
Abstract
Background
Most studies on intracranial abnormalities among headache sufferers were performed in selected clinical populations. The aim of this study was to evaluate the relationship between intracranial abnormalities and headache among middle-aged adults in the general population.
Methods
Participants in a large epidemiological study (the HUNT 3 study; 2006–2008) who answered a headache questionnaire and participated in a population-based imaging study of the head (HUNT MRI; 2007–2009) were included (n = 864; age, 50–65 at enrollment). Based on the responses to the HUNT 3 questionnaire, respondents were categorized as having migraine, tension-type headache, or unclassified headache. Logistic regression was used to compare the occurrence of intracranial abnormalities between groups.
Results
Intracranial abnormalities were more common in headache sufferers than in headache-free individuals (29% vs. 22%, respectively; p = 0.041). Adjusted multivariate analyses revealed that those with tension-type headache had higher odds of having minor abnormalities (odds ratio, 2.13; 95% confidence interval = 1.18–3.85). This association disappeared when those with only white matter hyperintensities were removed from the analysis.
Conclusions
Headache sufferers had increased odds of minor intracranial abnormalities. The increased odds were primarily related to the presence of white matter hyperintensities.
Keywords
Introduction
During the course of a single year, more than 50% of the adult population will suffer from headache (1). A considerable number of attacks are tension-type headache (TTH) or migraine, the two most common primary headache disorders, with an overall mean prevalence of 21% and 15%, respectively (2). Sometimes, however, headaches can originate from intracranial pathology, e.g. neoplasms or Chiari malformations (3,4). Pineal cysts can also cause headache (5–7). Furthermore, migraineurs, at least those experiencing aura as part of an attack, have an increased risk both of clinical and silent cerebral infarctions (8–12). Considering that headache may be secondary to intracranial pathology, and that migraine with aura is associated with an increased risk of cerebral ischemia, one might expect that headache sufferers show more abnormalities on neuroimaging than non-sufferers.
Several studies provide estimates on the prevalence of intracranial abnormalities among headache sufferers with normal neurological clinical examinations (13–18). Early reviews, mostly including studies based on computed tomography (CT), revealed that 2.4% of individuals with any headache, and 0.2%–0.4% with migraine, had “clinically significant” intracranial abnormalities (13–15). A later neuroimaging study, based on either magnetic resonance imaging (MRI) or CT (16), found fewer “significant/major” abnormalities compared to a study using MRI only (17). This was true for individuals having any headache (0.9% vs. 3.7%), TTH (0.8% vs. 1.4%), migraine (0.4% vs. 0.6%), and unclassified headache (3.7% vs. 14.1%) (16,17). Another MRI study found clinically important abnormalities in 0.7% of individuals with chronic or recurrent headache (18).
All of the aforementioned studies enrolled patients attending clinics for headache and, therefore, provide clinicians with information that is useful for making decisions regarding whether to perform neuroimaging of headache patients seeking medical help for the condition. However, general population studies are needed to circumvent potential referral bias in clinical populations, thereby evaluating the actual association between headache and intracranial abnormalities.
The aim of the present population-based study was to examine the relationship between intracranial abnormalities and headache among middle-aged adults drawn from the Nord-Trøndelag Health Studies (HUNT), and a neuroimaging sub-study (HUNT MRI).
Methods
Participant selection
HUNT are large population-based health surveys that were conducted in the Norwegian county of Nord-Trøndelag during 1984 to 1986 (HUNT 1), 1995 to 1997 (HUNT 2), and 2006 to 2008 (HUNT 3). Anyone aged 20 years or older at the respective time points was invited to participate. Details of the participants and how the HUNT studies were performed have been described previously (19–23).
The HUNT MRI neuroimaging study involved 1494 individuals (age range, 50–65) living within 45 minutes of Levanger Hospital and who had participated in all three HUNT studies. During 2007–2009, 1088 individuals provided informed consent to participate (a response rate of 71%), and 1006 underwent MRI of the head (476 men and 530 women) (24).
