Epidemiology, comorbidity, outcomes and classification including big data
MTIS2018-146
CORRELATION OF MIGRAINE ATTACKS WITH EXCESSIVE YAWNING
E. A. MacGregor1,*, S. Donoghue2 and M. Vives-Mestres2
1Barts Health NHS Trust, London, United Kingdom
2Curelator Inc, Cambridge, MA, United States
Introduction: Repetitive yawning is a common premonitory migraine symptom [1,2]. In contrast to other common premonitory symptoms such as neck pain and tiredness, repetitive yawning is more specific and has a high predictive value for a migraine attack [3].
Objectives: We used a digital platform (Curelator Headache® – now called N1-Headache®) to determine 1) how many individuals recorded excessive yawning and 2) for how many individuals an association between excessive yawning and migraine attacks can be identified statistically.
Methods: Individuals with migraine registered to use Curelator Headache®. They then used this daily, entering details of headaches and factors possibly associated with attack occurrence: presence of yawning was determined by a Yes/No response to the daily question ‘Did you notice excessive yawning (today)?’. To be eligible for analysis, data must include 90 tracked days or more, at least five migraine attacks, more than 50 answers to the yawning question, and excessive yawning must be reported on at least 5% of days, but not all days. After 90 days all factors were analysed and for each individual the association between excessive yawning and migraine occurrence was determined via a univariate Cox proportional hazard model [4].
Results: Of 852 individuals with migraine, 285 (33.5%) were eligible for analysis. Excessive yawning was associated with increased risk of migraine attack in 72 (25.3%), with decreased risk in 4 (1.4%) and no significant within-person association was identified in 189 (66.3%). Risk could not be assessed in 20 (7%) due to convergence problems in the Cox model. Of the 72 with increased riskthe median hazard ratio was 3 (IQR = 4–2.2) meaning that, for them, when yawning is present the occurrence of migraine is about three times the rate per unit time as when there is no yawning.
Conclusion: In some individuals excessive yawning is a discernible symptom that is a sensitive predictor of migraine. Early identification of migraine provides an opportunity for early intervention. Future studies can assess effective strategies during the premonitory stage to abort an attack.
Disclosure of Interest: E. A. MacGregor Conflict with: Clinical Advisory Board Member, S. Donoghue Conflict with: Employee of Curelator Inc, M. Vives-Mestres Conflict with: Employee of Curelator Inc.
Epidemiology, comorbidity, outcomes and classification including big data
MTIS2018-147
EFFICACY OF THE THERAPEUTIC INTERVENTION IN HEADACHE UNITS IN PATIENTS WITH CHRONIC MIGRAINE. EFUNCE II STUDY
J. M. Láinez Andrés1,*, D. García López1, J. García Ull1, S. Santos Lasaosa2, A. López Bravo2, P. Pozo Rosich3, M. Torres Ferrus3, A. L. Guerrero Peral4, F. J. Viguera Romero5, R. Leira Muiño6, P. Irimia Sieira7 and A. Mínguez Olaondo7
5Complejo Hospitalario Virgen de la Macarena, Sevilla
6Hospital Clínico Universitario, Santiago de Compostela
7Clinica Universitaria de Navarra, Pamplona, Spain
Introduction: There is very few data in the literature confirming that the therapeutic intervention in headache units is superior to the attention received by patients in other levels of the health system. It is highly relevant to have these data to demonstrate the important role of these units in treating headache patients to patients themselves, health authorities and insurances companies.
Objectives: Evaluate the efficacy of the therapeutic intervention in headache units in headache patients and compare this intervention with other care levels as well as validate a protocol that could be applicable in the evaluation of headache units.
Methods: Multicenter prospective study performed in 7 university headache units in different regions of Spain. Every center should include 20 consecutive patients with chronic migraine that were referred to the headache unit for the first time. We evaluated the clinical situation, treatment received, paraclinical studies performed, degree of patients’ satisfaction, labor performance and disability (MIDAS) and quality of life (MSQOL and SF-12) studies. All these parameters were registered during the first consultation, after six months and one year later
Results: A total of 120 patients were included. 86% were women. Mean age was 46,5 ± 11.9 years. All of them fulfilled the criteria for chronic migraine (IHCD III- Beta version). The headaches had begun 19,1 ± 9,8 years before. Mean number of headache days in the last 3 months. 62,8 ± 21,2. Mean number of days using analgesics in the last 3 months. 51,9 ± 26,9. Mean age of migraine start 19.1 ± 9,8. 70% were referred by neurologist or other specialist. Patients were attended 3–4 times in the year of follow-up.
A significant reduction of number of days with headache, number of days of acute medication use, mean intensity of headaches, absenteeism and presenteeism, and use of health resources were observed. These clinical results were very related with improvement of quality of life (MAQOL and SF-12) and disability scales (mean MIDAS from 60 to 20). Only 28% of patients were satisfied or very satisfied at their arrival in comparison with 72% after attending the headache unit.
Conclusion: This study confirms that Headache Units are efficient in treatment of chronic migraine patients, being clearly superior to other assistance levels. They offer a high degree of clinical improvement, patient satisfaction and important benefits regarding labor performance, disability and quality of life.
Epidemiology, comorbidity, outcomes and classification including big data
MTIS2018-148
FACIAL PRESENTATIONS IN PRIMARY HEADACHE SYNDROMES
C. Ziegeler* and A. May
Introduction: Facial involvement of the first trigeminal branch (V1) is common in primary headache disorders; but the involvement of the second (V2) and third (V3) branches is relatively rare, and its prevalence in primary headache disorders is not well investigated.
Objectives: We aimed to assess the prevalence of facial presentations (the involvement of V2 and V3) amongst primary headache patients treated in a university tertiary care center.
Methods: For the time period of 2010–2018 medical records of patients of our university headache and facial pain out-patient clinic were retrospectively investigated for a facial involvement and divided into three subtypes depending on pain localization and history. Type I was defined as pain mainly experienced in V1 with an additional facial spread. Type II describes pain now perceived solely in V2 and/or V3 in patients with a history of headache in V1. Type III describes pain that is perceived in V2 and/or V3 without any prior history of headache.
Results: In our extended database we had n = 2,912 completed patient data sets of which 281 reported facial pain either as an independent or additional symptom. Among all migraine patients, 2.2% (n = 43 out of 1,935) reported a facial involvement, most commonly in V2. Of these 43 patients, 25 (58.1%) experienced pain in V1 radiating to V2 and/or V3 (Type I), whereas 18 patients (41.9%) experienced the pain exclusively or predominately in V2 and/or V3 (II, III). In cluster headache 14.8% (n = 42 out of 238) of the patients reported a facial involvement, of which 42.9% perceived the pain either exclusively or predominantly in V2 and/or V3 (II, III). A facial involvement was seen in 45.0% of paroxysmal hemicrania patients (n = 9 out of 20), 23.8% of hemicrania continua patients (n = 10 out of 42), and 20.0% of SUNCT/SUNA patients (n = 3 out of 15).
Conclusion: Facial presentations in primary head syndromes are not uncommon. A better understanding of the underlying mechanisms could potentially lead to a better understanding of primary headache syndromes in general.
Further research is needed to determine whether facial presentations in primary headaches represent a continuum of the same syndrome or indeed separate disease entities. We suggest subdividing these patients into the three above mentioned subtypes (Type I, II, III) to allow for a more homogenous definition of each group.
Epidemiology, comorbidity, outcomes and classification including big data
MTIS2018-149
VESTIBULAR ASSOCAITES IS MORE COMMON IN MIGRENEURS WITHOUT FAMILY HISTORY OF MIGRAINE
M. Bozdag1, N. Oksuz1, D. Derici Yildirim2, B. Tasdelen2 and A. Ozge 3,*
1Neurology, Mersın University, Mersın
2Biostatistics
3Neurology, Mersın University, Mersin, Turkey
Introduction: Vestibular signs and symptoms are often accompanied by other subgroups of migraine as well as vestibular migraine.
Objectives: The objective of this study was to evaluate the effect of family history on vestibular symptoms.
Methods: This study included patients with definitive migraine diagnosis who had complete knowledge of migraine and vestibular symptoms (vertigo, dizziness, motion sickness) through Mersin University School of Medicine, Neurology Department Headache database. Migraine was diagnosed by the same specialist according to ICDH-3 criteria. Those with similar headache complaints at the family were considered as family history positive. After audiologic and vestibulocochlear evaluations patients with other vestibular pathologies and patients diagnosed with other headache syndromes were excluded in this study. Symptoms such as dizziness, vertigo and motion sickness were questioned during headache and headache free periods. Headache frequency, duration and severity were assessed by monthly headache diary.
The Shapiro-Wilk test was performed to test the suitability of the normal distribution of the numerical data. Descriptive analyses were presented using median or mean ± SD based on distribution normally or not. Categorical variables were summarized as count(percentage). Unadjusted comparisons were made using Mann-Whitney U test for continuous endpoints and the Chi-Square test for categorical endpoints. A multiple logistic regression model was used to identify independent predictors of family history and migraine type. Odds ratios with their 95% confidence intervals were estimated. A p value of less than 0.05 was considered statistically significant.
Table:
Family History
P
Yes N (%)
No N (%)
Vertigo
Yes
67 (9.4)
29 (37.7)
<0.001
No
649 (87.9)
48 (62.3)
Dizziness
Yes
113 (15.8)
42 (53.2)
<0.001
No
603 (84.2)
36 (46.8)
Motion sickness
Yes
134 (18.7)
33 (43.4)
<0.001
No
581 (81.39)
43 (56.69)
Results: 793 patients were included in the study and 685 (86.4%) were female.
The mean age was 35.35 ± 12.73 years.
The median of headache duration as 24.0 [5–48] hours; headache frequency as 6.0 [3–15] days/month and headache severity as 8.0 [7–10] points according to VAS (visual analog scale) were detected.
Family history of migraine in 716 patients (90.3%), vertigo in 96 patients (12.1%), dizziness in 154 patients (19.4%) and motion sickness in 167 patients (21.1%) were determined.
There was a statistically significant relationship between vestibular assocaites and family history. (vertigo p < 0.001, dizziness p < 0.001, motion sickness p < 0.001).
Vestibular assocaites were more common in migreneurs without family history of migraine.
In migreneurs without family history, dizziness rate was 3.175 times (OR = 3,175, %95 GA 1,690–5,966, p < 0,001) and vertigo rate was 2.45 times higher (OR = 2,45, %95 GA 1,27–4,72, p < 0,001).
Conclusion: In our study, it was determined that family history of migraine did not have a significant effect on frequency and severity of migraine-accompanying vestibular symptoms.
Epidemiology, comorbidity, outcomes and classification including big data
MTIS2018-150
IDIOPATHIC INTRACRANIAL HYPERTENSION AND RISK OF CARDIOVASCULAR DISEASES IN WOMEN: UK POPULATION BASED MATCHED COHORT STUDY
K. Nirantharakumar1,2, A. Subramanian1, N. J. Adderley1, A. Yiangou3,4,*, K. M. Gokhale1, S. Mollan3,5, A. J. Sinclair3,4
1Institute of Applied Health Research, University of Birmingham
2Centre for Endocrinology, Diabetes and Metabolism, Birmingham Health Partners
3Metabolic Neurology, Institute of Metabolism and Systems Research, University of Birmingham
4Department of Neurology, University Hospitals Birmingham
5Birmingham Neuro-Ophthalmology, Queen Elizabeth Hospital, Birmingham, United Kingdom
Introduction: Cardiovascular disease risk has not been previously evaluated in idiopathic intracranial hypertension (IIH).
Objectives: To estimate risk of composite cardiovascular events, heart failure, ischaemic heart disease, stroke/transient ischaemic attack, hypertension, and type 2 diabetes in women with idiopathic intracranial hypertension compared to general population controls matched on body mass index and age. To evaluate prevalence and incidence of the condition.
Methods: A population-based retrospective cohort study was performed through The Health Improvement Network (THIN), a nationally representative electronic primary care records database between 01/01/1990, and 01/05/2016. Women with idiopathic intracranial hypertension (n = 2083) were compared to a control cohort (n = 18,439) matched for age, gender and body mass index. Adjusted hazard ratios of cardiovascular outcomes calculated using Cox regression. Primary outcome was a composite of any cardiovascular disease. Secondary outcomes included each of the cardiovascular disease outcome separately and type 2 diabetes, hypertension, fragility fractures, and death.
Results: Higher absolute risks for all cardiovascular outcomes were observed in idiopathic intracranial hypertension compared to controls. Idiopathic intracranial hypertension was positively associated with composite cardiovascular events (adjusted hazard ratio 2.19, 95% confidence interval 1.63 to 2.93, p < 0.001), heart failure (2.79, 1.51 to 5.15, p = 0.001), IHD (1.84, 1.16 to 2.91, p = 0.009), stroke or transient ischaemic attack (1.97, 1.33 to 2.92, p = 0.001), and hypertension (1.43, 1.18 to 1.75, p < 0.001). There were no statistically significant differences in type 2 diabetes, fracture and mortality rates. Both incidence and prevalence of IIH increased from 2005 to 2015: incidence from 2.5 to 6.7 per 100,000 person years and prevalence from 31 to 68 per 100,000 females. Incidence increased markedly in those with BMI > 30Kg/m2 and was highest in the most deprived Townsend quintile.
Conclusion: Idiopathic intracranial hypertension in women is associated with increased cardiovascular risk compared to a cohort matched for age, gender and body mass index. The absolute risk for this young population was low, but noteworthy considering the young age and relatively short study period. There is a growing burden of the disease, most marked in those with obesity. This data suggests that management of risk factors for cardiovascular disease may reduce long-term morbidity.
Disclosure of Interest: K. Nirantharakumar: None Declared, A. Subramanian: None Declared, N. Adderley Conflict with: National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) West Midlands, A. Yiangou: None Declared, K. Gokhale: None Declared, S. Mollan: None Declared, A. Sinclair Conflict with: NIHR Clinician Scientist Fellowship (NIHR-CS-011-028), Medical Research Council, UK (MR/K015184/1), Conflict with: IIHUK Charity (Registered Charity in England and Wales no 1143522 & Scotland SCO43294).
Epidemiology, comorbidity, outcomes and classification including big data
MTIS2018-151
TENSION-TYPE HEADACHE IN A MEXICAN POPULATION. RESUILTS FROM PREMECEF
A. Marfil* and S. Barrera-Barrera1
1Clinica De Cefaleas, Hospital Universitario, Uanl, Clinica De Cefaleas, UANL, Monterrey, Mexico
Introduction: Clinical presentation of most headaches is not well known in Mexican population.
Objectives: To communicate results from PREMECEF (Primer Registro Mexicano de Cefaleas, First Mexican Registry on Headaches) regarding tension-type headache (TTH).
Methods: PREMECEF is a database that works as an electronic medical record oriented to headaches. It is filled by physicians. It was launched in July, 2017 and currently has three regional hospitals participating, one private. Data collected to June 30, 2108 are presented.
Results: Of 485 records, 136 (28%) were TTH, with 104 (76.5%) female, median age 41.5 (SD 18.3) y/o; TTH subtypes, 93 (68.4%) were chronic, with initial frequency of 1 episode/d in 25 (18.4%), and the same current frequency in 26 (19.1%). Oppressive quality 83 (61%), duration 6–12 hours in 14 (10.3%), holocraneal in 20 (14.7%), occipital irradiation in 11 (8.1%), mainly afternoon in 10 (7.4%), prodrome in 12 (9.6%), accompanying symptoms in 80 (58.8%) with nausea: 31 (22.8%), vomiting, 18 (13.2%), phonophobia and photophobia in 17 (12.5%), kinesophobia in 11 (8.1%), allodynia in 5 (3.7%), dysautonomia in 11 (8.1%), triggers in 31 (22.8%). Sleep quality: sleep time 6–8 hours, 56 (41.2%), in 15 (11%) the sleep has good quality; 6 (4.4%) had bruxism.
Conclusion: TTH is the most frequent headache. Our figures show a higher than expected presence of accompanying and prodromal symptoms. Kinesophobia, allodynia and dysautonomias could be due to other, non-recognized, headaches. Poor sleep quality is highly prevalent.
TTH clinical profile in our simple has some characteristics that deserve further study. This is the first of its kind study in our country.
Experimental research
MTIS2018-153
ALTERATIONS IN REGIONAL CEREBRAL BLOOD (RCBF) IN VISUAL SNOW ASSESSED USING ARTERIAL SPIN-LABELLED (ASL) FUNCTIONAL MAGNETIC RESONANCE IMAGING (FMRI)
F. Puledda1,*, F. Zelaya2, C. Schankin3 and P. J. Goadsby1
1Basic and Clinical Neuroscience
2Centre for Neuroimaging Sciences, Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, United Kingdom
3Department of Neurology, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland
Introduction: Patients with visual snow suffer a pan-field, dynamic visual disturbance described as continuous TV-static-like tiny flickering dots. The proposed diagnostic criteria require at least two additional visual symptoms from: palinopsia (afterimages and trailing), entoptic phenomena (floaters, blue field entoptic phenomenon, photopsia, self-light of the eye), photophobia and nyctalopia (1). The only previous neuroimaging study in patients with visual snow showed hypermetabolism in the area of the lingual gyrus using [18]F-FDG PET (2).
