
Abstract

Headache Pathophysiology – Basic Science
OC-LB-001
Novel migraine therapeutic target discovery by single-cell RNA sequencing of trigeminal ganglia
William Renthal1*
1Neurobiology, Harvard Medical School, Boston, United States
Objectives
Pain experienced in migraine involves the sensitization of trigeminal afferent neurons, but the extraordinary cellular diversity within trigeminal ganglia has limited our understanding of the molecular substrates through which this process occurs. Recent advances in single-cell RNA sequencing technology have enabled the massively parallel identification and molecular profiling of nearly all cells within heterogeneous tissues. We are using this powerful tool to identify unique gene expression patterns within individual trigeminal ganglion cell types, and aim to leverage this insight towards the discovery of fundamentally new targets in headache pathophysiology.
Methods
Single-cell RNA sequencing was performed on postmortem mouse and human trigeminal ganglia. Approximately ten thousand cells were collected with a custom-designed microfluidics device (inDrops) and sequenced using next-generation Illumina sequencing. Unsupervised principle component analysis and graph clustering generated groups of cells based on their measured gene expression patterns. Novel marker genes were then identified using gene set enrichment analysis.
Results
Bioinformatic analysis of mouse and human data from trigeminal ganglion single-cell RNA sequencing identified clusters of cells that represent neuronal, glial, vascular, and meningeal cell subtypes. Individual cell types are clearly delineated based on their gene expression profiles, which enabled the interrogation of specific subtypes of neurons (e.g. CGRP+ nociceptors) or glia (e.g. satellite glia). Each of these unique cell populations are confirmed by selective expression of known marker genes. After each cell type was determined, genome-wide enrichment analysis was performed to determine the set of genes that are selectively enriched in each cell type. Indeed, we have identified the genes that are highly enriched in both mouse and human CGRP+ neurons. These data establish a new resource for querying the expression level of genes within specific cell types of the mouse and human trigeminal ganglia.
Conclusion
The gene expression patterns of individual mouse and human trigeminal ganglia cells were reliably described by single-cell RNA sequencing. These data enabled the discovery of novel genes that are uniquely expressed within specific trigeminal cell subtypes such as CGRP+ neurons. Future studies are aimed at investigating the role of these genes in CGRP+ neuronal function and migraine pathophysiology.
Disclosure of Interest
None Declared
Migraine Acute Therapy
OC-LB-002
Non-invasive Vagus Nerve Stimulation (nVNS) for the Acute Treatment of Migraine: A Randomised Controlled Trial
Cristina Tassorelli MD, PhD1*, Licia Grazzi MD2, Marina de Tommaso MD, PhD3, Giulia Pierangeli MD, PhD4, Paolo Martelletti MD, PhD5, Innocenzo Rainero MD, PhD6, Pierangelo Geppetti MD, PhD7, Anna Ambrosini MD, PhD8, Paola Sarchielli MD, PhD9, Eric Liebler10, Piero Barbanti MD, PhD11 and On Behalf of the PRESTO Study Group
1Headache Science Centre, National Neurological Institute C. Mondino Foundation and University of Pavia, Pavia, Italy
2Headache Center, Carlo Besta Neurological Institute and Foundation, Milano, Italy
3Neurophysiology and Pain Unit, University Aldo Moro, Bari, Italy
4IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy
5Department of Clinical and Molecular Medicine, Sapienza University, Rome, Italy
6Department of Neuroscience, University of Turin, Turin, Italy
7Headache Centre, University Hospital of Careggi, Florence, Italy
8IRCCS Neuromed, Pozzilli (IS), Italy
9Neurologic Clinic, Santa Maria della Misericordia Hospital, Blocco M, Perugia, Italy
10electroCore, LLC, Basking Ridge, New Jersey, United States
11Headache and Pain Unit, IRCCS San Raffaele Pisana, Rome, Italy
Objectives
Pilot studies and clinical experience have suggested the safety, tolerability, and preliminary efficacy of non-invasive vagus nerve stimulation (nVNS; gammaCore®) for the treatment of migraine. nVNS is an attractive option for patients, with its ease of use, flexibility, and favourable adverse event profile. We explored the efficacy, safety, and tolerability of nVNS in the acute treatment of migraine in a multicentre, double-blind, randomised, controlled trial (RCT).
Methods
248 subjects with episodic migraine with or without aura were recruited for this prospective, parallel-group study conducted at 10 Italian tertiary headache centres. Entry criteria and efficacy end points were consistent with existing guidelines and previous nVNS studies. Within 20 minutes from migraine pain onset, subjects self-administered a 120-second stimulation to the right side of the neck that was immediately followed by a 120-second stimulation on the left side. Subjects were instructed to repeat both stimulations if pain did not improve at 15 minutes, and the subjects had the option of administering a third set of stimulations at 120 minutes if not pain free. Rescue medication use before 120 minutes was considered treatment failure. Up to 5 migraine attacks were treated in the double-blind period.
Results
Acute nVNS treatment (n = 120) led to significantly higher pain-free rates than sham (n = 123) for the first treated migraine attack at 30 minutes (12.7% vs 4.2%; P = 0.012) and 60 minutes (21.0% vs 10.0%; P = 0.023), with a nearly significant difference at 120 minutes (30.4% vs 19.7%; P = 0.067; primary end point; sensitivity analysis). Due to the inconsistency between the 120-minute finding and the 2 earlier findings, a post hoc repeated-measures test was performed, confirming that nVNS was superior to sham through 120 minutes (odds ratio: 2.3; 95% CI: 1.2, 4.4; P = 0.012). nVNS was superior to sham for the rate of mild/no pain at 120 minutes (40.8% vs 27.6%; P = 0.030) and 50% responder rates for no pain (32.4% vs 18.2%; P = 0.020) and mild/no pain (47.6% vs 32.3%; P = 0.026). nVNS was extremely well tolerated as demonstrated by a low incidence of adverse effects, which were mostly mild and transient.
Conclusion
This RCT demonstrates that nVNS is rapidly effective, well tolerated, and practical for the acute treatment of episodic migraine with or without aura. nVNS was superior to sham for pain freedom at 30 and 60 minutes but not at 120 minutes (primary end point). A repeated-measures test validated the primary end point, indicating the superiority of nVNS over sham through 120 minutes. This study provides a clinical rationale for nVNS use in the acute treatment of episodic migraine.
Funding
This study was sponsored by electroCore, LLC.
Disclosure of Interest
C. Tassorelli, MD, PhD Conflict with: Research grants from the European Commission and the Italian Ministry of Health, Conflict with: Consultancy fees from Allergan S.p.A., and electroCore, LLC, Conflict with: Principle investigator or collaborator for RCTs sponsored by Alder BioPharmaceuticals Inc., Eli Lilly and Company, and Teva Pharmaceutical Industries Ltd, L. Grazzi, MD Conflict with: Consultancy and advisory fees from Allergan S.p.A., and electroCore, LLC, Conflict with: Advisory fees Allergan S.p.A., and electroCore, LLC, M. de Tommaso, MD, PhD Conflict with: Advisory fees from Allergan S.p.A., Neopharmed, and Pfizer Inc., G. Pierangeli, MD, PhD: None Declared, P. Martelletti, MD, PhD Conflict with: Research grants, advisory board fees, or travel fees from ACRAF, Allergan S.p.A., Amgen Inc., electroCore, LLC, Novartis AG, and Teva Pharmaceutical Industries Ltd., Conflict with: Advisory board fees or travel fees from ACRAF, Allergan S.p.A., Amgen Inc., electroCore, LLC, Novartis AG, and Teva Pharmaceutical Industries Ltd., I. Rainero, MD, PhD Conflict with: Research grants from the European Commission – Horizon 2020, Conflict with: Consultancy fees from electroCore, LLC, and Mylan N.V., Conflict with: Principle investigator for RCTs sponsored by Axovant Sciences Ltd., and TauRx Pharmaceuticals Ltd., P. Geppetti, MD, PhD Conflict with: Research grants from Chiesi Farmaceutici S.p.A., Conflict with: Consultancy fees from Allergan S.p.A., electroCore, LLC, Evidera, Novartis AG, Pfizer Inc., and Sanofi S.p.A., Conflict with: Principle investigator for RCTs sponsored by Eli Lilly and Company, Novartis AG, and Teva Pharmaceutical Industries Ltd., A. Ambrosini, MD, PhD Conflict with: Consultancy fees from Almirall, S.A., Conflict with: Travel grants from Allergan S.p.A., and Almirall, S.A., P. Sarchielli, MD, PhD Conflict with: Clinical study fees from Allergan S.p.A., E. Liebler Conflict with: electroCore, LLC, Conflict with: Employee of electroCore, LLC, and receives stock ownership, P. Barbanti, MD, PhD Conflict with: Consultancy fees from Allergan S.p.A., electroCore, LLC, Janssen Pharmaceuticals, Inc., Lusofarmaco, and Visufarma, Conflict with: Advisory fees from Abbott Laboratories and Merck & Co., Inc.
Headache Epidemiology, Outcomes and Burden
OC-LB-003
Factors Associated with Acute Medication Overuse in Persons with Migraine: Results from the 2017 Migraine in America Symptoms and Treatment (MAST) Study
Todd J. Schwedt1*, Aftab Alam2, Michael L. Reed3, Kristina M. Fanning3, Sagar Munjal2, Dawn C. Buse4, David W. Dodick1 and Richard B. Lipton4
1Neurology, Mayo Clinic, Phoenix
2Clinical Development, Promius Pharma, Princeton
3Vedanta Research, Chapel Hill
4Department of Neurology, Albert Einstein College of Medicine, Bronx, United States
Objectives
Overuse of prescription and OTC medications to treat migraine attacks can lead to more frequent and/or persistent migraine. Objectives were to 1) estimate rates of medication overuse (MO) in a non-clinic sample of persons with migraine; 2) determine the association of headache frequency and other variables with presence of MO.
Methods
MAST Study participants were recruited from a nationwide online research panel. Stratified random sampling identified a representative cohort aged ≥18 years meeting modified ICHD-3β criteria for migraine. Those averaging ≥1 headache days per month over prior 3 months and using acute migraine medication(s) were eligible. ICHD-3β criteria identified persons with migraine and those having MO (or not) based on their frequency of acute headache medication use. Variables of interest included sociodemographics (age, gender, race, income, BMI, education, health insurance, smoking), past 30-day headache frequency category (1–4, 5–9, 10–14, ≥15 days/month), severity (0–10 pain intensity rating), migraine symptom severity score (MSSS) sum, psychological symptomology (PHQ-4, symptom score ≥6) and presence of allodynia (ASC-12, symptom score ≥3). Binary logistic regression identified the variables associated with MO in a hierarchal manner. Odds ratios (OR) and 95% confidence intervals (CI) were calculated for each variable.
Results
117,150 responded to an email survey, 95,821responses were usable and 14,396 met inclusion criteria. Mean age was 43.4 yrs, 73.1% were women, 81.5% were Caucasian, 70.8% were employed full- or part-time. There were 2,854 (19.8%) who met criteria for MO. Covariates were entered sequentially to an initial model predicting MO as a dichotomous outcome. Headache frequency (≥15 headache days per/mo vs. 1–4 days/mo; OR 14.51, CI 12.68, 16.62), pain intensity (OR 1.17, CI 1.13, 1.21) and MSSS (OR 1.04, CI 1.02, 1.06) were associated with MO. Respondents with psychological symptomology were 58% more likely to meet criteria for MO (1.58, 95% CI 1.42, 1.76), and respondents with cutaneous allodynia were 15% more likely to meet criteria (OR 1.15, CI 1.04, 1.27). Characteristics associated with less risk of MO included Caucasian race (OR 0.80, CI 0.71, 0.90), having health insurance (OR 0.74, CI 0.63, 0.87) and not smoking (0.71, 0.63, 0.87). In prior research, females were at greater risk for allodynia and individuals with allodynia were at greater risk for MO. Thus, we hypothesized that females would have greater odds of MO. However, modeling revealed male gender was associated with increased MO (OR 1.19, CI 1.06, 1.32). To explore this unexpected finding, a final model included a sex x allodynia interaction, which was significant (OR 1.31, CI 1.05, 1.62). Men with allodynia were found to be more likely to meet MO criteria vs. women with allodynia (unadjusted percents: 30.0% and 23.6% respectively).
Conclusion
At cross-section, roughly 20% of persons with migraine met criteria for medication overuse. As expected, persons with frequent headaches were more likely to meet MO criteria. However, after adjusting for headache frequency, headache intensity, and sociodemographics, a significant association between MO and psychological distress and cutaneous allodynia remained. Being Caucasian, having health insurance and not smoking were associated with reduced risk of MO. Of note, men with allodynia were more likely to meet criteria for MO than women with allodynia. In this cross-sectional study we cannot determine temporal sequence or causality for these associations, however treating modifiable predictors of MO is likely good clinical practice.
Disclosure of Interest
T. Schwedt Conflict with: Stock options from GBS Ventures and Second Opinion and Royalties from UpToDate., Conflict with: Received grant support from the National Institutes of Health, the US Department of Defense, the Patient Centered Outcomes Research Institute, the American Migraine Foundation, Arizona State University, and the Mayo Clinic, Conflict with: Serves as a consultant, advisory board member, or has received honoraria from Allergan, Amgen, American Headache Society, Autonomic Technologies, Avanir, Dr. Reddy’s Laboratories/Promius, GBS Ventures, Novartis, Second Opinion, Supernus, and Teva., A. Alam Conflict with: Employee of Dr. Reddy’s Laboratories and owns stock in the company., M. Reed Conflict with: Received support funded by Allergan, CoLucid, Dr. Reddy’s Laboratories/Promius Pharma, Endo Pharmaceuticals, GlaxoSmithKline, Merck & Co., Inc., NuPathe, Novartis, and Ortho-McNeil, via grants to the National Headache Foundation., K. Fanning Conflict with: Received support funded by Allergan, CoLucid, Dr. Reddy’s Laboratories/Promius Pharma, Endo Pharmaceuticals, GlaxoSmithKline, Merck & Co., Inc., NuPathe, Novartis, and Ortho-McNeil, via grants to the National Headache Foundation., S. Munjal Conflict with: Employee of Dr. Reddy’s Laboratories and owns stock in the company., D. Buse Conflict with: Grant support and honoraria from Allergan, Avanir, Dr. Reddy’s Laboratories/Promius Pharma, and Eli Lilly., Conflict with: Employee of Montefiore Medical Center, which has received research support funded by Allergan, CoLucid, Endo Pharmaceuticals, GlaxoSmithKline, MAP Pharmaceuticals, Merck, NuPathe, Novartis, Ortho-McNeil, and Zogenix, via grants to the National Headache Foundation., Conflict with: Editorial Board of the Current Pain and Headache Reports, Journal of Headache and Pain, Pain Medicine News, and Pain Pathways magazine., D. Dodick Conflict with: Stock/options: GBS/Nocira, Epien, and Mobile Health., Conflict with: Consulting fees: Acorda, Allergan, Amgen, Alder, Dr. Reddy’s Laboratories/Promius Pharma, Merck, Dr Reddy’s, Promius, eNeura, Eli Lilly & Company, Insys therapeutics, Autonomic Technologies, Teva, Xenon, Tonix, Trigemina, Boston Scientific, GBS, Colucid, Zosano, Laydenburg Thalmann, Biocentric, Pfizer (Japan) Royalties: Oxford University Press and Cambridge University Press (Book Royalty) Uptodate – editorial/honoraria. CME companies honoraria/publishing honoraria/royalites: Chameleon Communications, Medscape, WebMD, Academy for Continued Healthcare Learning, Haymarket Medical Education, Global Scientific Communications, HealthLogix, Academy for Continued Healthcare Learning, Meeting LogiX, Health LogiX, Wiley Blackwell, Oxford University Press, Cambridge University Press. Consulting use agreement: NAS. Board position: King-Devick Inc., R. Lipton Conflict with: Received grant support from the National Institutes of Health, the National Headache Foundation, and the Migraine Research Fund., Conflict with: Serves as consultant, serves as an advisory board member, or has received honoraria from Alder, Allergan, American Headache Society, Autonomic Technologies, Boston Scientific, Bristol Myers Squibb, Cognimed, CoLucid, Dr. Reddy’s Laboratories/Promius, Eli Lilly, eNeura Therapeutics, Merck, Novartis, Pfizer, and Teva, Inc. He receives royalties from Wolff’s Headache, 8th Edition (Oxford University Press, 2009).
Headache Pathophysiology – Basic Science
OC-LB-004
A unique inbred rat strain with sustained cephalic hypersensitivity as a model of chronic migraine-like pain
Gordon Munro1*, Steffen Petersen1, Inger Jansen-Olesen1 and Jes Olesen1
1Danish Headache Center, Glostrup, Denmark
Objectives
Animal models of migraine-like pain enabling study of behaviour typically involve the systemic administration of vasodilators or dural administration of inflammatory algogens. However, neither method mediates sustained effects on behaviour that might be required to drive long-term pathophysiological changes within trigeminovascular pain circuits. We acquired a breeding pair of spontaneous trigeminal allodynia (STA) rats which have previously been reported to exhibit episodic, fluctuating periorbital thresholds to mechanical stimulation indicative of migraine-like pain. We wanted to perform an independent comparative behavioural and pharmacological validation of this unique inbred strain.
Methods
Experiments were performed using two generations of STA rats bred in house. A first generation (F1) of adult female STA rats were compared with adult female Sprague-Dawley (SD) rats sourced from Charles River or Taconic. A second generation (F2) of female STA rats were compared with age-matched female (SD) rats bred in house to minimize epigenetic influences on behaviour. F2 STA and control SD males were also tested. An automated von Frey algesiometer and Randall-Selitto paw pressure applicator were used to measure periorbital (left and right sides) and hindpaw sensory thresholds (g) to cutaneous mechanical stimulation respectively. A hot plate (48°C) was used to measure hindpaw latency (s) as an index of thermal sensitivity. General behaviour was evaluated using the automated behavioural registration system LABORAS.
Results
The periorbital threshold to mechanical stimulation in F1 female STA rats (74 ± 9 g, mean ± SEM, n = 14) was 2 fold lower compared with Charles River or Taconic control SD rats (159 ± 21 g, n = 10 and 181 ± 12 g, n = 13; both P < 0.001). Hypersensitivity was specific for the cephalic region and unaffected by oestrus cycle status. In F2 female STA rats (n = 17), cephalic hypersensitivity manifested shortly after puberty (Day 48 post-partum) and was sustained into early adulthood (Day 130) compared with age-matched control SD rats (n = 8); F2 male STA rats were similarly sensitive. No difference in periorbital thresholds between the left and right sides of F2 female STA rats occurred indicating that the hypersensitivity was bilateral in its distribution. Noxious thermal stimulation of the hindpaw in F2 female STA rats was performed to exclude that lack of sensitivity was not due to stimulus modality. Remarkably, they were shown to exhibit a sustained hindpaw hypoesthesia compared with control SD rats, indicative of a clear loss in sensory function. STA rats also gained weight less rapidly than age-matched SD controls, suggesting that other phenotypic differences might exist between the sub-strains. Notably, characterization of general behaviour using LABORAS revealed no obvious differences in various motor-related behaviours between F2 female STA and control SD rats. Finally, we used a blinded cross-over paradigm to test efficacy of migraine-specific drugs against cephalic hypersensitivity in F2 female STA rats. Accordingly, both the 5HT1B/1D agonist sumatriptan (1 mg/kg, s.c.) and the CGRP receptor antagonist olcegepant (1 mg/kg, i.p.) produced a robust reversal of periorbital thresholds in F2 female STA rats compared with vehicle treatment (both P < 0.001 and n = 13).
Conclusion
Periorbital thresholds to mechanical stimulation in STA rats did not fluctuate episodically as described previously. Rather, following puberty they remained lower than control SD rats and the associated hypersensitivity sustained at least into early adulthood. This unique strain appears to possess a phenotype indicative of migraine chronicity which is exquisitely sensitive to migraine therapeutics, and could prove to be an invaluable resource in preclinical migraine drug discovery.
Disclosure of Interest
None Declared
Neuromodulation for Headache
OC-LB-005
Acute treatment of migraine with e-TNS: A multi-center, double-blind, randomized, sham-controlled trial
Denise E. Chou1*, Marianna S. Yugrakh1, Giti Gross1, Dana Winegarner2, Vernon Rowe2 and Deena Kuruvilla3
1Neurology, Columbia University Medical Center, New York
2Rowe Neurology Institute, Lenexa
3Neurology, Yale University School of Medicine, New Haven, United States
Objectives
There is an unmet need for non-invasive, well-tolerated and effective acute treatments for migraine. e-TNS (external trigeminal nerve stimulation) has shown encouraging results in open-labelled pilot studies (1–3). The objective of the current study was to assess the efficacy and safety of e-TNS as an acute treatment of migraine attacks with or without aura in a multi-center, double-blind, randomized, sham-controlled trial.
Methods
Subjects aged 18 to 65 years old with a diagnosis of episodic or chronic migraine, with or without aura, were recruited if they were experiencing an acute migraine attack lasting for at least 3 hours. Eligible patients were randomized 1:1 to verum or sham stimulation and treated with e-TNS applied via the Cefaly® neurostimulator device (CEFALY Technology, Seraing, Belgium), for a 1-hour treatment session at the clinic. Patients scored their pain intensity on a visual analogue scale (0 = no pain to 10 = maximum pain). Pain level was assessed before the treatment was applied (baseline score), after the 1 h treatment, at 2 h after the beginning of the treatment phase, and at 24 h after treatment. Rescue medication intake was also recorded during the 24 h observation period. The primary outcome measure was the mean change in pain score at the 1 h time point, compared to baseline. Secondary outcome measures were the mean change in pain score at the 2 h and 24 h time points compared to baseline, as well as the proportion of patients not requiring rescue medication within 24h of treatment.
Results
106 patients were randomized and included in the intention-to-treat (ITT) analysis. The primary outcome measure (mean pain intensity after the 1 h e-TNS session compared to baseline) was significantly reduced in the verum group compared to sham (−3.46 ± 2.32 vs. −1.78 ± 1.89, p < 0.001; or −59% vs. −30%, p < 0.001). Pain intensity was also significantly reduced in the verum group compared to sham at 2 h and 24 h. Rescue medication intake within the 24 h period was not significantly lower in the verum group. 99 patients were included in a modified intention-to-treat (mITT) analysis (randomized patients who underwent the 1 h stimulation treatment and provided headache sores at baseline and at the 1 h point). Mean pain intensity was significantly reduced in the verum group compared to sham at 1 h (−3.83 ± 2.13 vs. −1.85 ± 1.89, p < 0.001; or −65% vs. −32%, p < 0.001) and at 2 h and 24 h time points. In addition, the percentage of patients who were pain-free at 24 h was significantly higher in the verum group compared to sham (32% vs. 13%, p < 0.05). Regarding safety, one minor adverse event (nausea) occurred; there were no serious adverse events, nor were any subjective complaints or side effects reported in either group within the 24 h period.
Conclusion
The results of this multi-center, double-blind, randomized, sham-controlled trial demonstrate that e-TNS is an effective and well-tolerated treatment for the acute treatment of migraine.
*
Disclosure of Interest
D. Chou Conflict with: outside the submitted work: research funding from Teva, Alder, and Capnia, Conflict with: advisory boards: Eli Lilly, Amgen, Teva, Allergan, and Pernix, Conflict with: speaking honorarium from Medscape, M. Yugrakh: None Declared, G. Gross: None Declared, D. Winegarner: None Declared, V. Rowe: None Declared, D. Kuruvilla: None Declared
References:
1. Gérardy PY, Fabry D, Fumal A, Schoenen J. A pilot study on supra-orbital surface electrotherapy in migraine. Cephalalgia 2009;29(1):134
2. Kozminski M. Transcutaneous supraorbital nerve stimulation as a rescue therapy. Headache 2014;54(S1):12
3. Chou DE, Gross GJ, Casadei C, Yugrakh MS. External trigeminal nerve stimulation for the acute treatment of migraine: open-label trial on safety and efficacy. Neuromodulation 2017 Jun 5.
Headache Pathophysiology – Basic Science
OC-LB-006
TRPA1 and not TRPV1 activation inhibited by aspirin in human volunteers
Linde Buntinx1*, Sergio Barroso1, Joyce Vandendriessche1, Lin Chang1, Bart Morlion2 and Jan de Hoon1
1Center for Clinical Pharmacology, Department of Pharmaceutical and Pharmacological Sciences
2Leuven Center for Algology, Department of Cardiovascular Sciences, KU Leuven, Leuven, Belgium
Objectives
Transient receptor potential ankyrin 1 (TRPA1), an emerging target for migraine therapy, is activated by cinnamaldehyde (CA) and results in a reproducible increase in dermal blood flow (DBF) after local CA application1. This study investigates the mediators involved in this response in healthy volunteers.
Methods
DBF expressed as AUC from baseline until 60 min post-challenge

Results
Part I: After aspirin intake, CA-induced DBF was almost completely blocked (p < 0.001), in contrast to aprepitant, when comparing to no drug intake.
Part II: Inhibition of CA-induced DBF response by aspirin was confirmed (p < 0.001), compared to no drug intake. Additionally, indomethacin was also able to reduce the DBF response (p < 0.05), while celecoxib was not, compared to no drug intake. Interestingly, a difference was also found between aspirin and indomethacin p < 0.05), indicating that aspirin is a stronger inhibitor. Capsaicin-induced DBF was not reduced by intake of any drug, compared to no drug intake.
Conclusion
In healthy volunteers, COX-1 dependent vasodilating prostaglandins play an important role in CA-induced DBF and thus TRPA1 activation, while COX-2 and Substance P do not seem to contribute substantially to the response.
These results are of interest because:
(1) In mice, prostaglandins were reported not to play a role in CA-induced DBF2, which contributes to the emerging hypothesis that there are striking differences between human and rodent TRPA1 homologues complicating TRPA1-targeted drug discovery;
(2) Although both aspirin and indomethacin are both non-selective cox-inhibitors, aspirin seems to have a stronger inhibitory effect on CA-induced DBF, maybe since aspirin is an irreversible inhibitor and indomethacin is not;
(3) Although both TRPA1 and TRPV1 are reported to be co-expressed on the same peptidergic nerve endings, the vasodilatation induced via their activation seems to be induced by different second messengers.
Disclosure of Interest
None Declared
References
1. Buntinx L et al. Development of an in vivo target-engagement biomarker for TRPA1 antagonists in humans. Br J Clin Pharmacol 2016.
2. Aubdool AA et al. TRPA1 activation leads to neurogenic vasodilatation: involvement of reactive oxygen nitrogen species in addition to CGRP and NO. Br J Pharmacol 2016; 173: 2419–33.
Migraine Preventive Therapy
PO-01-178
A Randomized Pilot Study of Nuedexta® for the Prevention of Episodic Migraine
Ryan J. Cady1*, Timothy R. Smith1, Heather R. Manley1, Jim S. Sly1 and Roger K. Cady2
1Clinvest Research, Springfield
2Alder BioPharmaceuticals, Inc., Bothell, United States
Objectives
Nuedexta® (dextromethorphan and quinidine) is a potent NMDA and Sigma-1 receptor antagonist with high CNS availability and a long half-life which can potentially inhibit glutamate activity in the nervous system. Glutamate is one of the most potent excitatory neuropeptides in the nervous system and is a precursor to gamma-amino-butyric acid (GABA). Glutamate binds with the N-methyl-D-aspartate (NMDA) receptor to open ion channels and increase CNS excitability. Inhibition of the NMDA receptor has been shown to block pain transmission and has been implicated in migraine pathophysiology, peripheral and central sensitization as well as cortical spreading depression. The less studied Sigma-1 receptor is involved in calcium signaling and is implicated in pain processing. This pilot study explores the potential of daily Nuedexta® in reducing the frequency of frequent episodic migraine.
Methods
This was a double-blind, placebo-controlled, randomized study conducted at 6 centers. Forty-five subjects, 18 to 65 years of age, with frequent episodic migraine (6–14 days per month), with or without aura as defined by ICHD-3beta, entered a 4 week baseline period to confirm the diagnosis and establish baseline migraine characteristics. Subjects could maintain other current stable migraine prophylaxis throughout the study. Eligible subjects were randomized in a 1:1 ratio to daily Nuedexta® or Placebo for 16 weeks, completing daily electronic headache diaries and returned monthly for evaluations.
Results
A comparison of the number of headache days from the baseline month to each of the treatment period months between the Nuedexta® arm vs. the placebo arm revealed a significant interaction effect, F(3, 105) = 4.51, p = .01, η2p = .11. Subjects randomized to Nuedexta® (n = 20) reported a significantly greater reduction in headache days (−3.4 days, p < .001) during treatment weeks 12–16 while there was no significant change for those receiving placebo (−0.52 days, p = .69). A similar trend was seen with a significantly greater reduction in the number of migraine days for those receiving Nuedexta® (−2.95 days, p < .001) vs. placebo (−0.72 days, p = .57). Half of the subjects in the Nuedexta® arm (10/20) reported at least a 50% reduction in the number of migraines at the end of treatment, which was statistically significant compared to the placebo arm (3/17, p = .04) in the placebo arm. Subjects in the Nuedexta® arm reported significantly higher Headache Health Scores ™ compared to baseline during all treatment periods, while subjects in the placebo arm reported no significant change in Headache Health Scores™ during any of the treatment periods. A post-hoc analysis of subjects receiving Nuedexta® comparing the change in headache days from baseline to treatment weeks 12–16 showed an average decrease of −4.29 headache days in those with a history of migraine with aura compared to an average decrease of −2.92 headache days in those with a history of migraine without aura. Nuedexta® was well tolerated with the most common adverse event being nausea (5%).
Conclusion
Data from this pilot study suggests Nuedexta® may have benefit for the prevention of episodic migraine. Subjects reported fewer migraine and headache days, as well as significant increases in Headache Health Scores™ indicative of overall improvements for subjects’ quality of life. These data further support a potential role of glutamate in the pathophysiology of migraine. Few adverse events were reported with Nuedexta® relative to placebo. These positive results suggest the need for larger additional studies on the role of NMDA receptor antagonists and sigma-1 antagonists in the prevention of episode and chronic migraine.