HUNT MRI
The exclusion criteria for HUNT MRI were the same as those for standard MRI: i.e. ferromagnetic foreign body, weight >150 kg and claustrophobia. All participants were scanned in a 1.5 T General Electric Signa HDx 1.5 T MRI scanner equipped with an eight-channel head coil (GE Healthcare) and software version pre-14.0 M. T1-weighted magnetization-prepared rapid acquisition with gradient echo (MPRAGE) volume, transverse T2, T2*, and fluid-attenuated inversion recovery (FLAIR) sequences, a time of flight three-dimensional (3D) angio sequence, and diffusion-tensor imaging were obtained for each participant. The images were independently evaluated by two experienced neuroradiologists. Differences of opinion were resolved by consensus following discussion. White matter hyperintensities (WMH) were graded according to the Fazekas score (25). The neuroradiologists were not provided with clinical information, but knew the participants’ names and birth date. They were also able to access previous radiological assessments and clinical data in cases of abnormal findings. In addition, certain participants were interviewed by phone to verify a diagnosis of multiple sclerosis, cerebral contusion, or progressive supranuclear palsy, and to differentiate between silent and clinical infarctions of the brain.
Headache categories
Of the 1006 individuals who participated in HUNT MRI, 864 (86%) answered the first headache-related question in HUNT 3, “Have you suffered from headache during the last year?” and were considered respondents. A validation study showed that this screening question had a sensitivity of 88% and specificity of 86% (26) when used to identify headache sufferers.
Based on data derived from the subsequent 13 headache questions, respondents were categorized as having one of four mutually exclusive headache diagnoses: headache free, TTH, migraine, or unclassified headache (i.e. headache sufferers who did not fulfill the diagnosis of TTH or migraine). The unclassified headache group also included those likely to be suffering from headache related to the overuse of medication (i.e. reporting headache on >14 days per month and analgesic use four times or more per week; sensitivity, 75%; specificity, 100% (26)).
The questionnaire-based diagnoses of TTH and migraine adhere closely to the criteria set out in the second and third edition of the International Classification of Headache Disorders (ICHD) (3,4). However, there were two slight differences from the ICHD-criteria: Headache duration less than four hours was accepted as migraine because the HUNT studies did not specifically ask about untreated attacks, and sensitivity to light and sound was measured with one question in HUNT 3. Due to the higher specificity of the criteria for frequent episodic and chronic TTH sufferers, only participants experiencing an episode on ≥1 day/month were diagnosed as having TTH. The validity of these criteria was reported previously (TTH on ≥1 day/month: sensitivity, 96%, and specificity, 69%; migraine using restrictive criteria: sensitivity, 51%, and specificity, 95%) (26).
Demographic variables
Questionnaire-derived data from the HUNT 3 database included a subjective health assessment, which was measured by the question “How is your health at the moment?” Those selecting the two lowest of the four options were considered to have “fair” or “poor” general health. Employment status was determined by one question (“Are you employed?”), and had a dichotomous answer. Alcohol consumption was measured by the CAGE questionnaire (27) using a cutoff value ≥1 to indicate possible alcohol abuse. A physician measured blood pressure (BP) three times, and the mean of the two last systolic blood pressure (SBP) measurements were used.
MRI findings
Intracranial abnormalities occurring in ≥1% of respondents were analyzed separately, while findings occurring in <1% of respondents were grouped together as “rare abnormalities”. Infarctions were identified based on the FLAIR, T2- and T1-weighted images following standard radiological criteria, and classified as clinical if respondents had experienced relevant symptoms, or if lesions were previously identified by CT or MRI examinations that were performed as a part of previous diagnostic procedures. Lesions were classified as contusions based on a typical appearance on MRI and the respondent reporting a history of head trauma. WMH were classified as abnormal if graded 2 or 3 on the Fazekas scale (25) in the absence of multiple sclerosis. Cysts were grouped as either arachnoid or non-arachnoid. Respondents with more than one incidence of the same finding (e.g. multiple cysts) were still counted just once in that group.
Classification of intracranial abnormalities.

Not possible to classify, but considered benign based on repeated imaging. bWhite matter hyperintensities.
Ethics approval
The study was approved by the Norwegian Data Inspectorate, the Norwegian Board of Health, and the Regional Committee for Ethics in Medical Research. All participants provided written informed consent.