Objectives: In order to understand more about the pathophysiology of visual snow and to confirm previous neuroimaging results, we aimed to measure the changes in regional cerebral blood flow (rCBF) in patients with this condition. We used a 3D pseudo-continuous arterial spin labeling (3D-pCASL) fMRI sequence, which was performed on a 3T General Electric MR750 MRI scanner.
Methods: These are preliminary results of an ongoing study. Subjects (n = 19) and age and gender matched healthy volunteers (n = 19) were recruited following screening and informed consent. All subjects underwent a structural T1, T2 and FLAIR sequences followed by two six minute pCASL scans. During the pCASL scans, subjects were instructed to either look at a blank screen (baseline sequence) or at a simulation of visual snow (stimulation) on the same screen. Scanning was conducted over 70 minutes in a single session. Imaging was analysed using SPM 12 (www.fil.ion.ac.uk/SPM).
Results: A full factorial analysis was conducted to compare the rCBF of patients to healthy volunteers, both at baseline and during visual stimulation. Using a whole brain, voxel-wise analysis we found that, at baseline, patients with visual snow exhibit a significant increase in rCBF in large clusters that include the left cerebellum, bilateral cuneus and precuneus and parts of the occipital and parietal cortices (p < 0.001). We also found that when subject to the visual snow stimulus, patients showed a significant increase in rCBF in the left cerebellum, left insula, left parietal and left occipital cortices (p < 0.001). No significant reductions in rCBF were detected.
Conclusion: Patients with visual snow present significant increase in blood flow in various brain regions, namely the cerebellum, cuneus, precuneus, insula, occipital and parietal cortices, both at baseline and when subject to a visual stimulus simulating the snow itself.
This study suggests that measures of regional CBF using ASL may provide a sensitive surrogate marker of differences in resting state neuronal activity, in subjects who experience visual snow syndrome. These results are consistent with those reported in previous investigations using Positron Emission Tomography.
References
SchankinCJManiyarFHDigreKBGoadsbyPJ. Visual snow- a disorder distinct from persistent migraine aura. Brain.2014; 137: 1419–28.SchankinCManiyarFSprengerTChouDEEllerMGoadsbyPJ. The Relation Between Migraine, Typical Migraine Aura and Visual Snow (TM). Headache2014; 54: 8–8.
Experimental research
MTIS2018-152
EMG- GUIDED BOTULINUM TOXIN A ALLEVIATES SEVERELY DISABLED HEADACHE PATIENTS WITH HYPERACTIVE MUSCLES. A DOUBLE- BLIND RANDOMIZED PLACEBO-CONTROLLED CROSS-OVER STUDY.
D. S. Knudsen* and H. Kasch
Introduction: In chronic refractory headaches a mixture of migraine with or without aura (MwoA) and tension-type headache (TTH), may often co-exist. Likewise, post-traumatic and post-whiplash headache (whiplash associated disorder, WAD) may have features of both TTH and MwoA. If Intense, persisting neck-tenderness/muscle stiffness and jaw-clenching/bruxism co-exist, these hyperactive muscles may be treated by botulinum toxin A (BTX-A).
Objectives: In chronic refractory headaches a mixture of migraine with or without aura (MwoA) and tension-type headache (TTH), may often co-exist. Likewise, post-traumatic and post-whiplash headache (whiplash associated disorder, WAD) may have features of both TTH and MwoA. If Intense, persisting neck-tenderness/muscle stiffness and jaw-clenching/bruxism co-exist, these hyperactive muscles may be treated by botulinum toxin A (BTX-A).
Methods: 59 consecutive chronic headache patients naïve to BTX-A treatment (Male:13; Female:46, age: 39.5 ± 11.2, mean VAS headache 6.9 ± 1.6; median duration 71.5mths) with hyperactive muscles. The diagnoses were: MwoA = 11; TTH = 25; PTH = 7; WAD = 15; other = 1.
Some of the patients with more than one diagnosis, were categorized by the main diagnosis.
EMG from the cervical, capital splenius and the semi spinal muscles was measured. If measures of turns/sec were above 250, patients otherwise fulfilling criteria for participation were randomized to either 75 units of Dysport® (conc: 200 u/ml) or a similar volume of isotonic saline in a double-blind cross-over study of 2 × 4 months periods.
Half of the patients were randomized to treatment with saline first and Dysport® second and the other half to treatment with Dysport® first and saline second, using a computer program called minimize.
Results: Treatment outcome was evaluated by the patient’s charts.
During active treatment 43% reported headache relief as compared to 21% during placebo (Kruskal Wallis(K-W), p < 0.009). During active treatment 19% had 2 months+ of 50% pain-relief. During active treatment significantly more complained about heaviness of the head, 48%, but no other Adverse events (AE's) were more common during active treatment. (K-W, p < 0.003). During placebo 4% reported heaviness of the head, 8% had flulike symptoms (7% in active treatment), 12% had muscle soreness (29% in active treatment) and 0% reported worsening of the headache (5% in active treatment).
Conclusion: Severely affected headache patients with hyper active muscles, may respond to low dosages of EMG guided BTX-A injections in the neck muscles. However more studies are necessary, before recommendations for clinical use can be made.
General aspects of headache care
MTIS2018-154
ORGANIZATION, MANAGEMENT AND TREATMENT OF IDIOPATHIS INTRACRANIAL HYPERTENSION (IIH) IN A TERTIARY HEADACHE CLINIC – HOW TO CHARACTERIZE AND IMPROVE PATIENT CARE.
M. Eriksen*
Introduction:
Background: Observations in the Pain- and Headache Clinic in Aarhus have led to questions about the patient care offered to patients diagnosed with IIH.
Objectives: Background: Observations in the Pain- and Headache Clinic in Aarhus have led to questions about the patient care offered to patients diagnosed with IIH.
Methods: Both quantitative and qualitative data were included in order to generate a broader insight and understanding into the answer in how to improve patient care to patients diagnosed with IIH. The medical records of 33 identified patients diagnosed with IIH and undergoing treatment at the Pain-and Headache Clinic during 2017 were investigated. Four persons were furthermore chosen systematically for a telephone interview. The investigation of the medical records was turned into statistical material and the telephone interview was coded and abstracted into categories and through a further abstraction into four key themes that seemed of importance to improvement of patientcare to patients diagnosed with IIH.
Table:
Analysis: By analysing the data, four key themes appeared. The four key themes were coordination, help to lose weight, better health care service and education/information.
Results: The four themes; Coordination, Help to Lose Weight, better Health Care Service and Education/Information appeared to be of importance to the patients in characterizing and improving patient care to patients diagnosed with IIH. In order to improve the present patient care, new strategies and a multidisciplinary approach need to be devised on the basis of the four themes. As the incidence of IIH is expected to rise in the future due to the obesity epidemic there is a developing need of centres with expertise in IIH involving organization, management, and treatment of IIH and continued and ongoing curiosity of development in the management, organisation and treatment are of importance in offering the best quality of patient care.
Conclusion: The four themes; Coordination, Help to Lose Weight, better Health Care Service and Education/Information appeared to be of importance to the patients in characterizing and improving patient care to patients diagnosed with IIH. In order to improve the present patient care, new strategies and a multidisciplinary approach need to be devised on the basis of the four themes. As the incidence of IIH is expected to rise in the future due to the obesity epidemic there is a developing need of centres with expertise in IIH involving organization, management, and treatment of IIH and continued and ongoing curiosity of development in the management, organisation and treatment are of importance in offering the best quality of patient care.
Keywords: Idiopathic intracranial hypertension, Pseudo tumour cerebri, Patient care, Treatment, Organisation, Compliance, Adherence, Management and IIH, qualitative analysis method.
General aspects of headache care
MTIS2018-155
GREATER OCCIPITAL NERVE BLOCKADE: AN EVALUATION OF 1577 INJECTIONS
M. Weatherall1,* and D. Vanniasegaram2
1Department of Neurology, Buckinghamshire Healthcare Trust, Aylesbury
2Imperial College School of Medicine, London, United Kingdom
Introduction: Greater occipital nerve blockade is widely used as a treatment for primary and secondary headache disorders. We performed a service evaluation of 1577 injections performed in 861 patients over a ten year period.
Objectives: The primary objective was to establish the safety and frequency of adverse events in a large cohort of patients, including a significant number who underwent repeated injections. Secondary objectives included recording patient-reported outcomes to provide real world data on the utility and consistency of the intervention.
Methods: A retrospective review of medical records was undertaken by the authors. Information was recorded on the age and sex of the patient, the main headache diagnosis, the location and quantity of materials injected, immediate complications, and if available, subsequent adverse events and patient-reported outcome (frequency and severity of headaches).
Results: Records of 1577 injections performed in 861 patients (662 F, 199 M) were identified. Immediate complications were recorded in 32 cases, most commonly syncope or near-syncope. 12 patients reported immediate symptoms in ipsilateral trigeminal territory, presumably mediated through activation of the trigeminocervical complex. Delayed effects were reported in 145 cases, mostly commonly persistent pain at the injection site. Serious side effects were rare: 4 cases of alopecia were recorded, one patient had a significant localised allergic reaction, and there was one case of central serous retinopathy closely temporally related to the injection. 20 injections were given to women whilst pregnant, and 30 whilst breast-feeding, with no significant adverse consequences. 21 patients had ≥7 injections; 2 of the cases of alopecia occurred in this group but there was otherwise no evidence of any cumulative risk of adverse events from repeated injections. Follow-up data was available for 733/861 first injections. 261 patients (36%) reported an excellent or good response, 184 (25%) a fair or minimal response, 256 (35%) no response, and 32 (4%) were worse. For those who responded, the median duration of effect was two months. 24/34 (71%) patients who did not respond to a first injection failed to respond to a second injection, or got worse. Conversely, 70/119 (59%) of those who reported a good response to the first injection, did as well or better with a second injection, although 32 of these patients (27%) did not respond second time around.
Conclusion: Greater occipital nerve blockade is a safe intervention for patients with primary and secondary headache disorders. Serious adverse events are very rare; with the possible exception of alopecia, repeated injections are not associated with higher risks of adverse effects. More than 50% of patients will derive some benefit from the intervention. Response to the first injection is a good guide to likely response to further injections.
General aspects of headache care
MTIS2018-156
NITRATES IN FOOD AS A RISK FACTOR FOR MIGRAINE ATTACKS
S. Donoghue1,*, M. Vives-Mestres1 and E. Virre2
1Curelator Inc., Cambridge MA
2Departments of Neurosciences, UCSD, La Jolla CA, United States
Introduction: Nitrates are used as preservatives in foods such as processed meats. High doses cause headaches and may trigger migraine attacks in susceptible individuals (1). However there is less evidence that nitrates consumed in food trigger migraine, but some indirect evidence (2). Nevertheless it is listed as a causative agent in ICHD-3beta. To explore whether daily variation in nitrate intake in food is associated with increased (or decreased) risk of having migraine attacks, we used a digital platform, Curelator Headache® (now called N1-Headache ®) to statistically compare, in individuals, daily intake of nitrates and occurrence of attacks.
Objectives: To determine in individuals with migraine 1) how many suspect nitrates as a migraine trigger and 2) for how many an association between nitrate intake and occurrence of migraine attacks can be identified statistically.
Methods: Individuals with migraine registered to use Curelator Headache via website or the App Store and answered questions about personal suspected triggers, including nitrates, and their importance (1 = low; 10 = maximal). They then used Curelator Headache® daily for 90 days, entering details about headaches and tracking factors that may affect migraine attack occurrence. After 90 days all factors were analyzed and, for each individual, the association between self-reported daily nitrate intake (none, some, a lot) and time to migraine attack was determined via a univariate Cox proportional hazard model.
Results: Table 1 shows statistical associations between nitrates and attack risk according to the degree of suspicion as a trigger in 774 individuals.
Nitrates was suspected as a trigger at baseline by almost half of individuals, mostly at the ‘low’ or ‘mildly’ suspected levels. Only a low number of associations were found therefore it was not possible to test the relation between degree of suspicion and the proportions of individuals with associations. Not analyzed individuals had insufficient data for analysis, due to constant or low variability in nitrates intake (404, 52.2%), low number of attacks or convergence problems in the Cox model.
Conclusion: Although often suspected as a trigger, nitrates in food are not a common trigger. In those individuals who suspect, positive (possible trigger) and negative (possible protector) associations were found in an almost equal and very small number of individuals. In one third of individuals intake of nitrates was reported as constant or with low variability making analysis impossible. For 20% of individuals intake was consistently reported as ‘none’, possibly indicating avoidance of nitrate-containing foods.
Disclosure of Interest: S. Donoghue Conflict with: Curelator Inc. Consultant, M. Vives-Mestres Conflict with: Curelator Inc. employee, E. Virre: None Declared.
PATIENTS WHO USE THE EMERGENCY DEPARTMENT FOR MIGRAINE: A STUDY OF ATTENDANCE AND TREATMENT CHARACTERISTICS
A.-M. Logan1,*, I. Reid2, M. Yogarajah, H. Jarman and N. Nirmalananthan
1St Georges University NHS Foundation Trust
2St George's Medical School, St George's University of London, London, United Kingdom
Introduction: Primary headache is a common cause of Emergency Department (ED) attendance [1] and a challenge for clinicians who need to distinguish primary from secondary headaches in a safe and timely way.
Objectives: In this retrospective cross sectional study of electronic records in a UK major urban Emergency Department we identified Migraine/ Probable Migraine (PM) from other primary headaches in order to establish how patients with migraine present and are managed in the acute setting.
Methods: Data was collected for all patients with available electronic records, triaged as attending for headache, aged 16 years and over, from 1st December 2016 to 30th April 2017 as part of a service evaluation study. The International Classification of Headache Disorders (ICHD) 3rd edition [2] was used to classify headaches using C, D and E criteria of the classification for Migraine/PM. Non primary headaches were classified based on ED/specialty diagnosis and inability to fulfil the ICHD criteria. Attendances were recorded during the study period as the Index Event and two years prior to this. Further analysis of the Migraine/PM group only was carried out to show attendance and treatment characteristics.
Image:
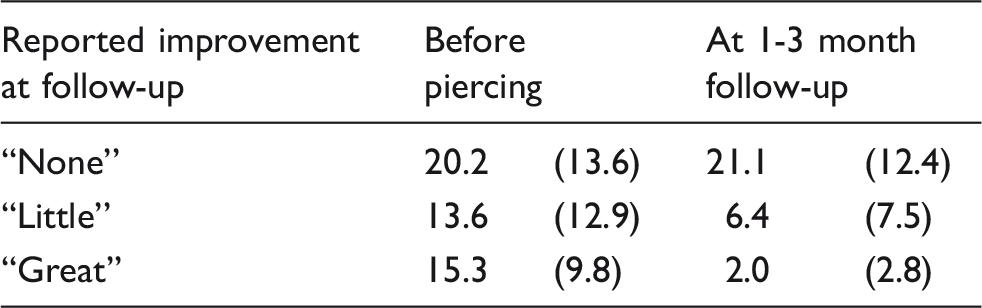
Results: Data was collected for 802 consecutive patients. 356 (46.5%) attendances were for non-primary headache, 196 (25.6%) for Migraine/PM and 213 (27.8%) for undefined headache due to lack of recorded headache features. 62 (31.6%) of Migraine/PM attendances and 67 (31.5%) undefined headache attendances resulted in brain imaging. 37(18.9%) in the Migraine/PM group were transported to ED by emergency vehicle. Timing analysis showed that 35% of attendances were acute, within 24 hours of the headache starting (Table 1).
59 (30.1%) of patients reported taking no treatment prior to ED attendance, 72 (36.7%) had used a low dose analgesic, 20 (10.2%) had used a triptan / analgesic combination and 20 (10.2%) an opiate preparation. In 49 (25%) of attendances treatment was not wanted / recorded, in 54 (27.6%) opiates were given. Triptans were used in 3 (1.5%) attendances.
Conclusion: This study shows how the ICHD classification [3] can be used to identify migraine in ED and highlights the frequent use of opiates [4] and scans [5] for migraine patients that has been seen acutely in other health systems. The proportion with undefined headache diagnoses adds weight to the calls for the use of a protocolised approach to headache management in ED [6, 7]. The use of emergency vehicles and the numbers of patients attending with non-acute symptoms may reflect the patient’s perception of the urgency of their need for headache care and warrants further investigation.
References
CerboR.et al.Primary headache in Emergency Department: prevalence, clinical features and therapeutical approach. J Headache Pain2005; 6(4): 287–9.Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia, 2018. 38(1): p. 1–211.FiesselerF.W.et al.Do ED patients with migraine headaches meet internationally accepted criteria?The American Journal of Emergency Medicine2002; 20(7): 618–623.McCarthyL.H.CowanR.P. Comparison of parenteral treatments of acute primary headache in a large academic emergency department cohort. Cephalalgia2015; 35(9): 807–15.Sahai-SrivastavaS.DesaiP.ZhengL. Analysis of headache management in a busy emergency room in the United States. Headache2008; 48(6): 931–8.MinenM.T.TanevK.FriedmanB.W. Evaluation and treatment of migraine in the emergency department: a review. Headache2014; 54(7): 1131–45.PariE.et al.Management of headache disorders in the Emergency Department setting. Neurological Sciences2015; 36(7): 1153–1160.