Disclosure of Interest
R. Cady Conflict with: Research Grant, T. Smith: None Declared, H. Manley: None Declared, J. Sly: None Declared, R. Cady: None Declared
Migraine Preventive Therapy
PO-01-179
Erenumab Reduces Weekly Migraine Days in Patients With Episodic Migraine During the First Week of Administration
Uwe Reuter1*, Gregor Broessner2, Todd J. Schwedt3, David Kudrow4, Elizabeth Leroux5, Thuy Vu6, Feng Zhang7, Hernan Picard7, Robert A. Lenz7 and Daniel D. Mikol7
1Charité Universitätsmedizin, Berlin, Germany
2Medizinische Universität Innsbruck, Innsbruck, Austria
3Mayo Clinic, Phoenix, AZ
4California Medical Clinic for Headache, Santa Monica, CA, United States
5South Health Campus, University of Calgary, Calgary, AB, Canada
6Amgen Inc., Thousand Oaks
7Amgen Inc., Thousand Oaks, CA, United States
Objectives
Subcutaneous erenumab, a fully human monoclonal antibody against the CGRP receptor, significantly reduces headache frequency in patients with episodic migraine. Here, we evaluated the response to erenumab 70 mg and 140 mg administered by subcutaneous injection from baseline through 2 weeks in reducing migraine days in patients with episodic migraine (≥4 and <15 headache days per month).
Methods
This post hoc analysis of a phase 3, randomized, double-blind, placebo-controlled clinical trial of erenumab (NCT02456740) evaluated: 1) the proportion of subjects with ≥50% reduction in weekly migraine days and 2) the percentage of subjects with migraine days each day during the first 2 weeks of treatment. Stratified Cochran-Mantel-Haenszel with nonresponder imputation was used for ≥50% responder rates. To visualize trend in daily migraine rate, a 7-day moving average of the observed percentages of patients experiencing a migraine day was calculated with a centering method. Nominal p-values are reported without multiplicity adjustment.

Results
Baseline mean weekly migraine days was 2.1 days for all treatment arms. At week 1, 28% of patients on placebo (n = 316) had ≥50% reduction in weekly migraine days compared to 34% receiving erenumab 70 mg (n = 312; P = 0.097) and 43% receiving erenumab 140 mg (n = 318; P < 0.001), increasing to 30%, 45%, and 47%, for placebo, 70 mg, and 140 mg, respectively, at week 2 (P < 0.001 for both 70 mg and 140 mg vs placebo). Moreover, the percentage of patients experiencing a migraine day was lower for the erenumab groups within several days after initiation of treatment, supporting that the onset of erenumab efficacy occurs within the first week of treatment, earlier for the 140 mg dose than for the 70 mg dose (Figure).
Conclusion
Among patients with episodic migraine, efficacy is observed within the first week of erenumab treatment. These results are similar to those reported for patients with chronic migraine, and taken together suggest that erenumab has a rapid onset of efficacy in patients with migraine.
Disclosure of Interest
U. Reuter Conflict with: Allergan, Amgen Inc., Eli Lilly & Co., Novartis, TEVA, Conflict with: Allergan, Amgen Inc., Eli Lilly & Co., Novartis, TEVA, G. Broessner Conflict with: OGN, EHF, Conflict with: Novartis, Pfizer, Allergan, Reckitt Benkiser, Conflict with: Novartis, Pfizer, Allergan, Reckitt Benkiler, Linde AG, T. Schwedt Conflict with: Nocira, Second Opinion, Conflict with: Allergan, Amgen, ATI, Avanir, Dr. Reddys, Nocira, Novartis, Conflict with: Nocira, UpToDate, Board of Directors American Headache Society, D. Kudrow Conflict with: Eli Lilly & Co., Amgen, Alder, E. Leroux Conflict with: Allergan, Conflict with: Eli Lilly & Co., Tribute/Aralez, Teva, Allergan, Novartis, T. Vu Conflict with: Amgen Inc., Conflict with: Amgen Inc., F. Zhang: None Declared, H. Picard Conflict with: Amgen Inc., Conflict with: Amgen Inc., R. Lenz Conflict with: Amgen Inc., Conflict with: Amgen Inc., D. Mikol Conflict with: Amgen Inc., Conflict with: Amgen Inc.
Migraine Preventive Therapy
PO-01-180
Efficacy of Erenumab (a fully human Mab targeting the CGRP receptor) in Chronic Migraine Patients with Prior Treatment Failure: a Subgroup Analysis of the Phase 2, Randomized, Double-Blind, Placebo-Controlled Study
Messoud Ashina1, Stewart Tepper2, Jan L. Brandes3, Uwe Reuter4*, Guy Boudreau5, David Dolezil6, Sunfa Cheng7, Dean Leonardi7, Robert Lenz7, Jan Klatt8 and Daniel Mikol7
1Danish Headache Center and Dept. of Neurology, University of Copenhagen, Copenhagen, Denmark
2Geisel School of Medicine at Dartmouth, Hanover
3Nashville Neuroscience Group and Dept. of Neurology, Vanderbilt University, Nashville, United States
4Dept. of Neurology, Charité Universitätsmedizin Berlin, Berlin, Germany
5Headache Unit, Neurology Dept., University Hospital Center of Montreal, Montreal, Canada
6Prague Headache Center, DADO MEDICAL s.r.o.,, Prague, Czech Republic
7Amgen Inc., California, United States
8Novartis Pharma AG, Basel, Switzerland
Objectives
To present results on prior prophylactic treatment failure (≥1, ≥2 and never failed) due to lack of efficacy and/or poor tolerability from a pre-specified subgroup analysis of the Ph 2 study of erenumab in patients with chronic migraine (CM).
Methods
Outcome measures

Results
With erenumab 70 mg and 140 mg, there were greater reductions at week 12 in MMD and more patients achieved ≥50% reduction in MMD vs Pbo across subgroups. Greater reduction in monthly acute MSMTDs was observed with erenumab 70 mg and 140 mg in patients who failed prophylactic medications vs Pbo. Cumulative monthly headache hours reduced with erenumab 140 mg vs Pbo in patients who failed prophylactic medications. Pbo effect was greatest in patients who never failed prophylactic medication. Across endpoints, reductions were greater with erenumab 140 mg than 70 mg.
Conclusion
Erenumab 140 mg showed better efficacy in patients who had failed ≥1 or ≥2 prophylactic medications.
Disclosure of Interest
M. Ashina Conflict with: Allergan, Amgen, Alder, ATI, and Eli Lilly, Conflict with: primary investigator — Amgen 20120178 (Phase 2), 20120295 (Phase 2), 20130255 (open-label extension), 20120297 (Phase 3), and GM-11 gamma-Core-R trials., S. Tepper Conflict with: ATI, Conflict with: Allergan, Amgen, ATI, Avanir, ElectroCore, eNeura, Teva, Zosano, Conflict with: Acorda, Allergan, Amgen, ATI, Avanir, Depomed, ElectroCore, eNeura, Impax, Kimberly-Clark, Pfizer, Scion NeuroStim, Teva, Zosano, Conflict with: Cleveland Clinic during this study, Conflict with: 2015 only — Allergan, Depomed, Impax, Pernix, Teva, Conflict with: advisory board — Alder, Allergan, Amgen, ATI, Acorda, Dr. Reddy’s, Kimberly-Clark, Teva, Pfizer, Zosano; salary — American Headache Society; royalties — University of Mississippi Press, Springer., J. Brandes Conflict with: consulting fees, speaking fees, and/or research grants: Allergan, Amgen, Avanir, Depomed, Clinvest, Daiichi Sankyo, Pernix, Merck, Supernus, Teva, Arteaus, and Eli Lilly., U. Reuter Conflict with: consulting fees, speaking/teaching fees, and/or research grants: Allergan, Amgen, Autonomic Technologies, CoLucid, ElectroCore, Novartis, Pharm Allergan, G. Boudreau Conflict with: Teva, Eli Lilly, Amgen, Allergan, Conflict with: Allergan, Novartis, D. Dolezil Conflict with: consulting fees, and speaking and/or teaching fees: Allergan, Amgen, Biogen Idec, Novartis, Bayer, and Teva., S. Cheng Conflict with: Amgen, Conflict with: Amgen, D. Leonardi Conflict with: Amgen, Conflict with: Amgen, R. Lenz Conflict with: Amgen, Conflict with: Amgen, J. Klatt Conflict with: Novartis, Conflict with: Novartis, D. Mikol Conflict with: Amgen, Conflict with: Amgen
Migraine Preventive Therapy
PO-01-181
The Impact of Fremanezumab on Migraine-Specific Health-Related Quality of Life and Overall Health Status in Chronic Migraine
Richard B. Lipton1*, Sanjay K. Gandhi2, Timothy Fitzgerald2, Paul P. Yeung2, Joshua M. Cohen2, Ronghua Yang2 and Ernesto Aycardi2
1Albert Einstein College of Medicine, New York
2Teva Pharmaceutical Industries, Frazer, United States
Objectives
Migraine is the sixth most disabling condition globally. Due to frequent attacks, chronic migraine (CM) adversely affects health-related quality of life (HRQoL). In clinical trials, fremanezumab, a fully humanized monoclonal antibody that selectively targets calcitonin gene-related peptide, reduced the frequency, severity, and duration of headaches in patients with CM. This study measured HRQoL using the Migraine-Specific Quality of Life (MSQoL) questionnaire and health status using the EuroQol 5-dimension 5 response level (EQ-5D-5L) questionnaire. We used these measures to compare outcomes in patients treated with fremanezumab versus placebo.
Methods
In this multicenter, randomized, double-blind, placebo-controlled study, patients with CM were randomized 1:1:1 to receive subcutaneous injections of fremanezumab quarterly dosing (675 mg at baseline and placebo at Weeks 4 and 8), fremanezumab monthly dosing (675 mg at baseline and 225 mg at Weeks 4 and 8), or placebo at each time point over a 12-week treatment period. The MSQoL questionnaire (version 2.1) assessed three domains: the role function-restrictive domain (RR), the role function-preventive domain (RP), and the emotional function (EF) domain. Scores range from 0 to 100, with higher scores indicating better HRQoL. Health status was measured using the EQ-5D-5L questionnaire, which allows patients to report their general health status on a visual analog scale (VAS, range from 0 to 100, with higher scores indicating better health). We assessed mean change from baseline (Day 0) in MSQoL domains using a mixed-effects repeated-measures model (with years since onset of migraine and baseline MSQoL domain score as covariates). EQ-5D-5L analyses were conducted using an analysis of covariance approach (with years since onset of migraine and baseline EQ-5D-5L score as covariates).
Results
The study included 375 patients in each of the fremanezumab treatment arms and 371 in the placebo arm. Compared with placebo, fremanezumab significantly improved MSQoL scores in patients with CM. The mean MSQoL score in the RR domain for each fremanezumab dose regimen was significantly increased versus placebo, from baseline to Week 12 (least-squares mean [LSM] ± standard error [SE] differences versus placebo: 5.6 ± 1.4 in the quarterly fremanezumab group and 6.3 ± 1.4 in the monthly fremanezumab group; both P < 0.0001). Significant (P < 0.05) improvements in the RP and EF domains of MSQOL were also observed. Significant improvements in each domain of MSQOL were observed as early as 4 weeks after the first dose and was sustained at all pre-defined assessments in the fremanezumab groups. As measured by the EQ-5D-5L VAS, patients with CM experienced statistically significant improvement in overall health status with fremanezumab quarterly (4.6 ± 1.1; P = 0.0402) and monthly (4.8 ± 1.1; P = 0.0291) dosing as compared with placebo (2.2 ± 1.1).
Conclusion
These results indicate that fremanezumab improves migraine-specific QoL and overall health status of patients with CM. These improvements highlight the positive impact of fremanezumab on CM patients’ ability to engage in and perform work and daily activities.
Disclosure of Interest
R. Lipton Conflict with: Teva, S. Gandhi Conflict with: Teva Pharmaceutical Industries, T. Fitzgerald Conflict with: Teva Pharmaceutical Industries, P. Yeung Conflict with: Teva Pharmaceutical Industries, J. Cohen Conflict with: Teva Pharmaceutical Industries, R. Yang Conflict with: Teva Pharmaceutical Industries, E. Aycardi Conflict with: Teva Pharmaceutical Industries
Migraine Preventive Therapy
PO-01-182
The Positive Impact of Fremanezumab on Work Productivity and Activity Impairment in Patients With Chronic Migraine
Richard B. Lipton1*, Sanjay K. Gandhi2, Timothy Fitzgerald2, Paul P. Yeung2, Joshua M. Cohen2, Ronghua Yang2 and Ernesto Aycardi2
1Albert Einstein College of Medicine, New York
2Teva Pharmaceutical Industries, Frazer, United States
Objectives
Migraine is a debilitating chronic disease that imparts a substantial indirect cost burden on corporations. The management and treatment of migraine costs US employers approximately $12 billion annually in productivity loss and accounts for up to 70–90% of total migraine-related annual costs. Chronic migraine (CM) creates an especially high societal burden. In clinical trials, fremanezumab, a fully humanized monoclonal antibody that selectively targets calcitonin gene-related peptide, reduced the frequency, severity, and duration of headaches in patients with CM. The purpose of this analysis was to evaluate the effect of subcutaneous fremanezumab on work productivity loss and activity impairment in patients with CM, as measured by the Work Productivity and Activity Impairment (WPAI) questionnaire.
Methods
In this Phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group study (NCT02621931), eligible patients aged 18–70, with a history of migraine (≥12 months) and prospectively confirmed CM (≥15 headache days and ≥8 migraine days per month), were randomized 1:1:1 to receive subcutaneous injections of fremanezumab quarterly dosing (675 mg at baseline and placebo at Weeks 4 and 8), fremanezumab monthly dosing (675 mg at baseline and 225 mg at Weeks 4 and 8), or placebo at each time point over a 12-week treatment period. Change in WPAI score from baseline to 4 weeks after administration of the last dose of study drug was an exploratory endpoint. The WPAI questionnaire includes questions regarding the impact of health on the extent of work loss and productivity impairment during work and other activities, with higher scores indicating greater impairment.
Results
The full analysis set included 375 patients in each of the fremanezumab dosage groups and 371 patients in the placebo group. Patients with CM treated with fremanezumab reported larger reductions from baseline in overall work productivity loss (composite of absenteeism and impairment while working [presenteeism]) compared with placebo (–16.6% ± 2.09% [quarterly] and −15.9% ± 2.02% [monthly] vs −9.1% ± 2.02% [placebo]), resulting in significant treatment differences for each fremanezumab treatment arm versus placebo (quarterly: −7.5% ± 2.24%, P = 0.0009; monthly: −6.8% ± 2.26%, P = 0.0026). The change from baseline in presenteeism was greater with fremanezumab than with placebo (–15.7% ± 1.89% [quarterly] and −14.9% ± 1.82% [monthly] vs −10.0% ± 1.82% [placebo]), resulting in significant treatment differences for each fremanezumab treatment arm versus placebo (quarterly: −5.7% ± 2.03%, P = 0.0049; monthly: −4.9% ± 2.05%, P = 0.0169). In addition, fremanezumab significantly reduced impairment of activity outside of work in the quarterly dosing arm of the study compared with placebo (–15.0% ± 1.70% vs −11.0% ± 1.7%; treatment difference of −4.0% ± 1.85%, P = 0.0311).
Conclusion
In this Phase III study, fremanezumab treatment resulted in significant improvements in work productivity and activity impairment, demonstrating the positive impact of fremanezumab on the ability of patients with CM to function both at and outside of work.
Disclosure of Interest
R. Lipton Conflict with: Teva, S. Gandhi Conflict with: Teva Pharmaceutical Industries, T. Fitzgerald Conflict with: Teva Pharmaceutical Industries, P. Yeung Conflict with: Teva Pharmaceutical Industries, J. Cohen Conflict with: Teva Pharmaceutical Industries, R. Yang Conflict with: Teva Pharmaceutical Industries, E. Aycardi Conflict with: Teva Pharmaceutical Industries
Migraine Preventive Therapy
PO-01-183
Early Onset of Action of Fremanezumab (TEV-48125) Versus Placebo by the First Week for the Preventive Treatment of Chronic Migraine
Paul Yeung1*, Ernesto Aycardi1, Marcelo Bigal1, Tricia Blankenbiller1, Melissa Grozinski-Wolff1, Yuju Ma1 and Jan Brandes2
1Teva Pharmaceuticals, Malvern
2Nashville Neuroscience Group, Nashville, United States
Objectives
Migraine is a prevalent disease which may progress over time. Migraine prevention is intended to reduce the frequency, severity, and disability associated with migraine attacks, and faster onset of action could increase the benefit to patients with migraine. Fremanezumab is a fully humanized monoclonal antibody targeting the calcitonin gene-related peptide (CGRP) ligand, a preventive treatment designed to specifically target a pathophysiologic mechanism of migraine. This analysis assesses the onset of action of fremanezumab in the prevention of migraine.
Methods
This is a 16-week, multicenter, randomized, double-blind, placebo-controlled, parallel-group study to compare the efficacy, safety, and tolerability of 2 subcutaneous dose regimens of fremanezumab and placebo (PBO) in adults with CM. Patients maintained a daily diary during a 28-day baseline period, and throughout the treatment period. Patients were assigned randomly to 1:1:1 ratio to 1 of 3 treatment groups: (1) monthly dosing: an initial dose of 675 mg fremanuzemab followed by 225 mg of fremanezumab at months 2 and 3, (2) quarterly dosing: a single dose of 675 mg of fremanuzemab at month 1, followed by placebo injections at months 2 and 3, and (3) monthly administration of matching placebo. The mean change from baseline (28-day run-in period) to the 12-week randomization period in the monthly average number of migraine days the primary endpoint in the EM study and secondary endpoint in CM study, and results at Weeks 1, 2, 3 and 4 were also assessed using a mixed-effect model for repeated measures.
Results
Chronic migraine with fremanezumab experienced statistically significant reduction in the number of monthly headache days of at least moderate severity during the 12-week period after 1st dose, for both dosing regimens [monthly (−4.6 days) and quarterly (−4.3 days); p < 0.0001] vs. placebo (−2.5 days), and during the 4 week period after 1st dose, for both dosing regimens (p < 0.0001). At Week 1, fremanezumab resulted in significant reduction in the weekly number of headache days of at least moderate severity (−1.1 days; p < 0.0001) versus placebo (−0.5 days). At Week 2, fremanezumab resulted in significant reduction in the weekly number of headache days of at least moderate severity (−1.2 days; p < 0.0001) versus placebo (−0.5 days). At Week 3, fremanezumab resulted in significant reduction in the weekly number of headache days of at least moderate severity (−1.2 days; p < 0.0001) versus placebo (−0.6 days). At Week 4, fremanezumab resulted in significant reduction in the weekly number of headache days of at least moderate days (−1.1 days; p = 0.0006) versus placebo (−0.7 days). Posthoc analysis indicated that more patients reported no headache of at least moderate severity with fremanezumab (69%; p = 0.0036) versus placebo (61%) by the next day after the first injection.
Conclusion
These results indicate that the onset of action with fremanezumab occurred rapidly for the preventive treatment of migraine. The significant improvement was maintained throughout three months of treatment for both monthly and quarterly subcutaneous injections.
Disclosure of Interest
P. Yeung Conflict with: Teva Pharmaceuticals, E. Aycardi Conflict with: Teva Pharmaceuticals, M. Bigal Conflict with: Teva Pharmaceuticals, T. Blankenbiller Conflict with: Teva Pharmaceuticals, M. Grozinski-Wolff Conflict with: Teva Pharmaceuticals, Y. Ma Conflict with: Teva Pharmaceuticals, J. Brandes Conflict with: Teva Pharmaceuticals
Migraine Preventive Therapy
PO-01-184
A Phase 3, Long-Term, Open-Label Safety Study of Self-Administered Galcanezumab Injections in Patients with Migraine
Virginia L. Stauffer1, Ryan Sides1, Angelo Camporeale1, Vladimir Skljarevski1, Jonna Ahl1 and Sheena K. Aurora1
1Eli Lilly and Company, Indianapolis, United States
Objectives
To evaluate the long-term safety and tolerability of galcanezumab (GMB), a humanized monoclonal antibody that selectively binds to the calcitonin gene-related peptide, for up to 1 year of treatment in patients with migraine.
Methods
Patients 18–65 years of age, who were diagnosed with migraine (including chronic migraine) and without prior exposure to GMB, were randomized 1:1 to open-label treatment with GMB 120 mg, with an initial loading dose of 240 mg, or GMB 240 mg given subcutaneously once monthly for 12 months. The initial dose of GMB was administered by site personnel, and subsequent doses were self-administered with a pre-filled syringe or autoinjector. Safety and tolerability were assessed by the incidence of serious adverse events (SAEs), treatment-emergent adverse events (TEAEs), and adverse events leading to study discontinuation (DCAEs). Pertinent laboratory values, vital signs, electrocardiograms (ECGs), and suicidality, assessed by the Columbia-Suicide Severity Rating Scale, were analyzed. In addition, change from baseline in the number of monthly migraine headache days (MHD), functioning (assessed by the Migraine Specific Quality of Life Role Function-Restrictive), and disability (assessed by Migraine Disability Assessment) were evaluated.
Results
One hundred thirty-five patients were randomized to each dose group. Most of the patients were female (>80%), with an average age of 42 years, and had an average of 10.6 MHD per month at baseline. Overall, 77.8% of the patients completed the study, and 4.8% discontinued due to AEs. The TEAEs reported in ≥10% of patients in the combined dose groups included injection site pain, nasopharyngitis, upper respiratory tract infection, injection site reaction, back pain, and sinusitis. The incidence of TEAEs and DCAEs were not significantly different between the two doses. There were 10 SAEs, each of which occurred once, 3 in the 120 mg group and 7 in the 240 mg group. Overall, there were no clinically meaningful differences between GMB doses in laboratory values, vital signs, or ECGs. None of the patients reported suicidal behavior, but 1 patient did discontinue due to suicidal ideation in the GMB 120 mg group. The overall least squares mean change in monthly MHD over 12 months for GMB 120 mg was −5.6 and for GMB 240 mg was −6.5. In addition, level of functioning was improved, and disability was reduced in both dose groups.
Conclusion
Treatment with self-administered GMB was safe and associated with reduction in the number of monthly MHD over 1 year of treatment. Overall, there were no clinically meaningful differences in tolerability and safety for GMB 120 mg compared to GMB 240 mg.
This study is registered as NCT02614287 at ClinicalTrials.gov.
Disclosure of Interest
V. Stauffer Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, R. Sides Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, A. Camporeale Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, V. Skljarevski Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, J. Ahl Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, S. Aurora Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company
Migraine Preventive Therapy
PO-01-185
A Multicenter, Prospective, Randomized, Open-label Study to Compare the Efficacy, Safety, and Tolerability of OnabotulinumtoxinA and Topiramate for Headache Prophylaxis in Adults with Chronic Migraine: The FORWARD Study
John F. Rothrock1*, Aubrey Manack Adams2, Esther Jo2, Xiang Zhao3 and Andrew M. Blumenfeld4
1George Washington School of Medicine, Washington DC
2Allergan plc, Irvine
3Pharmaceutical Product Development, LLC, Austin
4Headache Center of Southern California, The Neurology Center, Carlsbad, United States
Objectives
To compare the efficacy, safety and tolerability of onabotulinumtoxinA and topiramate for preventive treatment of chronic migraine (CM) in adults.
Methods
The FORWARD Study (ClinicalTrials.gov, NCT02191579) is a multicenter, randomized, parallel-group, prospective study. Adults with CM were randomized (1:1 ratio) to receive either 155 U of onabotulinumtoxinA (31 sites in a fixed-site, fixed-dose paradigm across 7 head/neck muscles) every 12 weeks (±7 days) for 3 treatment cycles or 50–100 mg/day of topiramate administered daily up to week 36. Patients who discontinued topiramate crossed over to receive onabotulinumtoxinA no earlier than 12 weeks and up to 3 treatment cycles. Patients recorded frequency, duration, and severity of headache, acute medication use, and interictal burden daily using an electronic diary. Other measures were assessed at follow-up clinic visits. The primary efficacy measure was a dichotomous variable (responder/nonresponder) defined as the proportion of patients with ≥50% reduction in headache day frequency during the 28-day period before week 32 (weeks 29–32). Analyses were performed on the ITT dataset using logistic regression. A worst-case imputation method was utilized to impute missing data; this replaces the missing value with the baseline value if the responder rate was missing at week 32 for any reason. Adverse events (AE) were monitored. Presented efficacy data are based on the week 32 assessment (weeks 29–32) whereas the safety data include AEs from randomization and cross-over phases.
Image
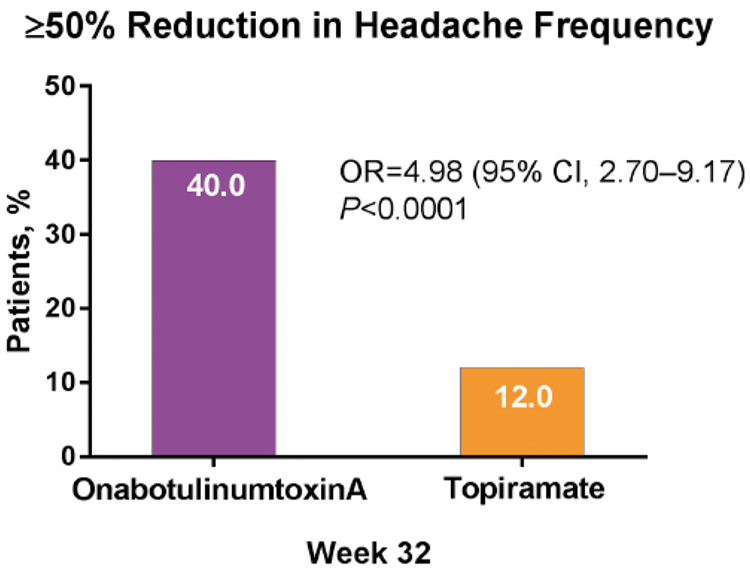
Efficacy of OnabotulinumtoxinA or Topiramate as Assessed by ≥50% Reduction in Headache Frequency from Baseline
Results
282 patients were enrolled (onabotulinumtoxinA n = 140; topiramate n = 142) at 35 US sites. Patients were primarily female (n = 239, 84.8%) and white (n = 229, 81.2%); baseline demographics and mean (SD) baseline headache days (onabotulinumtoxinA, µ = 22.1 [ ± 4.6]; topiramate, µ = 21.8 [±4.8]) were similar across treatment groups. The primary reasons for withdrawal were ineffective treatment (onabotulinumtoxinA, n = 7 [5.0%]; topiramate, n = 28 [19.7%]) and adverse effects (onabotulinumtoxinA, n = 5 [3.6%]; topiramate, n = 72 [50.7%]). 80 topiramate patients crossed over to onabotulinumtoxinA through the week-32 assessment. OnabotulinumtoxinA treatment demonstrated significantly higher proportion of patients with a ≥50% reduction in headache frequency at the week-32 assessment compared to baseline vs topiramate (40.0% vs 12.0%, respectively; OR, 4.98 [95% CI, 2.70–9.17]; P < 0.0001; Figure). Treatment-related AEs were reported by 17.7% and 69.0% of onabotulinumtoxinA and topiramate patients, respectively. One serious AE (nephrolithiasis) for topiramate was reported as related.
Conclusion
In this open-label study, preventive treatment of adults with CM with onabotulinumtoxinA demonstrated more favorable tolerability and was significantly more effective than topiramate.
Disclosure of Interest
J. Rothrock Conflict with: George Washington School of Medicine, Conflict with: Allergan-sponsored educational programs, A. Manack Adams Conflict with: Allergan plc, Conflict with: Allergan plc, E. Jo Conflict with: Allergan plc, X. Zhao Conflict with: Pharmaceutical Product Development, LLC has contracts with Allergan plc and other companies, Conflict with: Pharmaceutical Product Development, LLC, A. Blumenfeld Conflict with: Allergan, Pernix, Teva, Avanir, Depomed, Supernus, Conflict with: Allergan
Migraine Preventive Therapy
PO-01-186
The Impact of Fremanezumab on Headache-Related Disability in Patients With Chronic Migraine Using the Headache Impact Test (HIT-6)
Paul K. Winner1*, Timothy Fitzgerald2, Sanjay K. Gandhi2, Paul P. Yeung2, Joshua M. Cohen2, Ronghua Yang2 and Ernesto Aycardi2
1Palm Beach Neurology, West Palm Beach
2Teva Pharmaceutical Industries, Frazer, United States
Objectives
Patients with chronic migraine (CM) experience substantially impaired daily functioning and reduced quality of life, with the occurrence of daily or near-daily headache attacks. In clinical trials, fremanezumab, a fully humanized monoclonal antibody that selectively targets calcitonin gene-related peptide, reduced the frequency, severity, and duration of headaches in patients with CM. The impact of migraine cannot be fully understood only by assessment of the frequency of headaches. The 6-item Headache Impact Test (HIT-6) is a validated tool used to measure headache-related disability. This study uses HIT-6 to assess the effect of fremanezumab versus placebo on headache-related disability.
Methods
In this multicenter, randomized, double-blind, placebo-controlled, Phase III study, eligible patients with CM were randomized 1:1:1 to receive subcutaneous injections of fremanezumab quarterly dosing (675 mg at baseline and placebo at Weeks 4 and 8), fremanezumab monthly dosing (675 mg at baseline and 225 mg at Weeks 4 and 8), or placebo at each time point over a 12-week treatment period. As a secondary endpoint, change in HIT-6 score was evaluated from baseline (Day 0) to 4 weeks after administration of the last dose of study drug. HIT-6 scores range from 36 to 78, with higher scores indicating a greater impact of headache on the daily life of the respondent. Efficacy analyses for primary and secondary endpoints were performed in the full analysis set (FAS; all randomized patients who received at least one dose of study drug and had at least 10 days of post-baseline efficacy assessments on the primary endpoint) and repeated for the per-protocol analysis set (PPS; all patients who completed the study without violation of eligibility criteria or omission of drug administration). The data were analyzed using the analysis of covariance approach, with baseline HIT-6 score and years since onset of migraine used as covariates.
Results
Treatment with both fremanezumab dose regimens yielded significant improvements in disability, as measured by the reductions in HIT-6 scores from baseline to 4 weeks after administration of the last study dose. In the FAS, the least-squares mean ± standard error changes from baseline with fremanezumab quarterly (−6.4 ± 0.45 points) and (−6.8 ± 0.44 points) monthly dosing were larger than with placebo (−4.5 ± 0.45 points); this resulted in significant differences in HIT-6 score change from baseline for fremanezumab treated patients versus placebo (quarterly: −1.9 ± 0.49 points, P = 0.0004; monthly: −2.4 ± 0.49 points, P < 0.0001). Similar treatment differences with fremanezumab versus placebo were observed in the PPS (quarterly: −2.1 ± 0.51 points, P = 0.0001; monthly: −2.3 ± 0.51 points, P < 0.0001). P-values for treatment comparisons were based on the Wilcoxon rank-sum test.