Statistical analysis
A two-tailed independent t-test was used to examine differences in the prevalence of “any intracranial abnormalities” between the headache sufferers and headache-free groups. More extensive evaluation was performed by entering data from the headache and abnormality sub-groups into logistic regression analyses. Two adjusted multivariate analyses were performed, and the odds ratios (OR) and 95% confidence intervals (CI) were obtained. Model A included age as a continuous covariate, and sex as a categorical covariate. Model B additionally included SBP as a continuous covariate, and response to the CAGE questions as a categorical covariate. These adjustments were made because headache is influenced by age, sex (29), BP (30) and alcohol consumption (31): The occurrence of certain intracranial abnormalities increases with age (32), and at least some abnormalities are influenced by sex (33) and BP (34). CAGE data were missing for 9% of individuals; therefore, Model B was based on fewer individuals than Model A. Two additional analyses were carried out: multivariate analyses of the migraine group were repeated, this time including participants fulfilling the more sensitive “probable migraine” criteria (3), and multivariate analyses on the minor abnormalities group were repeated after excluding respondents with WMH as the only finding. All analyses were performed using IBM SPSS Statistics 19.
Results
Participant demographics and headache status
Background data for responders, non-responders, and headache groups.
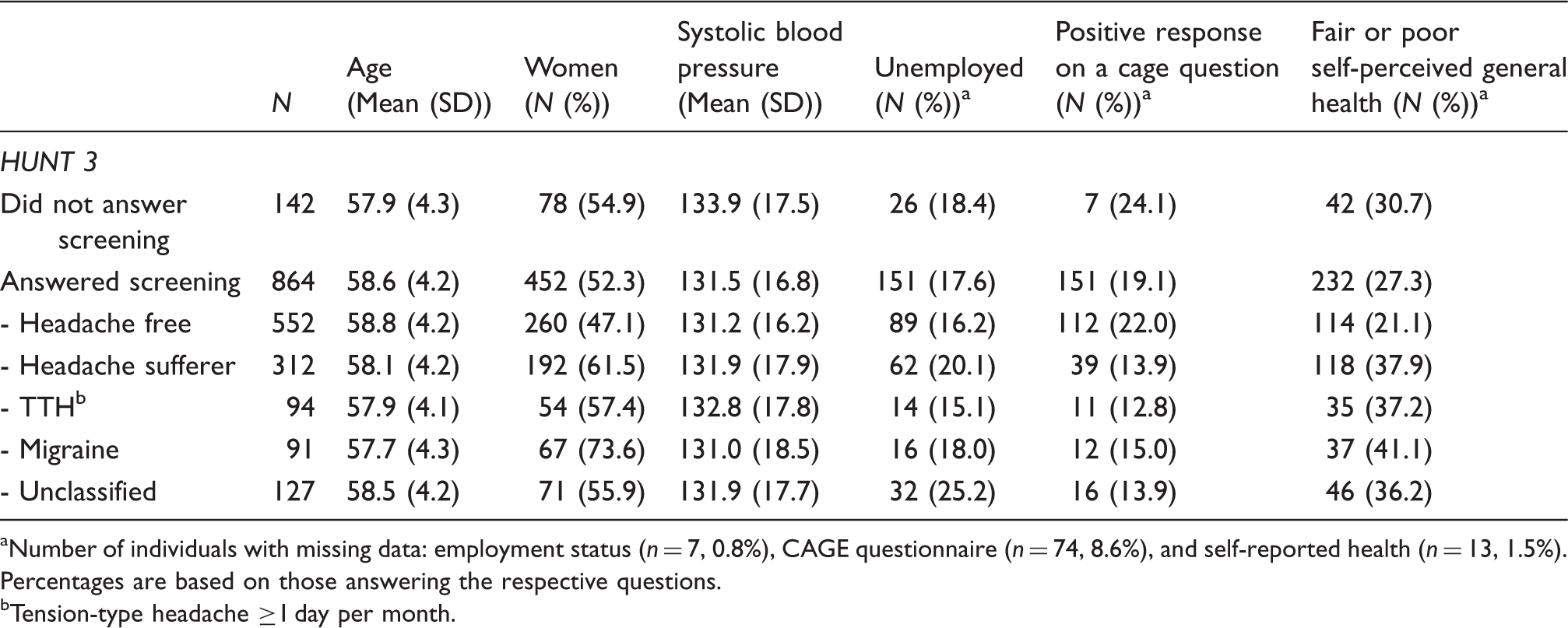
Number of individuals with missing data: employment status (n = 7, 0.8%), CAGE questionnaire (n = 74, 8.6%), and self-reported health (n = 13, 1.5%). Percentages are based on those answering the respective questions.