General aspects of headache care
MTIS2018-158
SELF-MANAGEMENT FOR PATIENTS WITH EPISODIC MIGRAINE: A PILOT OF COMMUNITY BASED GROUP EDUCATION SERVICE.
A.-M. Logan1,* and N. Nirmalananthan1
1Headache Service, Neurology Department, St George's University Hospitals NHS Foundation Trust, London, United Kingdom
Introduction: Self-management interventions have been shown to have a positive impact in patients with migraine [1]. Pressures on health services mean that new models of care are being sought, engaging patients in an active role in their migraine management.
Objectives: To assess the impact of a pilot community based group education service for patients with episodic migraine.
Methods: Episodic migraine patients were referred following a new hospital appointment to prevent further attendances or by their GP to prevent a hospital referral, to a 2 hour group session run by the Headache Practitioner. The session covered what migraine is, treatments, triggers, medication overuse, diaries, as well as living well with headache through advice on exercise, sleep and managing anxiety. Quantitative data of headache frequency, headache disability (HIT6) [2], diagnosis and referral was collected at the group with the HIT6 repeated at a subsequent telephone call. Qualitative data was recorded through a short questionnaire and comments recorded at the group and telephone call.
Image:
Results: 56 patients were referred, 82.1% were female, 17.9% male. 27 (48.2%) patients had high frequency migraine (HFEM) ≥ 8 migraine days per month, 21 (37.5%) patients had low frequency migraine (LFEM) on ≤7 migraine days per month, 2 (3.6%) patients had Chronic Migraine, 2 (3.6%) patients had Vestibular migraine and 4(7.1%) had unreported frequency. 37(66%) patients were hospital referrals and 19 (34%) GP referrals. 11 (57.9%) of GP referred patients had HFEM and 8(42.1%) had LFEM compared with 16 with HFEM (43.2%) and 13 with LFEM (35.1%) of hospital patients. 18 patients (32.1%) could be contacted 3 months after the session to complete outcome measures, of which 9(50%) were referred by GPs (table 1). For the whole group the HIT6 scores differed significantly between pre (mean 65.3, SD 4.37) and post (mean 59.6, SD 7.18) group, two tailed t = 2.89, df = 34, CI 95%1.7-9.75. The within person change was greater than the 2.5 points clinically relevant for the HIT6 [3]. Patients were asked immediately after the group to rate a statement saying that the session would help them manage their migraines more effectively. 48 (85.7%) of patient’s strongly agreed with the statement, 7(12.5%) agreed and 1(1.8%) did not respond.
Analysis of the comments showed important themes of attending with other migraine sufferers and how patients were able to implement changes as a result of the education through informed discussion with their GP or changes to lifestyle and medicines.
e.g. “It was very useful to make a working plan how to help myself to manage the migraines better”.
Conclusion: This pilot study of patients attending a self–management education group for episodic migraine experienced clinically meaningful reduction in disability and was highly rated for effectiveness by the patients who attended.
References
ProbynK.et al.Non-pharmacological self-management for people living with migraine or tension-type headache: a systematic review including analysis of intervention components. BMJ Open2017; 7(8): e016670–e016670.YangM.et al.Validation of the Headache Impact Test (HIT-6™) across episodic and chronic migraine. Cephalalgia2011; 31(3): 357–367.SmeltA.F.et al.What is a clinically relevant change on the HIT-6 questionnaire? An estimation in a primary-care population of migraine patients. Cephalalgia2014; 34(1): 29–36.
General aspects of headache care
MTIS2018-159
THE OPIOID USE IN TURKISH PATIENTS WITH EPISODIC AND CHRONIC MIGRAINE
D. H. Ertem1,*, I. Basarir1, G. B. Eryigit1, N. Kocabiyik1 and F. Ilik2
1Neurology, Sisli Hamidiye Etfal Training and Research Hospital, University of Health Sciences, Istanbul, Turkey., Istanbul
2Neurology, KTO Karatay University, Medicana Faculty of Medicine, konya, Turkey
Introduction: Despite the inadequate evidence of efficacy and safety of the use of opioids for treatment of migraine, it has been reported that patients with severe migraine headaches are prescribed for opioids for pain relief. Drug interactions, abuse, and tolerance are some disadvantages of opioid therapy in migraine. There are studies evaluating opiophobia, prejudice against the use of opioid analgesics by patients and physicians, and the use of opioids for the management of cancer pain in Turkey. However, the opioid use in Turkish migraineurs has not been well documented.
Objectives: The aim of this study was to assess the opioid therapy knowledge and use frequency among patients with episodic and chronic migraine.
Methods: In this prospective cohort study, we enrolled consecutive migraine patients in our headache clinic during the study period. The diagnosis of migraine was made according to the International Classification of Headache Disorders 3rd edition beta version. The socio-demographic and clinical characteristics were recorded for all patients. Furthermore, patients were asked about the knowledge and use of opioids for migraine headache pain.
Results: One hundred patients were enrolled, of which 69 were episodic migraine and 31 were chronic migraine. The mean age of patients was 41.41 ± 12.14, 82 % were female. The duration of migraine was 12.3 ± 10.37 years in episodic migraine and14.2 ± 9.2 years in chronic migraine. Eighty-eight per cent of patients with chronic migraine were treated with at least one preventive treatment. For acute migraine attack treatment, paracetamol, nonsteroidal anti-inflammatory drugs, triptans, and antiemetics were taken in frequency order. All subjects reported that any kind of opioids was not offered or prescribed by general practitioners and neurologists for their headache pain. Besides this, only 8 (8%) patients declared that they heard the use of opioids for the treatment of migraine but they never consulted their doctors.
Conclusion: Our results show that opioids are not preferred as an option for acute or preventive migraine treatment by Turkish migraineurs and their physicians.
References
Casucci G, Cevoli S. Controversies in migraine treatment: opioids should be avoided. Neurol Sci. 2013 May;34 Suppl 1:S125–8. doi: 10.1007/s10072-013-1395-8.ColakDOguzAYazilitasDImamogluIGAltinbasM. Morphine: patient knowledge and attitudes in the central anatolia part of Turkey. Asian Pac J Cancer Prev.2014; 15(12): 4983–8.Buse DC, Pearlman SH, Reed ML, Serrano D, Ng-Mak DS, Lipton RB. Opioid use and dependence among persons with migraine: results of the AMPP study. Headache. 2012 Jan;52(1):18–36. doi: 10.1111/j.1526-4610.2011.02050.x.Tepper SJ. Opioids should not be used in migraine. Headache. 2012 May;52 Suppl 1:30–4. doi: 10.1111/j.1526-4610.2012.02140.x.
General aspects of headache care
MTIS2018-160
SMARTPHONE OVERUSE AS A TRIGGER FACTOR FOR MIGRAINE ATTACKS
F. Ilik1, H. Buyukgol1, D. H. Ertem2,* and M. Uyar3
1Neurology, Karatay University, Medicana Faculty of Medicine, konya
2Neurology, Sisli Hamidiye Etfal Training and Research Hospital, University of Health Sciences, Istanbul
3Public Health, Necmettin Erbakan University Meram Faculty of Medicine, konya, Turkey
Introduction: Trigger factors for migraine attacks are usually identified such as hunger, dehydration, changes in weather, stress, hormonal changes, dietry factors, and bright light. The importance of the knowledge of trigger factors is that it can be helpful to predict migraine attacks and decrease the probability of an attack. It has been reported that high levels of screen time exposure are associated with migraine in young adults. Smartphone addiction has been defined as the overuse of smartphones to the extent that it disturbs the users’ daily lives.
Objectives: Some of our patients with migraine had reported that long and continuous smartphone use triggered their migraine attacks. In this study, we aimed to evaluate the impact of smartphone overuse on frequency and severity of attacks in patients with migraine without aura and to assess whether the use of excessive smartphone use could trigger migraine.
Methods: Three hundred and one consecutive newly diagnosed patients within normal physical and neurological examinations, who fulfil criteria of migraine without aura of The International Classification of Headache Disorders (2013 ICHD-III beta version), were enrolled in this study. Socio-demographical characteristics of patients were recorded. To evaluate the disability and severity of migraine, the Migraine Disability Assessment Questionnaire (MIDAS) and Visual Analogue Scale (VAS) were used. Smartphone overuse was assessed by smartphone addiction scale (SAS). Patients were assigned into two groups according to smartphone use: low smartphone users (median SAS score < 69) and high smartphone users (median SAS score ≥ 69). All the results were analysed by Statistical Package for the Social Sciences software version 22.0.
Results: Mean age of patients was 32.98 ± 6.19, 77.7 % were female. Mean duration of headache was 4.32 ± 3.15 years. The number of high smartphone users was 151 (50.16%). Among them, 60 high smartphone users (39.7%) reported that smartphone use was related to trigger their migraine attacks and 92.7% of these patients suffered from light sensitivity. Only 12 low smartphone users (8%) reported that smartphone use triggered their migraine attacks. The number of migraineurs whose attacks were triggered by smartphone use in high smartphone use group was significantly higher than the number of lower smartphone user group (p = 0.00). Moreover, VAS and MIDAS scores were significantly higher in patients using the smartphone more frequently than lower smartphone users (p = 0.01, p = 0.00, respectively).
Conclusion: Our results show that smartphone use is associated with migraine attacks. Patients with migraine without aura who were smartphone overusers had significantly higher pain intensity and disability scores. Our results support that smartphone overuse may be considered as a trigger factor for migraine attacks.
References
MontagniIGuichardECarpenetCTzourioCKurthT. Screen time exposure and reporting of headaches in young adults: A cross-sectional study. Cephalalgia.2016; 36(11): 1020–1027.DemirciSDemirciKAkgonulM. Headache in Smartphone Users: A Cross-Sectional Study. J Neurol Psychol.2016; 4(1): 5–5.
General aspects of headache care
MTIS2018-161
THE ASSOCIATION BETWEEN CHRONICITY OF MIGRAINE AND COMLEMENTARY AND ALTERNATIVE MEDICATION USE
D. H. Ertem1,*, I. Basarir1, G. B. Eryigit1, N. Kocabiyik1 and F. Ilik2
1Neurology, Sisli Hamidiye Etfal Training and Research Hospital, University of Health Sciences, Istanbul, Turkey., Istanbul
2Neurology, KTO Karatay University, Medicana Faculty of Medicine, konya, Turkey
Introduction: The term of Comlementary and Alternative Medication (CAM) is described by patients as all types of practices to prevent or treat illnesses which are not currently considered as a part of conventional medicine. Although the advance in medical and interventional treatment modalities for migraine, it is reported that some patients seek for CAM therapies due to their concerns about potential side effects of these therapies.
Objectives: We aimed to investigate the use of CAM therapies among patients with episodic and chronic migraine and to evaluate association between chronicity of migraine, demographic and clinical characteristics.
Methods: A questionnaire of a list of CAM modalities including traditional therapies specific to Turkish culture which was constructed by researchers through a literature review was given to all patients. Patterns of CAM treatment, patients` reluctance to share CAM use with their doctors were evaluated.
Results: One hundred patients were enrolled, of which 69 were episodic migraine and 31 were chronic migraine. The mean age of patients was 41.41 ± 12.14, 82 % were female. Twenty-four patients with chronic migraine had medication over use headache. Fifty patients reported that they had heard about CAM treatment for migraine and 36 of them had tried CAM at least once in their lives. Magnesium and Coenzyme Q10 pills (39%), hijama (blood drawing by local suction from small skin incisions) (%30.6), phytotherapy (medical herbalism, namely mint, sesame seed oil, black seed oil, rosemary) (%27.8), acupuncture (22%), vitamin supplements (22%), hypnose therapy (13.9%), and the others (massage, excercise, leeches, cupping, neural therapy, praying, amulet were used in frequency order. Homeopathic treatments were not used. Types of CAM use and number of patients did not differ between episodic and chronic migraine groups. There was no relationship between CAM use and medication overuse headache and demographic characteristics. However, duration of migraine and CAM use showed a moderate correlation regardless of chronicity (p = 0.017, r = 0.238).77.7 % of patients who used CAM stated that they preferred not to tell their physicians about CAM use if not asked and paid an average of 125.34 ± 213.28€ (range 0–874.12 €) for these treatments.
Conclusion: Our results show that both episodic and chronic migraineurs use different types of CAM modalities. CAM use is not related to chronicity of migraine and medication overused headache. Patterns of CAM treatment for migraine in Turkey differ from western practices. We observed that due to fear of disapproval, patients tended to hide CAM use from their doctors. Exploring the CAM use among migraineurs is essential for doctors regarding potential interactions and side effects of CAM therapies with conventional treatments.
References
Karakurum G, Coşkun O, Ucler S, et al. Complementary and alternative medicine by a sample of Turkish primary headache patients. Agri 2014;26:1–7.ZhangYDennisJALeachMJet al.Complementary and Alternative Medicine Use Among US Adults With Headache or Migraine:Results from the 2012 National Health Interview Survey. Headache.2017; 57(8): 1228–1242.
General aspects of headache care
MTIS2018-162
THE WORKLOAD, VALUE AND COMPLEXITY OF THE HEADACHE SPECIALIST NURSE
R. Bhola1,*, A. Bahra2 and P. J. Goadsby3
1NIHR-Wellcome Trust King’s Clinical Research Facility, King’s College Hospital, London
2Barts Health and The National Hospital for Neurology and Neurosurgery
3NIHR-Wellcome Trust King’s Clinical Research Facility, Kings College London, London, United Kingdom
Introduction: Due to its high prevalence and impact, headache is burdensome and costly to the sufferer, society and healthcare services. Multidisciplinary care is increasingly regarded as an efficient mode of service delivery (1). Professional nurses who have acquired the necessary education, skills and expertise increasingly meet patient needs in the UK. However, managing frequent and disabling primary headache, together with co-morbidities, present challenges and complexities.
Objectives: We aim to provide an overview of the workload, complexity and value of the specialist headache nurse.
Methods: We have evaluated patient needs within headache services and the service demands facing the team in practice. The broad aspects of the specialist nurse’s role, its complexity and the required skills will be illustrated.
Results: Our results will provide a representation of how complex care is delivered by the specialist nurse. These professional aspects will include: the nurse’s professional expertise in promoting patient safety, improving quality through audit and research (2), optimising the use of time and costs within the service, meeting the education needs of patients and others involved in patient care and treatment delivery e.g. ward based staff (3) and developing the service. A level of competence is achieved which is adapted to the needs of the organisation and service users and done within resource-constraints.
Conclusion: Patients in headache centres will typically present with complex needs and often co-morbidities. The specialist nurse has a key role within UK healthcare. To be effective and efficient the nurse will acquire the necessary education, skills and expertise to manage care and develop their services. The role of the specialist nurse could be extended with more nurses trained to provide the care and support for patients with headache between primary, secondary and tertiary care. Headache services can thus be optimised by the addition of specialist nurses, wherever they may be located in the world (4).
Disclosure of Interest: R. Bhola Conflict with: former clinical consultant with eNeura Inc; patent pending with eNeura for preventive treatment of migraine with sTMS., A. Bahra Conflict with: Advisory groups and satellite symposiums for Novartis., P. Goadsby Conflict with: declared for this meeting already, Conflict with: declared for this meeting already.
References
GaulCVisscherCMBholaRSorbiMGalliFRasmussenAJensenR. Team players against headache: Multidisciplinary treatment of primary headaches and medication overuse headache. J Headache Pain2011; 12: 511–519.Intravenous dihydroergotamine for inpatient management of refractory primary headaches. A Nagy, S Gandhi, R Bhola, PJ Goadsby. Neurology 2011; 77:1827–1832.Patient satisfaction with hospital management in a referral setting in the UK.Bhola R, Kaube H and Goadsby PJ. Cephalalgia 2004; 24: 1097.A trans-cultural comparison of the organisation of care at headache centres worldwide. R Bhola and PJ Goadsby. Cephalalgia. 2011;31:316–330.
Genetics and biomarkers of headache disorders
MTIS2018-163
RVCL-S, A HEREDITARY SMALL BLOOD VESSEL MODEL FOR MIGRAINE, STROKE AND VASCULAR DEMENTIA: SEARCHING FOR A PREDICTIVE BIOMARKER
I. De Boer1,*, N. Pelzer1, E. S. Hoogeveen2, S. R. Steenmeijer3, I. C. Notting3, H. A. Middelkoop1, M. C. Kruit2 and G. M. Terwindt1
1Neurology,
2Radiology,
3Ophthalmology, Leiden University Medical Center, Leiden, Netherlands
Introduction: Migraine, stroke and subsequent vascular dementia are the most prevalent neurological disorders causing disability at younger age (migraine) and severe disability and death at later age (stroke and dementia). New preventive therapies are urgently needed for these small vessel disorders. Retinal Vasculopathy with Cerebral Leukoencephalopathy and Systemic manifestations (RVCL-S) is an autosomal dominant neurovascular syndrome caused by mutations in the TREX1 gene for which no curative treatment is available. It manifests as a microangiopathy with retinopathy, migraine, stroke, and vascular dementia and serves as a monogenetic model for these common vascular disorders.