Conclusion
In this Phase III study, fremanezumab treatment demonstrated a significant improvement in headache-related disability in patients with CM.
Disclosure of Interest
P. Winner Conflict with: Teva, Amgen, Genetech, Novartis, Allergan, AstraZeneca, Biogen Idec, Ipsen, Conflict with: Teva, Amgen, Avinar, Novartis, Allergan, Conflict with: Allergan, Avinar, Teva, T. Fitzgerald Conflict with: Teva Pharmaceutical Industries, S. Gandhi Conflict with: Teva Pharmaceutical Industries, P. Yeung Conflict with: Teva Pharmaceutical Industries, J. Cohen Conflict with: Teva Pharmaceutical Industries, R. Yang Conflict with: Teva Pharmaceutical Industries, E. Aycardi Conflict with: Teva Pharmaceutical Industries
Migraine Preventive Therapy
PO-01-187
Fremanezumab blocks CGRP induced dilatation in human cerebral, middle meningeal and abdominal arteries.
Lena Ohlsson1, Lars Edvinsson1*, Erik Kronvall2 and Ola B. Nilsson2
1Dept of clinical Investigations
2Neurosurgery, Medicine, Lund, Sweden
Objectives
Fremanezumab (TEV-48125) is a fully humanized anti-CGRP monoclonal antibody (mAb) that has shown positive results in prevention of frequent episodic migraine (Bigal et al., 2015a) and of chronic migraine (Bigal et al., 2015b). Previous preclinical studies have revealed CGRP antagonistic effects on cerebral (CA) (Edvinsson et al., 2007) and middle meningeal arteries (MMA)(Juhl et al., 2007). The aim was presently to evaluate the antagonistic effects of fremanezumab on human arteries.
Methods
Arteries were removed in conjunction with neurosurgery (CA and MMA n = 4) or reconstructive abdominal surgery (AA n = 5). Ring segments of the vessels were mounted in a sensitive myograph, and the functional responses studied using pre-contraction with 30 mM potassium chloride (KCl), and CGRP was given in increasing concentrations (10-10–10-7 M). Increasing concentrations of fremanezumab or vehicle (0.01, 0.05, 0.1 mg/ml) were given 30 min prior to the CGRP administration.
Results
All included arteries responded with a strong stable contraction to the application of 30 mM KCl in buffer. During this precontraction CGRP caused a concentration-dependent relaxation which differed in potency between the types of arteries (CA/MMA = 100 %; AA 80%). Increasing concentrations of fremanezumab showed a shift in the EC50 value and at higher doses a reduction of Emax; CA/MMA = 99,2 nM at 0.01 mg/ml, and 5,6 nM at 0.05 mg/ml. The highest dose showed no relaxation at all to CGRP (total blockade). AA = 182 nM at 0.01 mg/ml and 3.05 nM at 0.1 mg/ml. Vehicle did not modify the responses. The highest dose blocked the response totally to CGRP.
Conclusion
This study has shown that CGRP relaxes human arteries 80–100% but with different EC50; the potency range was CA/MMA < AA. The antagonistic effect and potency of fremanezumab was similar in the human arteries, suggesting that the antibody may have effect in all the studied vessels.
Disclosure of Interest
L. Ohlsson: None Declared, L. Edvinsson Conflict with: Study supported by a grant from TEVA, Conflict with: Collaboration, E. Kronvall: None Declared, O. Nilsson: None Declared
Migraine Preventive Therapy
PO-01-188
Longer term outcomes for patients with chronic migraine treated with OnabotulinumtoxinA BOTOX and implications for a Headache Service: Real-life data for 120 patients treated at Sunderland Royal Hospital, UK
Gina Kennedy1*, Helen Nightingale1, Susan Richardson, Specialist Headache Nurse
1City Hospital Sunderland NHS Trust, Sunderland, United Kingdom
Objectives
OnabotulinumtoxinA BOTOX has been demonstrated to be an effective treatment for chronic migraine. A study of the longer term outcomes of 120 patients who received up to five cycles of OnabotulinumtoxinA BOTOX treatment for chronic migraine between March 2013 and March 2017 was done to help predict longer term service demand and consider implications for local headache services. The number of patients who successfully transformed into episodic migraine following OnabotulinumtoxinA BOTOX treatment were calculated. Out of this cohort of patients, the number who then relapse back into more than 15 headache days per month was calculated. This number together with the number of partial responders requiring ongoing OnabotulinumtoxinA BOTOX treatment will help predict service demand.
Methods
120 adults with chronic migraine were injected with OnabotulinumtoxinA BOTOX as per PREEMPT Protocol between March 2013-March 2017. Outcomes following the second, third and fifth treatments were defined according to NICE Guidance as transformation to episodic migraine (treatment success) based on <15 headache days/month for three months, partial response to treatment (treatment success) based on >30% reduction in headache days, and no response to treatment (treatment failure) based on <30% reduction in headache days. Headache Impact test scores were collected prior to every treatment with Onabotulinum toxinA BOTOX. Secondary outcomes were adverse events and reductions in oral migraine prophylactic or analgesia.
Results
After the first two cycles of treatment with OnabotulinumtoxinA BOTOX, 83.8 % patients were defined as treatment success which included 31.6 % whom successfully transformed into episodic migraine, and 52.2 % whom had a significant partial response. 15% of patients did not respond significantly to treatment.
Outcomes after the third (episodic 32.1%, partial 55.1%, no response 11.4%) and fifth (34.6%, partial 55.1%, no response 10.2%) cycles show a comparable pattern of response to that following the second cycle.
For those patients who transformed into episodic migraine, 86.4% of these patients relapsed back to more than 15 headache days per month up to six months later. The average length of time patients remained in an episodic migraine pattern was 3 months (range 3−17 months).
There was a reduction of the average HIT score by 5 points. Side effects were reported in 41% patients and were mild and tolerable in most cases. 35% patients were able to reduce or discontinue oral preventative (15.8%) or analgesia/triptan treatment (19.1%).
Conclusion
OnabotulinumtoxinA BOTOX remains a very effective treatment for chronic migraine. The majority of patients who respond to treatment require regular treatment in the long term. This study showed a consistent pattern of response over five cycles of treatment with 83.8% to 89.7% of patients achieving treatment success and requiring ongoing treatment. There is a trend for better outcomes with increasing number of treatment cycles. This allows future predications for service demand which may require increasing numbers of trained injectors and clinic capacity. Support in the community may be required in the long term. Cost effectiveness of the treatment can be measured in the reduction of oral medications, increased work productivity and reduced GP or emergency hospital admissions.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-189
The effectiveness of 12-week Tai Chi training in the prophylaxis of episodic migraine: a pilot randomized controlled trial in Chinese women
Yao Jie Xie1*, Stanley Sai-Cheun Hui2, Suzanne C. Ho3 and Lorna Kwai Ping Suen1
1School of Nursing, The Hong Kong Polytechnic University
2Department of Sports Science and Physical Education
3JC School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong, Hong Kong
Objectives
Tai Chi is a body-mind exercise. It’s prophylactic efficacy on migraine attack remains largely unknown. The purpose of this study was to test the effectiveness of a12-week Tai Chi training in the prophylaxis of episodic migraine in Chinese women.
Methods
A two-arm individual level randomized controlled trial was designed. Eighty-two local women aged 18 to 65 years and diagnosed with episodic migraine were randomized to the Tai Chi group or the waiting list control group. A modified 32-short form Yang-style Tai Chi training with 1 hour per day, 5 days per week for 12 weeks was adopted as intervention. The control group received a “delayed” Tai Chi training at the end of the trial. The primary outcomes were the difference in migraine days between 4 weeks before baseline and 9–12 weeks after randomization, and the proportion of subjects with at least a 50% reduction of the number of attacks per month. The changes of headache intensity (measured by Visual Analogue Scale) and duration (hours) were also analyzed.
Results
Of 189 women screened, 82 eligible women completed the baseline assessment. After randomization, 9 women withdrew immediately, finally 40 in Tai Chi group and 33 in control group were involved in the analysis. On average, women in Tai Chi group had 3.6 (95% CI: −4.7 to −2.5, P < 0.01) days reduction of migraine attack; 52.5% of them showed more than half of reduction in attack frequency. Compared with control group, the differences were statistically significant (both P < 0.001). The intensity and duration of headache had 0.6 (95% CI: −1.2 to −0.0, P < 0.05) units and 1.2 (IQR: −5.0 to 1.1, P < 0.05) hours reduction in Tai Chi group, respectively. Whereas no significant between-group differences were found (both P > 0.05).
Conclusion
The 12-week Tai Chi training significantly decreased migraine attack frequency. Its effectiveness on headache alleviation and duration shortening needs further larger sample investigations.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-190
A Phase 1 Study to Assess the Pharmacokinetics, Safety, Tolerability and immunogenicity of Fremanezumab (formerly TEV-48125) doses (225 mg, 675 mg and 900 mg) in Japanese and Caucasian Healthy Subjects
Orit Cohen-Barak1*, Xiaojun Hu1, Michele Rasamoelisolo1, Nicola Faulhaber1, Paul Yeung1, Esther Yoon2, Mohit Gandhi3 and Ernesto Aycardi1
1Global Research and Development, Teva Pharmaceutical Industries, Netanya, Israel
2PAREXEL International, Los Angeles
3PRA Health Sciences, Lenexa, United States
Objectives
Fremanezumab (formerly TEV-48125) is a fully humanized IgG2Δa monoclonal antibody that selectively blocks both CGRP isoforms (α- and β) from binding to the CGRP receptor. Fremanezumab was effective and well-tolerated as a preventive treatment of episodic migraine and chronic migraine in phase 2 and phase 3 trials. The present study evaluated the pharmacokinetic profile, safety, and immunogenicity of fremanezumab doses tested in the phase 2 and 3 trials (225 mg, 675 mg and 900 mg) following single administration in Japanese (n = 32) and Caucasian (n = 32) healthy subjects.
Methods
Japanese and Caucasian healthy subjects were enrolled into 1 of 4 cohorts: cohorts 1 and 3 were Japanese and cohorts 2 and 4 were Caucasians. Subjects in each cohort were randomly assigned to 1 of 4 treatments: 225, 675, or 900 mg fremanezumab, or placebo. In the first cohort only, a dose escalation scheme was applied where study drug was not escalated to the next dose level unless the safety and tolerability of the previous doses were acceptable by sponsor and clinical team. Caucasian subjects were matched to Japanese subjects based on gender, age (±10 year) and BMI (±20%). PK and immunogenicity sampling and safety & tolerability assessments occurred during 13 clinic visits including 1 inpatient visit from day −1 to day 6 and 12 ambulatory visits between post treatment days 8–225.
Results
Sixty-two subjects out of 64 completed the study; 2 Japanese subjects (1 225 mg and 1 900 mg fremanezumab) withdrew consent because of family emergencies. Overall median Tmax was similar across doses and ranged from 5 to 7 days. Mean half-lives were similar across doses (range 32.23 to 36.15 days). No differences due to race/ethnicity. Increases in Cmax and AUCs were slightly greater than dose proportional for both Japanese and Caucasian subjects. Fremanezumab exposures were generally higher with lower body weights. No deaths or SAEs; most frequently occurring AEs (≥2 subjects) were injection site reactions, abdominal pain, headache, upper respiratory tract infection, constipation and nasopharyngitis. Local tolerability of the SC fremanezumab injection was comparable between Japanese and Caucasian subjects. No treatment-induced anti-drug-antibodies occurred and there were no clinically meaningful changes in laboratory findings.
Conclusion
Overall fremanezumab was safe and well tolerated following SC single doses (225, 675, or 900 mg). Pharmacokinetic exposure parameters per dose were similar for Japanese and Caucasians. Half-life following SC injections support the once monthly SC injections of 225 mg and quarterly SC injections of 675 mg as a treatment doses.
Disclosure of Interest
O. Cohen-Barak Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries, X. Hu Conflict with: Teva Pharmaceutical Industries, M. Rasamoelisolo Conflict with: Teva Pharmaceutical Industries, N. Faulhaber Conflict with: Teva Pharmaceutical Industries, P. Yeung Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries, E. Yoon Conflict with: PAREXEL International, M. Gandhi Conflict with: PRA Health Sciences, E. Aycardi Conflict with: Teva Pharmaceutical Industries, Conflict with: Teva Pharmaceutical Industries
Migraine Preventive Therapy
PO-01-191
Cognitive Behavioral Therapy Experience in Patients With Refractory Chronic Migraine
Derya Uluduz*1, Devrimsel H. Ertem2, Ozge S. Onur3, Aynur Ozge4, Çağatay Karşıdağ3 and Aksel Siva2
1Departmenet of Neurology, Cerrahpasa School of Medicine
2Neurology, Istanbul University Cerrahpasa School of Medicine
3Neurology, Bakırkoy Research and Training Hospital, Istanbul
4Neurology, Mersin University Medical Faculty, Mersin, Turkey
Objectives
Cognitive Behavioral Therapy (CBT) for pain management is a form of therapy which aims to modify thoughts and behavior for realistic and balanced way and change in behaviors. CBT in migraine intends to arrange the behavioral interventions for controlling headache attacks. There are limited studies to assess the efficacy for CBT for patients with pharmacotherapy resistant chronic migraine in our population. We investigated the effects of CBT for patients with refractory chronic migraine on pain severity, attack frequency, disability, anxiety, and depression.
Methods
Fourteen patients with chronic migraine were referred from headache clinic to psychiatry department who participated regularly for follow-up therapy sessions once in 2 weeks for six months. After 2 sessions of psychiatric evaluation, subjects had CBT sessions lasting 30 minutes for 12 times and were taught for relaxation exercises. Hamilton Depression and Anxiety Inventories, for assesing the severity of pain visual analogue scale (VAS) and for evaluating migraine related disability Migraine Disability Assessment Test (MIDAS) were used before and after CBT.
Results
The number of male subjects was 5 and female subjects 9 and their mean age was 34.35 ± 8.17. The average disease duration was 13.07 ± 7.18 and 12 patients had a previous psychiatric evaluation. Seven patients had depression, 4 patients had anxiety disorders and 1 patients had trauma-related disorders. Nine patients were under migraine prophylactic therapies. Before CBT, Hamilton Depression scores were 29.07 ± 7.74 and after 14.21 ± 7.7 which was statistically significant. Before CBT, Hamilton Anxiety scores were 26.8 ± 11.7 and after 11.7 ± 2.6 which was statistically significant (p = 0.000). Before CBT, VAS scores were 8.07 ± 0.91 and after CBT, 3.71 ± 1.32 (p = 0.000). Before CBT, MIDAS scores were 55.5 ± 20.4 and after CBT, 20.12 ± 16.6 (p = 0.000).
Conclusion
CBT reduced migraine severity, number of attacks and disability statistically significant in patients with chronic migraine. CBT should be included in headachtreatment more often.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-192
Effect of iron administration for migraine with iron deficiency
Kazunori Tanaka1 and Eri Fujita2
1Neurosurgery, Saiseikai Matsuyama Hospital, Matsuyama
2General internal medicine, Shibuya Prime Clinic, Tokyo, Japan
Objectives
To examine the effects of iron replacement therapy in migraines complicated by iron deficiency.
Methods

Results
63 patients (13 men and 50 women) with migraine were enrolled in the study. Of them, overt iron deficiency was found in 7 patients (1 men and 6 women), and subclinical iron deficiency in 14 patients (0 men and 14 women). Prevalence of iron deficiency (overt and subclinical) in the patients with migraine was 33.3% (21/63). All patients with iron deficiency opted to receive iron replacement. After 3 months of therapy/observation, 11/21 patients in the iron replacement group were “cured”, 8/21 “improved”, 2/21 “did not change”, and 0/21 “unknown”; 11/42 patients in non-intervention group were “cured”, 15 “improved”, 13 “did not change”, and 3 “unknown”. Therefore, migraine was cured in 52% (11/21) patients in the iron administration group, while the proportion was merely 26% (11/42) in the non-intervention group. If therapeutic effect was defined as the sum of "cured” and “improved" groups, more therapeutic effect was found in 90% (19/21) the iron replacement group compared to 62% 26/42 in non-intervention group (p = 0.0215).
Conclusion
In patients with migraine complicated by overt or subclinical iron deficiency, oral iron replacement therapy led to improved control of symptom of migraine.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-193
Cognitive Behavioral Therapy in Turkish Patients With Refractory Chronic Migraine
Derya Uluduz1*, Devrimsel Harika Ertem1, Ozge S. Onur2 and Cagatay Karsidag2
1Neurology, Cerrahpasa School of Medicine
2Psychiatry, bakirkoy research and education hospital for psychiatric and neurological diseases, istanbul, Turkey
Objectives
Cognitive Behavioral Therapy (CBT) for pain management is a form of therapy which aims to modify thoughts and behavior for realistic and balanced way and change in behaviors. CBT in migraine intends to arrange the behavioral interventions for controlling headache attacks. There are limited studies to assess the efficacy for CBT for patients with pharmacotherapy resistant chronic migraine in our population. We investigated the effects of CBT for patients with refractory chronic migraine on pain severity, attack frequency, disability, anxiety, and depression.
Methods
Fourteen patients with chronic migraine were referred from headache clinic to psychiatry department who participated regularly for follow-up therapy sessions once in 2 weeks for six months. After 2 sessions of psychiatric evaluation, subjects had CBT sessions lasting 30 minutes for 12 times and were taught for relaxation exercises. Hamilton Depression and Anxiety Inventories, for assesing the severity of pain visual analogue scale (VAS) and for evaluating migraine related disability Migraine Disability Assessment Test (MIDAS) were used before and after CBT.
Results
The number of male subjects was 5 and female subjects 9 and their mean age was 34.35 ± 8.17. The average disease duration was 13.07 ± 7.18 and 12 patients had a previous psychiatric evaluation. Seven patients had depression, 4 patients had anxiety disorders and 1 patients had trauma-related disorders. Nine patients were under migraine prophylactic therapies. Before CBT, Hamilton Depression scores were 29.07 ± 7.74 and after 14.21 ± 7.7 which was statistically significant. Before CBT, Hamilton Anxiety scores were 26.8 ± 11.7 and after 11.7 ± 2.6 which was statistically significant (p = 0.000). Before CBT, VAS scores were 8.07 ± 0.91 and after CBT, 3.71 ± 1.32 (p = 0.000). Before CBT, MIDAS scores were 55.5 ± 20.4 and after CBT, 20.12 ± 16.6 (p = 0.000).
Conclusion
CBT reduced migraine severity, number of attacks and disability statistically significant in patients with chronic migraine. CBT should be included in headache treatment more often.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-01-194
A Phase 3, Randomized, Double-blind, Placebo-Controlled Study to Evaluate the Efficacy and Safety of Eptinezumab in Frequent Episodic Migraine Prevention: Primary Results of the PROMISE 1 (PRevention Of Migraine via Intravenous eptinezumab Safety and Efficacy 1) Trial
Joel Saper1*, Richard Lipton2, David Kudrow3, Joe Hirman4, David Dodick5, Stephen Silberstein6, George Chakhava7, Jeff Smith8 and David Biondi8
1Michigan Headache and Neurological Institute, Ann Arbor
2Department of Neurology, Montefiore Headache Center, Albert Einstein College of Medicine, Philadelphia
3California Medical Clinic for Headache, Lon Angeles
4Pacific Northwest Stats, Bothell
5Mayo Clinic, Phoenix
6Thomas Jefferson University Headache Center, Philadelphia, United States
7Multiprofile Clinic Consilium Medulla, Tbilisi, Georgia
8Alder BioPharmaceuticals, Bothell, United States
Objectives
Calcitonin gene-related peptide (CGRP) is associated with the facilitation of pain transmission and neuronal sensitization in both central and peripheral sensory pathways, and is believed to have an important role in migraine pathophysiology. PROMISE-1 is a Phase 3 study to evaluate the efficacy and safety of eptinezumab, an anti-CGRP monoclonal antibody, for the prevention of frequent episodic migraine (FEM).
Methods
Adult patients with 4 to 14 headache days per month, of which 4 or more met ICHD-II criteria for migraine, were randomized to receive eptinezumab 300 mg, 100 mg, 30 mg, or placebo by intravenous (IV) infusion every 12 weeks for 4 total doses. The current analyses use double blind data through Week 24 (2 doses). The primary endpoint was the mean change in migraine days over Weeks 1–12 compared to a 28-day baseline. Key secondary endpoints include: the percent of patients who achieved ≥75% reduction in monthly migraine days over Weeks 1–4 and Weeks 1–12; the percent of patients who achieved ≥50% reduction in monthly migraine days over Weeks 1–12; and the percent reduction in the proportion of patients experiencing migraine on the first day after infusion. Statistical significance versus placebo was pre-specified at the two-sided p value <0.05.
Results
888 patients were included in the efficacy evaluation. Baseline migraine days averaged 8.5 days/month across groups. There were highly significant decreases in monthly migraine days for Weeks 1–12 in the eptinezumab 300 mg, 100 mg, and 30 mg groups vs the placebo group (−4.3, −3.9, and −4.0 vs −3.2; p = 0.0001, p = 0.0179, and p = 0.0045* respectively). The 75% migraine responder rates over Weeks 1–4 were significantly greater in the eptinezumab 300 mg, 100 mg, or 30 mg groups vs the placebo group (31.5%, 30.8%, and 30.0% vs 20.3%; p = 0.0066, p = 0.0112, and p = 0.017*, respectively). The 75% migraine responder rate was maintained in the 300 mg group over Weeks 1–12 (300 mg, 29.7%, p = 0.0007; 100 mg, 22.2%, p = NS; 30 mg, 24.7%, p = 0.0272*, placebo, 16.2%). A significantly higher proportion of patients given eptinezumab had a ≥50% reduction in migraine days over Weeks 1–12 (300 mg, 56.3%, p = 0.0001; 100 mg, 49.8%, p = 0.0085*; 30 mg, 50.2%, p = 0.0064* placebo, 37.4%). The percentages of patients with a migraine on Day 1 decreased by ≥50% in the eptinezumab 300 mg and 100 mg groups (53.6% and 51.3%, respectively) and 44.6% in the 30 mg group vs. 20.7% with placebo (p = 0.0087*, p = 0.0167*, and p = 0.074* respectively). Adverse event rates for eptinezumab were similar to placebo.
*unadjusted
Conclusion
In PROMISE-1, eptinezumab demonstrated efficacy for migraine prophylaxis across several measures. Reductions in migraine activity were seen as early as Day 1 and maintained at similar levels over Weeks 1–4 and Weeks 1–12. Adverse event rates for eptinezumab were similar to placebo and its safety profile was consistent with previous studies.
Financial Support
Funding and support provided by Alder BioPharmaceuticals, Inc., Bothell, WA, USA.
Disclosure of Interest
J. Saper Conflict with: Alder BioPharmaceuticals, Inc., R. Lipton Conflict with: Alder BioPharmaceuticals, Inc., D. Kudrow Conflict with: Alder BioPharmaceuticals, Inc., J. Hirman Conflict with: Alder BioPharmaceuticals, Inc., D. Dodick Conflict with: Alder BioPharmaceuticals, Inc., S. Silberstein Conflict with: Alder BioPharmaceuticals, Inc., G. Chakhava Conflict with: Alder BioPharmaceuticals, Inc., J. Smith Conflict with: Alder BioPharmaceuticals, LTD, Conflict with: Alder BioPharmaceuticals, LTD, D. Biondi Conflict with: Alder BioPharmaceuticals, Inc., Conflict with: Alder BioPharmaceuticals, Inc.
Migraine Preventive Therapy
PO-01-195
A Phase 3 Placebo-Controlled Study of Galcanezumab in Patients with Chronic Migraine: Results from the 3-month Double-Blind Treatment Phase of the REGAIN Study
Holland C. Detke1, Shufang Wang1, Vladimir Skljarevski1, Jonna Ahl1, Brian A. Millen1, Sheena K. Aurora*1 and Jyun Yan Yang1
1Eli Lilly and Company, Indianapolis, United States
Objectives
To determine if galcanezumab (GMB), a humanized monoclonal antibody that selectively binds to the calcitonin gene-related peptide (CGRP), is superior to placebo in the prevention of chronic migraine at doses of 120 mg or 240 mg/month.
Methods
This was a Phase 3, double-blind, randomized, placebo-controlled, 3-month study with a 9-month open-label extension. Eligible patients 18–65 years of age with chronic migraine, defined as ≥15 headache days per month, of which at least 8 met criteria for migraine, were randomized 2:1:1 to subcutaneous injections of placebo (N = 558), GMB 120 mg (N = 278), or GMB 240 mg (N = 277) given once monthly for 3 months. The primary endpoint was the overall mean change from baseline in the number of monthly migraine headache days (MHD) during the 3-month double-blind treatment phase. Key secondary measures included the percentage of patients with ≥50%, ≥75%, and 100% reduction in monthly MHD, reduction in monthly MHD requiring acute migraine treatments, change in the Role Function-Restrictive (RF-R) domain score of the Migraine-Specific Quality of Life Questionnaire (MSQ), and change in the Patient Global Impression of Severity (PGI-S) rating.
Results
Mean number of monthly MHD at baseline was 19.4 and was similar across treatment groups. At the primary endpoint, both GMB doses demonstrated statistically significant difference from placebo in overall mean reduction (least square [LS] mean change) in number of monthly MHD during the 3-month double-blind treatment phase: placebo: −2.74, GMB 120 mg: −4.83, GMB 240 mg: −4.62 (p < .001 for each dose). Statistically significant improvements in MHD for both GMB doses were also observed at each month starting from Month 1. The mean percentages over all 3 months of patients with ≥ 50% reduction from baseline in MHD were significantly higher for both GMB doses than placebo (p < .001 for both doses). Compared with placebo, patients in the 240 mg GMB group also had significantly higher percentages of patients with ≥75% response rates (p < .001), greater reductions in monthly MHD requiring acute migraine treatment (p < .001), and greater improvement in the MSQ RF-R (p < .001) and PGI-S (p < .001). The 120-mg dose did not separate from placebo on those additional key secondary measures after multiplicity adjustment. There were no clinically meaningful differences between either GMB dose and placebo on any safety parameters except for a higher incidence of injection site reaction (p < .05), injection site erythema (p < .01), and sinusitis (p < .05) in the GMB 240 mg group relative to placebo.
Conclusion
Both doses of GMB were superior to placebo in the reduction in monthly MHD, with significantly higher percentages of patients reducing their monthly MHD by ≥50%. The 240 mg dose was also superior to placebo on most key secondary measures. Both GMB doses appear to be efficacious, safe, and well-tolerated for the preventive treatment of chronic migraine.
This study is registered as NCT02614261 at ClinicalTrials.gov.
Disclosure of Interest
H. Detke Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, S. Wang Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, V. Skljarevski Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, J. Ahl Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, B. Millen Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, S. Aurora Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, J. Y. Yang Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company
Migraine Preventive Therapy
PO-01-196
Efficacy and Safety of 2 Dose Regimens of Subcutaneous Fremanezumab (TEV-48125) Versus Placebo for the Preventive Treatment of Chronic Migraine
Ernesto Aycardi1, Marcelo Bigal1, Paul Yeung1, Tricia Blankenbiller1, Melissa Grozinski-Wolff1, Ronghua Yang1, Yuju Ma1, Stephen Silberstein2*, Peter J Goadsby3 and David Dodick4
1Teva, Malvern
2Jefferson Headache Center, Philadelphia, United States
3NIHR-Wellcome Trust King's Clinical Research Facility, King's College, London, United Kingdom
4Mayo Clinic, Arizona, United States
Objectives
Fremanezumab, a fully humanized monoclonal antibody targeting the calcitonin gene-related peptide (CGRP) ligand, is a preventive treatment designed to specifically target a pathophysiologic mechanism of migraine. This study evaluated the efficacy, tolerability and safety of two subcutaneous (SQ) dose regimens of fremanezumab in the preventive treatment of chronic migraine (CM).
Methods
This was a 16-week, multicenter, randomized, double-blind, placebo-controlled, parallel-group study in adults with CM. Patients maintained a daily diary during a 28-day baseline period. Patients were assigned randomly to 1:1:1 ratio to 1 of 3 treatment groups: (1) monthly dosing: an initial dose of 675 mg of fremanuzemab followed by 225 mg of fremanezumab at months 2 and 3 (2) quarterly dosing: a single dose of 675 mg of fremanuzemab at month 1, followed by placebo injections at months 2 and 3 and (3) monthly administration of matching placebo. The primary efficacy endpoint, the mean change from baseline (28-day run-in period) to the 12-week randomization period in the monthly average number of headache days of at least moderate severity was analyzed using an analysis of covariance method or the Wilcoxon rank sum test.
Results
Patients treated with fremanezumab had a significant reduction in the number of monthly headache days of at least moderate severity vs. placebo (−2.5 days) during the 12-week period after 1st dose, for both monthly (−4.6 days p < 0.0001) and quarterly (−4.3 days p < 0.0001) dosing regimens. Patients treated with fremanezumab had statistically significant reduction in the number of monthly migraine days during the 12-week period after the 1st dose, for both dosing regimens [monthly (−5.0 days from a baseline of 16.0 days) and quarterly (−4.9 days from a baseline of 16.2 days; p < 0.0001] vs. placebo (−3.2 days from a baseline of 16.3 days), and during the 4-week period after 1st dose, for both dosing regimens (p < 0.0001). Fremanezumab was also significantly superior to placebo for the following prespecified secondary endpoints; reduction in the number of monthly days of acute headache medication use for both monthly (−4.2 days) and quarterly (−3.7 days) versus placebo (−1.9 days); p < 0.0001). A ≥50% reduction in monthly average number of headache days of at least moderate severity were also statistically significantly improved with both dosing regimens [monthly (40.8%) and quarterly (37.6%); p < 0.0001] as compared to placebo (18.1%); improvement in disability as measured by the 6-item Headache Impact Test (HIT-6) with both dosing regimens [monthly (−6.8; p < 0.0001) and quarterly (−6.4; p = 0.0001)] as compared to placebo (−4.5). The most commonly-reported adverse event in the study was injection site pain, with similar rates in the placebo and active groups.
Conclusion
These results confirm the efficacy and favorable tolerability profile of fremanezumab, administered as both monthly and quarterly subcutaneous injections, for the preventive treatment of chronic migraine.