Tension-type headache ≥1 day per month.
Of the 312 headache sufferers, 91 had migraine, 94 had TTH, and 127 were unclassified. Fifty-two individuals fulfilled the less specific “infrequent episodic TTH” criteria, and eight individuals fulfilled the “medication-overuse headache” criteria; these individuals were assigned to the “unclassified headache” group. Using the “probable migraine” criteria led to 61 individuals formerly counted as suffering from unclassified headache being included in the migraine group.
MRI findings
Intracranial abnormalities related to current headache status.

Tension-type headache ≥1 day per month.
Pearson Chi-Square test; p = 0.041.
White matter hyperintensities with a Fazekas score 2 or 3 and no multiple sclerosis.
See Table 4 for details.
N = Number of respondents with a particular finding. Respondents may have several instances of the same abnormality, and one respondent may have more than one abnormality. Respondents with more than one type of abnormality are described in the text.
Rare abnormalities related to headache status.
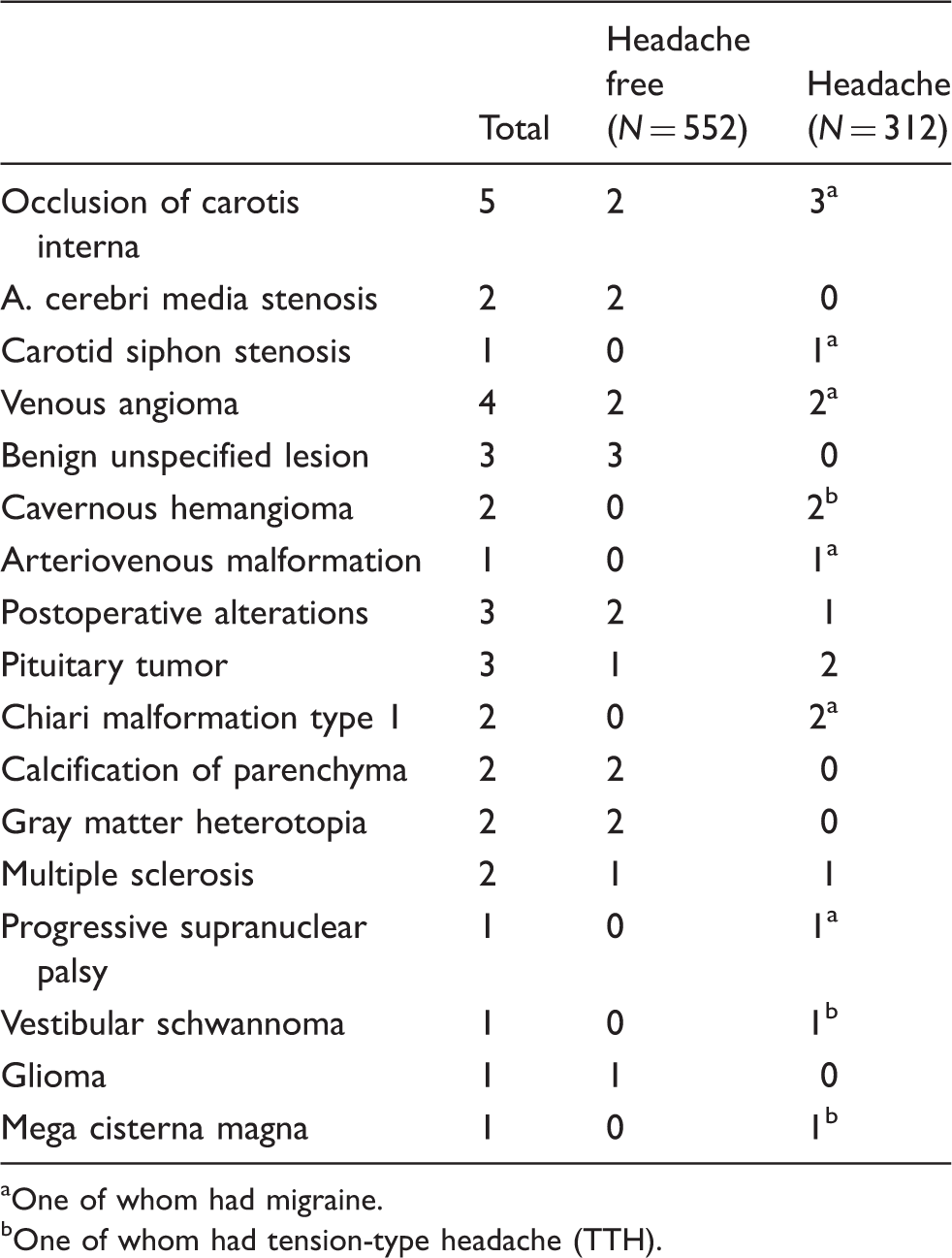
One of whom had migraine.