Objectives: We aim to find predictive biomarkers for disease progression in RVCL-S and to further dissect the disease mechanism by studying the natural history of the disease.
Methods: We are conducting a large follow up study on RVCL-S. Data from patients with a proven TREX1 mutation who participated in previous studies on RVCL-S in our centre (Terwindt et al, Brain 1998;Stam et al, Brain 2016) or visited our clinic for Cerebral Hereditary Angiopathies will be collected. This natural follow up will have a duration of at least 5 years. Mutation carriers will be assessed at least yearly, but based on clinical and radiological findings up to every 3 months, with a neurological, ophthalmological, and cognitive evaluation of disease activity, as well as a broad laboratory panel to assess systemic activity. Furthermore, non-invasive state of the art ophthalmological and radiological techniques will be used to study microcirculation in vivo.
Image:
Results: We aim to include 30 presymptomatic and 30 symptomatic patients in a our follow up study. Currently, n = 33 patients are included with follow up data for n = 21 patients (6 presymptomatic and 15 symptomatic, current follow up <= 4 years). Our first data show migraine without aura to occur at a relative late age and subcortical cognitive impairment in the domains of global and executive functioning at an early age. Imaging shows the known MRI described signs with impressive pseudo-tumours (figure 1) during the first years of follow up in n = 3 patients.
Conclusion: This is the first large prospective natural follow up study in RVCL-S. We aim to identify predictive biomarkers for RVCL-S, a monogenic model for common neurovascular disorders, such as migraine and stroke.
Disclosure of Interest: I. de Boer: None Declared, N. Pelzer: None Declared, E. Hoogeveen: None Declared, S. Steenmeijer: None Declared, I. Notting: None Declared, H. Middelkoop: None Declared, M. Kruit: None Declared, G. Terwindt Conflict with: independent support from Netherlands Organization for Scientific Research (NWO), European Community, the Dutch Heart Foundation, and the Dutch Brain Foundation.
References
Stam AH, et al. Retinal vasculopathy with cerebral leukoencephalopathy and systemic manifestations. Brain. 2016 Nov 1;139:2909–2922.Terwindt GM, et al. Clinical and genetic analysis of a large Dutch family with autosomal dominant vascular retinopathy, migraine and Raynaud's phenomenon. Brain. 1998 Feb;121:303–16.
Headache pathophysiology: basic science
MTIS2018-164
ENDOTHELIUM-DEPENDENT MICROVASCULAR VASODILATATION IN MIGRAINE/STROKE WOMEN: DEVELOPMENT OF A SEX-SPECIFIC METHOD
B. K. T. Zick1,2,*, K. M. Linstra1,2, J. Van den Berg1, E. E. Rubio-Beltrán1, J. H. J. Danser1, M. J. H. Wermer2, G. M. Terwindt2 and A. MaassenVanDenBrink1
1Division of Vascular Medicine and Pharmacology, Department of Internal Medicine, Erasmus University Medical Center, Rotterdam
2Department of Neurology, Leiden University Medical Centre, Leiden, Netherlands
Introduction: Migraine is associated with an increased risk of stroke, especially in women, possibly due to microvascular endothelial dysfunction. Recently, the assessment of microvascular endothelial function by measuring dermal blood flow (DBF) with laser Doppler perfusion imaging after local thermal hyperaemia (LTH), with and without iontophoretic administration of the nitric oxide synthase inhibitor L-NMMA, was validated in healthy men. In a large study aimed to identify female specific risk factors for cardiovascular disease with a special focus on migraine and stroke (CREW: CaRdiovascular hEalthy ageing in Women) we used this method in stroke/migraine women. However, ‘current-induced vasodilation’, an artefact caused by iontophoresis, was observed, inhibiting proper functional LTH assessment.
Objectives: The objective of the current study was to develop a more suitable protocol to reduce the current-induced vasodilation effect for assessment in women.
Methods: Different iontophoresis protocols were assessed in twelve young, healthy female subjects (18–40 years old). Current intensities were 40, 60 and 80 µA, during 15 min. Time to occurrence of current-induced vasodilation, which was defined as 200% of the baseline DBF values, was recorded. NO inhibition with the adjusted protocol was assessed. Based on these results, an adjusted protocol is now being validated in healthy, middle-aged (40-60 years old) female subjects.
Results: In 31 of the 36 measurements iontophoresis resulted in current-induced vasodilation. Time to current-induced vasodilation was not significantly different between the three different currents (p > 0.05). Based on the time until current-induced vasodilation, the protocol was adjusted from 15 to 7 min of iontophoresis, where 60 µA seemed to be the highest current possible with least subjects showing current-induced vasodilation. This adjusted protocol sufficiently inhibited NO-mediated vasodilation. Validation of the adjusted protocol in five healthy, middle-aged female subjects is being assessed and results will be presented at the congress.
Conclusion: The iontophoresis protocol using 60 µA during 7 min seems more reliable to assess NO-dependent DBF response during LTH than 100 µA during 15 min in women. Thus, the method for measuring microvasculature should be adapted when applied to women as sex-differences play a role in the mechanism of current-induced vasodilation.
Headache pathophysiology: basic science
MTIS2018-165
MODULATION OF THE TRIGEMINAL AUTONOMIC REFLEX BY NONINVASIVE VAGAL NERVE STIMULATION (NVNS): AN FMRI STUDY
M. Moeller1,*, C. F. Schroeder1 and A. May1
1Department of Systems Neuroscience, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Introduction: The trigeminal autonomic reflex plays an important role in trigeminal autonomic cephalalgias (TACs). Even though this reflex is quite well understood we still do not know which structures have a modulating effect on the reflex. Recent studies suggest that noninvasive vagal nerve stimulation is effective in cluster headache and further has an inhibitory effect on the trigeminal autonomic reflex. These findings suggest a modulating function of the vagal nerve. However, the mechanisms underlying this effect are still under debate.
Objectives: The aim of the present study was therefore to investigate the effect of nVNS on the reflex with a new high resolution fmri brain stem protocol.
Methods: All together 22 healthy participants (11 female, 11 male, mean age 25.64 ± 3.81) were included into the study, who were free from any headache or psychiatric diseases. The trigeminal autonomic reflex was activated by stimulation of the nasal mucosa with kinetic oscillation stimulation (KOS) during the fmri procedure. For KOS a balloon catheter with an inflatable tip was placed into the participants left nostril, which oscillated during stimulation (40 mbar/50 Hz). In general, this activates the reflex and leads to an increase in lacrimation.
A two-day within-subject design was used and the participants received either nVNS of the left cervical vagal nerve or sham stimulation of the left dorsal neck in a pseudorandomized order. For the fmri procedure each day consisted of 4 sessions, two sessions prior to the nVNS or sham and two sessions post stimulation. The fmri block design included 8 s of stimulation interleaved with 52 s of rest. For the general linear model analysis we performed a physiolological noise correction. In order to investigate the lower brain stem and the medulla we used a specific segmentation developed by Blaiotta and colleagues instead of the standard procedure for our SPM analysis.
Results: For the main effect we observed an increased bilateral activation of the insulae and the right SII area and a region in the right basal ganglia during intranasal stimulation (p < 0.001, uncorrected, minimum cluster extend of 10 voxel).
The comparison between nVNS and sham showed a decreased activation of brainstem networks including distinct nuclei at the level of the lower and mid pons after stimulation of the left cervical vagal nerve with nVNS during intranasal stimulation (p < 0.005, uncorrected, minimum cluster extend of 10 voxel).
Conclusion: In the present study we were able to replicate the results for the main effect from a previous study, where the same paradigm was used in order to activate the trigeminal autonomic reflex and to provoke lacrimation. Furthermore our preliminary data suggests an inhibitory effect on brain stem networks after nVNS. The inhibited regions are located in the region medial to the facial nerve in a region that could be interpreted as the superior salivatory nucleus, which is involved in the trigeminal autonomic reflex.
Disclosure of Interest: M. Moeller Conflict with: travel grant to the the american headache society 60th annual scientific meeting in san francisco by electrocore, Conflict with: talk at the electrocore industrial symposium at the american headache society 60th annual scientific meeting in san francisco, C. Schroeder Conflict with: none, Conflict with: none, A. May Conflict with: unrescricted scientific grant to the university medical center by electrocore.
Headache pathophysiology: clinical
MTIS2018-166
MIGRAINE AND CLUSTER HEADACHE CLASSIFICATION USING A SUPERVISED MACHINE LEARNING APPROACH: A MULTIMODAL MRI STUDY
R. Messina1,2,*, R. Leech3, F. Zelaya3, O. Dipasquale3, D. Wei4, M. Filippi2 and P. J. Goadsby4
1Headache Group, Department of Basic and Clinical Neuroscience, King’s College London, NIHR-Wellcome Trust King’s Clinical Research Facility, King’s College Hospital, London, London, United Kingdom
2Neuroimaging Research Unit, Institute of Experimental Neurology, Division of Neuroscience, San Raffaele Scientific Institute, Vita-Salute San Raffaele University, Milan, Italy
3Centre for Neuroimaging Science, Institute of Psychiatry, King’s College London
4Headache Group, Department of Basic and Clinical Neuroscience, King’s College London, NIHR-Wellcome Trust King’s Clinical Research Facility, King’s College Hospital, London, United Kingdom
Introduction: Neuroimaging studies have shown widespread structural and functional abnormalities in cortical and subcortical areas involved in multisensory processing, including pain, in migraine and cluster headache patients.
Objectives: The aim of our study was to identify a magnetic resonance imaging (MRI) pattern that best discriminate controls, migraine and cluster headache patients.
Methods: Functional, pulsed continuous arterial spin labelled and resting state (RS) functional MRI, and structural, diffusion tensor and 3D T1-weighted images, MR modalities were acquired from 20 migraineurs, 20 cluster headache patients and 15 controls. A dual regression analysis was used to study voxel-wise functional connectivity (FC) within brain regions involved in headache pathophysiology (thalamus, hypothalamus, dorsal pons and spinal trigeminal nucleus). Feature selection was performed using a probabilistic spatial independent components analysis. Support vector machine algorithms and a stepwise removal research were used to obtain the best accuracy rates for discrimination between patients and controls, and between patients.
Results: The overall accuracy for classifying the entire group of headache patients from controls was 82%. The best classification accuracy for discrimination between migraine and controls was 83%, and for cluster headache patients and controls it was 80%. The best classifier yielded an accuracy of 73% in distinguishing cluster headache patients from migraineurs. Distinct functional and structural MRI features contributed to the different classification models. The right thalamic RS FC was the most useful feature between headache and control groups. The right hypothalamic RS FC and the RS FC of the left pons had the highest feature importance when classifying migraineurs from controls. The right hypothalamic RS FC was also the most important MRI feature in migraine and cluster headache classification.
Conclusion: The combination of multiple functional and structural MRI patterns can accurately classify patients with primary headaches from a group of controls. Among the different brain networks involved in primary headaches, the thalamus, hypothalamus and pons play a central role in migraine and cluster headache pathophysiology.
Headache pathophysiology: clinical
MTIS2018-167
HIPPOCAMPAL VOLUME IS NORMAL IN CHRONIC MIGRAINE WITH MEDICATION OVERUSE
F. Riederer1,*, A. R. Gantenbein2, L. Michels3, S. Kollias3, C. Baumgartner1 and P. S. Sandor2
1Neurological Center Rosenhuegel and Karl Landsteiner Institute for Epilepsy Research and Cognitive Neurology, Vienna, Austria
2RehaClinic, Bad Zurzach
3Neuroradiology, University Hospital Zurich, Zurich, Switzerland
Introduction: In recent years temporal lobe structures have been suggested to be of importance in migraine pathophysiology. The hippocampus is considered to be involved in pain processing, pain-related anxiety and stress response. Studies on hippocampal volume in migraine have shown mixed results to date1.
Objectives: To investigate hippocampal volumes in patients with chronic migraine and medication overuse in comparison to a lare normal data base.
Methods: Hippocampal volumes of 58 patients with chronic migraine and medication overuse (42 women, mean age 43 ± 12 years) according to International Headache Society criteria were estimated based high resolution MRI of the brain and compared against a normal data base (58 matched controls, 42 women, mean age 42 ± 12 years, and controls from previous studies, in total N = 110)2
Results: Hippocampal volumes did not differ significantly between chronic migraine patients with medication overuse and healthy controls. Voxel-based analyses showed a small cluster of increased grey matter volume in the right hippocampus, not significant after correction for multiple comparisons. At an uncorrected threshold (p < 0.001), grey matter increases were found in regions including basal ganglia, hypothalamus, periaqueductal grey and cerebellum.
Conclusion: The present study does not support findings of volume change in the hippocampus in chronic migraine. Basal ganglia and periaqueductal grey matter abnormalities are in line with previous work3-5, changes in the hypothalamus merit further study.
References
LiuHYChouKHChenWT. Migraine and the Hippocampus. Current pain and headache reports2018; 22: 13–13.SchreglmannSRRiedererFGalovicMet al.Movement disorders in genetically confirmed mitochondrial disease and the putative role of the cerebellum. Movement disorders: official journal of the Movement Disorder Society2018; 33: 146–155.RiedererFGantenbeinARMartiMLuechingerRKolliasSSandorPS. Decrease of Gray Matter Volume in the Midbrain is Associated with Treatment Response in Medication-Overuse Headache: Possible Influence of Orbitofrontal Cortex. The Journal of neuroscience: the official journal of the Society for Neuroscience2013; 33: 15343–15349.RiedererFMartiMLuechingerRet al.Grey matter changes associated with medication-overuse headache: correlations with disease related disability and anxiety. The world journal of biological psychiatry: the official journal of the World Federation of Societies of Biological Psychiatry2012; 13: 517–525.NeebLBastianKVillringerKIsraelHReuterUFiebachJB. Structural Gray Matter Alterations in Chronic Migraine: Implications for a Progressive Disease?Headache2017; 57: 400–416.
Headache pathophysiology: clinical
MTIS2018-168
SELF-REPORTED PREVALENCE OF MIGRAINE TRIGGER FACTORS AND PATIENTS WILLINGNESS TO PARTICIPATE IN FUTURE TRIGGER RESEARCH
I. E. Verhagen1,2,*, G. L. J. Onderwater2, D. S. Van Casteren1,2, A. MaassenVanDenBrink1 and G. M. Terwindt2
1Division of Vascular Medicine and Pharmacology, Department of Internal Medicine, Erasmus University Medical Center, Rotterdam
2Department of Neurology, Leiden University Medical Center, Leiden, Netherlands
Introduction: Migraine is a multifactorial brain disorder characterised by recurring attacks of severe headache with neurological features. Exactly how attacks are initiated is unknown. Experimental administration of specific substances may provoke attacks. Many patients and physicians are convinced that attacks are provoked by external triggers such as food-items, alcohol, stress, and internal threshold-modulating factors such as hormones. However, evidence supporting this conviction is lacking.
Objectives: The aim of this study was to investigate the self-reported prevalence of several frequently reported migraine trigger factors and to assess patients willingness to participate in future research.
Methods: A survey concerning trigger factors in migraine was performed among 4032 migraine patients from the Leiden University Medical Centre Migraine Neuro Analysis programme (LUMINA) database. The prevalence of several frequently reported trigger factors was assessed. In addition, two separate groups of patients visiting our outpatient headache clinic were included. The first group comprised 53 male and female migraine patients who were asked about multiple trigger factors and willingness to participate in a prospective study. The second group included 48 female migraineurs who were asked about the influence of sex-hormonal changes on migraine and their willingness to participate in a clinical trial regarding hormonal treatment.
Results: In the LUMINA cohort 3785 patients (85% women) participated in the survey. Of these 38% had migraine with aura and 62% migraine without aura. The top three most reported trigger factors were stress (89%), followed by sleep deprivation (81%) and menstruation in women (78%). At our outpatient headache clinic 92% of male and female migraineurs indicated that more research needs to be performed addressing trigger factors in migraine, 64% was willing to participate in a trigger-diary study and 70% in a clinical trial. In the second group, 85% of women stated that the role of sex hormones in migraine should be further investigated, 77% of patients with sex-hormonal related migraine was willing to participate in a diary study and 58% in a clinical trial with hormonal treatment.
Conclusion: Stress, sleep deprivation and menstruation are the top three most patient-reported trigger factors in migraine. Our results indicate the need among migraine patients for research concerning trigger factors and they are promising when it comes to future inclusion of participants.
Migraine – acute therapy
MTIS2018-171
RIMEGEPANT 75 MG, AN ORAL CALCITONIN GENE-RELATED PEPTIDE ANTAGONIST, FOR THE ACUTE TREATMENT OF MIGRAINE: TWO PHASE 3, DOUBLE-BLIND, RANDOMIZED, PLACEBO-CONTROLLED TRIALS
R. B. Lipton1,*, V. Coric2, E. G. Stock2, D. A. Stock2, B. A. Morris2, T. J. McCormack2, M. Frost2, K. Gentile2, C. M. Jensen2, G. M. Dubowchik2, C. M. Conway2, R. Croop2 and P. J. Goadsby3
1Albert Einstein College of Medicine, New York
2Biohaven Pharmaceuticals, New Haven, United States
3NIHR-Wellcome Trust King’s Clinical Research Facility, King’s College London, United Kingdom
Introduction: A previous Phase 2 study of rimegepant — a novel, small molecule CGRP receptor antagonist — found that a 75 mg dose was safe and effective for the acute treatment of migraine.