Disclosure of Interest
E. Aycardi Conflict with: Teva Pharmaceutical, M. Bigal Conflict with: Teva Pharmaceutical, P. Yeung Conflict with: Teva Pharmaceutical, T. Blankenbiller Conflict with: Teva Pharmaceutical, M. Grozinski-Wolff Conflict with: Teva Pharmaceutical, R. Yang Conflict with: Teva Pharmaceutical, Y. Ma Conflict with: Teva Pharmaceutical, S. Silberstein Conflict with: Teva Pharmaceutical, P. J. Goadsby Conflict with: Teva Pharmaceutical, D. Dodick Conflict with: Teva Pharmaceutical
Migraine Preventive Therapy
PO-01-197
Phase 3 Studies (EVOLVE-1 & EVOLVE-2) of Galcanezumab in Episodic Migraine: Results of 6-Month Treatment Phase
Vladimir Skljarevski1*, Virginia L. Stauffer1, Qi Zhang1, Holland C. Detke1, Brian A. Millen1, Jyun Yan Yang1, Katherine J. Selzler1, Robert Conley1 2 and Sheena K. Aurora1
1Eli Lilly and Company, Indianapolis
2University of Maryland School of Medicine, Baltimore, United States
Objectives
Galcanezumab, a humanized monoclonal antibody that selectively binds to the calcitonin gene-related peptide, was investigated in two Phase 3 studies (EVOLVE-1 and EVOLVE-2) to determine superiority to placebo in the prevention of migraine headache.
Methods
EVOLVE-1 and EVOLVE-2 were double-blind, 6-month studies in patients with episodic migraine (4 to 14 monthly migraine headache days [MHD]) conducted in North America and globally, respectively. Patients were randomized 2:1:1 to monthly subcutaneous injections of placebo, galcanezumab 120 mg or 240 mg. Primary endpoint was overall mean change from baseline in the number of monthly MHD during Months 1–6. Key secondary measures included rates of ≥50%, ≥75%, and 100% reduction in monthly MHD and overall mean change from baseline in monthly MHD with acute migraine treatments, and mean change from baseline over Months 4–6 on the Role Function-Restrictive domain score of the Migraine-Specific Quality of Life Questionnaire (MSQ-RFR) and Patient Global Impression-Severity of Illness (PGI-S).
Results
Baseline mean number of monthly MHD was 9.1 for both studies. Both galcanezumab doses demonstrated a statistically significant improvement compared with placebo (both studies p < .001) for overall mean change in monthly MHD (EVOLVE-1: placebo = −2.81; GMB 120 mg = −4.73; GMB 240 mg = −4.57; EVOLVE-2: placebo = −2.28; GMB 120 mg = −4.29; GMB 240 mg = −4.18). Percentage of patients with MHD reductions of ≥50%, ≥75%, or 100% were significantly higher for each galcanezumab dose compared with placebo (both studies p < .001). Patients had a significantly greater overall mean reduction of monthly number of MHD with acute migraine treatment for both galcanezumab doses relative to placebo (both studies p < .001). Mean change in MSQ-RFR and PGI-S ratings were statistically significant for each galcanezumab dose versus placebo (MSQ-RFR: p < .001 and PGI-S: p < .05, in both studies). There were no statistically significant differences between galcanezumab and placebo on the most common treatment-emergent adverse events except for a greater incidence of injection-site pruritus (both studies/doses p < .01) and injection-site reaction (both studies/doses p < .05), and injection-site erythema (p < .05, galcanezumab 240 mg) in EVOLVE-2.
Conclusion
Both doses of galcanezumab met the primary and all key secondary objectives, after adjusting for multiplicity. Treatment effects were similar across galcanezumab doses for efficacy, and safety; however, there was a higher rate of injection-site pruritus and reaction in galcanezumab-treated patients in both studies. EVOLVE-1 and EVOLVE-2 demonstrated that galcanezumab, at either 120 mg or 240 mg monthly, provided clinical benefit and improved function in patients with episodic migraine.
Studies were registered as NCT02614183 and NCT02614196 at ClinicalTrials.gov.
Disclosure of Interest
V. Skljarevski Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, V. Stauffer Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Q. Zhang Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, H. Detke Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, B. Millen Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, J. Y. Yang Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, K. Selzler Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, R. Conley Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Adjunct Professor at University of Maryland School of Medicine, S. Aurora Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company, Conflict with: Eli Lilly and Company
Migraine Preventive Therapy
PO-01-198
A Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Effect of Erenumab on Exercise Time During a Treadmill Test in Patients with Stable Angina
Christophe Depre1*, Lubomir Antalik2, Amaal Starling3, Michael Koren4, Osaro Eisele1, Yumi Kubo1, Robert A. Lenz1 and Daniel D. Mikol1
1Amgen, Thousand Oaks, United States
2Regional Hospital, Cardiological Department, Bratislava, Slovakia
3Mayo Clinic, Scottsdale
4Jacksonville Center for Clinical Research, Jacksonville, United States
Objectives
During myocardial ischemia, cardiac sensory nerves release a number of vasodilatory mediators in addition to calcitonin gene-related peptide (CGRP). To date, the relative importance of the CGRP pathway among the many biochemical changes that occur during myocardial ischemia has not been established. Erenumab, a human anti-CGRP receptor monoclonal antibody, is being developed for preventive treatment of migraine. The primary objective of this study was to evaluate the effect of erenumab compared with placebo on exercise capacity in patients with stable angina as measured by total exercise time (TET) during an exercise treadmill test (ETT).
Methods
This study was a double-blind, placebo-controlled study in patients with stable angina due to documented coronary artery disease. Patients were randomized 1:1 to a single intravenous infusion of erenumab 140 mg or placebo stratified by baseline TET (<7 minutes or 3 7 minutes) defined as the average TET of two qualifying ETTs performed during screening. Following study drug administration, a post-administration ETT was conducted on Day 1. The primary endpoint was the change from baseline in exercise duration as measured by TET with a non-inferiority margin of −90 seconds and was analyzed using an analysis of variance model with treatment, randomization strata (<7 or ≥7 minutes), age (<65, ≥65) and sex as covariates. Secondary efficacy endpoints included time to onset of ≥1 mm ST-segment depression and time to onset of exercise-induced angina during the ETT. Safety follow-up visits occurred every 2–4 weeks for 12 weeks. At the time of primary analysis all patients had a postbaseline ETT and 38 patients (43%) had completed the week 12 visit.
Results
Eighty-nine patients were enrolled in the study. Baseline demographics and disease characteristics were similar between groups. In the erenumab group, the LS mean (SE) change from baseline in TET was −2.9 [14.8] seconds and in the placebo group it was 8.1 [14.4] seconds. The adjusted mean (90% confidence interval [CI]) treatment difference in change from baseline in TET was −11.0 (–44.9, 22.9) seconds. The TET change from baseline in the erenumab group was non-inferior to that observed in the placebo group, as the lower bound of the CI (–44.9) did not reach the pre-defined non-inferiority margin of −90 seconds, supporting the hypothesis that erenumab does not substantially decrease exercise duration. There was no difference observed between erenumab and placebo groups for the secondary endpoints of time to exercise-induced angina (hazard ratio [90% CI: 1.11 [0.73, 1.69], p = 0.69) or time to onset of ≥1 mm ST-segment depression (hazard ratio [95% CI]: 1.14 [0.76, 1.69], p = 0.59). Adverse events were reported by 13.6% of erenumab-treated patients and by 27.3% of placebo patients. Maximum changes from baseline in vital signs (systolic blood pressure, diastolic blood pressure and heart rate) during the ETT were similar between the two groups.
Conclusion
Erenumab did not adversely affect exercise time in an at-risk population of patients with stable angina. No new safety concerns were identified. These results suggest that inhibition of the CGRP pathway does not worsen myocardial ischemia and support the hypothesis that other vasodilatory mechanisms and the CGRP pathway are redundant responses in patients with chronic stable angina.
Disclosure of Interest
C. Depre Conflict with: Amgen, Conflict with: Amgen, L. Antalik: None Declared, A. Starling Conflict with: eNeura, Eli Lilly & Company, Amgen, Alder, M. Koren Conflict with: Jacksonville Center for Clinical Research that received research and consulting fees from Amgen, O. Eisele Conflict with: Amgen, Conflict with: Amgen, Y. Kubo Conflict with: Amgen, Conflict with: Amgen, R. Lenz Conflict with: Amgen, Conflict with: Amgen, D. Mikol Conflict with: Amgen, Conflict with: Amgen
Migraine Preventive Therapy
PO-01-199
Eptinezumab Infusion Associated with Meaningful Reductions in Daily Migraine Activity on Day 1 and Over Weeks 1 Through 4 in Patients with Frequent Episodic Migraine: Results of the PROMISE-1 (PRevention Of Migraine via Intravenous eptinezumab Safety and Efficacy 1) Trial
Roger Cady1*, Timothy Smith2, David Biondi1, Gary Berman3, Marshall Freeman4, Joe Hirman5 and Eric Kassel1
1Alder BioPharmaceuticals, Inc., Bothell
2StudyMetrix Research, LLC, St. Louis
3Clinical Research Institutes, Minneapolis
4Headache Wellness Center, Greensboro
5Pacific Northwest Stats, Bothell, United States
Objectives
Calcitonin gene-related peptide (CGRP) is associated with the facilitation of pain transmission and neuronal sensitization in both central and peripheral sensory pathways, and is believed to have an important role in migraine pathophysiology. PROMISE-1 is a Phase 3 study to evaluate the efficacy and safety of eptinezumab, an anti-CGRP monoclonal antibody, for the prevention of frequent episodic migraine (FEM). Here we describe the effect of eptinezumab on migraine activity from Day 1 and through Week 4 after an intravenous (IV) infusion.
Methods
Adult patients with 4 to 14 headache days per month, of which 4 or more met ICHD-II criteria for migraine, were randomized to receive eptinezumab 300 mg, 100 mg, 30 mg, or placebo by IV infusion every 12 weeks for 4 total doses. Current analyses use double blind data through Week 24 (2 doses). The primary endpoint was the mean change in monthly migraine days over Weeks 1–12. Key secondary endpoints evaluated here are the percentage of patients with a migraine (migraine prevalence) on the day after the first infusion (Day 1) and the percentage of patients who had ≥75% reduction in monthly migraine days over Weeks 1–4. An exploratory analysis evaluated the percentage of patients with a migraine on any given day during Weeks 1–4. Statistical significance versus placebo was pre-specified at the two-sided p value <0.05.
Results
888 patients received study treatment and were included in the efficacy analyses. Baseline migraine days averaged 8.5 days/month across groups. There were highly significant decreases in mean change from baseline in monthly migraine days for Weeks 1–12 in the eptinezumab 300 mg, 100 mg, and 30 mg groups vs the placebo group (−4.3, −3.9, and −4.0 vs −3.2; p = 0.0001, p = 0.0179, and p = 0.0045* respectively). The percentages of patients with a migraine on Day 1 decreased by over 50% in the eptinezumab 300 mg and 100 mg groups (53.6% and 51.3%, respectively) and 44.6% in the 30 mg group vs. 20.7% with placebo (p = 0.0087*, p = 0.0167*, and p = 0.074* respectively). These reductions were maintained at similar magnitudes through Week 4 as evidenced by mean daily migraine prevalence by week for Weeks 1–4. Nearly 1/3 of patients in the 300 mg, 100 mg, and 30 mg groups had a ≥75% reduction in migraine days vs. placebo over Weeks 1–4 (31.5%, 30.8%, and 30.0% vs. 20.3%; p = 0.0066, p = 0.0112, and p = 0.017*, respectively). Adverse event rates for epitinezumab were similar to placebo.
*unadjusted
Conclusion
In PROMISE-1, eptinezumab demonstrated efficacy for migraine prevention across several measures. Reductions in migraine prevalence of up to 54% were seen as early as Day 1 and maintained at similar levels through Week 4. These results are consistent with the finding that nearly 1/3 of patients given eptinezumab had a ≥75% reduction in migraine days over Weeks 1–4. Adverse event rates were similar to placebo and eptinezumab’s safety profile was consistent with previous studies.
Financial Support
Funding and support provided by Alder BioPharmaceuticals, Inc., Bothell, WA, USA.
Disclosure of Interest
R. Cady Conflict with: Alder BioPharmaceuticals, Inc., Conflict with: Alder BioPharmaceuticals, Inc., T. Smith Conflict with: Alder BioPharmaceuticals, Inc., D. Biondi Conflict with: Alder BioPharmaceuticals, Inc., Conflict with: Alder BioPharmaceuticals, Inc., G. Berman Conflict with: Alder BioPharmaceuticals, Inc., M. Freeman Conflict with: Alder BioPharmaceuticals, Inc., J. Hirman Conflict with: Alder BioPharmaceuticals, Inc., E. Kassel Conflict with: Alder BioPharmaceuticals, Inc., Conflict with: Alder BioPharmaceuticals, Inc.
Migraine Preventive Therapy
PO-01-200
Benefit-Risk Assessment of Migraine Prophylaxis Treatments Using Likelihood of Being Helped or Harmed (LHH)
Pamela Vo1*, Shihua Wen1, Marie-Losee Martel2, Dimos Mitsikostas3, Uwe Reuter4 and Jan Klatt1
1Novartis Pharma AG, Basel, Switzerland
2Xcenda UK, London, United Kingdom
31st Neurology Department, Aeginition Hospital, National and Kapodistrian University of Athens, Athens, Greece
4Department of Neurology, Charité Universitätsmedizin Berlin, Berlin, Germany
Objectives
A key measure of successful therapy in migraine is the ability to sustain efficacy. Numerous prophylactic medications are available for this chronic disorder; however most of them have major shortcomings primarily due to variable efficacy and poor tolerability due to side effects. This study aimed to evaluate the benefit-risk of novel CGRP receptor antagonist erenumab, relative to other approved prophylactic migraine therapies
Methods
Potential trials for inclusion were identified via a published systematic literature review1 updated up to November 2016 using MEDLINE. As at the time of evaluation erenumab’s complete pivotal trial results were unpublished, clinical study reports were used (NCT02066415, NCT02456740). The ≥50% responder rates and discontinuations due to adverse events were defined as primary efficacy and tolerability variables to generate numbers needed to treat (NNT) and harm (NNH). The LHH as a quantitative benefit-risk measure was computed based on the ratio of NNH/NNT. Sensitivity analyses were conducted using alternative efficacy and tolerability data.

Results
Of 146 articles assessed, 9 RCTs (11 articles) met inclusion/exclusion criteria and were deemed of high quality per the Jadad score. Propranolol, topiramate, and onabotulinumtoxinA (the latter approved for CM only) were retained as comparators as they are approved for migraine prophylaxis and available in the majority of European countries. Table 1 shows an NNT of around 6 in both CM and EM for erenumab. This low NNT is numerically comparable to topiramate and onabotulinumtoxinA and show the strong treatment benefit of erenumab. NNH showed substantial differences among treatments, with higher numbers indicating better tolerability for erenumab. A favorable relative benefit-risk was seen for erenumab with LHHs of 41.7 and 166.7 for CM and EM respectively. In comparison, LHHs were lower in CM for topiramate (1.6 and 3.3) and onabotulinumtoxinA (4.3), and in EM, for topiramate (1.6) and propranolol (2.2). Sensitivity analyses showed results’ robustness despite residual variations and overall magnitude of LHH consistently favored erenumab.
Conclusion
While all prophylactic migraine treatments were more likely to help than harm (LHH > 1), erenumab showed LHHs of high magnitude, providing additional evidence to support the favorable benefit-risk profile of erenumab to patients across the entire spectrum of migraine compared with other migraine prophylactic treatments available in Europe.
Disclosure of Interest
P. Vo Conflict with: Novartis, S. Wen Conflict with: Novartis, M.-L. Martel Conflict with: Xcenda, D. Mitsikostas Conflict with: 1st Neurology Department, Aeginition Hospital, National and Kapodistrian University of Athens, U. Reuter Conflict with: Department of Neurology, Charité Universitätsmedizin Berlin, J. Klatt Conflict with: Novartis
Migraine Preventive Therapy
PO-01-201
Efficacy and Safety of 2 Dose Regimens of Subcutaneous Administration of Fremanezumab (TEV-48125) Versus Placebo for the Preventive Treatment of Episodic Migraine
Ernesto Aycardi1, Marcelo Bigal1, Paul Yeung1, Tricia Blankenbiller1, Melissa Grozinski-Wolff1, Ronghua Yang1, Yuju Ma1, Stephen Silberstein2, Peter J Goadsby3 and David Dodick4
1Teva Pharmaceuticals, Malvern
2Jefferson Headache Center, Philadelphia, United States
3NIHR-Wellcome Trust King’s Clinical Research Facility, King’s College, London, United Kingdom
4Mayo Clinic, Scottsdale, United States
Objectives
Fremanezumab, a fully humanized monoclonal antibody targeting the calcitonin gene-related peptide (CGRP) ligand, is a preventive treatment designed to specifically target a pathophysiologic mechanism of migraine; it has proven efficacy in the treatment of migraine. This study evaluated the efficacy, tolerability and safety of two subcutaneous (SQ) dose regimens of fremanezumab in the preventive treatment of episodic migraine (EM).
Methods
This was a 16-week, multicenter, randomized, double-blind, placebo-controlled, parallel-group study in adults with EM. Patients maintained a daily diary during a 28-day baseline period. Patients were assigned randomly to 1:1:1 ratio to 1 of 3 treatment groups: (1) monthly dosing with 225 mg of fremanezumab (2) quarterly dosing: a single dose of 675 mg of fremanuzemab at month 1, followed by placebo injections at months 2 and 3 and (3) monthly administration of matching placebo. The primary efficacy endpoint, the mean change from baseline (28-day run-in period) to the 12-week randomization period in the monthly average number of migraine days was analyzed using an analysis of covariance method or the Wilcoxon rank sum test.
Results
Patients treated with fremanezumab had a significant reduction in the number of monthly migraine days during the 12-week period vs. placebo (−2.2 days from a baseline of 9.1 days), for both dosing regimens [monthly (−3.7 days from a baseline of 9.2 days) and quarterly (−3.4 days from a baseline of 8.9 days); p < 0.0001], and during the 4-week period after 1st dose, for both dosing regimens (p < 0.0001). Patients treated with fremanezumab had a significant reduction in the number of monthly headache days of at least moderate severity during the 12-week period for both dosing regimens [monthly (−2.9 days) and quarterly (−3.0 days); vs placebo (−1.5 days); p < 0.0001), and during the 4-week period after 1st dose, for both dosing regimens (p < 0.0001). Fremanezumab resulted in a statistically significant reduction in the number of monthly days of acute headache medication use for both [monthly (−3.0 days) and quarterly (−2.9 days); p < 0.0001] versus placebo (−1.6 days). A ≥50% reduction in monthly average number of migraine days was also significantly improved with both dosing regimens [monthly (47.7%) and quarterly (44.4%); p < 0.0001] as compared to placebo (27.9%). Improvement in disability was observed as measured by Migraine Disability Assessment (MIDAS) with monthly (−24.6; p = 0.0021) and quarterly (−23.0; p = 0.0023) as compared to placebo (−17.5). The most commonly-reported adverse event in the study was injection site pain with rates in active groups 4% higher than placebo.
Conclusion
These results confirm the efficacy and favorable tolerability profile of fremanezumab, administered as both monthly and quarterly subcutaneous injections, for the preventive treatment of episodic migraine.
Disclosure of Interest
E. Aycardi Conflict with: Teva Pharmaceuticals, M. Bigal Conflict with: Teva Pharmaceuticals, P. Yeung Conflict with: Teva Pharmaceuticals, T. Blankenbiller Conflict with: Teva Pharmaceuticals, M. Grozinski-Wolff Conflict with: Teva Pharmaceuticals, R. Yang Conflict with: Teva Pharmaceuticals, Y. Ma Conflict with: Teva Pharmaceuticals, S. Silberstein Conflict with: Teva Pharmaceuticals, P. J. Goadsby Conflict with: Teva Pharmaceuticals, D. Dodick Conflict with: Teva Pharmaceuticals
Migraine Preventive Therapy
PO-01-202
Evaluating Clinically Meaningful Within-Subject Change in Functioning Associated with Migraine Prevention Using the Migraine Physical Function Impact Diary (MPFID)
Ariane K. Kawata1, Asha Hareendran2, Jiat-Ling Poon1, Andrew Thach3, Pooja Desai3*, Yumi Kubo3, Daniel D. Mikol3, David W. Dodick4, Richard B. Lipton5 and Stewart J. Tepper6
1Evidera – Evidence, Value & Access by PPD, Bethesda, MD, United States
2Evidera – Evidence, Value & Access by PPD, London, United Kingdom
3Amgen Inc., Thousand Oaks, CA
4Department of Neurology, Mayo Clinic Arizona, Phoenix, AZ
5Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY
6Geisel School of Medicine at Dartmouth, Department of Neurology, Dartmouth-Hitchcock Medical Center, Lebanon, NH, United States
Objectives
To establish a clinically meaningful within-patient change (CMWPC) in migraine impact scores as measured by the Migraine Physical Function Impact Diary (MPFID) and to evaluate these CMWPCs in the STRIVE study, a Phase 3 clinical trial of erenumab subjects with episodic migraine (EM).
Methods
MPFID is a 13-item questionnaire that measures the impact of migraine on physical function in the past 24 hours. Monthly MPFID domain scores (Impact on Everyday Activities [EA; 7 items] and Physical Impairment [PI; 5 items]) are based on daily scores averaging across migraine and non-migraine days and range from 0–100 (higher score = greater impact). A Global Impact on Everyday Activities score (G-EA) is generated from a single item. CMWPCs for MPFID were developed using anchor- and distribution-based methods using data pooled across treatment groups from a clinical trial of erenumab for the prevention of migraine (ARISE; NCT02483585) and data from adults with EM who recently initiated or changed their migraine preventive regimen in an observational study. Clinically relevant anchor variables, including ≥30% and ≥50% reduction in monthly migraine days (MMD) and ≥20% and ≥50% reduction in MPFID G-EA score, were used to estimate average within-subject point change from baseline in MPFID domain scores; distribution-based estimates based on variability were considered supportive. These CMWPCs were used to examine the proportion of responders to treatment in a post-hoc analysis of data from the STRIVE study, where adults with EM were randomized 1:1:1 to subcutaneous monthly placebo or erenumab 140 mg or 70 mg for 24 weeks. Cumulative distribution function (CDF) plots were generated to describe % of subjects within each treatment group achieving the range of CMWPCs from baseline in MPFID domain scores.
Results
Using multiple anchors and distribution-based methodology, estimates from the ARISE study and an observational study suggested that CMWPCs starting at 3-point change in MPFID EA and PI domains represented clinically meaningful within-subject change. In the STRIVE study, larger proportions of erenumab-treated subjects than placebo subjects achieved a ≥5-point reduction (pre-specified endpoint) from baseline to mean of weeks 13–24 in PI (140 mg: 42.5%; 70 mg: 39.1% vs placebo: 30.1%, p < 0.05 for both) and EA domain scores (140 mg: 50.3%; 70 mg: 49.0% vs placebo: 34.5%, p < 0.001 for both). Post-hoc analyses as described by CDF curves by treatment groups showed that more subjects in 140 mg and 70 mg erenumab groups compared to placebo had greater reductions in EA and PI domain scores. The erenumab groups had consistently larger proportions of responders compared to placebo starting as low as a 3-point change from baseline score and across a range of CMWPCs.
Conclusion
Reductions starting at 3 points in MPFID domains are representative of CMWPCs. Treatment with erenumab 140 mg and 70 mg in the STRIVE study was related to clinically meaningful reductions in the impact of migraine on physical functioning compared to placebo, based on greater proportions on erenumab experiencing within-subject change of 5 points or more. This supports the utility of MPFID as a marker for migraine clinical benefit and demonstrates the value of erenumab as a preventive therapy to improve functioning in adults with EM.
Disclosure of Interest
A. Kawata Conflict with: Employee of Evidera, A. Hareendran Conflict with: Pfizer Ltd, Conflict with: Employee of Evidera, J.-L. Poon Conflict with: Employee of Evidera, A. Thach Conflict with: Amgen Inc., P. Desai Conflict with: Amgen Inc., Conflict with: Amgen Inc., Y. Kubo Conflict with: Amgen Inc., Conflict with: Amgen Inc., D. Mikol Conflict with: Amgen Inc., Conflict with: Amgen Inc., D. Dodick Conflict with: Epien Medical (Stock), Second Opinion (stock), GBS (stock), Neuroassessment systems (Know-how License with Employer-Mayo Clinic), Conflict with: Served on advisory boards and/or has consulted for Allergan, Amgen, Alder, Dr Reddy’s, Merck, eNeura, Eli Lilly & Company, INSYS therapeutics, Autonomic Technologies, Teva, Xenon, Tonix, Trigemina, and Boston Scientific, GBS, Merck, Colucid, Zosano., Conflict with: Amgen, Conflict with: Received editorial honoraria and/or royalties from Oxford University Press, Cambridge University Press, Web MD. UptoDate, R. Lipton Conflict with: National Institutes of health, the National Headache Foundation, the Migraine Research Fund, Conflict with: Serves as a consultant, serves as an advisory board member, or has received honoraria from Alder, Allergan, American Headache Society, Autonomic Technologies, Boston Scientific, Bristo Myers Squibb, Cognimed, CoLucid, Eli Lilly, eNeura Therapeutics, Merck, Novartis, Pfizer, and Teva, Conflict with: Receipt of royalties: Royalies from Wolff's Headache, 8th Edition (Oxford University Press, 2009), S. Tepper Conflict with: ATI, Conflict with: Alder, Allergan, Amgen, ATI, Avanir, Teva, Zosana, Conflict with: Consultant: Acorda, Alder, Allergan, Amgen, ATI, Avanir, Eli Lilly, Kimberly-Clark, Pernix, Pfizer, Teva, Zosana; Salary: American Headache Society, Conflict with: Advisors board: Allergan, Amgen, ATI, Avanir, BioVision, Dr Reddy's, Kimberly-Clark, Scion Neurostim, Teva, Pfizer, Conflict with: Receipt of royalties: University of Mississippi Press
Headache Pathophysiology – Imaging and Neurophysiology
PO-01-203
Impaired cholinergic transmission in migraine: a short-latency afferent inhibition (SAI) study
Gianluca Coppola1*, Davide Di Lenola2, Francesca Cortese2, Cherubino Di Lorenzo3 and Francesco Pierelli4
1Research Unit of Neurophysiology of Vision and Neurophthalmology, G. B. Bietti Foundation IRCCS, Rome
2Department of medico-surgical sciences and biotechnologies, Sapienza University of Rome Polo Pontino, Latina
3Department of Neurology, Don Gnocchi Foundation-IRCCS, Milan
4Headache Clinic, Neuromed IRCCS, Pozzilli, Italy
Objectives
Short-latency afferent inhibition (SAI) is a form of inhibition related to the cholinergic activity in the cerebral cortex. It consists in an electrical stimulation of a peripheral nerve that can suppress motor cortex excitability, as tested by transcranial magnetic stimulation (TMS), when given at a short interstimulus interval (ISI) between 18 and 21 ms. SAI is considered an in-vivo way to study the sensorimotor integration mechanisms, and is influenced by the excitatory effect of acetylcholinergic thalamocortical afferents on the inhibitory GABAergic (typically GABAa) cortical networks.
Methods
We recruited 30 migraine without aura patients (16 between [MO] and 14 during [MI] attacks), and we compared them to a group of 16 healthy volunteers (HV). We first recorded somatosensory evoked potentials N20 latency and N20-P25 peak-to-peak amplitude at the contralateral parietal area. Afterward, SAI was recorded in all study’s participants as follows: after a conditioning single pulse delivered on the median nerve at the wrist, a TMS pulse was delivered with ISIs derived from the latency of N20 plus 2 to 8 ms in steps of 2 ms and in random order. Five stimuli were delivered at each ISI. We calculated the SAI slope of the linear regression between the unconditioned motor evoked potential (MEP) amplitude and the 4-conditioned MEPs as a measure of cortical excitability.
Results
Compared with HV, SAI was significantly reduced in MO, but enhanced in MI patients (slope HV = +11.2, MO = +242, MI = −129). In both HV and MO groups, but not in MI, the SAI slope positively correlated with the SSEP N20-P25.
Conclusion
The reduction of SAI in MO patients and its enhancement in MI patients suggests a decrease and an increase respectively in facilitatory thalamocortical cholinergic activity on GABAergic network activity in the motor cortex. Since from the correlation analysis emerges that slope of SAI normally correlates with the parietal response in MO, but not in MI, we argue that more dysfunctional sensorimotor integrative mechanisms might characterize migraineurs during an attack.
Disclosure of Interest
None Declared
Headache Pathophysiology – Imaging and Neurophysiology
PO-01-204
Cognitive function performance of migraine in auditory evented-related potential and functional magnetic resonance imaging
Shih C. Sen1*, Liu C. Ju2, Wu M. Ting3 and Cheng P. Wen4
1Department of Neurology, Kaohsiung Veterans General Hospital
2Science Education & Enviromental Education,
3Department of Radiology, Kaohsiung Veterans General Hospital
4Department of Medical Education and Research, Kaohsiung Veterans General Hospital, Taiwan, Republic of China, Kaohsiung, Taiwan
Objectives
Migraine is a common and painful condition that affects many people, predominantly from young adulthood to middle age; the years of maximum work and family commitments. Although treatment guidelines were proposed for acute and preventive treatment of migraine, the pathogenesis of migraine was still uncertain. Recent studies showed learning disabilities and attention deficits disorder in children and adolescents with migraine and adult migraine patients often reported cognitive complaints, especially regarding attention and memory. Cognitive function change in migraine patients was highly suspected. Because the migraine without aura (MoA) patients are more common, we selected MoA patients as experimental group. We hope to compare the difference of brain physiologic & cognitive function change between MoA patients and normal people by these non-invasive electrophysiologic & neuroimaging techniques [auditory event-related potential (ERP) and functional magnetic resonance imaging (fMRI)] and cognitive assessment [Mini-Mental State Examination (MMSE) and Wechsler Memory Scale-Third Edition (WES-III)]. This study showed some cognitive impairment in MoA patients, especial over recall memory and working memory. These cognitive change could be compatible with some findings in these electrophysiologic & neuroimaging techniques.
Methods
Nineteen migraine subjects (M/F = 5/14, age = 42 ± 10 y/o) and thirteen healthy controls (M/F = 5/8, age = 32 ± 9 y/o) who had no history of neurological disease participated in this study. All participants received MMSE (Folstein et al., 1975) & WES-III (Larrabee, 1999) mental tests and auditory ERP & fMRI examinations. The auditory ERP and fMRI examination were performed during the ictal phase of the MoA patients. We used an auditory oddball paradigm to analyze target processing using event-related potentials and measured latency and amplitude of P300 target stimulus in P3, Pz and P4 three sites. We also compared the functional connectivity in resting-state fMRI (rsfMRI) between controls and MoA patients and analyzed the data according to Stanford University laboratory. All imaging data were acquired from a 3.0T MR scanner (Skyra, Siemens, Erlangen, Germany).