One of whom had tension-type headache (TTH).
Abnormalities vs. headache status
Headache status and odds ratios for intracranial abnormalities.
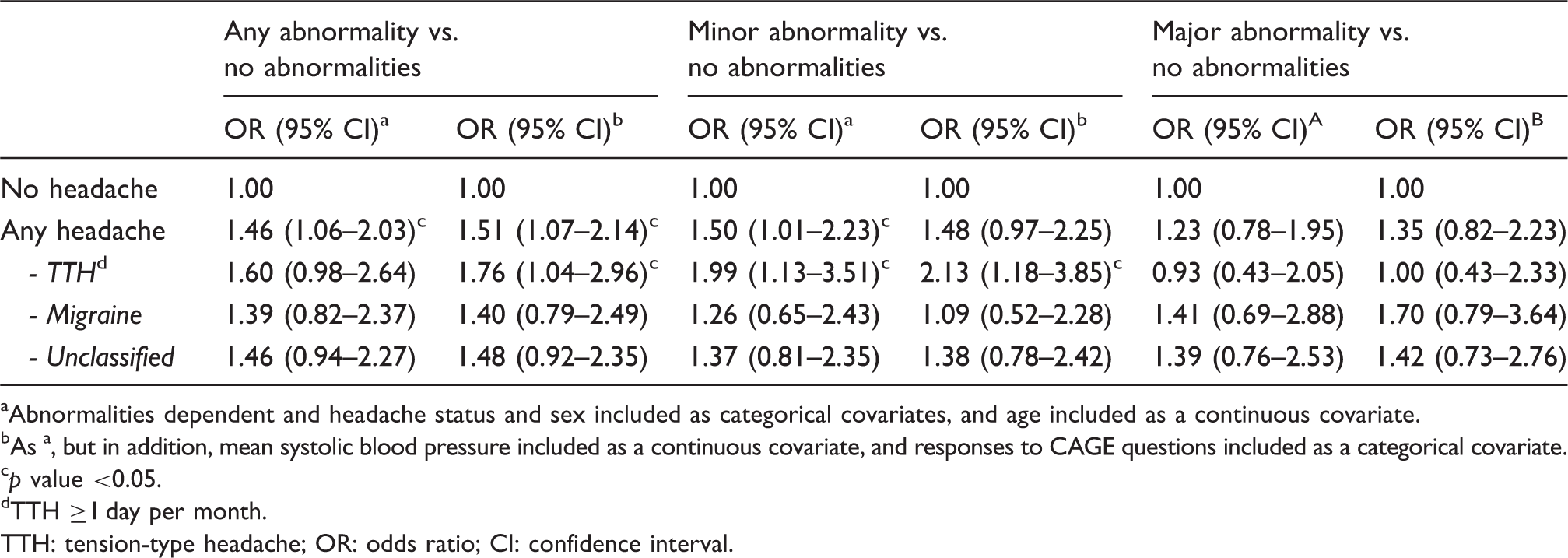
Abnormalities dependent and headache status and sex included as categorical covariates, and age included as a continuous covariate.
As a, but in addition, mean systolic blood pressure included as a continuous covariate, and responses to CAGE questions included as a categorical covariate.
p value <0.05.
TTH ≥1 day per month.
TTH: tension-type headache; OR: odds ratio; CI: confidence interval.
Discussion
The results of the present study show that headache sufferers were more likely to have intracranial abnormalities than headache-free individuals. However, this association was true only for minor abnormalities and disappeared when WMH were excluded.
