptide could revolutionize prophylactic migraine treatment not only by enhancing acceptance and adherence but also by reducing the risk of medication overuse or by converting overuse to non-overuse (35).
Antidepressants
Many MOH patients suffer from co-morbid affective disorders whose presence is associated with poor treatment response and frequent relapse into MOH after detoxification (1,13,17,35). In the current analysis, the rate of affective disorders was similar in all three study periods. However, the usage of antidepressive treatment increased significantly from 4% in P1 to more than one third in P3. Considering this, affective disorders in patients with MOH obviously often remained untreated in earlier years.
Strengths and limitations
To the best of our knowledge, this is one of the largest clinic-based samples of consecutive MOH patients ever published. The study covers a period of more than three decades and reflects the evolution of MOH characteristics over time. The main limitations are the retrospective study design and the inclusion of inpatients from a tertiary headache centre, bearing the risk of a bias towards more severely affected patients. Accordingly, the results cannot be transferred to the general population.
Conclusion
This retrospective study in a large number of patients with MOH admitted for inpatient withdrawal therapy over a period of 32 years shows a trend towards changes in the preexisting headache type, a decrease in the time since onset of headache and MOH, a decrease in the number of drug doses used per month, changes in the type of the drugs overused and an increase in, but still low rate, of prophylactic medication prior to admission.
Footnotes
Public health relevance
This study highlights the evolution of medication overuse headache over a period of 32 years and represents one of the largest retrospective samples of MOH patients admitted for inpatient detoxification ever published.
The article clearly demonstrates the important role of triptans in contemporary medication overuse patterns.
Contradicting European treatment guidelines, opioid overuse in MOH patients increased over time. Therefore, every effort has to be made to reduce the intake of opioids in patients with chronic headache and non-cancer pain.
The low percentage of patients receiving prophylactic medication shows a still unmet need for more educational work on chronic migraine and MOH.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.