Results
Our results showed MoA patients have some cognitive impairment in the total score & recall score in MMSE and index scores & percentiles of working memory in WMS-III. More prolonged distal latency and reduced amplitude P300 target stimulus in the MoA patients. There was decreased functional connectivity in rsfMRI in the basal ganglion, higher visual and primary visual networks of MoA patients.
Conclusion
These results suggested that patients with migraine might present a higher risk of cognitive impairment and the auditory ERP & rsfMRI data provided an evidence of the cognitive dysfunction in these patients.
Disclosure of Interest
None Declared
Cluster Headache and Other Trigeminal Autonomic Cephalalgias
PO-02-149
Infusion of calcitonin gene-related peptide provokes cluster headache attacks
Anne Luise Vollesen1*, Agneta Snoer1, Rasmus Paulin Beske1, Song Guo1, Jan Hoffmann2, Rigmor Højland Jensen1 and Messoud Ashina1
1Neurology, Danish Headache Center, Rigshospitalet Glostrup, Copenhagen, Denmark
2Department of Systems Neuroscience, University Medical Center Eppendorf, Hamburg, Germany
Objectives
To investigate whether calcitonin gene-related peptide (CGRP) provokes cluster headache attacks.
Methods
We randomly allocated 32 cluster headache patients (3 groups: 9 active phase episodic cluster headache, 9 remission phase episodic cluster headache, and 14 chronic cluster headache patients) to receive intravenous infusion of 1.5 µg/min CGRP or placebo over 20 min on two study days separated by at least 7 days. Headache characteristics including cephalic autonomic symptoms were recorded. The primary end-point was difference in incidence of cluster headache attacks within 90 min by CGRP compared with placebo.
Results
CGRP induced cluster headache attacks in 8/9 patients compared to 1/9 after placebo in active phase (P = 0.046). None of the patients in remission phase reported attacks either after CGRP or placebo (P > 0.999). Seven out of 14 patients chronic cluster headache reported attacks after CGRP and none of the patients reported attacks after placebo (P = 0.023). Chronic cluster headache patients who developed attacks had a higher attack burden the month before provocation than those who did not develop attacks.
Conclusion
CGRP provokes cluster attacks in episodic cluster headache in active phase but not in remission. Periodicity or attack burden may influence the incidence of CGRP induced attacks in chronic cluster headache. We suggest that attack induction only during active phase may reflect the hypothalamic control of cluster headache. Our data also cautiously suggest efficacy of CGRP antagonism in the treatment of cluster headache.
Disclosure of Interest
A. L. Vollesen: None Declared, A. Snoer: None Declared, R. P. Beske: None Declared, S. Guo: None Declared, J. Hoffmann Conflict with: Allergan, Autonomic Technologies Inc. (ATI), Chordate Medical AB, Novartis and Teva, Conflict with: Speaking honoraria from Allergan, Novartis and Teva, R. H. Jensen Conflict with: Lectures for Pfizer, Berlin-Chemie, Norspan, Merck and Autonomic Technologies and is a member of the advisory boards of Autonomic Technologies, Medotech and ElectroCore., M. Ashina Conflict with: Alder, Allergan, Amgen, ATI and Eli Lilly., Conflict with: Speaking/teaching fees, honoraria Alder, Allergan, Amgen, ATI and Eli Lilly.
Cluster Headache and Other Trigeminal Autonomic Cephalalgias
PO-02-150
Chronic cluster headache is associated with traumatic head injury and familial cluster headache
Rasmus P. Beske1*, Nunu Lund1, Mads Barløse2, Anja Petersen1 and Rigmor H. Jensen1
1Dept. of Neurology
2Dept. of Clinical Physiology, Nuclear Medicine and PET, Danish Headache Center, Glostrup, Denmark
Objectives
We wish to describe the clinical differences between the chronic (cCH) and episodic (eCH) form of cluster headache (CH) and the association with familial CH and traumatic head injury (THI).
Methods
Patients from the Danish Cluster Headache survey aged 18–65 years, diagnosed with CH according to ICHD-II, completed questionnaires and structured interviews. Familial CH was defined as either one or more 1st or 2nd degree relative with CH.
Results
400 patients (cCH: 154 and eCH: 246) and 200 headache-free controls participated. cCH patients reported longer attack duration with treatment (47 min vs. 34 min, p < 0.05), more attacks per day (4.07 vs 3.33, p < 0.01 than in eCH patients) and autonomic symptoms as ptosis (60 % 48 %, p < 0.05) and eyelid edema (34 % vs 23 % p < 0.05) were also more frequently reported in cCH than eCH.
A history of CH within the family was more frequent among patients than controls (16.75 % vs 2.5% p < 0.0001), and in addition more frequent among cCH than eCH (23 % vs 13 %, p < 0.05). THI was also more frequent in patients vs controls (43% vs 25%, p < 0.0001) and was reported more often in cCH patients than in eCH (53 %, vs 38 %, p < 0.01). THI was not more frequent among sporadic CH than familial CH (43 % vs 46 %, p = 0.68)
Conclusion
Not only the duration of the remission period differ between cCH and eCH patients, but cCH patients also experience more frequent and longer lasting attacks compared with eCH patients. Despite our expectation, THI was not more frequent in sporadic CH than in familial CH, and this may indicate that THI is not at risk factor for developing CH. Further, familial CH is more frequently reported in cCH than in eCH which could point to differences in heritability and genetic load. Consequently, it is pivotal for future genetic studies to address the difference between the two phenotypes.
Disclosure of Interest
None Declared
Cluster Headache and Other Trigeminal Autonomic Cephalalgias
PO-02-151
Epidemiologic study of cluster headache prevalence in a medium-size city of brazil
Mauro Eduardo Jurno1*, Carlos Alberto Bordini2, Bárbara S. R. Pereira1, Felipe A. S. Fonseca1, Gabriel A. Teixeira1, Ludimila Q. Maffia1, Maria R. A. Barros1 and Vívian F. Camilo1
1Neurologia, Faculdade de Medicina de Barbacena, Barbacena
2Neurologia, Clinica Neurologica de Batatais, Batatais, Brazil
Objectives
To determine the prevalence of cluster headache (CH) in Barbacena, a medium size city in the State of Minas Gerais, Brazil.
Methods
The total population of Barbacena, totals 126.284 inhabitants and Family Health Strategy Program covers 84.610 of them. In order to identify patients with cluster headache, 36.145 of these were screened following which aquestionnaire was completed by 181 health agents, distributed among the 28 health posts belonging to the Family Health Strategy network. The completed questionnaires were selected based on the clinical criteria established by the International Headache Society, and those patients (aged 18 year of age or over) with a possible CH diagnosis were later assessed by a headache specialist. This is an observational, cross-sectional study.
Results
In all, 15 patients were diagnosed as having CH, comprising a prevalence of 0.0414%; or 41.4/100,000 inhabitants.
Conclusion
Cluster Headache prevalence in Barbacena is lower than that observed in many locations worldwide.
Disclosure of Interest
None Declared
Epidemiology
PO-02-152
Exploring insulin resistance in migraine: a population-based study
Sylvie Streel1*, Jean Schoenen2 and Michèle Guillaume1
1Department of Public Health, Liege University
2Department of Neurology, Headache Research Unit, CHR Citadelle, Liege, Belgium
Objectives
An association between migraine and insulin resistance (IR) has been reported in some studies but data are conflicting. This study aimed to assess IR according to migraine type in the general population.
Methods
Among the 751 participants to the NESCaV population survey, 116 were migraineurs without aura (MO) and 79 were migraineurs with aura (MA). Diagnosis of migraine was based on the ef-ID migraine questionnaire. All participants had a clinical examination, a general blood test and filled-out a self-administered questionnaire. The homeostatic model assessment of IR (HOMA-IR), b-cell function (HOMA-B) and the quantitative insulin sensitivity check index (QUICKI) were used to calculate IR. Data were analyzed by weighted regression procedures and reported as means with 95% confidence interval (95%CI).
Results
After adjusting for stratification (gender, age, district) and other factors (smoking, physical inactivity, arterial hypertension, dyslipidemia, body mass index, antidiabetics and corticosteroids treatment), MA subjects presented lower fasting blood glucose levels than non-migraineurs and MO subjects: 5.05 (95%CI: 4.83–5.29) vs. 5.26 (5.01–5.51) vs. 5.31 mmol/L (5.03–5.61), respectively (p = 0.018). A significant difference in HOMA-B was observed between MA subjects, non-migraineurs and MO subjects: 111 (95%CI: 92–134) vs. 95 (80–111) vs. 95 (76–117), respectively (p = 0.037). No difference was observed for insulin (p = 0.60), HOMA-IR (p = 0.83) and QUICKI (p = 0.71).
Conclusion
This population-based study demonstrated a decrease in fasting blood glucose levels and an increase of HOMA-B scores in MA subjects. These findings highlight the importance of a systematic exploration of glucose metabolism especially in MA subjects, already known to be more exposed to cardiovascular diseases.
Disclosure of Interest
None Declared
Headache and Gender
PO-02-153
Untangling the burden of menstrual migraine from headache day frequency: Results from the 2017 Migraine in America Symptoms and Treatment (MAST) Study
Jelena M. Pavlovic1, Michael L. Reed2, Kristina M. Fanning2, Sagar Munjal3, Aftab Alam3, Todd J. Schwedt4, David W. Dodick4, Dawn C. Buse1 and Richard B. Lipton1
1Department of Neurology, Albert Einstein College of Medicine, Bronx
2Vedanta Research, Chapel Hill
3Clinical Development, Promius Pharma, Princeton
4Neurology, Mayo Clinic, Phoenix, United States
Objectives
Among women of child-bearing potential who have migraine, the International Classification of Headache Disorders characterizes pure menstrual migraine (PMM), menstrually related migraine (MRM) and non-menstrual migraine (NMM). The objective of this study was to assess the relative frequency and burden of migraine in a population sample of women representing these 3 migraine subtypes.
Methods
Survey data were obtained from a general US population sample of women with migraine from the 2017 Migraine in America Symptoms and Treatment (MAST) Study. The survey collected sociodemographic features, headache characteristics, time since most recent menstruation, use of exogenous hormones and data on the relation of headache to the menstrual cycle. Eligible women were <55 years old, met ICHD criteria for migraine and reported at least one period in the last 12 months. Modified ICHD-3 beta diagnostic criteria were used via a validated questionnaire to screen women for migraine and to classify them as PMM, MRM or NMM. The burden of migraine was assessed using the Migraine Disability Assessment Scale (MIDAS: cut point 310, moderate-to-severe disability) and a 4-item measure of anxiety and depression (Patient Health Questionnaire, PHQ-4: cut point of 36, moderate-to-severe depressive and anxious symptomology). Allodynia was assessed using the 12-item Allodynia Symptom Checklist, (ASC-12: cut point of 33, presence of cutaneous allodynia). In order to assess the burden of menstrually related attacks independent of headache frequency, binary logistic regression contrasted women who met criteria for PMM and MRM with a NMM reference group. Covariates included headache day frequency, highest headache intensity, age, race, BMI and the use of exogenous hormones.
Results
Among 9,953 women meeting criteria for migraine, 6,269 met the additional inclusion criteria for the analysis (mean age 34.7, 74.8% Caucasian). Women were classified as PMM (n = 271, 4.3%), MRM (n = 2,374, 37.9%) or NMM (n = 3,624, 57.8%) based on their retrospective self-report of timing for migraine headache attacks in the prior 3 months. Women with PMM were somewhat older (Chi 51.5, p < .001) and more likely to be married (Chi 17.0, p < .001). A higher proportion of the MRM group had high disability, psychological symptomology, attack–related allodynia symptoms, and higher average monthly headache day frequency (PMM 2.8 days, MRM 4.7 days and NMM 3.5 days). After adjusting for covariates, PMM and NMM did not differ in the aforementioned outcomes. In comparison with the NMM group, the MRM group had higher odds of moderate-to-severe disability (OR 1.30, CI 1.15, 1.47) and higher odds of ictal allodynia (OR 1.28, CI 1.15, 1.43). There were no differences in psychological symptomology (OR 1.04, CI 0.92, 1.19).
Conclusion
MRM was diagnosed in 38% of our sample. Independent of overall headache frequency, these women were more likely to have moderate-to-severe headache-related disability and more likely to report attack-related allodynia than women with NMM or PMM. The greater burden in MRM may reflect biological differences among these subgroups. While the underlying factors that contribute to higher disability and allodynia in the MRM group requires further investigation, these findings confirm a need for more effective methods to reduce the burden of MRM.
Disclosure of Interest
J. Pavlovic Conflict with: Received honoraria from Allergan plc, Dr. Reddy’s Laboratories/Promius Pharma, and the American Headache Society, M. Reed Conflict with: Received support funded by Allergan, CoLucid, Dr. Reddy’s Laboratories/Promius Pharma, Endo Pharmaceuticals, GlaxoSmithKline, Merck & Co., Inc., NuPathe, Novartis, and Ortho-McNeil, via grants to the National Headache Foundation., Conflict with: Received support funded by Allergan, CoLucid, Dr. Reddy’s Laboratories/Promius Pharma, Endo Pharmaceuticals, GlaxoSmithKline, Merck & Co., Inc., NuPathe, Novartis, and Ortho-McNeil, via grants to the National Headache Foundation., K. Fanning Conflict with: Received support funded by Allergan, CoLucid, Dr. Reddy’s Laboratories/Promius Pharma, Endo Pharmaceuticals, GlaxoSmithKline, Merck & Co., Inc., NuPathe, Novartis, and Ortho-McNeil, via grants to the National Headache Foundation., S. Munjal Conflict with: Dr. Reddy’s Laboratories and owns stock in the company., A. Alam Conflict with: Dr. Reddy’s Laboratories and owns stock in the company., T. Schwedt Conflict with: Stock options from GBS Ventures and Second Opinion and Royalties from UpToDate., Conflict with: Received grant support from the National Institutes of Health, the US Department of Defense, the Patient Centered Outcomes Research Institute, the American Migraine Foundation, Arizona State University, and the Mayo Clinic., Conflict with: Serves as a consultant, advisory board member, or has received honoraria from Allergan, Amgen, American Headache Society, Autonomic Technologies, Avanir, Dr. Reddy’s Laboratories/Promius Pharma, GBS Ventures, Novartis, Second Opinion, Supernus, and Teva, D. Dodick Conflict with: Stock/options: GBS/Nocira, Epien, and Mobile Health., Conflict with: Consulting fees: Acorda, Allergan, Amgen, Alder, Dr. Reddy’s Laboratories/Promius Pharma, Merck, Dr Reddy’s, Promius, eNeura, Eli Lilly & Company, Insys therapeutics, Autonomic Technologies, Teva, Xenon, Tonix, Trigemina, Boston Scientific, GBS, Colucid, Zosano, Laydenburg Thalmann, Biocentric, Pfizer (Japan)Royalties: Oxford University Press and Cambridge University Press (Book Royalty) Uptodate – editorial/honoraria. CME companies honoraria/publishing honoraria/royalites: Chameleon Communications, Medscape, WebMD, Academy for Continued Healthcare Learning, Haymarket Medical Education, Global Scientific Communications, HealthLogix, Academy for Continued Healthcare Learning, Meeting LogiX, Health LogiX, Wiley Blackwell, Oxford University Press, Cambridge University Press. Consulting use agreement: NAS. Board position: King-Devick Inc., D. Buse Conflict with: grant support and honoraria from Allergan, Avanir, Dr. Reddy’s Laboratories/Promius Pharma, and Eli Lilly., Conflict with: She is an employee of Montefiore Medical Center, which has received research support funded by Allergan, CoLucid, Endo Pharmaceuticals, GlaxoSmithKline, MAP Pharmaceuticals, Merck, NuPathe, Novartis, Ortho-McNeil, and Zogenix, via grants to the National Headache Foundation., Conflict with: Editorial Board of the Current Pain and Headache Reports, Journal of Headache and Pain, Pain Medicine News, and Pain Pathways magazine., R. Lipton Conflict with: Received grant support from the National Institutes of Health, the National Headache Foundation, and the Migraine Research Fund., Conflict with: He serves as consultant, serves as an advisory board member, or has received honoraria from Alder, Allergan, American Headache Society, Autonomic Technologies, Boston Scientific, Bristol Myers Squibb, Cognimed, CoLucid, Dr. Reddy’s Laboratories/Promius Pharma, Eli Lilly, eNeura Therapeutics, Merck, Novartis, Pfizer, and Teva, Inc. He receives royalties from Wolff’s Headache, 8th Edition (Oxford University Press, 2009).
Headache and Gender
PO-02-154
Etiological beliefs and experiences of gender suffering with headaches at the University Hospital Teaching Center of Yaounde(UHTCY)
Loveline FRI FON1*
1Comunity Healthcare Awarenes Center Cameroon, Douala, Cameroon
Objectives
To descript the etiological beliefs of headaches according to gender and how these headaches are treated.
Methods
This descriptive and qualitative study was conducted from September 25th to December 12th, 2016 at the University Hospital Center of Yaounde. The study population consisted of 12 patients and spouses of five patients. Data was collected on the etiological beliefs of sufferers, self-esteem and relationship withrelatives. An interview guide and a sound recorder were used for data collection. The analysis consists in gathering information according to the objectives.
Results
Patients ages varied from 3 to 68 years old. Etiological factors reported by patients included; aging (1/12); diabetes(1/12); spinal diseases(1/12); hormonal changes in women(7/12) child birth(4/12) and mysticism(8/12). Three children between the ages 3 to 11 years did not mention any etiological factor. Relationships with relatives have been destabilized with the husbandfor one woman and with the family in-laws for another one. Other relationships have been more bonding as partners turn to be more affectionate.
Conclusion
Most of the sufferer mentioned the etiological factors listed above. Some have gone into depression because of a destabilized relationship with the family.
Sensitization on early medical consultation and treatment could be of great importance.
Disclosure of Interest
None Declared
Headache Classification
PO-02-155
Incorrect patient perception of the number of Headache types they have
Alan Rapoport1*, Jim Blythe2 and Rob Cowan3
1UCLA
2Information Sciences Institute, USC, Los Angeles
3NEUROLOGY, STANFORD UNIVERSITY, PALO ALTO, United States
Objectives
Most patients who think they have several headache types, actually have only migraine. Many patients report several headache types with varying symptoms and carry multiple headache diagnoses. This often results in excessive testing and inappropriate treatments. The objective of this work is to determine how often a patient's perception of the number of different types of headache they have is accurate.
Methods
We reviewed 3118 reports generated by a validated on-line questionnaire from BonTriage with responses tied to ICHD 3 beta diagnostic criteria. Patients were asked how many distinct headache types they had, and then were queried in detail about each type We then used ICHD diagnostic criteria to form clinical impressions. A rule-based engine was then used to generate these diagnoses.
Results
3118 patient histories were collected and analyzed. Of these, 1622 reported 1 headache type, 1020 reported 2, and 476 reported more than 2. Migraine was a frequent diagnosis. Many patients with one type of migraine and other headaches there were similar to tension-type headache had only the diagnosis of chronic migraine.
Conclusion
It appears from this study that patient's perception of multiple headache types is accurate only 29% of the time. When more than one headache type is reported, the most common headaches represented are migraine or chronic migraine or migraine with head trauma. Chronic migraine is also seen. This study suggests that further education regarding the natural history of migraine and how it presents is an important educational element often lacking in the management of migraine.
Disclosure of Interest
None Declared
Headache Classification
PO-02-156
Chronic Secondary Headache in Children: A Case Report
Rizqi R. Pikir1*, Sitti Radhiah1, Aminuddin Harahap1, Retno Wisanti1, Fadjar Aribowo1, Bing Rudyanto1 and Budi Muliantoro1
1Pediatrics, Hang Tuah Medical Faculty – Dr. Ramelan Navy Hospital, Surabaya, Indonesia
Objectives
Headache is a common reason for pediatric patients to seek medical care. Headaches can result from any of a number of causes, including genetic predisposition, trauma, an intracranial mass, a metabolic or vascular disease, or sinusitis. Recognition that pediatric headaches can result from primary and secondary causes is crucial to their treatment.
Methods
Male 8-years old with severe headache. Throbbing pain felt in his face (around the eyes, cheeks and forehead), both sides affected with right more dominant. The pain get worsen in the morning, when moving his head, strain or bend down, and when experience extreme changes in temperature. The pain was almost daily in the last five months and last for 15–45 minutes during attack, followed by pain free between attacks. He also had chronic rhinitis since couple years ago. Physical and neurological examinations were normal. Numeric Rating Scale (NRS) was 10 during acute attacks. He was referred from primary healthcare service and ever treated with paracetamol, ibuprofen but no reduction either in intensity or frequency of pain. The head X-Ray and CT-Scan resulted normal condition, but the head MRI showed bilateral sphenoidalis sinusitis and ethmoidalis sinusitis. Then he was given a combination of paracetamol, decongestan and board spectrum antibiotics for sinusitis.

Results
Patients had remission of cluster headache period within 7 days of treatment with combinations of paracetamol with tramadol as abortive treatments, decongestan and amoxicillin with clavulanic acid 50 mg/kg/day three daily for 10 days as initial treatment. There were no attacks anymore. NRS reduce until zero. Sinus headaches are an uncommon type of headache caused by inflamed sinuses (sinusitis). Sinus headache typically occurs in the area of the sinuses in the area of the cheeks (maxillary sinus), bridge of the nose (ethmoid sinus), or above the eyes (frontal sinus). Less often it may refer pain to the top or back of the head (sphenoid sinus. Sinus headache may occur on one side or both sides of the head and the neck is typically not involved. The symptoms are frequently worsened by bending over or coughing (as with migraine), and examination of the facial area may reveal local tenderness, redness, swelling, and possibly the presence of clear or discolored nasal discharge. Sinus disease can happen to people who suffer from migraine or to those who do not and may lead to increased migraine activity in migraine sufferers, often confusing the diagnosis. Upon determining that a headache's origin is a sinus infection, short-term antibiotics (typically less than 2 weeks) and decongestants (several days only) may be prescribed. Allergic sinusitis may respond to simple antihistamine and steroid-based nasal sprays. A chronic sinus infection may require weeks of therapy, various antibiotic regimens, or the judicious use of supportive steroid preparations. Sometimes nasal surgery is indicated to correct underlying anatomical factors.
Conclusion
The initial presentation of sinus infection is so similar to migraine that it is often mistakenly diagnosed and treated like just another headache. However, despite overlapping symptoms, differences between the two entities can be distinguished through a careful evaluation.
Disclosure of Interest
None Declared
Headache Education for Clinicians and Patients
PO-02-157
The Prevalence and Characteristics of Cranial Autonomic Symptoms (CAS) in Migraine Patients with or without Aura
Mansoureh Togha1*, Abolfazl Farbod2 and Zeinab Ghorbani3
1Headacahe, Iranian Center of Neurological Researches, Neuroscience Institute
2Headacahe department
3Headacahe, Iranian Center of Neurological Research, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran, Islamic Republic Of
Objectives
Cranial autonomic symptoms (CAS) include a broad spectrum of symptoms such as conjunctival injection, lacrimation, nasal congestion, eyelid oedema, forehead or facial sweating, miosis, ptosis and facial flushing which all are key features of trigeminal autonomic cephalalgias (TACs). However, CAS may also present with migraine attacks. Based on the literature, compared with TACs patients, these symptoms are more bilateral, less severe, often unrelated to the headache side and less dependent to headache attack in migraine patients. It has been also reported that CAS can occur in 27% to 73% of migrainures. In this study we aimed to explore the prevalence and characteristics of CAS in migraine with and without aura.
Methods
This retrospective study was conducted on patients with migraine diagnosis referred to a private headache clinic in Tehran between January 2011 to January 2015. Migraine diagnosis was based on the latest international headache society criteria (ICHD III). Medical records, status of CAS and other non-autonomic parameters of patients with migraine (with or without aura) were recorded. Data analysis was performed using SPSS19.
Results
Of 657 patients (aged 38.78 ± 14.15 years), 68.6% were female, and 60.1% had episodic migraine. Regarding headache characteristics, in 40.6% of patients it was unilateral. The mean frequency and intensity of headache were 7.83 ± 1.71 and 13.28 ± 8.48 days, respectively. The prevalence of CAS was as follows: conjunctival injection (28.9%), lacrimation (24.4%), nasal congestion (15.2%), ear fullness (15.2%), rhinorhea (11%), eyelid oedema (10.2%), forehead or facial sweating (4.9%), flushing (4.1%), ptosis (2.1%) and miosis (0.9%). 64.2% of patients had at least one CA symptom. Presence of CAS was significantly higher in migraineurs with aura (80.6%) than those without aura (61.4%, (p = 0.00)). However, CAS did not differ between patients with unilateral and bilateral headaches. Tearing and nasal congestion were also significantly more prevalent in patients with more severe and frequent headaches (17.3%, 15.0%, 25.2% and 17.0%, respectively p < 0.05) than others.
Conclusion
Due to high prevalence of CAS in our study, these symptoms might not be a specific characteristic of TACs, especially for differentiation of hemicrania continua that share some common characteristics with chronic migraine. Also, these finding may raise a question about the possible distinctive therapeutic approaches in migraine with and without autonomic features. Our findings further confirm the idea of involvement of trigeminal autonomic reflex in the migraine headaches. Furthermore, the presence of CAS might be a sign of migraine progression. Larger prospective studies are suggested for more precise results.
Disclosure of Interest
None Declared
Headache Epidemiology, Outcomes and Burden
PO-02-159
Characteristics and diagnoses of acute headache in pregnant women–a retrospective cross-sectional study
Bianca Raffaelli1, Eberhard Siebert2, Heike Israel-Willner1, Jeannette Körner1, Thomas Liman1, Uwe Reuter1, Lars Neeb1*
1Department of Neurology with Experimental Neurology
2Institute of Neuroradiology, Charité Universitätsmedizin Berlin, Berlin, Germany
Objectives
Acute headache is one of the most frequent neurological symptoms in pregnant women. Early diagnosis of underlying secondary conditions has a major influence on patient outcome, especially in emergency settings. However, at the time being no well-established guideline for diagnostic evaluation of acute headache during pregnancy exists. We aimed to characterize acute headache in pregnant women in a European urban population concerning demographic, clinical, and diagnostic features, and to determine predictors of secondary headache.
Methods
We analysed retrospectively the data of 151 pregnant women who received neurological consultation due to acute headache between 2010 and 2016 at the Charité hospital in Berlin, Germany. To assess risk factors for secondary headache in these patients we compared multiple anamnestic and clinical features of the primary and secondary headache group. Subgroup proportions were compared using chi-squared test. Logistic regression was used to assess the correlation between clinical features with a p value ≤0.02 in univariate analyses as independent variables and the dependant variable being the final diagnosis secondary headache.
Results
Patients had a mean age of 30.1 (IQR 10.0) years, a mean gestational age of 22.2 (±10.1) weeks and 2.1 (±1.7) pregnancies. 57.6% of the patients were diagnosed with primary headache, most common migraine with aura (41.3%), migraine without aura (33.3%) and tension type headache (21.8%). Within secondary headaches, the most common aetiologies were infections (29.7%) and hypertensive disorders (22.0%). The primary and secondary headache group were similar in most anamnestic and clinical features. In univariate analysis, secondary headaches were associated with complications during current pregnancy (28.1 vs. 12.6%, p = 0.017), history of secondary headache disorders (14.1 vs. 3.4%, p = 0.017), progressive pain dynamic (37.2 vs. 19.3%, p = 0.046), seizures (4.7 vs. 0.0%, p = 0.041), abnormal internal examination (15.9 vs. 4.8%, p = 0.025), elevated blood pressure (31.7 vs. 8.4%, p < 0.001), fever (14.1 vs. 1.1%, p = 0.002) and abnormal neurological examination (35.9 vs. 11.5%, p < 0.001). In multivariate logistic regression, history of secondary headache disorders [OR 6.6; 95% CI 1.3–33.1], elevated blood pressure [OR 7.2; 95% CI 2.3–22.6], fever [OR 12.1; 95% CI 1.3–111.0] and abnormal neurological examination [OR 9.9; 95% CI 2.7–36.3] represented independent predictors for secondary headache. Regarding additional diagnostic procedures, blood tests were conducted in 94.7% of the cases, urine analysis in 57%, lumbar puncture in 13.2% and neuroimaging in 50.3%. Abnormal thrombocytes, GOT, GPT and CRP, proteinuria, as well pathologic results of lumbar puncture and/or neuroimaging were associated with secondary headache.
Conclusion
Secondary headache disorders are common during pregnancy, occurring in over one third of acute headache cases receiving neurological consultation. Most anamnestic and clinical features may not allow a clear distinction between primary and secondary headaches. Clinicians should pay particular attention in presence of secondary headache history, elevated blood pressure, fever and abnormal findings in the neurological examination. These symptoms can be considered as predictors for secondary headache in pregnant women. However, attack features alone cannot adequately discriminate between primary and secondary headache. Additional diagnostic investigations, including laboratory tests and neuroimaging, are essential for the diagnostic process.
Disclosure of Interest
None Declared
Headache Epidemiology, Outcomes and Burden
PO-02-160
Predictors of Allodynia in Persons with Migraine: Results from the 2017 Migraine in America Symptoms and Treatment (MAST) Study
David W. Dodick1*, Michael L. Reed2, Kristina M. Fanning2, Sagar Munjal3, Aftab Alam3, Dawn C. Buse4, Todd J. Schwedt1 and Richard B. Lipton4
1Neurology, Mayo Clinic, Phoenix
2Vedanta Research, Chapel Hill
3Clinical Development, Promius Pharma, Princeton
4Department of Neurology, Albert Einstein College of Medicine, Bronx, United States
Objectives
Prior work has identified associations between cutaneous allodynia, increased migraine day frequency and inadequate acute treatment response. The objectives of this study were to 1) estimate rates of allodynia in migraineurs who met ICHD-3beta medication overuse (MO) criteria vs. those who did not (nonMO), and 2) determine the influence of headache day frequency and other relevant covariates on the presence of allodynia.