Objectives: Herein we present the results of 2 methodologically identical Phase 3 studies comparing rimegepant 75 mg with placebo in the acute treatment of migraine.
Methods: Two double-blind, randomized, placebo-controlled, multicenter studies were conducted (Study 301, NCT03235479; Study 302, NCT03237845). Adults aged ≥18 years with ≥1-year history of ICHD 3-beta migraine could participate. Coprimary endpoints were pain freedom and freedom from the most bothersome symptom (MBS) at 2 h postdose. Subjects received rimegepant or matching placebo and treated a single migraine attack of at least moderate pain intensity. Secondary endpoints were tested using a prespecified hierarchical approach.
Results: In both studies more than 85% of subjects were women, the mean age was about 41 years, and subjects had ∼5 attacks per month. Rimegepant was superior to placebo at 2 h postdose for pain freedom, freedom from the MBS, and pain relief in both studies (P < .03). Durable efficacy versus placebo was also observed at later timepoints, including use of rescue medication within 24 h (301: 20.4% vs 31.8%; 302: 21.0% vs 37.0%); sustained pain freedom 2–48 h (301: 11.6% vs 7.2%; 302: 9.9% vs 6.0%); sustained pain relief 2–48 h (301: 33.7% vs 23.9%; 302: 36.3% vs 22.6%); and normal function at 2 h (301: 33.3% vs 21.8%; 302: 32.6% vs 23.4%). The overall safety of rimegepant was favorable and similar to placebo on tests of liver function.
Conclusion: In adults with migraine, a single 75 mg dose of rimegepant oral tablet was significantly more effective than placebo, with comparable safety. These findings complement the positive results seen in previous research.
Disclosure of Interest: R. Lipton Conflict with: receives grant support from the National Institutes of Health, the National Headache Foundation, and the Migraine Research Fund; serves as consultant, advisory board member, or has received honoraria from Alder, Allergan, American Headache Society, Biohaven Pharmaceuticals, Boston Scientific, Bristol Myers Squibb, Cognimed, Dr. Reddy’s Laboratories/Promius Pharma, Eli Lilly and Company, eNeura Therapeutics, Merck, Novartis, Pfizer, and Teva, Inc; holds stock options in Biohaven Pharmaceuticals and eNeura Therapeutics; receives royalties from Wolff’s Headache, 8th Edition., V. Coric Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals, E. Stock Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals, D. Stock Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., B. Morris Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., T. McCormack Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals, M. Frost Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals, K. Gentile Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals, C. Jensen Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., G. Dubowchik Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals, C. Conway Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals, R. Croop Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals, P. Goadsby Conflict with: personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities with Alder Biopharmaceuticals, Allergan, Amgen, Electrocore, Eli-Lilly, eNeura, Novartis, and Teva; personal compensation in an editorial capacity for Journal Watch, Up-to-Date, Oxford University Press, Massachusetts Medical Society, and Walters Kluwer; compensation for serving on the Board of Directors of Trigemina Inc.; research support from Amgen.
Abstract number: MTIS2018-171 Table:
301 (N = 1084)
302 (N = 1072)
Rimegepant n = 543
Placebo n = 541
P-value
Rimegepant n = 537
Placebo n = 535
P-value
2 h postdose (%):
Pain-free
19.2
14.2
.03
19.6
12.0
<.001
MBS-free
36.6
27.7
.002
37.6
25.2
<.001
Photophobia-free
34.9
24.8
<.001a
37.4
22.3
<.001d
Phonophobia-free
38.6
30.9
.03b
36.7
26.8
.004e
Pain relief
56.0
45.7
<.001
58.1
42.8
<.001
Nausea-free
46.9
41.6
.182c
48.1
43.3
.208f
aRimegepant n = 470 and placebo n = 483 bRimegepant n = 345 and placebo n = 366 cRimegepant n = 318 and placebo n = 322 dRimegepant n = 489 and placebo n = 477 eRimegepant n = 362 and placebo n = 374 fRimegepant n = 355 and placebo n = 336
Migraine – acute therapy
MTIS2018-169
DISABILITY IMPROVEMENTS OVER 12 MONTHS WITH LASMIDITAN FOR ACUTE TREATMENT OF MIGRAINE: INTERIM ANALYSIS OF MIGRAINE DISABILITY ASSESSMENT (MIDAS) SCALE CHANGES IN THE GLADIATOR STUDY
R. B. Lipton1,*, L. Lombard2, D. D. Ruff2, R. M. Nichols2 and J. H. Krege2
1Department of Neurology, Montefiore Headache Center, Albert Einstein College of Medicine, Bronx, NY
2Eli Lilly and Company, Indianapolis, IN, United States
Introduction: Lasmiditan is a novel, selective 5-hydroxytyptamine1F receptor agonist under investigation for the acute treatment of migraine in adults. The Phase 3 studies SAMURAI (NCT02439320) and SPARTAN (NCT02605174) evaluated three doses of lasmiditan (50 mg [SPARTAN only], 100 mg and 200 mg). In comparison with placebo, all doses of lasmiditan showed significantly higher rates of freedom from pain two hours post dose. GLADIATOR (NCT02565186) is a prospective randomised open-label Phase 3 study to evaluate long-term intermittent use of lasmiditan for acute treatment of migraine.
Objectives: Interim analysis of the effects of lasmiditan on migraine disability assessed with the Migraine Disability Assessment (MIDAS) scale in GLADIATOR.
Methods: Patients eligible for SAMURAI or SPARTAN had at least moderate migraine disability (MIDAS score ≥11).1,2 Patients who completed these studies were offered participation in GLADIATOR with randomisation to lasmiditan 100 mg or lasmiditan 200 mg (1:1). Patients were to use lasmiditan as first treatment for each new migraine attack (with a second dose permitted between 2 and 24 hours for rescue or recurrence of migraine) for up to 12 months. The analysis is based on the MIDAS questionnaire administered at baseline and at months 3, 6, 9 and 12. MIDAS measures lost time due to migraine in days over 3 months in the domains of activity limitations at work, household work or family, social and leisure activity.3,4 MIDAS has demonstrated reliability and validity; scores correlate with clinical judgement on the need for medical care.3,4 This interim analysis includes patients with MIDAS data at baseline and post-baseline; changes were modelled using a mixed model repeated measures analysis.
Results: Total MIDAS scores are shown in Table 1. At baseline, patients randomised to lasmiditan 100 mg had a mean score of 29.4 and patients randomised to lasmiditan 200 mg had a mean score of 28.9. Improvements from baseline increased over time for both doses and were statistically significant at all timepoints. At 12 months, improvements in MIDAS score reached 12.5 for lasmiditan 100 mg and 12.2 for lasmiditan 200 mg. Mean days with headache in past 3 months decreased from 15.5 at baseline to 8.8 at 12 months and from 15.5 to 8.2 at 12 months (both P < 0.001) in the lasmiditan 100 mg and 200 mg groups, respectively. There were no significant differences between the lasmiditan doses.
Conclusion: In this uncontrolled, open-label study, patients randomised to lasmiditan 100 mg or lasmiditan 200 mg had, on average, severe migraine disability at baseline (mean MIDAS score 21+) and showed a large, clinically meaningful improvement over 12 months of treatment. Migraine disability and headache days improved over time with both doses. These results warrant further investigation in a controlled study.
Disclosure of Interest: R. Lipton Conflict with: RBL is the Edwin S. Lowe Professor of Neurology at the Albert Einstein College of Medicine in New York. He receives research support from the NIH: 2PO1 AG003949 (Program Director), 5U10 NS077308 (PI), RO1 NS082432 (Investigator), 1RF1 AG057531 (Site PI), RF1 AG054548 (Investigator), 1RO1 AG048642 (Investigator), R56 AG057548 (Investigator), K23 NS09610 (Mentor), K23AG049466 (Mentor), 1K01AG054700 (Mentor). He also receives support from the Migraine Research Foundation and the National Headache Foundation. He serves on the editorial board of Neurology, and is senior advisor to Headache, and associate editor to Cephalalgia. He has reviewed for the National Institute on Aging (NIA) and National Institute of Neurological Disorders and Stroke (NINDS), holds stock options in eNeura Therapeutics and Biohaven Holdings; serves as consultant, advisory board member, or has received honoraria from: American Academy of Neurology, Alder, Allergan, American Headache Society, Amgen, Autonomic Technologies, Avanir, Biohaven, Biovision, Boston Scientific, Dr. Reddy’s, Electrocore, Eli Lilly and Company, eNeura Therapeutics, GlaxoSmithKline, Merck, Pernix, Pfizer, Supernus, Teva, Trigemina, Vector, Vedanta. He receives royalties from Wolff’s Headache 7th and 8th Edition, Oxford Press University, 2009, Wiley and Informa., L. Lombard Conflict with: Employee and minor shareholder of Eli Lilly and Company, D. Ruff Conflict with: Employee and minor shareholder of Eli Lilly and Company, R. Nichols Conflict with: Employee and minor shareholder of Eli Lilly and Company, J. Krege Conflict with: Employee and minor shareholder of Eli Lilly and Company.
MIDAS total scores in patients with baseline and post-baseline data randomised to lasmiditan 100 mg or lasmiditan 200 mg in GLADIATOR
Lasmiditan 100 mg
Lasmiditan 200 mg
Time of measurement
Mean MIDAS total score for 3 months preceding the assessment (SD)
Least squares mean change from baseline (SE)
Mean MIDAS total score for 3 months preceding the assessment (SD)
Least squares mean change from baseline (SE)
Baseline
29.4 (22.4) n = 972
—
28.9 (21.1) n = 1063
—
3 months
21.2 (20.4) n = 818
7.7* (0.7)
21.1 (21.7) n = 884
7.0* (0.7)
6 months
19.1 (20.2) n = 672
9.8* (0.7)
18.1 (19.5) n = 719
9.2* (0.7)
9 months
17.3 (17.0) n = 541
11.0* (0.9)
16.1 (21.4) n = 581
10.1* (0.8)
12 months
15.3 (16.1) n = 429
12.5* (0.9)
13.4 (18.1) n = 418
12.2* (0.8)
*P value < 0.001 vs baseline (mixed model for repeated measures) There were no significant differences between the lasmiditan doses MIDAS, Migraine Disability Assessment; SD, standard deviation; SE, standard error
References
Kucaet al.J Head and Face Pain2017; 57: 1311–2.Wietechaet al.Cephalalgia2017; 37(suppl): 367–8.Stewartet al.Neurology1999; 53: 988–94.Stewartet al.Neurology2001; 56: S20–8.
Migraine – acute therapy
MTIS2018-170
A PHASE 1 STUDY TO EVALUATE THE BIOEQUIVALENCE OF ORAL TABLET AND ORALLY DISSOLVING TABLET FORMULATIONS OF RIMEGEPANT, A SMALL MOLECULE CGRP RECEPTOR ANTAGONIST
R. Croop1,*, A. Ivans1, D. Stock1, J. Hould1, B. A. Morris1, J. Stringfellow1, C. M. Jensen1, J.-A. Moulin2, R. Larouche2, M. Tanguay2, V. Coric1 and R. B. Lipton3
1Biohaven Pharmaceuticals, New Haven, United States
2Syneos Health, Quebec, Canada
3Albert Einstein College of Medicine, New York, United States
Introduction: Rimegepant is an orally administered small molecule calcitonin gene-related peptide (CGRP) receptor antagonist in development for the acute treatment of migraine.
Objectives: This study compared the rate and extent of absorption of rimegepant Orally Dissolving Tablet (ODT) administered sublingually with rimegepant oral tablet in healthy fasted volunteers.
Methods: This was a single center, randomized, 4-period, 2-sequence, fully replicated, crossover bioequivalence study. Two treatments were given twice: 75 mg rimegepant ODT administered sublingually until fully dissolved then swallowed without water, and 75 mg rimegepant oral tablet swallowed with water. Eligible subjects included adult nonsmokers, aged 18 to 55 years, with BMI between 18.5 and 30.0 kg/m2 and weight of at least 50.0 kg for males and 45.0 kg for females. Pharmacokinetic parameters included Cmax, AUC0-t, AUC0-inf, and Tmax. The formulations were considered bioequivalent if, after analyses of primary pharmacokinetic endpoints Cmax, AUC0-t, and AUC0-inf, the 90% CIs for the ratio of geometric means for all 3 endpoints were within 80% to 125%.
Results: In total, 35 subjects were enrolled, and 34 (97.1%) completed the study. The population was 80% male and 80% White; and had a mean age of 37.7 years, BMI of 25.9 kg/m2 and weight of 76.6 kg. Statistical comparisons of the log-transformed Cmax, AUC0-t, and AUC0-inf of rimegepant ODT administered sublingually with rimegepant tablet showed that all 90% CIs of geometric mean ratios were within the predefined range of 80% to 125% for bioequivalence. Median Tmax was 1.5 hours for rimegepant ODT administered sublingually versus 2 hours for rimegepant oral tablet. A statistical comparison, using Proc Mixed, found the least-squares means (standard errors) for the ODT and tablet to be 1.48 (0.098) hours and 1.92 (0.163) hours, respectively. The difference in Tmax, 0.44 hours (26 minutes), was statistically significant (P = 0.0021). Adverse events (AEs) were reported by 17 subjects; 88.2% of these AEs were mild. One subject withdrew from the study due to a moderate AE of external otitis that was considered unrelated to treatment. No severe or serious AEs were reported.
Conclusion: Rimegepant ODT administered sublingually and rimegepant oral tablet were bioequivalent, and both formulations were well tolerated. The earlier Tmax seen with rimegepant ODT might result in an earlier onset of action for this fast dissolving formulation.
Disclosure of Interest: R. Croop Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals, A. Ivans Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., D. Stock Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., J. Hould Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., B. Morris Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., J. Stringfellow Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., C. Jensen Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., J.-A. Moulin Conflict with: Employed by Syneos Health., R. Larouche Conflict with: Employed by Syneos Health., M. Tanguay Conflict with: Employed by Syneos Health., V. Coric Conflict with: Employed by and holds stock/stock options in Biohaven Pharmaceuticals., R. Lipton Conflict with: receives grant support from the National Institutes of Health, the National Headache Foundation, and the Migraine Research Fund; serves as consultant, advisory board member, or has received honoraria from Alder, Allergan, American Headache Society, Biohaven Pharmaceuticals, Boston Scientific, Bristol Myers Squibb, Cognimed, Dr. Reddy’s Laboratories/Promius Pharma, Eli Lilly and Company, eNeura Therapeutics, Merck, Novartis, Pfizer, and Teva, Inc; holds stock options in Biohaven Pharmaceuticals and eNeura Therapeutics; receives royalties from Wolff’s Headache, 8th Edition.
Migraine – acute therapy
MTIS2018-172
ASSESSMENT OF MEDICATION OVERUSE HEADACHE (MOH) BY GENERAL PHYSICIANS, PHARMACISTS AND PHARMACY ASSISTANTS: AN INTERNET-BASED SURVEY
C. Gaul1,*, T. Weiser2 and H. Graeter2
1MIGRAINE AND HEADACHE CLINIC, Koenigstein im Taunus
2Medical Affairs. Sanofi, Frankfurt, Germany
Introduction: Tension-type headache and migraine are frequently treated with over-the-counter (OTC) analgesics like ibuprofen (IBU), paracetamol (PARA), acetylsalicylic acid (ASA) or the combination of PARA, ASA and caffeine (APC). The efficacy and safety of these drugs has been proven. However, overuse may result in medication overuse headache (MOH).
Objectives: The aim of this study was to collect data on health care providers’ understanding of MOH.
Methods: In June/July 2017, general physicians (n = 150), pharmacists (n = 151), and pharmacy assisstants (PAs) (n = 154) answered an internet-based survey on MOH performed by DocCheck Research, Köln, Germany. Herein we present the results on IBU, PARA, ASA and APC.
Results: 88% of the HCPs rated the topic MOH as very important. 34% of the participants thought that for IBU, PARA, or ASA the critical maximum duration of daily intake to avoid MOH is 2 weeks. This was estimated by 55% of the participants for APC. Moreover, 15% set the upper limit for the combination at 4 days. In total, the risk for MOH was estimated as … “very high” by 50% of the participants for the mono-analgesics compared to 86% for the combinations with caffeine.
Furthermore, the perceived benefit and risk for the various preparations varied greatly. For example, 53% of HCPs rated the efficacy of IBU in migraine as “very high/high”, 47% the tolerability and 27% the risk for MOH, for APC 21%, 15% and 64%, i.e. the benefits were assessed lower and the risks higher.