Methods
Participants in the MAST Study were recruited from a nationwide online research panel. Stratified random sampling identified a representative cohort of individuals aged ≥18. A validated migraine diagnostic screen using modified ICHD-3β criteria identified individuals with migraine. Those averaging at least 1 headache day per month over the previous 3 months who reported the use of acute migraine medication(s) were eligible to participate. The presence of cutaneous allodynia on days with headache was identified using the Allodynia Symptom Checklist (ASC-12, score ≥3). ICHD-3β criteria were used to identify MO and nonMO respondents based on monthly usage frequency of acute medications. Binary logistic regression modeling included the following covariates: monthly headache frequency category (1–4, 5–9, 10–14, ≥15 days/month), a pain intensity measure (0–10 intensity rating), the migraine symptom severity score (MSSS) sum, sociodemographics (age, gender, race, income, BMI, smoking) and depression and anxiety symptomology (PHQ-4, sum score ≥6). Allodynia was treated as a dichotomous outcome. Covariates were added to the model in a hierarchal manner and retained if significant. Odds ratios (OR) and 95% confidence intervals (CI) are provided for models and Chi-square tests (p < .05) for group comparisons.
Results
N = 117,150 individuals responded to an email survey invitation about health issues; 95,821 surveys were usable and matched US Census on sex, age, and income. A total of 14,396 acute medication users met inclusion criteria. Mean age was 43.4 years, 73.1% were women, 81.5% were Caucasian, 70.8% were employed full- or part-time and 40.1% met criteria for allodynia. 50% of MO respondents met criteria for allodynia vs 37.5% of nonMO respondents (p < .001). The unadjusted logistic model (OR 1.68, CI 1.55, 1.83) indicated that MO respondents were 68% more likely to report cutaneous allodynia vs. nonMO respondents. The OR was attenuated somewhat with the addition of PHQ/psychological symptomology to the model (OR 1.55, CI 1.42, 1.69), and was attenuated further with the addition of headache frequency and intensity covariates (OR1.15, CI 1.04, 1.27) but retained significance (p = 0.006). Modeling results also found being female was associated with increased odds of having allodynia (OR 1.71, CI 1.57, 1.87), as was being Caucasian (OR 1.16, CI 1.05, 1.27). The presence of PHQ/psychological symptomology (OR 1.83, CI 1.68, 2.00), having frequent (≥15 days/month) headache (OR 1.41, CI 1.23, 1.61 vs. 1–4 headache days/month reference group), increasing MSSS (1.17, CI 1.15, 1.19) and pain intensity (OR 1.11, CI 1.08, 1.14) were also associated with greater odds of having cutaneous allodynia.
Conclusion
Attack-related cutaneous allodynia is associated with medication overuse even when relevant covariates (headache frequency, headache intensity, sociodemographics and psychological symptomology) are accounted for. This finding supports the clinical approach of minimizing the overuse of acute medications. Other factors associated with the presence of allodynia included symptoms of depression and anxiety, headache frequency, headache intensity and being female
Disclosure of Interest
D. Dodick Conflict with: Stock/options: GBS/Nocira, Epien, and Mobile Health., Conflict with: Consulting fees: Acorda, Allergan, Amgen, Alder, Dr. Reddy’s Laboratories/Promius Pharma, Merck, Dr Reddy’s, Promius, eNeura, Eli Lilly & Company, Insys therapeutics, Autonomic Technologies, Teva, Xenon, Tonix, Trigemina, Boston Scientific, GBS, Colucid, Zosano, Laydenburg Thalmann, Biocentric, Pfizer (Japan) Royalties: Oxford University Press and Cambridge University Press (Book Royalty) Uptodate – editorial/honoraria. CME companies honoraria/publishing honoraria/royalites: Chameleon Communications, Medscape, WebMD, Academy for Continued Healthcare Learning, Haymarket Medical Education, Global Scientific Communications, HealthLogix, Academy for Continued Healthcare Learning, Meeting LogiX, Health LogiX, Wiley Blackwell, Oxford University Press, Cambridge University Press. Consulting use agreement: NAS. Board position: King-Devick Inc., M. Reed Conflict with: Received support funded by Allergan, CoLucid, Dr. Reddy’s Laboratories/Promius Pharma, Endo Pharmaceuticals, GlaxoSmithKline, Merck & Co., Inc., NuPathe, Novartis, and Ortho-McNeil, via grants to the National Headache Foundation., K. Fanning Conflict with: Received support funded by Allergan, CoLucid, Dr. Reddy’s Laboratories/Promius Pharma, Endo Pharmaceuticals, GlaxoSmithKline, Merck & Co., Inc., NuPathe, Novartis, and Ortho-McNeil, via grants to the National Headache Foundation., S. Munjal Conflict with: Employee of Dr. Reddy’s Laboratories and owns stock in the company., A. Alam Conflict with: Employee of Dr. Reddy’s Laboratories and owns stock in the company., D. Buse Conflict with: Grant support and honoraria from Allergan, Avanir, Dr. Reddy’s Laboratories/Promius Pharma, and Eli Lilly., Conflict with: Employee of Montefiore Medical Center, which has received research support funded by Allergan, CoLucid, Endo Pharmaceuticals, GlaxoSmithKline, MAP Pharmaceuticals, Merck, NuPathe, Novartis, Ortho-McNeil, and Zogenix, via grants to the National Headache Foundation., Conflict with: Editorial Board of the Current Pain and Headache Reports, Journal of Headache and Pain, Pain Medicine News, and Pain Pathways magazine., T. Schwedt Conflict with: Stock options from GBS Ventures and Second Opinion and Royalties from UpToDate., Conflict with: Received grant support from the National Institutes of Health, the US Department of Defense, the Patient Centered Outcomes Research Institute, the American Migraine Foundation, Arizona State University, and the Mayo Clinic., Conflict with: Serves as a consultant, advisory board member, or has received honoraria from Allergan, Amgen, American Headache Society, Autonomic Technologies, Avanir, Dr. Reddy’s Laboratories/Promius Pharma, GBS Ventures, Novartis, Second Opinion, Supernus, and Teva., R. Lipton Conflict with: Received grant support from the National Institutes of Health, the National Headache Foundation, and the Migraine Research Fund., Conflict with: Serves as consultant, serves as an advisory board member, or has received honoraria from Alder, Allergan, American Headache Society, Autonomic Technologies, Boston Scientific, Bristol Myers Squibb, Cognimed, CoLucid, Dr. Reddy’s Laboratories/Promius Pharma, Eli Lilly, eNeura Therapeutics, Merck, Novartis, Pfizer, and Teva, Inc. He receives royalties from Wolff’s Headache, 8th Edition (Oxford University Press, 2009).
Headache Epidemiology, Outcomes and Burden
PO-02-161
An Online Survey of Patients with Hemiplegic Migraine
Celene Grayson1, Emma L. Leach2 3, Simon N. Pimstone1 4, Robin Sherrington1, David Monteith1, Yigal P. Goldberg1*
1Xenon Pharmaceuticals Inc., Burnaby, Canada
2Former Employee, Xenon Pharmaceuticals Inc., Burnaby
3Heart Centre, St. Paul's Hospital
4Department of Medicine, Division of General Internal Medicine, University of British Columbia, Vancouver, Canada
Objectives
Hemiplegic migraine (HM) is a rare type of migraine with aura with a unique genetic etiology, pathophysiology and a distinct and defining clinical characteristic of motor weakness. HM exists in either a familial (FHM) or sporadic (SHM) form depending on the presence of a family history. Due to the rarity of HM, there is a paucity of data regarding the spectrum of the HM phenotype. The objective of this study was to conduct an online survey in order to better understand the variability in the symptomatology of HM attacks, the use of medications to treat or prevent HM attacks and to explore the burden of the disorder in patients with HM.
Methods
A detailed questionnaire was developed to obtain self-reported data from patients who experience HM symptoms. The patient questionnaire was hosted online and comprised 45 questions investigating demographic information, aura symptoms, HM attacks, other migraine attacks, family history, comorbidities and medication use. Free text boxes were included throughout the questionnaire to collect qualitative data from patients regarding the impact of HM symptoms on their lives. Patients were also asked if their diagnoses came from a physician and the specialty of the physician. Online patient responses were screened for study eligibility using the 3rd International Classification of Headache Disorders (ICHD-3 beta) diagnostic criteria for HM, with individual follow-up by email or telephone interview where necessary. 380 patients who met the ICHD-3 beta criteria for HM were enrolled into the study for this analysis, however, the study is still open and collecting additional patient responses. The patient survey protocol and questionnaire were approved by an independent institutional review board (Veritas).
Results
Patients reported the onset of HM attacks between 2–65 years of age with 56% reporting an onset at ≤30 years of age. Attacks including motor weakness occurred at least once a month in 76% of patients and 69% reported that motor weakness occurred in every attack. The duration of motor weakness during an attack was variable and ranged from minutes to days, typically lasting up to 2 hours in 37% of the patients, however, 12% of patients reported motor weakness persisting more than 72 hours. 67% of the respondents had been diagnosed by a physician, of which 86% were either a neurologist or headache specialist. Frequently reported consequences of HM in patients' lives included impacts on eating and drinking, driving, working and self-care in addition to significant physical, social and emotional impacts. 51% of patients reported they are currently taking a preventive medication, the most common of which was topiramate, while amitriptyline, verapamil and propranolol were the next most frequently used. Only 13 to 34% of patients are currently on or continuing to take any of these reported medications, suggesting a 66 to 87% rate of treatment failure.
Conclusion
HM is a highly variable and often severely debilitating disorder. Many patients who experience hemiplegic migraine symptoms have difficulty in obtaining a diagnosis from a knowledgeable medical practitioner. There is no current standard of care for this condition and current therapies appear to have a high failure rate.
Disclosure of Interest
C. Grayson Conflict with: Xenon Pharmaceuticals Inc., E. Leach: None Declared, S. Pimstone Conflict with: Xenon Pharmaceuticals Inc., R. Sherrington Conflict with: Xenon Pharmaceuticals Inc., D. Monteith Conflict with: Xenon Pharmaceuticals Inc., Y. Goldberg Conflict with: Xenon Pharmaceuticals Inc.
Headache Epidemiology, Outcomes and Burden
PO-02-162
Inpatient Detoxification in Medication Overuse Headache – 32 Years Experience in 807 Patients
Sabine Salhofer-Polanyi1, Karin Zebenholzer1*, Thomas Berndl1, Kastriot Kastrati1, Sandra Raab1, Patricia Schweitzer1, Tim Stria1, Pavao Topic1 and Christian Wöber1
1Department of Neurology, Medical University of Vienna, Vienna, Austria
Objectives
About 2–3% of the general population and 11–70% of chronic headache patients suffer from medication overuse headache (MOH). Definitions according to the IHS, overused substances, as well as the management of MOH has changed over time and recently, inpatient detoxification is only recommended to patients with complicated MOH. To the best of our knowledge, no systematically collected data is available on how the above mentioned changes affected clinical characteristics of MOH patients, who are hospitalized for inpatient detoxification. The aim of our study was therefore to evaluate changes over time in clinical characteristics of these patients.
Methods
Percentages of hospital admissions within particular periods and overused medication. Abbr.: P1: 1984–1993, P2 1994–2003, P3 2004–2015. 1P-value: Chi-square test

Results
Within 32 years, a total of 807 patients accounted for 935 hospital admissions (78% women, 22%men, mean age 46.4 ± 12.2): 199 admissions in P1, 360 in P2 and 376 in P3. Underlying headache diagnoses were migraine, tension type headache, and other headaches in 50.6%, 44%, and 5.4%, respectively. Migraine was found in 42.7% and tension type headache in 50% of admissions in P1 and in 53.2% and 35.1% in P3, respectively (p = 0.017). Median time since first manifestation of the underlying headache disorder changed from 20 years in P1 to 16 years in P3 (p < 0.001). Median time since first manifestation of MOH changed from three years in P1 to two years in P3 (p < 0.001). In P1 the majority of admissions for inpatient detoxification was due to ergotamine-overuse, while in P3 it was due to overuse of simple-analgesics. Ergotamine overuse decreased and triptan overuse increased significantly during the study period (p < 0.001) (see table 1). The median cumulative number of single-dose administrations decreased from 120 per month in P1 to 90 in P3 (p = 0.001).
Conclusion
Clinical characteristics of MOH patients changed over 32 years. Nowadays, patients predominantly suffer from migraine, have a shorter history of migraine and MOH before start of inpatient detoxification, and the cumulative number of single-dose administrations is lower. As expected, the overuse of ergotamines decreased, whereas triptan overuse increased during the study period.
Disclosure of Interest
None Declared
Headache Epidemiology, Outcomes and Burden
PO-02-163
THE DIAGNOSTIC AND THERAPEUTIC JOURNEY OF PATIENTS PRIOR TO REVIEW IN HEADACHE CLINIC
Mahima Kapoor1, Anish Bahra1*
1Queen Square, WC1H 3BG, United Kingdom
Objectives
Headache is a common medical problem that causes great morbidity; worldwide, migraine on its own is the cause of 1.3% of all years of life lost to disability. Referrals for headaches account for up to one-third of new specialist neurology appointment in the United Kingdom even though GPs only refer 2–3% of patients consulting for headaches to neurologists. There are numerous, easily accessible guidelines aimed at all healthcare professionals who care for patients with headaches, however, it is known that a minority of migraine patients use specific anti-migraine drugs, and medication overuse is consistently underdiagnosed. There also continues to be a significant delay in diagnosis and access to treatment for patients with trigeminal autonomic cephalalgias. Given the issues outlined above, our objective was to review the past diagnoses, investigations and management of 526 patients referred to a tertiary headache clinic in London.
Methods
A retrospective audit was conducted of new headache referrals to one neurologist between June 2006 and June 2016. Data was collected from the electronic patient records system.
Results
526 patients were included in the audit, 69.5% were female. There were 845 diagnoses within the cohort; 224 of episodic migraine, 196 of chronic migraine, and 194 patients were identified as having medication overuse. 76 patients (14.4%) had a diagnosis of trigeminal autonomic cephalalgia, 39 of cluster headache, 12 of SUNCT/SUNA, 19 and 8 of paroxysmal hemicrania (PH) and heimcrania continua (HC), respectively. 49.8% of patients had 2 or more diagnoses. Regarding the patients with migraine, 123 of the patients with chronic migraine also had a diagnosis of medication overuse. 82% of migraine patients had tried a preventative agent, and 83% had seen at least one neurologist previously. Only 34.3% of referral letters mentioned discussion with patient about medication overuse. The most frequently used medication was amitriptyline in this cohort. 44% had tried propranolol before, at an average dose of 109 mg (standard deviation 76.4 mg), with only 6.6% still being on it at the time of review; 30.6% found it ineffective and 26.5% ceased it secondary to intolerability. 41% tried topiramate, at an average dose of 127.9 mg (standard deviation 95.7 mg). 59% of patients had a MRI prior to review and 73% of them were normal. Analgesia withdrawal was suggested to 55% of patients, and topiramate and propranolol were the most frequently prescribed medications at their first consultation. Of the 39 patients with cluster headaches, 70% had tried verapamil, at an average dose of 618 mg, and 5% had tried lithium. Acute treatment was prescribed to 75%. Of the 21 patients with HC or PH, only 8 had previously tried indomethacin. Of the 14 patients with SUNCT/SUNA, 6 tried each of pregabalin and lamotrigine, at an average dose of approximately 300 mg each.
Conclusion
Our audit shows that the prevalence of medication overuse, in a population that has seen both primary and secondary physicians is high, and first-line, evidence based treatments are most frequently trialled, but at sub-optimal doses and imaging remains a frequent investigation, that is usually normal.
Disclosure of Interest
None Declared
Headache Epidemiology, Outcomes and Burden
PO-02-164
An analysis of headache attack occurrence on days of the week and hours of the day using the MigrnX mobile system
George L. McLendon1, Dawn C. Buse2*, Jing Zhao1, Russ A. Bodner3, Alexander Dzeda4 and Richard B. Lipton5
1Carolinas Healthcare System, Charlotte
2Montefiore Medical Center, Bronx
3Carolinas Healthcare System, Concord
4SensorRX, Inc., Houston
5Albert Einstein College of Medicine, Bronx, United States
Objectives
To use novel data from the MigrnX mobile system to characterize the distribution of reported migraine attacks by day of the week and hour of the day.
Methods
An IRB approved study was conducted in a Carolinas Health System, Northeast Neurology practice using the MigrnX mobile (Android and iOS) tool (copyright SensorRx) to collect real time data from patients regarding migraine attacks. MigrnX records and shares actionable data for providers (e.g., migraine attack occurrence, pain intensity, associated symptoms, and medication usage) in a 5 touch format requiring less than 15 seconds of user time. MigrnX also uses embedded smart phone sensors to automatically record ancillary data associated with headache (e.g., date, time, weather, light, sound, etc.) which can be used to correlate and predict headache patterns via machine learning. Patients were diagnosed with migraine by a neurologist using ICHD-3beta criteria. We used descriptive statistics to characterize the patterns of migraine occurrence by day of the week and hour of the day and tested for deviation from the expected random distribution using a Chi-square test over a 90-day window.

Results
We report data from 111 patients meeting ICHD-3beta criteria for migraine (median age 42, age range 24–62). Most were Caucasian (80%) and female (76%). They entered 1,056 migraine attacks in a 90-day window. Over 90 days, the mean number of migraine attacks was 9.6, median 5, SD 11.8. The lowest frequency was 1 attack (N = 24, 21.6%) and the highest was 59 (N = 1, 0.9%). The modal number of migraine attacks per month was 1 (N = 31, 27.9%), ranging from 0 (N = 24, 21.6%) to 20 (N = 1, 0.9%).
Migraine occurrence by day differed from the predicted random occurrence (p < 0.001). Attacks were most common on Wednesdays (17.3%) and Tuesdays (16.8%) and least common on Saturdays (9.5%). Attacks were most frequently reported between noon to 10 pm. The most frequent time of day for migraine attacks was 4–6 pm (13.8%) followed by 8–10 pm (13.5%). Attacks were least frequently reported between 6–8 am (1.4%). (See Table).
Conclusion
This analysis of the MigrnX diary system reveals important information about the distribution of attacks in persons with migraine. We found that migraine attack occurence peaked midweek and later in the day with a low on Saturdays as well earlier in the day. The availability of large-scale, real-time patient reports as provided by MigrnX should find broad application in both esearch and patient care.
Disclosure of Interest
G. McLendon: None Declared, D. Buse Conflict with: Allergan, Avanir, Amgen, and Dr. Reddy’s Laboratories, Conflict with: Eli Lilly, Conflict with: Montefiore Medical Center, which in the past 12 months, has received research support funded by Allergan, Alder, Avanir, CoLucid, Dr. Reddy’s Laboratories, and Labrys via grants to the National Headache Foundation and/or Montefiore Medical Center, Conflict with: Editorial board of Current Pain and Headache Reports, the Journal of Headache and Pain, Pain Medicine News, and Pain Pathways magazine, J. Zhao: None Declared, R. Bodner Conflict with: Shareholder in Sensorrx, Conflict with: Sensorrx, Inc, A. Dzeda: None Declared, R. Lipton Conflict with: eNeura Therapeutics, Conflict with: NIH, Conflict with: Alder, Allergan, American Headache Society, Amgen, Autonomic Technologies, Avanir, Biohaven Inc, Boston Scientific, Colucid, Dr. Reddy’s, Electrocore, Eli Lilly, eNeura Therapeutics, Glaxo, Merck, GlaxoSmithKlein, Pfizer, Teva, Vedanta, Conflict with: Served on the editorial board of Neurology and as senior advisor to Headache. Received support from the Migraine Research Foundation and the National Headache Foundation. He has reviewed for the NIA and NINDS. Receives royalties from Wolff’s Headache, 8th Edition, Oxford Press University, 2009 and Informa
Headache Epidemiology, Outcomes and Burden
PO-02-165
Awarness of migraine in Neo-Latin countries: a study in 12 headache centers located over 7 countries
Michele Viana1*, Farihah Khaliq1, Grazia Sances1, María de Lourdes Figuerola2 3, Vittorio Di Piero4, Pierangelo Geppetti5, Rosario Iannacchero6, Ferdinando Maggioni7, Mauro Eduardo Jurno8, Ecaterina Chiriac9, Alejandro Marfil10, Filippo Brighina11, Nelson Barrientos Uribe12, Cristina Pérez Lago13, Carlos Bordini14, Franco Lucchese4, Valerio Maffey4, Giuseppe Nappi1, Giorgio Sandrini1 15, Cristina Tassorelli1 15
1Headache Science Center, C. Mondino National Neurological Institute, Pavia, Italy
2Hospital de Clínicas José San Martín
3Hospital Alemán, Buenos Aires, Argentina
4Sapienza University, Rome
5University of Florence, Florence
6A.O. “Pugliese – Ciaccio”, Catanzaro
7Padua University, Padua, Italy
8FAME/FUNJOB and FHEMIG, Barbacena, Brazil
9National Headache Center – Republic of Moldova, Chisinau city, Moldova, Republic of
10Hospital Universitario, Monterrey, Mexico
11Policlinico Universitario, Palermo, Italy
12Hospital DIPRECA, Santiago, Chile
13Hospital Maciel, Montevideo, Uruguay
14Clínica Neurológica Batatais, Batatais, Brazil
15University of Pavia, Pavia, Italy
Objectives
To assess the awareness of migraine (M) and previous diagnostic and therapeutic paths in naif migraineurs visited by a headache specialists in several neo-latin coutries.
Methods
This is a multicentre study was conducted in parallel in 12 headache centers located over 7 neo-latin speaking countries and coordinated by Mondino Institute, Pavia, Italy. Each center recruited up to 100 consecutive M patients (pts) aged 18 to 75 years who had been referred for a first visit. After receiving diagnosis of M, pts answered questions about 1) the type of headache they thought to suffer from; 2) their perceptions of the cause of M; 3) the previous diagnosis received by health professionals; and 4) previous visits/investigations/treatments for M.
Results
1161 pts were enrolled. Only 326 pts (28%) knew that they suffered from M, while 72% pts did not. 64% of pts simply called their M headache. Other common names were cervical pain (4%, mostly in Italy), tension-type headache (3%, mostly in Mexico, Chile and Uruguay), sinusitis (1%).
Factors associated with the awareness of M were: a high education level (p = <0.001), positive family history of M (p = 0.032), duration of the attack (p = 0.002), pain localised to the lateral head (p = 0.007), throbbing quality of pain (p = 0.007), presence of vomiting (p = 0.014) and presence of phonophobia (p = 0.011).
Mexico had the highest rate of M awareness (51%) followed by Chile (39%), Argentina (34%), Brazil (30%), Italy (25%), Moldova (17%) and Uruguay (12%).
5% of pts was aware that the cause of attacks was M predisposition, 50% of the patients attributed their headache to one of M triggers, while in Brazil and Argentina about 12% of pts causally related their M to anxiety, depression and other psychological problems.
All our pts had previously visited by a GP for M, but only 8% of them diagnosed it as M. The majority of pts (80%) has been visited by at least one specialist for their M, but only 35% of them formulated the correct diagnosis.
High rates of migraine diagnosis were observed in Moldova (53%), Argentina (68%) and Uruguay (52%), but a minority of pts in these countries was aware to suffer from M: 17%, 34% and 11% respectively.
50% of pts were prescribed a X-ray and/or CT and/or MRI of the cervical spine. 76% of pts underwent to imaging of brain and/or cervical spine that exposed them to radiation.
28% of patients had previously received a symptomatic migraine specific medication and 29% had received at least one migraine preventative medication.
Conclusion
Although M is the 3rd most common pathology worldwide and the 7th for disability, there is poor awareness of it among pts even after consultation with at least one physician. These findings speak in favor of the importance of educating doctors and patients in the field of M in order to reduce its burden worldwide.
This work was developed by the Italian Linguistic Group of IHS and supported by Mondino Institute (grant of the Italian Ministry of Health RC 2013–2015).
Disclosure of Interest
None Declared
Headache Pathophysiology – Basic Science
PO-02-167
VEGF-dependent signaling between dural endothelial cells and dural afferents: a potential neurovascular mechanism contributing to migraine headache.
Blaine Jacobs1*, Yesenia Morales1, Jasper Kuhn1, Theodore Price1 and Gregory Dussor1
1University of Texas at Dallas, Richardson, United States
Objectives
Historically, cranial vasodilation was considered the major contributing event in the pathophysiology of migraine. However, recent reports indicate little to no dilation of cranial blood vessels during spontaneous migraine. The reverse is also true; blood vessel dilation does not always produce migraine. A recent meta-analysis of 375,000 individuals identified 38 loci for migraine, the majority of which corresponded to genes associated with vascular disease and regulation of vascular tone. These opposing data highlight the unclear role of cranial blood vessels in migraine pathophysiology. One potential unifying hypothesis however is that the cells which comprise dural blood vessels (e.g. endothelial cells) contribute to migraine pathology independent of changes in vascular tone. Therefore, the purpose of this study was to determine the contribution of endothelial cell-specific signaling via Vascular Endothelial Growth Factor (VEGF) to dural afferent activation and headache.
Methods
Mouse dura mater was dissociated and dural endothelial cells were sorted using biotinylated PECAM-1 (CD-31) antibody and Dynabeads M-280 streptavidin-coated magnetic beads. Dural endothelial cells were subsequently cultured after bead-based purification. Once 80–90% confluent, cells were serum starved overnight, and then treated with Interleukin-6 (IL-6) for 24 h. The endothelial cells were washed and the conditioned media (CM) collected for 5 h at 37°C. Next, the dural endothelial cell CM was concentrated and probed for VEGF (1:200; sc-507) via western blot. Additionally, primary cultures of trigeminal ganglion (TG) were stimulated with recombinant human VEGF and changes in intracellular calcium levels assessed via Fura-2. Using a pre-clinical migraine model, recombinant human VEGF or endothelial cell CM was injected supradurally and the referred mechanical sensitivity of the periorbital region of the face assessed using withdrawal thresholds to von Frey filaments.
Results
There was a significant increase in VEGF release from primary cultures of dural endothelial cells stimulated with IL-6 ([80 ng/ml]) for 24 h compared to control. Correspondingly, 41% of TG neurons in culture respond to [5 nM] VEGF with an average percent increase in intracellular calcium (from baseline to peak response) of 45.9% ± 39 (average % increase ± SD). A subsequent KCl [50mM] exposure after VEGF increased intracellular calcium in these cells by 70.9% ± 56; N = 39 TG neurons. Using a preclinical migraine model we found that supradural injection of VEGF [50 pmols] significantly increased mechanical allodynia in the periorbital region of the face compared to heat inactivated VEGF (95°C for 5 min) also applied to the dura (N = 6, 2-way ANOVA, Bonferroni post-hoc, ****, p < 0.0001). Additionally, supradural injection of endothelial cell CM significantly increased mechanical allodynia in the periorbital region of the face compared to the vehicle (DMEM) (N = 4, 2-way ANOVA, Bonferroni post-hoc, **, p < 0.01).
Conclusion
These findings show that VEGF is released by dural endothelial cells, it activates trigeminal ganglion neurons, and it causes headache behaviors when applied to the dura mater. Since dural endothelial cells directly contact the circulating blood in the lumen, they may release VEGF in response to various immunological stimuli present in the blood including IL-6, a cytokine previously shown to be elevated in jugular blood of migraine patients during attacks. Thus, the pain of migraine may occur due to signaling events between vascular endothelial cells and dural afferent neurons, without a requirement for dilation of cranial vessels.
Disclosure of Interest
None Declared
Headache Pathophysiology – Basic Science
PO-02-168
Abnormal response of the systemic circulation to nitroglycerin in migraine
Willebrordus P. Van Oosterhout1*, Guus G. Schoonman2 3, Dirk P. Saal4, Michel D. Ferrari1 and Gert J. Van Dijk1
1Neurology, Leiden University Medical Center, Leiden
2Neurology, Elizabeth TweeSteden Hospital, Tilburg/Waalwijk
3Neurology, LUMC, Leiden
4Neurology, St. Franciscus Gasthuis, Rotterdam, Netherlands
Objectives
Migraine and vasovagal syncope are associated epidemiologically and may share part of their pathophysiology too. Vasovagal syncope can be provoked through systemic vasodilatation using nitroglycerin, which can also be used to provoke a migraine attack, through as yet impartially known mechanisms. Here, we report on the effects and responses of the systemic cardiovascular system on a vasodilatory influence in migraine and matched controls.
Methods
Sixteen female migraine without aura patients and ten age- and gender matched controls were included. Nitroglycerin (0.5 µg kg−1 min−1) was administered intravenously to provoke a migraine attack. Subjects lay in the supine position, and finger photoplethysmography was used to measure mean arterial pressure (MAP), heart rate (HR), cardiac output (CO), stroke volume (SV) and total peripheral resistance (TPR) continuously in periods before infusion (for 10 min), during it (for 20 min) and directly afterwards (for 10 min). Per block and 1-minute averages were used in generalized estimating equations models.

Results
The per block analysis comparing averages during nitroglycerin infusion with baseline showed increases in HR (p < 0.001; both groups), and decreases in CO (p < 0.001; both groups), MAP (p = 0.002; migraine) and SV (p < 0.001; migraine, p = 0.03; controls), which were confirmed by the time-series analysis using 1-minute averages (all p < 0.001). The per block average TPR during infusion was higher than at baseline (p = 0.006; migraine), with the 1-minute showing a decrease after an initial migraine specific increase. There were also differences in the other parameters between the groups (1-minute average analysis; p < 0.001 for group*time interaction): CO and SV decreased faster and more prolonged in the migraine group. MAP showed an initial migraine-specific increase, but then a decrease over time. HR increased more in the migraine group (Figure 1).
Conclusion
Nitroglycerin induced overall decreases in SV, CO and MAP, suggesting increased venous pooling, and the increases in HR and TPR represent compensation attempts. The larger decreases of SV and CO in migraine suggest that nitroglycerin induced more venous pooling in the migraine group. MAP was similar between groups at the start, increased initially in the migraine group at nitroglycerin infusion and then decreased. This suggests an initial ample compensatory increase in MAP in the migraine group, that ultimately was no longer sufficient. Overall, this points to an abnormal susceptibility towards vasodilation of the systemic circulation in migraine.
Disclosure of Interest
None Declared
Headache Pathophysiology – Basic Science
PO-02-169
Transcriptomic Profiling of Trigeminal Nucleus Caudalis and Spinal Cord Dorsal Horn
Rikke Elgaard Christensen1*, Lisette J. A. Kogelmann1, Thomas F. Hansen1, Inger Jansen-Olesen1 and Jes Olesen1
1Danish Headache Center, Glostrup, Denmark
Objectives
The somatosensory system can be divided into the trigeminal pathway and the spinothalamic pathway. Even though the two systems are homologous in terms of function, differences in nociceptive signalling and gene expression must exist, as several signalling substances cause headache but not peripheral pain. Furthermore, migraine can be treated with highly specific drugs that do not have an effect on other types of pain. Recently, RNA-Sequencing has been used to characterise transcriptomes from trigeminal and dorsal root ganglia. However, the tissues where the signal is relayed to secondary afferents are largely unstudied. Thus, we aimed at investigating the transcriptomes from laminae I-V of the trigeminal nucleus caudalis (TNC) and laminae I-V from the dorsal horn of the thoracic part of the spinal cord (SDH).
Methods
Significantly DE migraine-relevant genes. Asterisk denotes the value and tissue with highest expression. TNC: Trigeminal nucleus caudalis, SDH: spinal cord dorsal horn

Results
We found 3,591 genes to be DE; 1,696 were higher expressed in TNC and 1,895 were lower expressed in TNC compared to SDH. There was no difference between ratios of cell-specific markers between the two tissues, thus difference in cell type distribution is not causing differential expression. We describe the differential gene expression of relevant ion channels and G-protein coupled receptors, such as Mas-related G protein-coupled receptors, serotonin receptors, pituitary adenylate cyclase activating polypeptide-38 and vasoactive intestinal polypeptide, calcitonin gene-related peptide and histamine, and their receptors.
Pathway analysis showed 13 overrepresented pathways among the genes higher expressed in TNC and 11 overrepresented pathways among the genes lower expressed in TNC compared to SDH. Two of the most interesting findings were the differences in gene expression in the GABAergic pathway (KEGG pathway 04727) and the cGMP signalling pathway (KEGG pathway 04022). Furthermore, we characterised the expression of 36 of the 41 migraine-associated loci found by GWAS. Below a table of some of the significantly DE migraine-relevant genes is included.
Conclusion
We describe differential expression of several genes believed to be involved in pain signalling. Also, the GABAergic and cGMP pathways showed different signalling between tissues. Thus, many genes are expressed differently in TNC and SDH in naïve rats. Further analysis of these findings may lead to increased understanding of migraine mechanisms and to novel drug targets.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-02-170
Double blind trial of sumatriptan for cilostazol induced headache in migraine without aura patients. Intracellular VS extracellular mechanisms
Katrine Falkenberg1*, Jes Olesen1, Messoud Ashina1, Song Guo1 and Bara A Dunga1
1Danish Headache Center, Glostrup, Denmark
Objectives
There remains a great need for more effective anti-migraine drugs with fewer side-effects. A human model to test new drugs is needed, but still not developed. This is the third attempt in a series, aiming to develop such a model. To validate whether cilostazol could be used as a model in migraine patients, we tested the effect of sumatriptan on the induced headache and hypothesized that sumatriptan would reduce the headache score.
Methods
200 mg of cilostazol was given on two separate days to 30 patients with migraine without aura. The patients treated the induced headache in a double-blind cross-over design with 50 mg of sumatriptan and placebo. Headache intensity and accompanying symptoms were registered in a questionnaire until 12 hours after intake. To verify the sensitivity of the patient material, as many as possible (15) participants also treated their spontaneous attacks in a double-blind cross-over design with sumatriptan and placebo and filled out the same questionnaire.
Results
Cilostazol induced headache with some migraine characteristics in all participants on both study days and 77% fulfilled criteria for a migraine-like attack on one or both provocation days. There was no reduction in headache score 2 h after any of the two treatments (P = 0.15 for sumatriptan), but a significant increase after placebo (P = 0.0002) indicating some effect of sumatriptan. At 4 h after treatment, the difference in median headache score was significant (P = 0.017). The participants subsequently treated spontaneous migraine attacks with sumatriptan double blindly. The difference between placebo and sumatriptan was not significant at 2 h (P = 0.26), but was highly significant 4 h after intake (P = 0.006) due to a significant decrease in headache score after sumatriptan (P = 0.0003).
Conclusion
Cilostazol induced a headache indistinguishable from spontaneous migraine attacks but spontaneous attacks responded better than cilostazol induced attacks to sumatriptan. The low efficacy on cilostazol induced migraine has bearings upon the mechanisms of migraine and the mechanisms of action of sumatriptan. Sumatriptan acts via 5-HT1B/D/F receptors in the cell membrane which are coupled to G-proteins that inhibit adenylate cyclase and thereby decrease intracellular cyclic adenosine monophosphate (cAMP) concentration. Cilostazol works directly intracellularly by inhibiting Phosphodiesterase 3 (PDE3) which breaks down cAMP and hence causes intracellular cAMP accumulation. Sumatriptan and cilostazol thus have opposing effects on cAMP-level. We also know from previous studies of NO donors that work directly intracellularly that they don’t respond to sumatriptan. On the basis of these studies we propose that cilostazol- and perhaps NO based models will respond to new drugs that act intracellularly or directly on ion channels responsible for intracellular signaling. But these models will not respond to drugs acting extracellularly e.g. CGRP receptor antagonists. The attacks induced by cilostazol are identical to spontaneous attacks and will therefore be highly valuable in the investigation of the pathophysiological mechanisms behind migraine, e.g. via imaging.
Disclosure of Interest
None Declared
Migraine Acute Therapy
PO-02-171
Use of Most Bothersome Symptom as a Co-Primary Endpoint in an Acute Treatment of Migraine Trial
David W. Dodick1*, Stewart J. Tepper2, Deborah Friedaman3, Amy Gelfand4, Robert P. Cowan5, Pete Schmidt5, Jean Engels6, Alan Rapoport7 and Donald J. Kellerman8
1Mayo Clinic, Scottsdale
2Dartmouth-Hitchcock, Hanover
3UT Southwestern, Dallas
4University of California, San Francisco, San Francisco
5Stanford University, Palo Alto
6Engels Consulting, Minneapolis
7David Geffen Medical School, Los Angeles
8Zosano Pharma, Fremont, United States
Objectives
In October 2014, the FDA issued a Guidance Document for Acute Migraine Treatment. In the FDA document, the use of subject-identified migraine-associated most bothersome symptom (MBS) in addition to pain is recommended as a co-primary efficacy endpoint. Recently, this approach was utilized in a multi-center, dose-ranging efficacy and safety trial of a novel intracutaneous formulation of zolmitriptan (M207), and herein we report the results with this novel endpoint.
Methods
Number (%) of Subjects Pain Free and MBS Free at 2 Hours

Results
365 subjects were randomized; 321 treated with study drug (n = 244 for M207 and 77 for placebo) and had at least one post-treatment symptom assessment and comprised the modified intent to treat population. The most commonly reported MBS was PT (50.5%), followed by PN (26.8%), and N (22.7%). The 2-hour pain free rate was higher in the M207 3.8 mg group compared to the placebo group, 41.5% vs 14.3%, as was the 2-hour MBS freedom rate, 68.3% vs 42.9% (p < 0.001 for both, CMH test). Co-primary efficacy results as a function of their selected MBS are shown above.
In an additional post-hoc analysis, the percentage of subjects who were both pain free and MBS free at 2 hours following M207 3.8 mg was 40.2%, and somewhat similar percentages were seen when categorized by MBS (PT 33.3%, PN 40.9% and N 55.6%).
Conclusion
Approximately 50% of subjects selected photophobia as their MBS. Those who selected nausea showed the largest treatment effect. Subjects who selected phonophobia as their MBS had the smallest therapeutic gain for MBS freedom. MBS as a co-primary endpoint is a viable and patient-centered alternative to utilizing four co-primary endpoints in acute treatment of migraine trials and is worthy of discussion in future IHS clinical trial guidelines.
Disclosure of Interest
D. Dodick Conflict with: Zosano Pharma Advisor, S. Tepper Conflict with: Zosano Pharma Advisor, D. Friedaman Conflict with: Zosano Pharma Advisor, A. Gelfand Conflict with: Zosano Pharma Advisor, R. Cowan Conflict with: Zosano Pharma Advisor, P. Schmidt Conflict with: Zosano Pharma, Conflict with: Zosano Pharma, J. Engels Conflict with: Zosano Pharma, A. Rapoport Conflict with: Zosano Pharma Advisor, D. Kellerman Conflict with: Zosano Pharma, Conflict with: Zosano Pharma
Migraine Acute Therapy
PO-02-172
Lasmiditan inhibits CGRP release in the mouse trigeminovascular system.
Alejandro Labastida-Ramírez1*, Eloísa Rubio-Beltrán1, Ingrid M. Garrelds1, Kristian A. Haanes1, Kayi Y. Chan1, Joe Kovalchin2, Kirk W. Johnson2, Alexander H. Danser1, Carlos M. Villalón3 and Antoinette MaassenVanDenBrink1
1Department of Internal Medicine, Division of Vascular Medicine and Pharmacology, Erasmus University Medical Center, Rotterdam, Netherlands
2Eli Lilly and Company, Lilly Corporate Center, Indianapolis, United States
3Pharmacobiology, Cinvestav-IPN, Unidad Sur, Mexico City, Mexico
Objectives
Migraine pathophysiology is associated with activation of the trigeminovascular system, CGRP release and cranial vasodilatation. Triptans are 5-HT1B/1D/(1F) receptor agonists with vasoconstrictive effects that inhibit trigeminal CGRP release prejunctionally, but they are contraindicated in patients with cardiovascular disease. In contrast, lasmiditan is a selective 5-HT1F receptor agonist devoid of vasoconstrictor properties. The present study investigated the modulation of trigeminal CGRP release by lasmiditan and sumatriptan.
Methods
The effects of sumatriptan and lasmiditan (both 30 µM) were investigated on KCl-induced CGRP release from isolated preparations of dura mater, trigeminal ganglion (TG) and trigeminal nucleus caudalis (TNC) from mice. The release of CGRP was measured by enzyme-linked immunoassay. Experiments were approved by the Erasmus University Medical Center’s institutional ethics committee, in accordance with National Institute of Health guidelines.
Results
In contrast to vehicle, sumatriptan significantly inhibited (p < 0.05) CGRP release by 49% in the dura mater (n = 8), 48% in the TG (n = 9), and 75% in the TNC (n = 7). Interestingly, lasmiditan also inhibited (p < 0.05) CGRP release by 47% in the dura mater (n = 8), 59% in the TG (n = 9), and 70% in the TNC (n = 5).
Conclusion
Based on our results, the clinical efficacy observed with lasmiditan and sumatriptan may be due to inhibition of CGRP release from peripheral and central trigeminal nerve terminals. In mice, the 5-HT receptor subtypes activated by lasmiditan at the concentration evaluated could be 5-HT1F or 5-HT1A. However, prior publications would support that the release of CGRP is most likely mediated by the 5-HT1F receptor, not 5-HT1A. Since activation of 5-HT1F receptors is not associated with vasoconstriction, this may represent a therapeutic advantage over the vasoactive triptans.
Disclosure of Interest
A. Labastida-Ramírez: None Declared, E. Rubio-Beltrán: None Declared, I. Garrelds: None Declared, K. Haanes: None Declared, K. Chan: None Declared, J. Kovalchin Conflict with: Employee Eli Lilly, K. Johnson Conflict with: Employee Eli Lilly, A. Danser: None Declared, C. Villalón: None Declared, A. MaassenVanDenBrink Conflict with: Research support from Eli Lilly
Migraine Acute Therapy
PO-02-173
In vitro characterization of agonist binding and functional activity at a panel of serotonin receptor subtypes for lasmiditan, triptans and other 5-HT receptor ligands and activity relationships for contraction of human isolated coronary artery
Eloísa Rubio-Beltrán1*, Alejandro Labastida-Ramírez1, Antoon Van den Bogaerdt2, Ad J. Bogers3, Eric Zanelli4, Laurent Meeus5, Alexander J. Danser1, Kirk W. Johnson6, Joseph Kovalchin6, Carlos M. Villalón7 and Antoinette MaassenVanDenBrink1
1Div. of Pharmacology, Dept. of Internal Medicine, Erasmus University Medical Center
2Heart Valve Bank
3Department of Cardiothoracic Surgery, Erasmus University Medical Center, Rotterdam, Netherlands
4Déclion Pharmaceuticals, Inc., Boxford, MA, United States
5Ogeda S.A., Gosselies, Belgium
6Eli Lilly and Company, Lilly Corporate Center, Indianapolis, IN, United States
7Pharmacobiology, Cinvestav-IPN, Unidad Sur, Mexico City, Mexico
Objectives
Ergot alkaloids and triptans (5-HT1B/1D receptor agonists) are well-established antimigraine drugs, but their use is contraindicated in patients with coronary artery disease. In contrast, lasmiditan is a selective 5-HT1F receptor agonist devoid of coronary vasoconstrictive properties. We investigated the binding and functional agonist pharmacological properties of individual anti-migraine drugs (ergotamine, sumatriptan, zolmitriptan, naratriptan, rizatriptan, almotriptan, eletriptan, frovatriptan, donitriptan, avitriptan, alniditan, lasmiditan, LY334370, LY344864, 5-HT and 5-carboxamidotryptamine on a panel of human 5-HT receptors.
Methods
In vitro radiolabelled competition and second messenger activity assays were performed using membrane preparations from CHO cells transfected with gene constructs for human orthologs of 5-HT1A, 5-HT1B, 5-HT1D, 5-ht1E, 5-HT1F, 5-HT2A, 5-HT2B and 5-HT7 receptors. We related radioligand binding affinity and second messenger activation to the contractile potency of these compounds in human isolated coronary arteries as determined earlier by our group or from other publications (for almotriptan and frovatriptan).
Results
The potency of these compounds to inhibit forskolin-induced cAMP increase was positively correlated to their potency to contract the human isolated coronary artery in case of the 5-HT1B receptor, and was negatively correlated for the 5-HT1F receptor.
Conclusion
Our results indicate that, as expected, 5-HT1B receptor-induced inhibition of cAMP responses, directly correlates to human coronary artery contraction. Furthermore, the negative correlation between the human coronary artery contraction and activation of 5-HT1F receptors seems a cardiovascular safety advantage over 5-HT1B receptor agonists; future studies should elucidate the underlying mechanism. Finally, our results confirm that lasmiditan is a selective 5-HT1F receptor agonist devoid of vasoconstrictive properties.
Disclosure of Interest
E. Rubio-Beltrán: None Declared, A. Labastida-Ramírez: None Declared, A. van den Bogaerdt: None Declared, A. Bogers: None Declared, E. Zanelli Conflict with: Eli Lilly and Company, L. Meeus Conflict with: Eli Lilly and Company, A. Danser: None Declared, K. Johnson Conflict with: Eli Lilly and Company, J. Kovalchin Conflict with: Eli Lilly and Company, C. Villalón Conflict with: Eli Lilly and Company, A. MaassenVanDenBrink Conflict with: Eli Lilly and Company
Migraine Acute Therapy
PO-02-174
A Double-Blind, Placebo-Controlled, Study Evaluating the Efficacy of DFN-02 (Nasal Spray of Sumatriptan 10 mg + Permeation Enhancer) in Migraine With or Without Aura
Sagar Munjal1* and Elimor Brand-Schieber2
1Clinical Development and Medical Affairs
2Clinical Development, Promius Pharma, a subsidiary of Dr. Reddy's Laboratories, Princeton, United States
Objectives
DFN-02 is a sumatriptan 10 mg intranasal spray containing 1-O-n-dodecyl-β-D-maltopyranoside 0.2% (DDM), a permeation enhancer. DFN-02 is being developed for the treatment of acute migraine with or without aura. The safety and efficacy of sumatriptan are well established. Following DFN-02 intranasal administration, sumatriptan plasma concentration peaked 5 minutes faster than subcutaneously injected 4 mg and 6 mg Imitrex®. This pharmacokinetic profile of DFN-02 may provide improved therapeutic effect via the nasal route. This study was conducted to primarily compare headache pain freedom response between DFN-02 and placebo at 2 hours postdose in acute migraine with moderate to severe predose pain.
Methods
Subjects were randomized in a double-blinded fashion to treat one migraine attack (DB1) with DFN-02 or placebo within one hour of experiencing moderate (Grade 2) or severe (Grade 3) headache pain; the primary endpoint was the proportion of subjects with pain freedom (Grade 0) at 2 hours postdose compared between DFN-02 and placebo. Subjects were then re-randomized to receive DFN-02 or placebo to treat a migraine attack at any headache pain level. Subjects reported data in real-time eDiary. Safety was evaluated throughout the study.
Results
There were 107 subjects randomized, 93 had data in DB1, 86 continued, and 75 completed DB2. The study met its primary endpoint: in DB1, 43.8% of patients (n = 21/48) taking DFN-02 were pain-free at 2 hours compared with 22.5% taking placebo (n = 9/40; p = .044). DFN-02 was also superior to placebo in alleviating the most bothersome symptom (MBS) (70.7% versus 39.5% MBS free; p = .007). After taking DFN-02, 38.9% of subjects (n = 14/36) were pain-free from 2–24 hours versus 13.8% (n = 4/29) on placebo (p = .029). DFN-02 reduced migraine-associated symptoms (i.e. nausea/photophobia/phonophobia; p = .026/.005/.004) and disability at 2 hours (p < .001). For DB2 trends were similar, however, fewer endpoints reached statistical significance, possibly due to a high placebo response. There were no discontinuations due to adverse events (AEs) and no reported serious AEs during the study. Overall DFN-02 was well tolerated.
Conclusion
The DFN-02 (sumatriptan 10 mg + DDM) treatment group had statistically significant higher proportion of subjects who had their moderate to severe migraine pain reduced to none (pain freedom) and symptom relief (including their most bothersome) at 2 hours postdose, compared with placebo. This novel product may provide an effective noninvasive option for the acute treatment of migraine.
Disclosure of Interest
S. Munjal Conflict with: Dr. Reddy's Laboratories, Conflict with: Owns stock in Dr. Reddy's Laboratories, E. Brand-Schieber Conflict with: Dr. Reddy's Laboratories, Conflict with: Owns stock in Dr. Reddy's Laboratories
Migraine Acute Therapy
PO-02-175
Experience with Delayed Treatment of Migraine and Morning Migraine Treatment Using Intracutaneous Zolmitriptan (M207)
Pete Schmidt1*, Whitney Halladay1, Jean Engels1 and Alan Rapoport2
1Zosano Pharma, Fremont
2Ronald Reagan UCLA Medical Center, Los Angeles, United States
Objectives
Migraineurs are typically instructed to treat migraine attacks with triptans early or when pain is still mild, as current data suggest that triptans are less effective when used late in a migraine attack. In practice, this becomes challenging, as patients often treat late for many reasons, including certainty that they are having a migraine attack and not a tension-type headache.
A new adhesive dermally-applied microarray (ADAM) system of zolmitriptan delivery (M207) recently demonstrated efficacy in a phase 2 b/3 trial in episodic migraine. Subjects in this trial were instructed not to treat until their headache pain was moderate or severe and thus treatment was often delayed in relation to the onset of the headache. We sought to analyze the effects of delayed time-to-treatment on the efficacy of ADAM zolmitriptan.
Methods
A Cochran-Mantel-Haenszel test controlling for baseline randomization stratification by most bothersome symptom other than pain [MBS] was performed to compare M207 3.8 mg to placebo for each of the co-primary endpoints (pain freedom and freedom from MBS, both at 2 hours). A subject’s MBS was defined as the symptom other than pain that is present during the majority of migraine attacks and was most bothersome to the subject. This could be either photophobia, phonophobia or nausea. We performed post-hoc analyses for the subgroup of subjects who awoke with their migraine versus those who did not, and also for those who treated more than 2 hours after headache onset versus those who treated in under 2 hours.
Results
Approximately 51% of patients reported waking up with headache pain already present at moderate to severe intensity. The mean time to migraine treatment after subject-estimated headache onset in all groups was 4.96 hours and the median was 1.79 hours. 33.3% and 69.4% of the M207 subjects treating ≥2 hours achieved the co-primary endpoints (pain freedom and freedom from MBS), respectively, compared with 10.3% and 41.0% receiving placebo. In those treating <2 hours, 46.5% and 65.1% receiving active treatment achieved the co-primary endpoints, compared with 19.4% and 47.2% receiving placebo.
In subjects who awoke with moderate to severe headache pain, 44.4% and 72.2% of subjects receiving active treatment achieved the co-primary endpoints, versus 15.9% and 38.6% of subjects receiving placebo.
All comparisons achieved statistical significance (nominal p-values less than 0.05), with the exception of MBS freedom in those treating in <2 hours (p = 0.0899).
Conclusion
Therapeutic gain with M207 for the co-primary endpoints was nearly the same for subjects who treated in <2 hours, as compared to those who treated ≥2 hours after migraine onset. Consistent with these findings, M207 also provided a significant therapeutic gain i(28.5%) n those who woke up with migraine (i.e. morning migraine).
Disclosure of Interest
P. Schmidt Conflict with: Zosano Pharma, W. Halladay Conflict with: Zosano Pharma, J. Engels Conflict with: Zosano Pharma, A. Rapoport Conflict with: Zosano Pharma
Migraine Acute Therapy
PO-02-176
Migraine Treatment Patterns and Opioid Use Among Chronic and Episodic Migraine Patients Identified by a Clinician-Administered Semi-Structured Diagnostic Interview
Justin S. Yu1*, Jelena M. Pavlovic2, Stephen D. Silberstein3, Michael L. Reed4, Steve H. Kawahara5, Robert P. Cowan6, Firas Dabbous7, Karen L. Campbell1, Riya Pulicharam5, Hema N. Viswanathan1 and Richard B. Lipton8
1Allergan plc, Irvine
2Montefiore Medical Center;The Saul R. Korey Department of Neurology, Albert Einstein College of Medicine, Bronx
3Jefferson Headache Center, Philadelphia
4Vedanta Research, Chapel Hill
5DaVita Medical Group, El Segundo
6Stanford University School of Medicine, Stanford
7Independent consultant, La Jolla
8Headache Center; Department of Neurology, Albert Einstein College of Medicine; Department of Epidemiology and Population Health, Albert Einstein College of Medicine, Bronx, United States
Objectives
Chronic migraine (CM) remains suboptimally treated. Opioids have been used for acute treatment of migraine, but are not recommended for regular use due to the risks of medication overuse, tolerance, dependence, and opioid hyperalgesia. The objectives of this study were to describe migraine treatment patterns and opioid use in CM and episodic migraine (EM) patients.
Methods
An observational study using retrospective claims data and survey data was conducted in a large medical group. Eligible patients were ≥18 years old, had ≥12 months of continuous medical and pharmacy enrollment prior to the screening date, and had ≥1 medical claim with a migraine diagnosis (ICD-9/10 code of 346.xx/G43.xxx) in the 12 months prior to the screening date. A Semi-Structured Diagnostic Interview (SSDI) administered by a trained clinician was used to determine if a patient had CM (≥15 headache days/month) or EM (<15 headache days/month). The SSDI included 31 questions related to headache symptoms, frequency, disability, medication use, and diagnosis. Acute treatment of migraine, preventive treatment of migraine, opioid use, and baseline characteristics were assessed for CM and EM patients based on claims data collected in the 12 months prior to the screening date. Results were summarized using descriptive analyses.
Results
Of the 192 patients included, 129 had CM and 63 had EM. The CM cohort had a mean age of 49.4 years (SD = 12.6) and was 93.8% female. The EM cohort had a mean age of 48.9 years (SD = 15.4), and was 82.5% female. In relation to migraine treatment patterns, 67.4% of CM patients and 55.6% of EM patients had ≥1 claim for both acute and preventive medications. 53.5% of CM patients and 36.5% of EM patients also had ≥1 opioid claim (p < 0.05); the mean number of opioid claims was 4.0 (SD = 7.1) among all CM patients and 2.8 (SD = 8.2) among all EM patients. Additionally, 33.3% of CM patients and 15.9% of EM patients had ≥3 opioid claims. The mean Deyo-Charlson Comorbidity Index scores were 0.3 (SD = 0.7) for the CM cohort and 0.2 (SD = 0.5) for the EM cohort. Furthermore, 13.2% of CM patients and 7.9% of EM patients had a diagnosis for a pain disorder other than migraine (e.g. psychogenic pain, central pain syndrome, chronic pain syndrome).
Conclusion
Approximately two-thirds of patients with CM filled prescriptions for both acute and preventive medications in the past year. The majority of patients with CM and about a third of patients with EM also received an opioid prescription in the same time period. Treatment patterns, including opioid use, in CM patients indicate opportunities for better management through improved care.
Disclosure of Interest
J. Yu Conflict with: Allergan plc, Conflict with: Allergan plc, J. Pavlovic Conflict with: Allergan plc, the American Headache Society, S. Silberstein Conflict with: Allergan, Inc.; Amgen; Cumberland Pharmaceuticals, Inc.; ElectroCore Medical, Inc.; Labrys Biologics; Eli Lilly and Company; Merz Pharmaceuticals; and Troy Healthcare, Conflict with: Alder Biopharmaceuticals; Allergan, Inc.; Amgen; Avanir Pharmaceuticals, Inc.; eNeura; ElectroCore Medical, LLC; Labrys Biologics; Medscape, LLC; Medtronic, Inc.; Neuralieve; NINDS; Pfizer, Inc.; and Teva Pharmaceuticals., M. Reed Conflict with: Vedanta Research has received funding from Allergan, Amgen, CoLucid, Dr. Reddy’s Laboratories, Endo Pharmaceuticals, GlaxoSmithKline, Merck & Co., Inc., NuPathe, Novartis, and Ortho-McNeil, via grants to the National Headache Foundation., Conflict with: Vedanta Research, S. Kawahara Conflict with: DaVita Medical Group, R. Cowan: None Declared, F. Dabbous: None Declared, K. Campbell Conflict with: Allergan plc, Conflict with: Allergan plc, R. Pulicharam Conflict with: DaVita Medical Group, H. Viswanathan Conflict with: Allergan plc, Conflict with: Allergan plc, Conflict with: Patents or other intellectual property in Allergan plc, R. Lipton Conflict with: eNeura Therapeutics and Biohaven, Conflict with: NIH, Migraine Research Foundation, the National Headache Foundation, Conflict with: Alder, Allergan, Amgen, Autonomic Technologies, Avanir, Boston Scientific, Colucid, Dr. Reddy’s, Electrocore, Eli Lilly, eNeura Therapeutics, GlaxoSmithKlein, Merck, Pfizer, Teva, Vedanta., Conflict with: Royalties from Wolff’s Headache, 8th Edition, Oxford Press University, 2009 and Informa. Editorial board of Neurology. Senior advisor to Headache. Reviewered for the NIA and NINDS
Migraine Acute Therapy
PO-02-177
Higher Treatment Satisfaction and Reduced Functional Disability in Subjects with Acute Migraine Treated with DFN-02 (Sumatriptan 10 mg+ 0.2 % DDM) Compared with Placebo
Elimor Brand-Schieber1* and Sagar Munjal2
1Clinical Development
2Clinical Development and Medical Affairs, Promius Pharma, a subsidiary of Dr. Reddy's Laboratories, Princeton, United States
Objectives
The majority of migraine sufferers report dissatisfaction with their migraine medication. This study evaluated treatment satisfaction and functional disability in acute migraine patients who use DFN-02 10 mg (sumatriptan 10 mg +0.2% DDM, a permeation enhancer).
Methods
Subjects were randomized in a double-blinded fashion to treat one migraine attack (DB1) with DFN-02 or placebo within one hour of experiencing moderate or severe headache pain; the primary endpoint was the proportion of subjects with pain freedom at 2 h postdose. Subjects were then re-randomized to receive DFN-02 or placebo to treat a migraine attack at any level of headache pain (DB2). Subjects reported data in real-time in an eDiary. Safety was evaluated throughout the study. Among secondary endpoints, treatment satisfaction was assessed using a validated Patient Perception of Migraine Questionnaire-Revised (PPMQ-R). At baseline, subjects evaluated their usual migraine medication and at 24 h postdose, they evaluated the study medication. The PPMQ-R Global Satisfaction item alone was used at 2 h postdose. Functional disability was evaluated using a 4-point scale (0 = no disability, 1 = mild, 2 = moderate, 3 = severe) at predose and 2 h and 24 h postdose.
Results
In subjects acutely treating a migraine with moderate to severe predose headache pain in DB1, mean scores for functional disability significantly improved (p < .001) for DFN-02 at 2 h postdose (−1.2) (n = 48) compared with placebo (−0.6) (n = 39). No differences in disability were observed between treatments at 24 h postdose. For the PPMQ-R subscales, comparing DFN-02 treatment (n = 36) to the subjects’ usual migraine treatment (n = 48), the Total PPMQ-R score at 24 h postdose was significantly higher for DFN-02 (62.16 for usual migraine treatment versus 74.56 for DFN-02; p = .012). Similarly, the Overall Satisfaction item was significantly better (p = .013) for DFN-02 at 2 h postdose (n = 48) compared with usual migraine medication assessed at baseline (n = 48).
Subjects treated with DFN-02 (n = 37) had significantly higher satisfaction compared with placebo (n = 30) for the Efficacy subscale (mean score 65.23 versus 42.53; p = .016) and the Function subscale (mean score 68.92 versus 42.08; p = .001), but no significant difference was observed for Ease-of-use subscale (mean score 78.83 versus 85.28; p = .520) at 24 h postdose. The Total Score (Efficacy + Function + Ease of use) was significantly better for DFN-02 compared with placebo (mean score 70.99 versus 56.63; p = .016). The Global items: Medication Effectiveness and Overall Satisfaction were significantly better for DFN-02 at 24 h (p = .027 and p = .019, respectively). Moreover, the Overall Satisfaction item was significantly better for DFN-02 than placebo at 2 h postdose (p = .003). The placebo treatment had a significantly better Tolerability subscale (94.83) than DFN-02 (88.51) at 24 h postdose (p = 0.026), however, the Global Side Effects item, was not significantly different between the treatment groups (p = .383). Results from DB2 show similar trends overall but few comparisons reached statistical significance, possibly due to a high placebo effect.
Conclusion
Subjects using DFN-02, an intranasal spray of sumatriptan 10 mg +DDM, to acutely treat a migraine attack at moderate to severe headache pain levels reported clinically and statistically significant greater satisfaction with medication effectiveness and had lower disability compared with placebo and greater satisfaction compared with their usual migraine medication. These data demonstrate that DFN-02 has the potential to reduce disability and to improve migraine treatment experience compared with usual migraine medication.
Disclosure of Interest
E. Brand-Schieber Conflict with: Dr. Reddy's Laboratories, Conflict with: Owns stock in Dr. Reddy's Laboratories, S. Munjal Conflict with: Dr. Reddy's Laboratories, Conflict with: Owns stock in Dr. Reddy's Laboratories
Migraine Acute Therapy
PO-02-178
A review of pharmacokinetic variability of single doses of oral triptans with some possible clinical implications
Peer Tfelt-Hansen1*
1Danish Headache Center, Glostrup Sygehus, Copenhagen, Denmark
Objectives
Wide interindividual variability in plasma concentrations of sumatriptan after oral administration was observed in the first pharmacokinetic studies of the drug. Later, 2 pharmacokinetic studies in migraine patients indicated that both the speed of absorption and the levels of plasma concentrations of an oral triptan could be important for the clinical response to these drugs.