Conclusion: MOH was regarded as a very important topic by the interviewed HCPs. Interestingly, the risk of MOH was overestimated according to the criteria of the International Classification of Headache Disorders. Mono preparations were assessed differently compared to analgesics containing caffeine, although according to current scientific knowledge both do not have a different risk for MOH (Bigal et al, 2008). There were also discrepancies between the perceptions and current data of efficacy in migraine: APC was rated worse than IBU, although the superiority of the combination was shown in a comparative study and meta-analysis (Goldstein et al., 2006; Petersen, 2017). For the patients, an evidence-based assessment of the benefits and risks of acute pain analgesics for the treatment of tension-type headache and migraine would be desirable.
Disclosure of Interest: C. Gaul Conflict with: Consulting fees from Sanofi., T. Weiser Conflict with: Employee of Sanofi, H. Graeter Conflict with: Employee of Sanofi.
References
Bigal ME, Serrano D, Buse D, Scher A, Stewart WF, Lipton RB. Acute migraine medications and evolution from episodic to chronic migraine: a longitudinal population-based study. Headache. 2008 Sep;48(8):1157–68.Goldstein J, Silberstein SD, Saper JR, Ryan RE Jr, Lipton RB. Acetaminophen, aspirin, and caffeine in combination versus ibuprofen for acute migraine: results from a multicenter, double-blind, randomized, parallel-group, single-dose, placebo-controlled study. Headache. 2006 Mar;46(3):444–53.PetersenK-UKopsMHeintzeK. WHO step 1 analgesics in the treatment of (migraine) headache. Pharmakon2017; 5: 69–74.
Migraine – preventive therapy
MTIS2018-174
EFFICACY, SAFETY, AND TOLERABILITY OF ORALLY ADMINISTERED ATOGEPANT FOR THE PREVENTION OF EPISODIC MIGRAINE: RESULTS FROM A PHASE 2B/3 STUDY
P. J. Goadsby1,*, D. W. Dodick2, J. M. Trugman3, M. Finnegan3, H. Lakkis3, K. Lu3 and A. Szegedi3
1NIHR-Wellcome Trust King's Clinical Research Facility, King's College, London, United Kingdom
2Mayo Clinic, Phoenix
3Allergan plc, Madison, United States
Introduction: Atogepant is a novel, oral CGRP receptor antagonist in development for the prevention of migraine.
Objectives: This study evaluated the efficacy, safety, and tolerability of atogepant versus placebo for the prevention of episodic migraine.
Methods: Multicenter, randomized, double-blind, placebo-controlled, parallel-group study (NCT02848326). Adult patients with a history of migraine, with or without aura, were included. Patients with 4–14 migraine days in the 28-day baseline period were randomized 2:1:2:1:2:1 to placebo, atogepant 10 mg QD, 30 mg QD, 30 mg BID, 60 mg QD, or 60 mg BID, respectively, and treated for 12 weeks for the prevention of episodic migraine. Primary efficacy endpoint was change from baseline in mean monthly migraine days across the 12-week treatment period. Safety and tolerability were evaluated.
Results: Of patients randomized (n = 834), 825 were in the safety population, and 795 were included in the primary efficacy population. Mean age was 40.1 years; majority white (76.1%), female (86.5%), and had not taken preventive treatment for migraine in the past (n = 593, 71.9%). At baseline, patients reported an average 7.67 (SD = 2.49) migraine days. Mean change in migraine days across the 12-week treatment period (adjusted p-values for comparisons versus placebo): placebo (−2.85), atogepant 10 mg QD (−4.00, p = 0.0236), 30 mg QD (−3.76, p = 0.0390), 60 mg QD (−3.55, p = 0.0390), 30 mg BID (−4.23, p = 0.0034), 60 mg BID (−4.14, p = 0.0031). A total of 480 patients (58.2%) reported treatment-emergent adverse events (AEs); 170 (20.6%) were considered treatment-related. The most common treatment-emergent AEs were nausea, fatigue, constipation, upper respiratory tract infection, nasopharyngitis, urinary tract infection, and blood creatine phosphokinase increase (reported in >5% of patients in at least one treatment group). Seven patients (0.8%) reported serious AEs; none were considered related to treatment. Following daily dosing, 11 cases of ALT/AST elevations ≥3 × the upper limit of normal were reported; the number of cases were balanced across treatment groups (placebo [n = 3], 10 mg QD [n = 2], 30 mg QD [n = 1], 60 mg QD [n = 3], 30 mg BID [n = 1], 60 mg BID [n = 1]).
Conclusion: All 5 atogepant treatment arms showed statistically significant differences from placebo in reductions from baseline in mean migraine days across the 12-week treatment period. Reductions in mean migraine days and treatment differences versus placebo were clinically relevant. Atogepant was well-tolerated with no treatment-related serious adverse events.
Disclosure of Interest: P. Goadsby Conflict with: Has reported personal fees from Akita Biomedical and Alder Biopharmaceuticals, grants and personal fees from and Amgen, personal fees from Autonomic Technologies Inc., Avanir Pharma, Cipla Ltd, Colucid Pharmaceuticals, Ltd., Dr Reddy’s Laboratories, grants and personal fees from Eli-Lilly and Company, personal fees from Electrocore LLC, grants and personal fees from eNeura Inc., personal fees from Novartis, Pfizer Inc., Promius Pharma, Quest Diagnostics, Scion, Teva Pharmaceuticals, and Trigemina Inc., and personal fees from MedicoLegal work, Journal Watch, Up-to-Date, Oxford University Press outside the submitted work. In addition, Dr. Goadsby has a Magnetic stimulation patent for headache pending to eNeura., D. Dodick Conflict with: Within the last 36 months, Dr. Dodick reports personal fees from Acorda, Amgen, Alder, Allergan, Autonomic Technologies, Biohaven, Colucid, Eli Lilly, eNeura, Foresight Capital, Neurolief, Zosano, WL Gore, Vedanta Associates, Promius Pharma, Magellan Healthcare, CC West Ford Group, Nocira, Novartis, NuPathe, Supernus, Electrocore, Tonix, Teva, Alcobra, Insys, Ipsen, Charleston Laboratories, Biocentric, Theranica, Xenon. ZP Opco. Travel expense reimbursement and speaking fee from Sun Pharma. Anticipated income from consulting within next 3 weeks not previously reported: Impel pharmaceuticals (currently under review by Mayo Clinic Medical Industry Relations Committee). Compensation for activities related to data safety monitoring committee from Axsome. Speaking fees, or fees related to CME content development: Healthlogix, Medicom Worldwide, Medlogix Communications, MedNet, Miller Medical Communications, PeerView Operation Services America, Web MD/Medscape, American Academy of Neurology, American Headache Society, PeerView Institute for Medical Education, Chameleon Communications, Academy for Continued Healthcare Learning, Universal Meeting Management, Haymarket Medical Education, Global Scientific Communications, UpToDate, Meeting LogiX. Royalties from editorial or book publishing: Oxford University Press, Cambridge University Press, Wiley Blackwell, Sage, Wolters Kluwer Health. Consulting use agreement through employer: NeuroAssessment Systems, Myndshft. Hold equity in: Aural Analytics, Healint, Theranica, Second Opinion/Mobile Health, Epien. Board of Directors position: King-Devick Technologies, Ontologics., J. Trugman Conflict with: full-time employee and stockholder of Allergan plc, M. Finnegan Conflict with: Full-time employee of Allergan plc, H. Lakkis Conflict with: Full-time employee and stock/stock option holder of Allergan plc, K. Lu Conflict with: Full-time employee and stock/stock option holder of Allergan plc, A. Szegedi Conflict with: Full-time employee of Allergan plc and stockholder of Allergan and Merck.
Migraine – preventive therapy
MTIS2018-176
STUDY CGAL: A PLACEBO-CONTROLLED STUDY OF GALCANEZUMAB IN PATIENTS WITH EPISODIC CLUSTER HEADACHE: RESULTS FROM THE 8-WEEK DOUBLE-BLIND TREATMENT PHASE
J. M. Martinez1, P. J. Goadsby2,3, D. W. Dodick4, J. N. Bardos1, T. M. Myers Oakes1, B. A. Millen1, C. Zhou1, S. A. Dowsett1, S. Aurora1,*, J. Y. Yang1, R. R. Conley1,5
1Eli Lilly and Company, Indianapolis, United States
2NIHR-Wellcome Trust King’s Clinical Research Facility, King’s College London, London, United Kingdom
3University of California, San Francisco
4Mayo Clinic, Phoenix
5University of Maryland School of Medicine, Baltimore, United States
Introduction: Cluster headache is one of the most disabling pain disorders but, to date, preventive treatments have not been developed specifically.
Objectives: We assessed the efficacy and safety of galcanezumab, a humanized monoclonal antibody that selectively binds to calcitonin gene-related peptide (CGRP), in individuals with episodic cluster headache.
Methods: This study comprised a screening period; a prospective baseline period; an 8-week, double-blind, placebo-controlled treatment period; and a washout period. We present findings from the double-blind treatment period. Participants were randomized 1:1 to galcanezumab 300 mg (N = 49) or placebo (N = 57) subcutaneously (SC) once monthly. The primary endpoint was overall mean change from baseline in weekly cluster headache attack frequency across Weeks 1–3. The key (gated) secondary endpoint was the proportion of participants achieving a reduction from baseline of ≥50% in weekly cluster headache attack frequency at Week 3.
Results: The mean change in weekly cluster headache attack frequency across Weeks 1–3 was −8.7 for galcanezumab versus −5.2 for placebo (treatment groups difference in mean change, −3.5 [95% CI −6.7, −0.2]; p = 0.036). The percentage of participants achieving ≥50% reduction in weekly cluster headache attack frequency at Week 3 was 76% for galcanezumab versus 57% for placebo (p = 0.04). Four participants (8%) in the galcanezumab group discontinued during the double-blind period versus 12 (21%) in placebo. In the placebo group, 8 (14%) discontinued due to lack of efficacy versus 1 (2%) with galcanezumab (p = 0.036). There were no clinically meaningful differences between treatment groups on tolerability or safety parameters except for a greater incidence of injection site pain with galcanezumab versus placebo (8.2% vs 0%, p = 0.043).
Conclusion: In individuals with episodic cluster headache, galcanezumab reduced the weekly cluster headache attack frequency across Weeks 1–3 and resulted in a greater percentage achieving a ≥50% reduction in the weekly cluster headache attack frequency at Week 3. The safety profile of galcanezumab in this population was similar to that seen previously in patients with episodic or chronic migraine.
Disclosure of Interest: J. Martinez Conflict with: Full-time employees and minor shareholders of Eli Lilly and Company, P. Goadsby Conflict with: grants and personal fees from Amgen and Eli Lilly and Company, and personal fees from Alder Biopharmaceuticals, Allergan, Autonomic Technologies Inc., Dr Reddy's Laboratories, Electrocore LLC, eNeura, Novartis, Scion, Teva Pharmaceuticals, and Trigemina Inc., and personal fees from MedicoLegal work, Journal Watch, Up-to-Date, Oxford University Press, Massachusetts Medical Society, and Wolters Kluwer; and a patent Magnetic stimulation for headache assigned to eNeura without fee., D. Dodick Conflict with: Reports (within the past 36 months) personal fees from Acorda, Amgen, Alder, Allergan, Autonomic Technologies, Biohaven, Colucid, Eli Lilly, eNeura, Foresight Capital, Zosano, WL Gore, Vedanta Associates, Promius Pharma, Magellan Healthcare, CC West Ford Group, Nocira, Novartis, NuPathe, Supernus, Electrocore, Tonix, Teva, Alcobra, Insys, Ipsen, Charleston Laboratories, Biocentric, Theranica, Xenon. ZP Opco. Travel expense reimbursement and speaking fee from Sun Pharma. Compensation for activities related to data safety monitoring committee from Axsome. Speaking fees, or fees related to CME content development: Healthlogix, Medicom Worldwide, Medlogix Communications, MedNet, Miller Medical Communications, PeerView Operation Services America, Web MD/Medscape, American Academy of Neurology, American Headache Society, PeerView Institute for Medical Education, Chameleon Communications, Academy for Continued Healthcare Learning, Universal Meeting Management, Haymarket Medical Education, Global Scientific Communications, UpToDate, Meeting LogiX. Royalties from editorial or book publishing: Oxford University Press, Cambridge University Press, Wiley Blackwell, Sage, Wolters Kluwer Health. Consulting use agreement through employer: NeuroAssessment Systems, Myndshft. Hold equity in: Healint, Theranica, Second Opinion/Mobile Health, Epien. Board of Directors position: King-Devick Technologies, Ontologics., J. Bardos Conflict with: Full-time employees and minor shareholders of Eli Lilly and Company, T. Myers Oakes Conflict with: Full-time employees and minor shareholders of Eli Lilly and Company, B. Millen Conflict with: Full-time employees and minor shareholders of Eli Lilly and Company, C. Zhou Conflict with: Full-time employees and minor shareholders of Eli Lilly and Company, S. Dowsett Conflict with: Full-time employees and minor shareholders of Eli Lilly and Company, S. Aurora Conflict with: Full-time employees and minor shareholders of Eli Lilly and Company, J. Yang Conflict with: Full-time employees and minor shareholders of Eli Lilly and Company, R. Conley Conflict with: Full-time employees and minor shareholders of Eli Lilly and Company.
Migraine – preventive therapy
MTIS2018-173
ONABOTULINUM TOXIN A IN REFRACTORY CHRONIC MIGRAINE WITH MEDICATION OVERUSE
A. Benchiheub1,*, L. McCorkell1, C. Rankin1 and A. Tyagi1
1Neurology, Queen Elizabeth Univ. Hospital, Glasgow, United Kingdom
Introduction: Onabotulinum toxin A is standard treatment for chronic migraine once medication overuse is addressed. This treatment in Scotland is currently only used for refractory migraine where atleast 6 oral preventive treatments have been tried.
Objectives: To compare the response rates to onabotulinum toxin A treatment in patients with refractory migraine with or without medication overuse.
Methods: We conducted a retrospective analysis on all patients who were commenced on Onabotulinum toxin A treatment over a 3 month time period between Aug 17 and Nov 17. Data was collected directly from the patients medical records, clinic letters and Headache diaries, as well as from the Onabotulinum toxin A database.
Results: 31 patients were commenced on Onabotulinum toxin A treatment over 3 months. 17 of these patients were overusing their abortive treatments prior to their first Onabotulinum toxin A cycle. Of these patients; 4 met the positive stopping criteria after 2 cycles, 8 have had a positive response and are continuing treatment, and 5 were discontinued after their 2nd cycle as they met the negative stopping criteria. Of the remaining 14 patients who were not overusing abortive treatments prior to first Onabotulinum toxin A cycle; there were no patients who met the positive stopping criteria after 2 cycles, 9 patients had a positive response and are continuing treatment, 5 patients discontinued after their 2nd cycle as they met the negative stopping criteria.
Conclusion: There was no difference in response to Onabotulinum toxin A between Medication overuse patients and non medication overuse patients; suggesting that medication overuse does not affect the success rate of Onabotulinum toxin A treatment even in patients with refractory Chronic Migraine.
Total No of Patients
No of Patients who had a Positive response (Continuing)
No of Patients who met Positive stopping Criteria
No of Patients who met Negative Stopping Criteria
Medication overuse
17
8
4
5
Non Medication Overuse
14
9
0
5
Migraine – preventive therapy
MTIS2018-175
DAITH PIERCING, VAGUS NERVE STIMULATION AND MIGRAINE PREVENTION
C. Blatchley1,* and A. Wilkins2
1London Migraine Clinic, London
2University of Essex, Colchester, United Kingdom
Introduction: Daith ear piercing has been associated with anecdotal reports of reduced migraines for over 20 years, corroborated by three recent retrospective online surveys researched by the authors (over 3000 respondents, of which 500 had migraines >10yrs and piercing >12 months). Recent anecdotal reports from piercers suggest immediate headache reduction and improved visual comfort directly after piercing.
Daith piercings pass through a ridge of cartilage innervated by the vagus nerve, unlike other ear piercings which do not and are not associated anecdotally with migraine reduction.
Objectives: To follow patients undergoing Daith piercing for migraines, and ascertain immediate changes in visual discomfort induced by high-contrast gratings and assess any subsequent changes in headache frequency.
Methods: 40 consecutive patients (39 women) completed a headache questionnaire before undergoing a Daith piercing as treatment for longstanding headache. Visual discomfort was assessed before and immediately after piercing. Patients looked at a succession of 10 gratings of increasing contrast and reported any discomfort measured on a 6-point ordinal scale. The responses were compared to a control group of 40 healthy women.
(The gratings were horizontal, circular in outline, subtending 10 degrees; they had a square-wave luminance profile, a spatial frequency of three cycle per degree and increased linearly in log contrast from 2.7% to 94%).
Patients were followed up 1–3 months after piercing. This follow-up will continue.
Table 1: Mean (SD) headaches per month
Reported improvement at follow-up
Before piercing
At 1-3 month follow-up
“None”
20.2
(13.6)
21.1
(12.4)
“Little”
13.6
(12.9)
6.4
(7.5)
“Great”
15.3
(9.8)
2.0
(2.8)
Results:Control group: the gratings induced no visual discomfort in any volunteer
Patient group: follow-up data were available for 34(74%) of the 40 patients. Of these, 8 reported no effect on migraines and 26 reported improvement (13 “a little” and 13 “great”). Prior to piercing, 0 of the 8 non-responders reported severe visual discomfort, compared to 15 of the 26 responders (p < .005 by Fishers exact test). Immediately after piercing, only 4 of the 26 reported severe discomfort (p < .003 by Fishers exact test). There was no significant difference in visual discomfort between those later reporting “little” and “great” improvement in their migraines.
We then analysed the change in headache days before and 1–3 months after piercing. See Table 1
Other migraine symptoms were also reduced in responders but not in non-responders
Conclusion: The data suggest Daith piercing can reduce:
1. migraine frequency
2. visual discomfort from grating patterns (which is known to reflect cortical excitability in migraine[1,2])
The retrospective surveys also suggest a specific non-responder group, and a long term action >12months in some responders
Electrical stimulation of the vagus nerve reduces cortical excitability in epilepsy[3]. Transcutaneous electrical stimulation of the auricular branch is used in the treatment of migraines[4].
The response to Daith piercing is consistent with vagus nerve stimulation and an associated reduction in cortical excitability.
Extended follow-up and a randomised controlled trial are indicated.
References
HuangJZongXWilkinsAet al.fMRI evidence that precision ophthalmic tints reduce cortical hyperactivation in migraine. Cephalalgia2011; 31(8): 925–936.HuangJCooperTGSatanaBKaufmanDICaoY. Visual distortion provoked by a stimulus in migraine associated with hyperneuronal activity. Headache2003; 43: 664–71.EnglotDJChangEFAugusteKI. Vagus nerve stimulation for epilepsy: a meta-analysis of efficacy and predictors of response. Journal of Neurosurgery2011; 115: 1248–55.StraubAEllrichJErenOet al.Treatment of chronic migraine with transcutaneous stimulation of the auricular branch of the vagal nerve (auricular t-VNS): a randomized, monocentric clinical trial. J Headache Pain2015; 16: 543.
Migraine – preventive therapy
MTIS2018-177
PREVENTIVE TREATMENTS (ACUPUNCTURE, NUTRACEUTICALS OR DRUG) FOR PEDIATRIC MIGRAINE: A PROSPECTIVE STUDY
I. Toldo*, A. C. Milocchi1, E. Piretti2, M. P. Rossaro1, M. Nosadini1, S. Sartori1 and P. A. Battistella1
1Department of Woman's and Child’s Health, University of Padua, Padua
2Child Neurology and Psychiatric Unit of Cavalese, Azienda Provinciale per i Servizi Sanitari di Trento, Trento, Italy
Introduction: The use of preventive treatments for paediatric migraine may be limited by partial efficacy, adverse effects, contraindications for comorbidities, off-label use in children, lack of definite guidelines and scarcity of controlled studies. Studies on acupuncture as preventive treatment of pediatric migraine are rare (1,2).
Objectives: The aim of the study is to describe the effect of three interventions (acupuncture, nutraceuticals or drug) for migraine prevention in children and adolescents.
Methods: Observational and prospective clinical study conducted at the Juvenile Headache Centre of Padua between October 2016 and June 2018, with the following inclusion criteria: children age 6–17 years; diagnosis of migraine according to the International Classification of Headaches Disorders (ICHD-3, 2018); migraine without or with aura with more than 4 attacks per month or chronic migraine lasting for at least 6 months; preventive treatments for 3 months with acupuncture (A) (1/week for 2 months then 2/month, total 10 times) or nutraceuticals (N) (magnesium with multivitamins) or pizotifen (P) (the only drug licensed in Italy for migraine prophylaxis in children).
The following outcomes were evaluated at the baseline (T0) before treatment, and 1 month after the end of treatment (T1): headache diary (number of attacks per month, number of symptomatic drugs per month); PedMidas questionnaires (total score); patient satisfaction (0-10). The outcomes have been valuated
Results: 56 cases were enrolled in the study (18 A, 16 N, 22 P). The most interesting results of the study have been summarized in Table 1. The median score of patient satisfaction (0 = insufficient; 10 = very satisfied) was higher for A (9; IQR: 8–9.5), than N (7; IQR 3.5-8) and P (7; IQR 6–9).
Conclusion: It is not possible to statistically compare the three groups (A, N, P) because the characteristics at baseline differ. However, the effect (on all the variables) of A and N appears clinically significant and superior to that of P. Patients treated with A were very satisfied. Acupunture may be a valid preventive treatment for migraine in children and adolescents, and warrants further studies.
ACUPUNCTURE (N = 18)
NUTRACEUTICAL (N = 16)
PIZOTIFEN (N = 22)
Number of migraine attacks /30 days, median [IQR]
T0
10 (4; 19)
5 (3; 23)
3 (1; 6)
T1
3 (1; 8)
2 (1; 4)
2 (1; 3)
T0-T1
4 (1.25; 9)
3 (0; 6)
0 (0; 0)
Number of symptomatic drugs /30 days, median [IQR]
T0
4 (2; 5)
3 (1; 6)
3 (0; 4)
T1
2 (0; 3)
1 (0; 2)
1 (0; 4)
T0-T1
2 (0; 3)
1,5 (-0.5; 4.2)
-0,5 (-1; 0)
PedMIDAS, median [IQR]
T0
47 (17; 85)
16 (11; 30)
19 (10; 34)
T1
15 (5; 64)
9 (6; 20)
7 (1; 24)
T0-T1
13 (7;34)
7 (-0.25; 15.4)
12.7 (8.7; 24)
Legend: T0 = baseline; T1 = 1 month after the end of a 3-months treatment; T1-T0 = difference between T0 and T1. IQR = interquartile range.
References
PintovSet al.Acupuncture and the opioid system: implications in management of migraine. Pediatr Neurol.1997; 17(2): 129–33.GottschlingSet al.Laser acupuncturein children with headache: a double-blind, randomized, bicenter, placebo-controlled trial. Pain.2008; 137(2): 405–12.
Migraine – preventive therapy
MTIS2018-178
ONE-YEAR TREATMENT WITH GALCANEZUMAB IN PATIENTS WITH CHRONIC MIGRAINE: RESULTS FROM THE OPEN-LABEL PHASE OF THE REGAIN STUDY
H. C. Detke*, L. Q. Li1, S. Wang1 and S. K. Aurora1
1Eli Lilly and Company, Indianapolis, United States
Introduction: Chronic migraine is a neurological condition with a high disease burden and unmet clinical need.
Objectives: To assess long-term efficacy and safety of galcanezumab (GMB), a humanized monoclonal antibody that selectively binds to calcitonin gene-related peptide, in adult patients with chronic migraine.
Methods: This was a phase 3, double-blind (DB), randomized, placebo-controlled, 3-month study with a 9-month open-label extension (OLE). Eligible patients aged 18 to 65 years with chronic migraine, defined as ≥15 headache days per month, of which ≥8 met criteria for migraine, were randomized 2:1:1 to subcutaneous injections of placebo (N = 558), GMB 120 mg with a 240 mg loading dose (N = 278), or GMB 240 mg (N = 277), given once monthly for 3 months. Patients who entered the OLE received a 240 mg loading dose of GMB, followed by a maintenance dose of 120 mg/month at the next month, with flexible dosing thereafter (120 or 240 mg/month). Efficacy measures included number of monthly migraine headache days (MHD), ≥50% reduction in monthly MHD, and Role Function-Restrictive (RF-R) domain score of the Migraine-Specific Quality of Life Questionnaire (MSQ). Change from baseline in continuous and categorical measures over 12 months was analyzed using mixed model repeated measures analysis and generalized linear mixed models (GLIMMIX), respectively. OLE results are reported by prior DB treatment assignment.
Results: Of 1037 patients who completed DB treatment, 1022 subsequently entered the OLE, with 825 completing. Patients previously treated with placebo showed a rapid mean reduction in monthly MHDs after the first open-label dose and maintained this improvement over time, whereas the previous 120 mg and 240 mg GMB groups generally maintained or improved upon gains from the DB treatment phase (month 12: placebo, −8.41; GMB 120 mg, −8.89; GMB 240 mg, −7.99 from a baseline of 19.4 MHDs). The mean percentage of patients with ≥50% reduction from baseline ranged from 44.5% to 45.6% at month 6 and 53.3% to 56.9% at month 12. Mean improvement from baseline on the MSQ RF-R ranged from 26.5 to 30.2 points at month 6 and 29.0 to 32.9 points at month 12 on the 100-point scale. The most common (≥5%) treatment-emergent adverse events were nasopharyngitis (9.6%), upper respiratory tract infection (6.2%), and injection-site reaction (5.9%). A total of 4.5% of patients discontinued due to an adverse event, and 4 patients (0.4%) discontinued due to an injection site–related adverse event. There were no clinically meaningful changes in any of the safety measures.
Conclusion: Final OLE results support the observation that GMB appears effective, safe, and well tolerated for the preventive treatment of chronic migraine. Galcanezumab had a favorable safety profile after 1 year of treatment at doses of 120 or 240 mg/month. No new safety findings were identified.
Disclosure of Interest: H. Detke Conflict with: Employee and shareholder of Eli Lilly and Company, L. Li Conflict with: Employee and shareholder of Eli Lilly and Company, S. Wang Conflict with: Employee and shareholder of Eli Lilly and Company, S. Aurora Conflict with: Employee and shareholder of Eli Lilly and Company.
Migraine – preventive therapy
MTIS2018-179
SINGLE-PULSE TRANSCRANIAL MAGNETIC STIMULATION (STMS) FOR THE TREATMENT OF MIGRAINE: A PROSPECTIVE REAL WORLD EXPERIENCE
G. Lambru1,2, B. Hill2,*, J. Lloyd1, A. Al-Kaisy3, A. P. Andreou1,2
1Wolfson CARD, King’s College London
2The Headache Centre
3Pain Management and Neuromodulation, Guy's and St Thomas' Hospital, London, United Kingdom
Introduction: Single pulse transcranial magnetic stimulation (sTMS) is a non-invasive neuromodulation technique which has been approved in 2014 by the National Institute for Health and Care Excellence (NICE) for the acute and preventive treatment of migraine. However, its effectiveness in a real world NHS service has not been explored yet. The Headache Centre, Guy’s and St Thomas’ NHS Trust is currently the only NHS service commissioned to offer sTMS to migraine patients. Here we present our interim results.
Objectives: This is an open-label prospective clinical audit. It aims to evaluate the effectiveness of sTMS (eNeura) as a non-pharmacological modality for the treatment of migraine with and without aura in a real world setting.
Methods: The audit is ongoing. We present here the outcome of the first 44 consecutive treated patients with chronic or high frequency episodic migraine. Audit inclusion criteria were a documented diagnosis of chronic migraine documented in a headache diary and patients willingness in filling a headache diary and HIT-6 score, which were used to collect clinical outcomes. Change in headache days, migraine days and HIT-6 at 3 months of treatment compared to baseline were analysed. Adverse events and treatment compliance were also collected.
Results: Forty-two migraine patients (11 with aura, 31 without aura) treated with sTMS were analysed. Twenty patients (47.6%) received sTMS after failing BotoxÒ therapy, hence were considered refractory to medical treatments. At baseline, patients displayed an average of 14.7 headache days (HD)/month, 11.1 migraine days (MD)/month and HIT-6 score of 63.3. Following 3-month trial, 28 patients (64%) obtained a clinically meaningful benefit (- 2.7 MD/month and -5.4 points on HIT-6 score) hence continued the treatment. Seventeen patients (36%) did not benefit from the therapy and discontinued the treatment. Of those, the majority were Botox non-responders. At 6 months 1 out of 28 responders stopped the treatment due to lack of effect durability. Amongst responders, five patients continued sTMS treatment for 12 months, 10 for nine months and 12 for six months. Treatment compliance was satisfactory with sTMS used up to eight pulses three times a day. Side effects were minor and include, worsening of the headache (n = 3), transient mild dizziness during the treatment (n = 1) and scalp tenderness (n = 2).
Conclusion: sTMS may constitute an effective and well tolerated preventive treatment option for difficult-to-treat high frequency/chronic migraine patients in a real world setting. Since sTMS is less costly than BotoxÒ on the NHS, it could be included as one of the three preventive treatment to offer to chronic migraine patients prior to Botox.
Disclosure of Interest: G. Lambru Conflict with: honoraria for travelling and educational material from Allergan, ATI, Novartis, Nevro., B. Hill: None Declared, J. Lloyd: None Declared, A. Al-Kaisy: None Declared, A. Andreou Conflict with: Eneura.
Migraine – preventive therapy
MTIS2018-180
ONABOTULINUMTOXINA: AN EFFECTIVE TOOL IN THE THERAPEUTIC ARSENAL FOR CHRONIC MIGRAINE WITH MEDICATION OVERUSE
E. Caronna1,*, V. J. Gallardo2, N. Hernández-Beltrán3, M. Torres-Ferrus4,5, P. Pozo-Rosich1,6
1Neurology, Hospital Universitari Vall d'Hebron
2Headache and Neurological Pain Research Group,, Vall d'Hebron Research Institute (VHIR), Barcelona, Spain
3Neurology, Neuroclinica and Promedan,, Medellín, Colombia
4Neurology, Hospital Universitari Vall d’Hebron
5Headache and Neurological Pain Research Group
62Headache and Neurological Pain Research Group, Vall d'Hebron Research Institute (VHIR), Barcelona, Spain
Introduction: Up to 50% of patients with chronic migraine (CM) associate acute pain medication overuse (MO). In daily practice, patients seemed to improve after treatment with onabotulinumtoxinA, but there are no established therapeutic protocols.
Objectives: To evaluate the early response of onabotulinumtoxinA as a treatment tool in patients with CM and MO.
Methods: This is a retrospective study in patients with CM and MO who received two cycles of onabotulinumtoxinA infiltrations following PREEMPT protocol. We evaluated the efficacy of onabotulinumtoxinA in MO resolution, defined as less than 10 days/month of acute medication intake (triptans, opioids and combinations) or 15 days/month (non-steroidal anti-inflammatory drugs – and simple analgesics). In addition, we analyzed changes in headache frequency, pain intensity, and headache-related disability (MIDAS scale). A multivariate analysis was carried out to identify factors independently related to MO resolution.
Results: We included 139 consecutive patients with CM and MO. After 2 cycles of onabotulinumtoxinA, 73.4% had >50% reduction in acute medication intake and 57.6% achieved MO resolution. A 7.9% of patients did not use any acute medication after treatment. Even though both MO-ongoing group and MO-resolution group improve headache frequency, the reduction was significantly higher for the group which discontinued the use of acute medication after onabotulinumtoxinA treatment (p < 0.001). In this group, 73.0% reduced headache frequency >50% and daily headache changed from 71.2% to 23.2% (p < 0.001). Both groups showed an improvement in pain intensity and in MIDAS score (p < 0.05). In the multivariate analysis we observed that MO resolution had an inverse association with medication intake at baseline (OR:0.294, p < 0.05) and a direct association with frequency (OR:20.455, p < 0.001) and MIDAS score (OR: 6.465, p < 0.05) improvements.
Conclusion: OnabotulinumtoxinA has an early beneficial effect on the discontinuation of acute medication in patients with CM and MO. Therefore, onabotulinumtoxinA might be considered a therapeutic tool in CM with MO.
Migraine – preventive therapy
MTIS2018-181
ANTI-CGRP MONOCLONAL ANTIBODIES FOR THE TREATMENT OF EPISODIC MIGRAINE: AN OVERVIEW OF AVAILABLE RESULTS AND COMPARISON WITH THE CURRENTLY USED PROPHYLACTICS
F. Vandervorst*, Laura Van Deun, Jacques De Keyser, Koen Paemeleire and Jan Versijpt
Introduction: Recently, the first anti-CGRP monoclonal antibody, erenumab, was approved by both the FDA and EMA for the preventive treatment of migraine in adults, probably announcing the use of this novel treatment in clinical daily practice in the near future.
Objectives: The objective of the present study was to present an early overview on currently available, combined efficacy results of all four anti-CGRP monoclonal antibodies in the treatment of episodic migraine. Secondly, these results and the amount of evidence gathered until now from randomized controlled trials (RCTs), is compared to the results of the currently used prophylactics for episodic migraine.
Methods: Results from published RCTs in non-refractory episodic migraine patients (published in full article, abstract or press release) available up to the 1st of August 2018, were included. The mean reduction of monthly migraine days (MMD) versus placebo was used as the endpoint of choice. This same endpoint was calculated for 6 other currently used prophylactics in episodic migraine, all with level A or B evidence for use in clinical practice.
Results: Results from five phase 2 and four phase 3 RCTs with anti-CGRP monoclonal antibodies were available where, in total, 2519 patients were treated. The latter number is already the highest number of patients studied in RCTs with a prophylactic agent in episodic migraine although the number of RCTs with topiramate was equal (1293 subjects treated) and for beta-blockers even higher (26 with 1425 subjects treated, combined for propranolol and metoprolol). The other number of subjects studied in RCTs were 436 for valproate (6 RCTs), 132 for candesartan (2 RCTs), 436 for valproate (6 RCTs), 41 for venlafaxine (1 RCT) and 383 for amitriptyline (5 RCTs).