In clinical practice, when treating migraine patients with oral triptans, it would often be useful to know the extent of oral variability potential of these drugs when trying to tailor a triptan to a patient.
The aim of this review is therefore to provide treating physician with this information based on published pharmacokinetic studies on the oral triptans.
Methods
PubMed and Web of Science concentration were searched with the terms “name of a triptan” and “oral pharmacokinetics”. I included in the review pharmacokinetic studies presenting the following quantitative parameters for variability of Cmax (maximum plasma concentration) and Tmax (time to maximum concentration): mean, SD (standard deviation) or CV (coefficient of variation). If not presented in the paper the CV was calculated as SD/mean.
The distribution of the CVs for Cmax for each drug is presented as either lower or higher than 40%.
For Tmax the range for CVs for each drug is presented.
Results
A total of 43 pharmacokinetic studies on single dose, oral administration of 5 triptans were retrieved (none for naratriptan and frovatriptan): 12 studies with rizatriptan (5 – 10 mg), 9 studies with almotriptan (12.5 – 25 mg), 4 studies with eletriptan (30 – 80 mg), 9 studies with sumatriptan (25 – 300 mg), and 4 studies with zolmitriptan (2.5 – 10 mg). I found no studies with variability data for naratriptan and frovatriptan.
CVs for Cmax in studies with the 5 triptans was distributed as follows: rizatriptan, <40% = 5, >40% = 7; almotriptan, <40% = 9, >40% = 0; eletriptan, <40% = 0, >40% = 4; sumatriptan, <40% = 7, >40% = 2; zolmitriptan, <40% = 3, >40% = 1.
The ranges for CVs for Tmax were: rizatriptan = 27% – 87%; almotriptan = 28% – 65%, sumatriptan = 26% – 58%. For eletriptan the CVs were 59% and 64% in 2 studies.
Two additional studies investigated oral absorption of a triptan both during and outside migraine attacks. There was no difference in mean Cmax but the CV ratios (during attacks/outside attacks) were: 95%/59% (rizatriptan 5 mg), 65%/40% (sumatriptan 25 mg), 76%/39% (sumatriptan 50 mg), and 52%/41% (sumatriptan 100 mg).
Conclusion
A CV > 40% is generally regarded as indicating a high degree of variability in the item reported;
and the present review thus indicates moderate/high variability of the early oral absorption of several triptans. Almotriptan is probably an exception with smaller variability.
The variability observed in this review with fasting subjects could be higher during migraine attacks as indicated by an increased CV ratio for Cmax for migraine attacks versus outside attacks in 4 cases.
When treating a migraine attack with a triptan the physician should be aware that the dose administered can in reality “be equivalent to both lower or higher doses” than the declared dose of the tablet because of the pharmacokinetic variability. There can be no firm recommendations of how to deal with this problem; but a rational use of the trial and error method will probably benefit the patients.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-02-180
Phase 3 Study (SPARTAN) of Lasmiditan Compared to Placebo for Acute Treatment of Migraine
Linda A. Wietecha1, Bernice Kuca2, Michael G. Case1, Katherine J. Selzler1, Sheena K. Aurora1*
1Eli Lilly and Company
2CoLucid Pharmaceuticals, Inc., a wholly owned subsidiary of Eli Lilly and Company, Indianapolis, United States
Objectives
To compare efficacy on headache pain and the patient-centric measure of most bothersome symptom (MBS; nausea, phonophobia, or photophobia) at 2 hours post-dose and safety following treatment with lasmiditan 200 mg, 100 mg, 50 mg, or placebo.
Methods
In this randomized, double-blind, placebo-controlled study, patients with at least moderate disability (Migraine Disability Assessment Score ≥11) were randomized 1:1:1:1 to a first dose of lasmiditan treatment (200 mg, 100 mg, or 50 mg) or placebo (ClinicalTrials.gov number NCT02605174). Patients were asked to take the first dose within 4 hours of onset of a migraine attack (moderate severity or worse and not improving). If needed, patients took a randomly assigned second dose of either their previously assigned lasmiditan dose or placebo for rescue or recurrence of migraine (2 to 24 hours post-initial dose); patients randomized to placebo received placebo as the second dose. The primary analyses compared the proportions of patients (modified intent-to-treat population [mITT]) in the lasmiditan 200-mg group with the placebo group who were headache pain-free and who were MBS-free at 2 hours post-first dose. Comparisons were made via logistic regression with terms for treatment group and background migraine preventative use. Lasmiditan 100 mg and 50 mg were also compared to placebo and safety was assessed by treatment-emergent adverse events.
Results
Results will be provided once data become available to include the following:
- Primary Efficacy Analyses: treatment comparison between lasmiditan 200 mg and placebo for patients who are headache pain-free and patients who are MBS-free at 2 hours post-first dose.
- Secondary Efficacy Analyses: treatment comparison between lasmiditan 100 mg and 50 mg with placebo for patients who are headache pain-free and patients who are MBS-free at 2 hours post-first dose.
- Safety Results
Conclusion
Conclusions will be provided once data become available.
Disclosure of Interest
L. Wietecha Conflict with: Minor shareholder of Eli Lilly and Company, Conflict with: A full-time employee of Eli Lilly and Company, B. Kuca Conflict with: A full-time employee of CoLucid Pharmaceuticals, Inc., a wholly owned subsidiary of Eli Lilly and Company, M. Case Conflict with: Minor shareholder of Eli Lilly and Company, Conflict with: A full-time employee of Eli Lilly and Company, K. Selzler Conflict with: Minor shareholder of Eli Lilly and Company, Conflict with: A full-time employee of Eli Lilly and Company, S. Aurora Conflict with: Minor shareholder of Eli Lilly and Company, Conflict with: A full-time employee of Eli Lilly and Company
Migraine Preventive Therapy
PO-02-181
Healthcare resource utilization among migraine sufferers in the EU5 from the patient perspective
Pamela Vo1*, Aikaterini Bilitou2, Juanzhi Fang3, Annik Laflamme1 and Shaloo Gupta4
1Novartis Pharma AG, Basel, Switzerland
2Novartis Global Services Center, Dublin, Ireland
3Novartis Pharmaceuticals Corporation, New Jersey
4Kantar Health, NY, United States
Objectives
Migraine is a disabling neurological condition. The purpose of this study was to understand the incremental burden of migraine on healthcare resource utilization (HRU) in adults in Europe from the National Health and Wellness Survey (NHWS), a self-administered, internet-based questionnaire.
Methods
A retrospective, cross-sectional analysis of NHWS responses collected in 2016 from the EU5 (France, Germany, Italy, Spain, and UK) was performed. Adult (≥18 years old) respondents with a self-reported migraine diagnosis who completed the migraine module and with migraine experienced for ≥4 headache days in the past month were matched by propensity scores using sociodemographic characteristics to respondents without migraine (controls). HRU was evaluated via the number of healthcare provider (HCP) visits, emergency department (ED) visits and hospitalizations in the past six months. Mann-Whitney and Chi-square tests were used to determine significant differences between groups.
Results
Among respondents with migraine (≥4 headache days/month; n = 218), 79.4% were female, the mean age was 43.25 years (SD = 13.48), and 60.1% were married or living with partner. Furthermore, 39.9% completed a university education and 62.4% were employed. Analysis of the propensity score-matched sample of 218 migraineurs and 218 controls showed that in the 6 months prior to questionnaire completion, the mean number of HCP visits (8.48 vs. 5.13, p < 0.001) and ED visits (0.46 vs. 0.21, p = 0.011) were significantly higher for migraine patients than those without migraine. The number of hospitalizations was higher among migraine patients (0.18 vs. 0.11, p = 0.056) but marginally significant. Compared with matched controls, a significantly higher proportion of migraine respondents had ≥1 visits to a general/family practitioner (77.1% vs. 67.4%, p = 0.025), neurologist (13.8% vs. 3.7%, p < 0.001), and psychiatrist (13.3% vs. 3.2%, p < 0.001) in the prior 6 months. The proportion of individuals with ≥1 ED visit was significantly higher for migraine patients than those without migraine (20.6% vs. 12.4%, p = 0.02) whereas the proportion hospitalized (12.8% vs. 7.3% p = 0.056) was slightly higher, but marginally significant.
Conclusion
Results demonstrated a statistically significant increase in HRU in terms of HCPs, neurologists, psychiatrists, and ED visits for migraine patients compared with non-migraine controls. To help reduce the burden of migraine on the European healthcare system better treatment options for migraineurs should be investigated.
Disclosure of Interest
P. Vo Conflict with: Novartis, A. Bilitou Conflict with: Novartis, J. Fang Conflict with: Novartis, A. Laflamme Conflict with: Novartis, S. Gupta Conflict with: Kantar Health
Migraine Preventive Therapy
PO-02-182
The Effects of Aerobic Exercise on migraine headache intensity
Maryam Seyfi-shahpar1, Maryam Abolhasani2, Soodeh Razeghi Jahromi1 3*, Fahimeh Martami1, Mansoureh Togha3, Zeinab Ghorbani3 4
1Department of Clinical Nutrition and Dietetics, Faculty of Nutrition and Food Technology, Beheshti University of Medical Sciences
2Sports Medicine Research Center, Neuroscience Institute
3Headache Department, Iranian Center of Neurological Research, Neuroscience Institute
4School of Nutritional Sciences and Dietetics, Tehran University of Medical Sciences, Tehran, Iran, Islamic Republic Of
Objectives
For people with migraine, exercise is often suggested to health promotion and disease prevention. Recently the role of exercise in the management of migraine is considered, but there are no guidelines in the literature regarding how patients with migraine should be instructed to exercise. The aim of this study was to evaluate the influence of an aerobic exercise on migraine intensity.
Methods
In this study 50 untrained patients were recruited and randomized to two groups. The intervention group (n = 25) participated in aerobic exercise program 3 times per week during 8 weeks, for 45–60 minutes with intensity between 50% to 65% of maximal heart rate. Control group only received common medical treatment without change. Borg’s Rate of Perceived Exertion scale (RPE scale, 6–20) was used to set the training intensity. Each training session included a 15-minute warm-up period (intensity: RPE scale, 11–13).the intensity of migraine headache was measured at the baseline and after intervention with VAS (Visual Analog Scale).
Results
The intensity of migraine headache reduced significantly in exercise group (1.95 ± o.8) compared to control group (0.81 ± 1). (P = 0.00)
Conclusion
Incorporating exercise into common headache treatments may be a useful approach to managing migraine headache symptoms. According to our study aerobic exercise with moderate intensity can reduce intensity of migraine headache. Future study is recommended to evaluate the efficacy of other types of exercise with different intensity in migraine headache management.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-02-183
Multi-species probiotic mixture can attenuate the severity of episodic migraine- a double blind randomized controlled trial
Fahimeh Martami1, Maryam Seyfi-shahpar1, Zeinab Ghorbani2 3, Soodeh Razeghi Jahromi1 3*, Mansoureh Togha3 and Hossein Ansari4
1Department of Clinical Nutrition and Dietetics, Faculty of Nutrition and Food Technology, Beheshti University of Medical Sciences
2School of Nutritional Sciences and Dietetics
3Headache Department, Iranian Center of Neurological Research, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran, Islamic Republic Of
4UC San Diego, San Diego, United States
Objectives
Migraine is a recurrent disorder with a lifetime prevalence of 13% in men and 33% in women. Pro-inflammatory cytokines can act on the nociceptors of the trigeminal nerve, causing migraine. A strong trigger of pro-inflammatory immune responses is the leakage of lipopolysaccharides from the intestinal lumen into the circulation. Probiotics are able to improve the intestinal barrier defense mechanism and stimulate the production of tight junctional protein mucins. These effects limit small intestinal permeability and suppress inflammation. Therefore probiotics supplementation can have beneficial effect in migraineurs. In current double blind, placebo-controlled trial, we investigated the effect of a probiotic supplementation containing 14 bacterial strains as an adjuvant therapy on severity and incidence of episodic migraine.
Methods
50 migraineurs, 35 female and 15 male (mean age of 38.74 ± 7.5 Y) were recruited and randomly assigned to placebo and probiotic group (two capsules/d for 8 weeks). Probiotic supplement (Bio-Kult-protexin: 2 × (10)^9 CFU/capsule) contained 14 bacterial strains included Bacillus subtilis PXN 21, Bifidobacterium bifidum PXN 23, Bifidobacterium breve PXN 25, Bifidobacterium infantis PXN 27, Bifidobacterium longum PXN 30, Lactobacillus acidophilus PXN 35, Lactob. delbrueckii ssp. bulgaricus PXN 39, Lactob. casei PXN 37, Lactob. plantarum PXN 47, Lactob. rhamnosus PXN 54, Lactob. helveticus PXN 45, Lactob. salivarius PXN 57, Lactococcus lactis ssp. lactis PXN 63, Streptococcus thermophilus PXN 66. Episodic migraine was diagnosed by neurologist according to ICHD III beta critaria. Demographic characteristics, medications, precedent medical history of gastrointestinal disorders, anthropometric measurements, and Migraine disability assessment scale (MIDAS) were documented at baseline visit and at the end of the study. During the intervention, all patients were instructed to record frequency, intensity (10-point scale), and duration of migraine attacks, as well as used analgesics.
Results
Eight weeks of probiotic consumption resulted in significant reduction of the frequency (from 7 ± 3 to 4 ± 3 days/week), intensity (7 ± 2 to 5 ± 1), and duration (7.25 ± 3.7 to 7.02 ± 3.7 hours/day) of attacks (P = 0.001, 0.000, 0.004 respectively). In placebo group, the intensity and frequency of attacks did not changed significantly. Probiotic supplementation also significantly affect MIDAS and analgesics consumption (p < 0.001). The mean reduction of the frequency, intensity, MDAS, and analgesics consumption was significantly greater in probiotic group compared to placebo (P = 0/001, 0.007, 0.000, and 0.007 respectively). The differences remained significant after adjusting for confounding factors.
Conclusion
In patients with episodic migraine, adding probiotic to current prophylactic medication might beneficially affect headache control.
Disclosure of Interest
None Declared
Migraine Preventive Therapy
PO-02-184
Real-world patient perspective on the burden and impact of migraine
Elena Ruiz de la Torre1, Paolo Martelletti2 3, Audrey Craven1 4, Donna Walsh4, Simon Evans5, Paula Dumas6, Hans-Christoph Diener7, Michel Lanteri-Minet8, Todd J. Schwedt9, Jean-Pierre Malkowski10, Monisha Sodha11, Susann Walda11, Anne Aronsson11, Annik Laflamme10, Pamela Vo10*
1European Headache Alliance
2European Headache Federation
3Department of Clinical and Molecular Medicine, Sapienza University of Rome, Rome, Italy
4European Federation of Neurological Associations
5Migraine Action, United Kingdom
6Migraine Again, United States
7Department of Neurology and Headache Center, University of Duisburg-Essen, Germany
8Département d’Evaluation et Traitement de la Douleur, Centre Hospitalo-Universitaire de Nice, France
9Department of Neurology, Mayo Clinic, United States
10Novartis Pharma AG, Basel
11GFK Health, Switzerland
Objectives
Migraine is a prevalent condition affecting about 11% of the adult population. It has debilitating symptoms and affects patient functioning. The present study was undertaken to understand the full burden and impact of migraine in everyday life from the patient’s point of view.
Methods
This cross-sectional study was conducted using Online Bulletin Boards (OBB). This interface was developed for online survey, discussions and interactions led by a trained facilitator over a period of 4 consecutive days. Adults with chronic and episodic migraine aged between 25 and 60 years old were recruited to participate in 6 OBBs established in Germany, Italy and USA (2 per country). Participants were blinded to each other and agreed to partake for at least 30 minutes each day in the OBBs, where they were asked to respond to specific questions on migraine and to provide their perspective on statements and other participants’ blinded responses. All responses were aggregated by country and qualitatively analyzed.

Results
A total of 60 migraine patients participated in this pilot phase of a large global study (20 per country). About half (47%, n = 28) reported having been diagnosed with migraine, either by a general practitioner (GP) or neurologist within the year following the date of their 1st symptoms. Table 1 summarizes the 3 most common migraine attack triggers, symptoms, and coping mechanisms reported by patients. All respondents reported important limitations resulting from migraines in private, professional and social aspects of life, mainly the disruption of daily routines, significant strain on personal relationships, difficulty caring for children, and missed days of work, deadlines, or social events. Anxiety and frustration were most frequently reported as emotional consequences of migraine in private/social life (92% and 72%) and work (97% and 88%). 87% of patients (n = 52) had seen a physician for migraine management but many (85%, n = 51) did not consult regularly, especially if their diagnosis had occurred long ago. Two thirds (n = 38/63%) of respondents reported getting functional and emotional support from family and friends, but wished for improved understanding/compassion from others and more efficacious medications.
Conclusion
This study highlights the substantial functional and emotional burden migraine exerts on individuals, as well as the significant unmet needs that remain for these patients despite currently available care and treatment options.
Disclosure of Interest
E. Ruiz de la Torre: None Declared, P. Martelletti Conflict with: Department of Clinical and Molecular Medicine, Sapienza University of Rome, Italy, A. Craven: None Declared, D. Walsh: None Declared, S. Evans: None Declared, P. Dumas: None Declared, H.-C. Diener: None Declared, M. Lanteri-Minet: None Declared, T. Schwedt: None Declared, J.-P. Malkowski Conflict with: Novartis, M. Sodha Conflict with: GFK Health, S. Walda Conflict with: GFK Health, A. Aronsson Conflict with: GFK Health, A. Laflamme Conflict with: Novartis, P. Vo Conflict with: Novartis
Migraine Preventive Therapy
PO-02-185
Burden and impact of migraine: a caregiver’s perspective
Elena Ruiz de la Torre1, Paolo Martelletti2 3, Audrey Craven1 4, Donna Walsh4, Simon Evans5, Paula Dumas6, Hans-Christoph Diener7, Michel Lanteri-Minet8, Todd J. Schwedt9, Jean-Pierre Malkowski10, Monisha Sodha11, Susann Walda11, Anne Aronsson11, Annik Laflamme10, Pamela Vo10*
1European Headache Alliance
2European Headache Federation
3Department of Clinical and Molecular Medicine, Sapienza University of Rome, Rome, Italy
4European Federation of Neurological Associations
5Migraine Action, United Kingdom
6Migraine Again, United States
7Department of Neurology and Headache Center, University of Duisburg-Essen, Germany
8Département d’Evaluation et Traitement de la Douleur, Centre Hospitalo-Universitaire de Nice, France
9Department of Neurology, Mayo Clinic, United States
10Novartis Pharma AG, Basel
11GFK Health, Switzerland
Objectives
Migraine has far-reaching impacts on the family and relatives of individuals with migraine and only limited evidence is available to describe this reality. In an effort to better understand the full burden and impact of migraine, this study sought to describe the effect of migraine from the caregiver’s perspective.
Methods
This cross-sectional study was conducted as a feasibility assessment for a global migraine survey, using Online Bulletin Boards (OBB). This interface was developed for online survey, discussions and interactions led by a trained facilitator over a period of 4 consecutive days. Caregivers aged 25 years or older who were caring for an adult migraine patient in their household were recruited to participate in 3 OBBs established in Germany, Italy and USA (1 per country). The participants were blinded to each other and agreed to partake for at least 30 minutes each day in the OBBs, where they were presented and asked to respond to specific questions on migraine and provide their perspectives on statements and other participants’ blinded responses. All responses and inputs were aggregated by country and qualitatively analyzed.
Results
A total of 30 caregivers participated in this pilot phase of a large global study (10 per country). All caregivers reported that they were highly involved in the management of migraine and that they spent an average of 15 hours per month supporting their family member suffering from migraine. Stress, exhaustion and feeling overwhelmed with the amount of work resulting from their caregiving activities were reported by 83% (n = 25/30) of respondents. They described themselves as powerless witnesses of the frequent and intense suffering of their loved ones and wanting to be helpful while knowing the limits of what they could do. 60% (n = 18/30) of caregivers reported a worsening of personal relationships over time due to migraines. Regardless of whether they were employed, unemployed or retired, 83% of caregivers (n = 25/30) reported that their caregiver role affected their lives due to the significant changes it imposed on their own daily routines and schedules. This thereby affected private life, social engagements, relationships, and professional obligations, including having fear of losing employment. Most caregivers (87%, n = 26/30) reported ambivalent feelings, being torn between commitment, self-sacrifice and resentment, but all agreed that migraine patients were thankful for their help and assistance.
Conclusion
Caregiving has a major impact on the lives of close relatives supporting migraine patients. This study highlights how the burden of migraine extends beyond the patients, with substantial functional and emotional impacts of the disease on caregivers as well. This pilot also confirmed the unique opportunity that this type of study and interface provides for insights into the caregivers’ experience and unmet needs in the current treatments available to migraine patients.
Disclosure of Interest
E. Ruiz de la Torre: None Declared, P. Martelletti Conflict with: Department of Clinical and Molecular Medicine, Sapienza University of Rome, Italy, A. Craven: None Declared, D. Walsh: None Declared, S. Evans: None Declared, P. Dumas: None Declared, H.-C. Diener: None Declared, M. Lanteri-Minet: None Declared, T. Schwedt: None Declared, J.-P. Malkowski Conflict with: Novartis, M. Sodha Conflict with: GFK Health, S. Walda Conflict with: GFK Health, A. Aronsson Conflict with: GFK Health, A. Laflamme Conflict with: Novartis, P. Vo Conflict with: Novartis
Other Primary Headache Disorders
PO-02-186
Outcome of Inpatient Management of Refractory New Daily Persistent Headache
Shathabish Kariyanna1*, Merle Diamond2 and Athena Kostidis3
1Headache Medicine, Loyola University Medical Center/Diamond Headache Clinic
2Headache Medicine, Presence St.Joseph Hospital, Chicago
3Headache Medicine, Loyola University Medical Center, Maywood, United States
Objectives
New Daily Persistent Headache (NDPH) is one of the chronic refractory headache conditions and there is limited evidence about its treatment. NDPH causes a severe burden and impairs the functioning of patients that suffer from it. Objective is to determine the outcome of comprehensive inpatient treatment of patients diagnosed with refractory NDPH, mainly whether there is an acute improvement in pain scale when comparing admission to discharge headache assessment.
Methods
This is a retrospective chart review of 73 patients who underwent comprehensive inpatient treatment program which included pharmacological, psychological and ancillary therapy for NDPH. All patients had previously failed multi-approach outpatient treatment and some had failed inpatient treatment as well. Records were reviewed of patients admitted between January 2015 and December 2016. All patients satisfied the ICHD-3 diagnostic criteria for NDPH. At least a 3-point improvement in pain score at discharge was considered clinically significant.
Results
The headache pain rating on a 0–10 pain scale was at a mean of 7.2 at admission and 3.1 on discharge (P < .00001). The majority (55/73, 75.3%) of patients had clinically significant improvement in their pain score and (33/73, 45.2%) had 5 or more points improvement. The average length of stay was 8.4 days. Out of 73 patients, 60 had migraine phenotype, 4 had tension type and 9 patients had both. Age range was between 18 and 73 with mean of 36.7 years. The bulk of the patients 63% were female and males accounted for remaining 37%. The average time since headache onset was 2.5 years. Medication overuse at the time of admission was seen in 29 patients and 50% of them overused opiates. Intravenous Dihydroergotamine (DHE) was the mainstay pharmacological treatment (64/73, 87.7%) patients received. There were minimal known non serious adverse events. The average total DHE dosage during the hospital stay was 10.5 mg which was given in doses ranging from 0.5 to 1 mg per predefined protocol. The majority of the remaining patients received IV sodium valproate or other IV medications mentioned below. All patients were provided with as needed non-opiate IV medications based on their pain level. These medications included NSAID, muscle relaxants and neuroleptics.
Conclusion
Comprehensive inpatient treatment significantly improves pain score in patients with refractory NDPH who had previously not responded to different outpatient therapies. IV DHE therapy with predefined protocol may be considered as current standard for refractory NDPH. Controlled trials may confirm this and further studies may provide a better picture of managing this refractory primary headache syndrome.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-02-187
Highly positive effect on health care costs and productivity after treatment of medication-overuse headache – results from the multicenter COMOESTAS project
Pernille Jellestad1, Louise N. Carlsen1, Maria L. Westergaard1, Rigmor H. Jensen1* and Cristina Tassorelli2
1Danish Headache Center, Copenhagen, Denmark
2Headache Science Centre Mondino Institute, Pavia, Italy
Objectives
To estimate direct and indirect headache-related healthcare costs from baseline to 6 months after treatment of MOH patients.
Methods
This prospective longitudinal study was a part of the COMOESTAS project. Patients with MOH were included from four European and two Latin American headache centers. Costs of acute medication, costs of health care services, and measurement of productivity were calculated before and after MOH treatment.
Results
A total of 475 patients (71%) completed the treatment and were followed up after 6 months. Direct healthcare costs were significantly reduced by 52% (P < 0.001) for the total study population. Significant reductions were seen in both number of consumed tablets with 71% (P < 0.001) and number of visits to physicians with 43 % (P < 0.001). Fifty percent of patients reduced their number of consumed tablets ≥80%. Productivity loss (absenteeism from work and reduction of productivity ≥50 % during the workday due to headache) were reduced by 21% and 34% respectively (P < 0.001).
Conclusion
Globally standardized treatment of MOH significantly reduced the direct healthcare costs and increased productivity. This emphasizes the urgent need for awareness and treatment of MOH.
Disclosure of Interest
None Declared
Other Secondary Headache Disorders
PO-02-188
“Pure” detoxification for medication-overuse headache is the most effective treatment: A randomized controlled trial with 6- and 12-month follow-up
Louise N. Carlsen1, Signe B. Munksgaard1*, Lars Bendtsen1 and Rigmor H. Jensen1
1Danish Headache Center, Department of Neurology, Rigshospitalet, University of Copenhagen, Glostrup, Denmark
Objectives
There is lack of evidence on how acute headache medication should be reduced during detoxification for medication-overuse headache (MOH). The aim of this study was to compare the effect of a two-month complete stop of all acute headache medication with a restricted intake in MOH patients.
Methods
MOH-patients were included in a prospective, open-label study and randomized to a 2-months outpatient detoxification program with either A) no acute headache medication or B) acute headache medication restricted to two days/week. Both groups received education on MOH and headache in general and were followed up at 2, 6 and 12 month.
Results
We included 72 patients. Of these 59 succeeded in detoxification, 58 (81%) were followed-up at 6 months and 53 (74%) at 12 months. Patients in program A had a significantly higher reduction in the primary efficacy parameter headache frequency (25 to 13 days/month; 46%) at 6-months follow-up than patients in program B (25 to 19 days/month; 22%) (p = 0.005). After 12 months, headache frequency was reduced by 45% to 13.8 days/month in Program A, and by 31% to 17.0 days/month in Program B (p = 0.14).
Significantly more patients in program A reverted to episodic headache at 6-month (70% vs. 42%, p = 0.04) and 12-month follow-up (74% vs. 42%, p = 0.02).
The number of patients with chronic migraine was decreased from 15 to 1 in program A and from 17 to 8 in program B (p = 0.02).
There were no differences in drop-out rates between the two groups.
Conclusion
Detoxification without any acute medication for two months was more effective than detoxification with restricted intake of analgesics in reducing headache frequency, in converting MOH to episodic headache and particularly in reducing the number of patients with chronic migraine.
Disclosure of Interest
L. Carlsen: None Declared, S. Munksgaard Conflict with: Merck, Allergan, Conflict with: Berlin-Chemie, UCB, L. Bendtsen Conflict with: Allergan, Novartis and Biogen, R. Jensen Conflict with: ATI, Electrocore, Eli-Lilly and Linde Gas ltd, Conflict with: Pfizer, Berlin-Chemie, Allergan, Merck, ATI
Other Secondary Headache Disorders
PO-02-189
Prevalence of Migraine in Patients with Idiopathic Intracranial Hypertension (IIH) in Comparison to the general population
Mansoureh Togha1*, Kamran Shirbache1, Reza Rahmanzadeh1, Zeinab Ghorbani1, Shirin Behbahani1 and Farshid Refaeian1
1Headache department, Iranian Center of Neurological Research, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran, Islamic Republic Of
Objectives
Idiopathic intracranial hypertension (IIH) is a neurological disorder that is characterized by increased intracranial pressure (ICP) accompanied by a small or normal sized ventricles of the brain. The main presenting symptom of IIH is headache that usually is severe. IIH may lead to visual and hearing impairment or even loss of vision. The initial treatment would be medical and conservative. However, some patients may even need surgical intervention to divert CSF flow to decrease the intracranial pressure. On the other hand it seems that migraine headache is common among IIH patients and sometimes it is misdiagnosed as the headache of IIH and might lead to inappropriate management. In the present study, the prevalence of migraine in IIH patients is explored in comparison with the normal population.
Methods
In this case-control study, the presence of migraine in 108 IIH patients was evaluated in comparison to 103 non-IIH subjects. The diagnosis of IIH and migraine was done according to the diagnosis criteria of high opening CSF pressure (>25–40cmH2O) and (ICHD III beta) criteria. In order to collect the required information, all subjects were interviewed by a trained medical student. A checklist for migraine diagnosis was filed. Demographic data was collected. IIH patient’ medical documents were explored and variables such as age, BMI (Body Mass Index), Cerebro-Spinal Fluid pressure, presence or absence of Papilledema were studied. Data analysis was done using Stata software, Version 11.
Results
211 subjects (86.7% female) with mean age of 38.04 ± 12.19 and mean BMI of 28.12 ± 4.93 kg/m2 were studied. In the IIH patients 93 cases (81.6%) had papilledema and the mean CSF pressure was 32.10 cm H2O (Range: 26 cm H2O to 65 cm H2O). There were 70 (64.8%) and 22 (21.4%) migraine patients in case and control groups respectively which the difference was found significant (P-value<0.001). In 26 of 70 (24.1%) migraine cases in IIH group the disorder was diagnosed after developing IIH. The risk of affecting by migraine in IIH patients was 6.17 times greater than the non-IIH group (95%CI = 3.56–14.36 p < 0.01).
Conclusion
According to the higher probability of migraine and even the possibility of developing new onset migraine in IIH patients, taking precise headache history in the follow up period is necessary. This consideration prevents misdiagnosis of migraine headache as the recurrence of IIH or uncontrolled IIH and its inappropriate management.
Disclosure of Interest
None Declared