The overall mean reduction of MMD versus placebo for the anti-CGRP monoclonal antibodies was −1,58 days. This endpoint could only be calculated in a fraction of the RCTs of the other migraine prophylactics and yielded −0,86 for candesartan (2 RCTs), −0,75 for topiramate (2 RCTs), −1,75 for valproate (3 RCTs), −0,92 for beta-blockers (4 RCTs), −3,02 for venlafaxine (1 RCT) and −1,10 for amitriptyline (1 RCT).
Conclusion: Efficacy results of anti-CGRP monoclonal antibodies are at least comparable to those of the currently used prophylactics in episodic migraine. The level of evidence however seems already as high or even higher given the number of RCTs conducted, all with large groups of patients. Although long term safety data and efficacy results in treatment-refractory migraine patients are still partly lacking, from a purely clinical point of view, the treatment of episodic migraine with anti-CGRP monoclonal antibodies is emerging as a first line treatment.
Other primary headache
MTIS2018-182
EXAMINING THE IMPACT OF SPHENOPALATINE GANGLION STIMULATION ON LONGITUDINAL PATTERNS OF ACUTE PAIN RELIEF ACROSS MULTIPLE CLUSTER HEADACHE ATTACKS: RESULTS FROM THE PATHWAY CH-2 TRIAL
S. J. Tepper1,* and J. S. McGinley1
1ATI, Los Angeles, United States
Introduction: Cluster headache (CH) is a highly disabling chronic neurological condition and the pain is recognized as among the most severe known to humans.1,2,3 Current treatment options have significant efficacy and side effect limitations and recent clinical trial failures in chronic cluster headache have further underscored the need for effective treatments to treat this disabling condition. 4,56,7,8,9 The sphenopalatine ganglion (SPG) has long been a clinical target to treat headache disorders.10 SPG stimulation with the SPG Microstimulator System was shown to be effective for the treatment of CH in a previous study
Objectives: The goals of the current study were two-fold. First, we identified common patterns of pain relief through the first hour post-treatment across multiple ipsilateral cluster headache (CH) attacks. Second, we tested whether treating attacks with sphenopalatine ganglion (SPG) stimulation produced more favorable patterns of change in pain relief over time compared to a sham comparison group.
Methods: Data for the current study came from the Pathway CH-2 Trial, a multi-centre, interventional, randomised, placebo-controlled, parallel group, double-blind study focused on evaluating the safety and efficacy of an SPG neurostimulation system for the treatment of chronic CH. The current study focused on evaluating acute data where subjects reported on multiple attacks during the experimental period of the trial. Our primary outcome was pain relief at 15 minutes and 60 minutes post-treatment. Multilevel latent class analysis (MLCA) was used to identify unique patterns of change in pain relief and test for treatment group differences in these patterns of change over time.
Table: Model-implied probabilities of class membership by treatment group
SPG
Sham
Comparision
Early Sustained Releif (ESR)
79.5%
29.6%
x2 (1) = 10.51, p = .001
Late Onset Relief (LOR)
5.7%
10.7%
X2 (1) = 0.73, p = .39
No Relief (NR)
14.9%
59.6%
X2 (1) = 6.90, p = .009
SPG Sham Comparison Early Sustained Relief (ESR) 79.5% 29.6% χ2(1) = 10.51, p = .001 Late Onset Relief (LOR) 5.7% 10.7% χ2(1) = 0.73, p = .39 No Relief (NR) 14.9% 59.6% χ2(1) = 6.90, p = .009
Results: The analysis sample consisted of 76 participants reporting a total of 992 attacks (across individuals, median number of attacks reported was 10). Results from the pain relief MLCA showed that attacks were best represented by 3 different patterns of relief: 1. Early Sustained Relief (ESR: High probability of relief at 15 min and 60 min), 2) Late Onset Relief (LOR: low probability of relief at 15 min and high probability of relief at 60 min, and 3) No Relief (NR: low probability of relief at both 15 min and 60 min). Individuals varied in their propensity to experience each of these attack subtypes (p < 0.05). Contrasting the three attack subtypes showed that, using both LOR and NR attacks as references, an average individual treating with SPG stimulation group had greater odds of ESR attacks compared to sham (ORESR/LOR = 10.75; ORESR/NR = 5.08; p < 0.05). Findings showed that the probability of an individual in the SPG group having an ESR attack was 80% compared to 30% for sham (p < 0.01) and their probability of NR attacks was significantly reduced (SPG: 15% vs. Sham: 60%, p < 0.01).
Conclusion: Previous research has demonstrated that SPG stimulation works to relieve pain rapidly during CH attacks, but this study uniquely assessed how treatment impacts clinically meaningful attack subtypes that arise in practice. MLCA supported a three-class solution and showed that the SPG group had an increased likelihood of experiencing ESR attacks compared to sham. Future research should replicate these analyses in other representative samples and extend this work to other important CH outcomes.
Paediatric headache
MTIS2018-183
AN AUDIT IN TO THE NEUROIMAGING EXPERIENCE OF PATIENTS REFERRED TO THE HEADACHE SERVICE – HOW CLOSE ARE WE ALIGNED WITH THE NICE GUIDELINE (CG150) FOR IMAGING IN CHILDREN WITH PRIMARY HEADACHES?
S. Talib, S. Ramji, H. Nightingale1,*, P. Prabhakar1 and K. Mankad1
1Neurology, Great Ormond Street Hospital, London, United Kingdom
Introduction: The Children’s Headache at Great Ormond Street Hospital (GOSH) sees many children with irretractable primary headaches. Often these children have a form of brain imaging done prior to their appointment. NICE recommends against imaging in individuals with primary headaches that lack signs of secondary headaches as it often results in incidental findings that have no correlation with their clinical symptoms inciting anxiety in patients rather than reassurance.
Objectives: This audit investigates how closely aligned the Headache Clinic is with the NICE guidelines CG150, specifically looking at whether these patients had prior imaging, and whether these showed abnormal or incidental findings. The audit aims to identify any correlation between a specific headache diagnosis and incidental findings on brain imaging, and whether brain imaging altered the diagnosis.
Methods: Our audit looks at 280 patients over the age of 12 years seen at the GOSH Headache Clinic from September 2012, over a period of 5 years. Data was sourced from the electronic clinical patient database, reviewing clinic letters to see if they aligned with the guidelines on specific recommendations. All diagnoses were cross-referenced with the International Classification of Headache Disorders. Brain imaging at GOSH was scrutinised to look for any abnormalities and the classify the findings.
Results: 246 patients had a form of brain imaging, 29 patients had a brain scan at GOSH, and 232 had a scan at their local hospital. Overall 88% of patients had brain imaging and 83% had a scan prior to their appointment. Of these scans, 52 had abnormal findings, equating to 21% of scanned patients with an incidental finding. None of these however altered the patients’ diagnoses in clinic.
Correlations between abnormal findings and patient diagnosis were minimal, as the majority of the diagnoses were common headache disorders. However of the patients diagnosed with migraine with aura, 34% had an abnormal finding, of which 25% were due to white matter changes. Patients with CSF pressure changes all had an abnormal finding of an arachnoid cyst, however this was limited to only 2 patients. 26% of patients with a secondary headache had an abnormal finding on imaging, however this did not change diagnosis.
Conclusion: Whilst NICE recommends against brain imaging in the setting of a primary headache, sometimes imaging is necessary to exclude diseases, particularly at a specialist paediatric centre. Patients in this sample may have had complex underling diseases, which could explain deviation from guidelines. The abnormalities found on imaging did not alter patient diagnoses as these were incidental findings. However the patients with altered CSF pressure all had arachnoid cysts, and patients diagnosed with migraine with aura were more likely to have an abnormal brain scan. Whilst migraine with aura is a primary headache, it may be worthwhile further investigating if there is a link between migraine with aura, and risk of abnormalities on imaging.
Secondary headaches
MTIS2018-184
PRIORITY SETTING PARTNERSHIP DISCOVERS THE TOP 10 RESEARCH QUESTIONS FOR IDIOPATHIC INTRACRANIAL HYPERTENSION
S. P. Mollan1,*, K. Hemmings2, C. P. Herd3, A. Denton2, S. Williamson2 and A. J. Sinclair4
1Neuro-Ophthalmology, University Hospitals Birmingham NHS FT, Birmingham
2IIH UK, Newcastle
3Institute of Clinical Sciences
4Metabolic Neurology, University of Birmingham, Birmingham, United Kingdom
Introduction: Idiopathic Intracranial Hypertension (IIH) which causes debilitating headaches and in some permanent visual loss is under-researched. The current Cochrane review highlighted only two clinical trials in IIH.
Objectives: This James Lind Alliance Priority Setting Partnership (PSP) was commissioned by IIH UK, a patient charity, to encourage people with direct and personal experience of IIH to collectively identify and prioritise the top 10 uncertainties that impact on everyday clinical practice for the management IIH.
Methods: A modified nominal group technique was used to engage participants who had experience of IIH including: people with IIH, carers, family and friends, healthcare professionals.
They were invited to participate in two rounds of surveys to identify what issues they deemed should be prioritised for research in IIH. Unique research questions unanswered by current evidence were identified for the interim survey and participants were asked to identify their top 10 research priorities from this list. The top 26 uncertainties were presented to a consensus meeting with key stakeholders then agreeing the top 10 research priorities.
Results: 356 participants provided 2405 responses, 140 were deemed to be out of scope. 2,265 were grouped into 64 indicative questions. 14 were deemed to be already known or they would be unanswerable by research. 48 questions were then presented in the interim prioritisation survey. 512 people took part (401 with IIH, friends or carers and 111 healthcare professionals). The most popular 26 were then taken for the final workshop. 24 stakeholders, these included patients, carers, neurologists, ophthalmologists, radiologists, neurosurgeons, and nurses took part in the consensus workshop. They agreed the top 10 research priorities. The overarching research aspiration was to understand the aetiology and management of IIH. The top 10 research priorities for IIH included aetiology of IIH; the pathological mechanisms of headache in IIH; new treatments in IIH; the difference between acute and gradual visual loss; the best ways to monitor visual function; biomarkers of the disease; hormonal causes of IIH; drug therapies for treatment of headache; weight loss and its role in IIH; and finally, the best intervention to treat IIH and when should surgery be performed.
Conclusion: These research priorities identify crucial gaps in the existing evidence for those who develop and those who manage IIH.
Secondary headaches
MTIS2018-185
HEADACHE CURED BY HEPATIC TRANSPLANT: A CASE REPORT
D. Moreno Ajona1,* and P. Irimia1
1Neurology, University of Navarre Clinic, Pamplona, Spain
Introduction: Intracranial hypertension related to cerebral oedema may occur in up to 80% of cases fulminant hepatic failure. Cerebral oedema, however, is usually not associated with intracranial hypertension in chronic liver disease. Headache is not considered a common symptom in these patients.
Objectives: The purpose of this report is to describe a single case of a patient with intracranial hypertension headache caused by liver disease.
Methods: The patient was a 52-year-old man who was previously diagnosed of porto-mesenteric venous thrombosis due to antiphospholipid syndrome, treated by placing transjugular intrahepatic porto-sistemic shunt (TIPS). He reported headache episodes for approximately 2 years. He started with bi-occipital pressure-like pain that clearly worsened with the Valsalva manoeuvre, and also with physical activity. Progressively, the episodes became more frequent, until pain was constant throughout the day.
Results: Neurological examination showed dysarthria, right facial paresis and postural hands tremor. Brain MRI and MRV showed no signs of venous thrombosis. Several lumbar punctures were performed, obtaining CSF opening pressure, ranging 25-32 cm of CSF. Treatment with acetazolamide (up to 750 mg / 12 hours) as well as topiramate (25 mg OD) obtained only partial relief. Following a confusion state, blood analysis showed hyperammonaemia (305 µg/dL) with normal liver enzymes. Symptoms persisted until hepatic transplant was performed 3 years later. Since then, the patient obtained complete relief of his headache.
Conclusion: Hyperammonaemia can lead to cerebral oedema which, if maintained, may cause intracranial hypertension headache. High ammonium levels reaching the brain after TIPS may have been the cause for this patient’s headache.
Secondary headaches
MTIS2018-186
SUBCUTANEOUS ADIPOSE TISSUE FROM PATIENTS WITH IDIOPATHIC INTRACRANIAL HYPERTENSION DISPLAYS UNIQUE TRANSCRIPTOMIC AND METABOLIC FEATURES
C. Westgate1,2,*, M. Walsh3, I. Akerman1,2, G. Smith1,2, H. Botfield1,2, K. Markey1,2, D. Hebenstreit3, R. Singhal4, C. Ludwig1,2, G. Lavery1,2, A. Sinclair1,2,5
1Institute of Metabolism and Systems Research, University of Birmingham
2Centre for Endocrinology, Diabetes and Metabolism, Birmingham Health Partners, Birmingham
3School of Life Sciences, University of Warwick, Warwick
4Upper GI and Minimally Invasive Unit, Heart of England NHS Foundation Trust
5Department of Neurology, University Hospitals Birmingham, Queen Elizabeth Hospital, Birmingham, United Kingdom
Introduction: Idiopathic intracranial hypertension (IIH) is characterised by raised intracranial pressure (ICP), papilledema and chronic debilitating headache. IIH has a strong association with obesity. Over 95% of patients are obese women of reproductive age and the incidence is rising with the global epidemic of obesity. Truncal adiposity correlates with ICP and weight-loss lowers ICP and treats IIH. No mechanism explains the link between obesity and raised ICP. We hypothesise that adipose tissue from IIH patients is transcriptomically and metabolically distinct and contributes to raised ICP.
Objectives: We aimed to phenotype adipose tissue from IIH patients.
Methods: Phenotyping of subcutaneous (SC) adipose tissue from fasted female IIH patients and healthy age, BMI and gender matched controls derived from elective NHS bariatric lists, was achieved through RNA sequencing, histomorphometric analysis and nuclear magnetic resonance (NMR) metabolomics.
Results: Morphometric analysis showed that IIH and control SC adipocytes are indistinguishable in terms of size and cross-sectional area.
RNA sequencing highlights that IIH SC adipose has 693 upregulated genes and 400 downregulated genes (P < 0.05), where gene set enrichment analysis demonstrates a strong downregulation in ribosomal protein genes (P < 0.0001) and an upregulation in genes associated with lipid biosynthesis (P < 0.01). Analysis shows enrichment of genes associated with subjects gaining weight (P < 0.0001).
NMR metabolomics demonstrates increased glycerol production in IIH SC adipose vs control (186 ± 67 vs 97 ± 25 μM; p < 0.05 n = 6 vs 6). Lipid generating amino acids leucine and isoleucine were preferentially consumed by IIH SC adipose vs control. IIH SC adipose leptin secretion was elevated compared to controls (8309 ± 1593 vs 2366 ± 431 pg/24h/100 mg; p < 0.01, n = 11-12). Together, these data are indicative of altered lipid metabolism and function in IIH SC adipose tissue.
Conclusion: These data suggest that IIH SC adipose tissue is both transcripomically and metabolically distinct from matched controls. We propose that SC adipose derived factors, such as leptin, coupled with changes in lipid turnover may mechanistically contribute to raised ICP and warrants further investigation.
TACs
MTIS2018-187
PREMONITORY AND POSTDROME SYMPTOMS IN 28 CLUSTER HEADACHE PATIENTS IN A REFERRAL PRACTICE
M. Khalil1,*, D. Wei1 and P. J. Goadsby1
1Institute of Psychiatry, Psychology & Neuroscience, King's College London, London, United Kingdom
Introduction: Premonitory and postdrome symptoms in cluster headache are not well understood. It is important to elucidate their character in order to improve our understanding of the condition.
Objectives: To characterise the clinical phenotype and evolution of the “premonitory” and “postdrome” phases in a cluster headache attack.
Methods: This retrospective study was conducted as an audit in a tertiary headache centre. We identified cluster headache patients as per the International Classification of Headache Disorders 3rd edition (ICHD-3) from 2014 until 2017
Table:
Results: We identified 28 cluster headache patients. The majority were males (n = 18, 64%), with a median age of 48 (interquartile range of 40 to 56). Twenty-six patients (93%) had migraine biology. The median delay to diagnosis was 1 year and on average, a patient saw 4 clinicians before being diagnosed. Premonitory and postdrome symptoms were described 96%, with the median number of symptoms being 3. The commonest symptoms in the “premonitory” phase were, cranial autonomic symptoms, mood changes, neck stiffness and concentration difficulties with median duration before onset of pain of 10 minutes. The commonest postdrome symptoms were lethargy, cranial autonomic features, mood disturbance and poor concentration with median duration after the attack of 45 minutes.
Conclusion: Premonitory and postdrome symptoms are common in cluster headache patients; however, their durations are markedly shorter than those in migraine headache. Further studies are needed to compare the difference in those symptoms across the two condition and whether having migraine biology has an impact on their character and the duration.
Disclosure of Interest: M. Khalil: None Declared, D. Wei: None Declared, P. Goadsby Conflict with: Already submitted for this conference, Conflict with: Already submitted for this conference.