Comparison with earlier studies
Several challenges are encountered when comparing these results with those of earlier reports. Earlier study populations were more selective in that they often involved referred patients or included only patients with normal findings on neurological examination (13–18,35). Also, significant abnormalities might be easier to detect when patients are referred for a specific clinical problem. In the present study, the participants were older than those in earlier studies, which is important since headache prevalence declines after the age of 50 (29). In addition, most of the earlier studies were retrospective evaluations of patients referred to a hospital, and the MRI protocol was not identical for all patients. It is also worth noting that CT (13–16) is a less sensitive method of detecting intracranial abnormalities than MRI, and that the quality of imaging techniques has improved since the earlier studies were carried out. In some studies, the images were interpreted by radiologists (16,18); however, other studies do not describe who evaluated the images (17,35). There are also differences in the type of abnormality reported (e.g. WMH were not always included) and the categorization of the abnormalities. We have provided a detailed description of all intracranial abnormalities (Tables 3 and 4) and have analyzed sub-groups based on the likelihood of the results affecting patient management (Tables 1 and 5).
Major abnormalities
Headache sufferers did not have more major abnormalities compared to headache-free individuals (Table 5). The present study is quite different from previous studies, and we found that the proportion of headache sufferers with major abnormalities (11%) was higher than reported earlier (13–18,35). An early review (mostly of CT studies) found that 2.4% of headache sufferers had potentially treatable abnormalities (13), whereas later MRI studies put the figure between 0.7% (18) and 4% (17). The proportion of individuals in each headache sub-group that had major abnormalities (Table 3) was also higher in the present study. The fact that earlier studies found fewer major intracranial abnormalities overall may perhaps be due to the exclusion of individuals with neurological findings, younger study populations, less-sensitive neuroimaging techniques, and differences in how the abnormalities were reported and grouped.
Previous studies (8–12) show that headache sufferers, especially young, female migraineurs with aura, have an increased risk for cerebral infarction. Here, we did not find more infarctions among sufferers than non-sufferers. However, the present study may have lacked sufficient power to detect such a difference, as cerebral infarctions are rare events, and the sub-group of migraineurs who had suffered a cerebral infarction was quite small (n = 4; Table 3). Interestingly, both of the two respondents with Chiari malformations suffered from headache (Table 4), one from migraine and one from unclassified headache.
Even though we did not find increased odds of major abnormalities among headache sufferers, there is no doubt that major intracranial abnormalities (e.g. neoplasms) can cause headache. However, having a headache does not in itself seem to be a strong predictor for such abnormalities in the general population.
Minor abnormalities
The present study found that the rates of minor abnormalities among headache sufferers were lower (17%) than those reported in earlier studies. Tsushima and Endo (18) identified minor abnormalities in 44% of headache sufferers, and Jordan et al. (35) identified such abnormalities among 49%. The latter study included extracranial abnormalities (Tsushima and Endo did not describe if they included such abnormalities), and the presence of sinus disease in 21% of this sample may explain some of the differences between our results and their own.
We also found that 3.6% of headache-free individuals and 4.2% of headache sufferers had arachnoid cysts, a higher prevalence than reported by two previous studies (1.4% (33) and 0.5% (32)). We note that there was no difference in the prevalence of arachnoid cysts >20 mm among headache sufferers and non-sufferers (both 1.6%); therefore, large cysts did not seem to cause headache in our population. Regarding the presence of other types of cysts, Peres et al. suggested that abnormal melatonin secretion from pineal cysts may cause headache (5,6), and a case-control study by Seifert et al. found an association between pineal cysts and migraine (7). Since only one respondent in our study had a pineal cyst, the statistical relationship with headache could not be investigated in a meaningful manner. However, we note that the respondent did not report any headache in the HUNT 3 study (data on file).
Headache sufferers had increased odds of minor intracranial abnormalities (Table 5). WMH were the minor abnormality that showed the largest difference in prevalence between headache sufferers and non-sufferers (Table 3). Thus, it may be that the increased odds of minor abnormalities are due to the presence of WMH. This is supported by the fact that the odds did not increase when respondents with WMH as the only finding were excluded from the analysis, but this could also be due to lack of power. If this association is true, it is in line with previous studies showing that WMH are more prevalent among individuals suffering from headache (12,36,37). However, earlier studies found the strongest association between minor intracranial abnormalities and migraine, while we found that only the TTH sub-group had increased odds of minor abnormalities. We note that earlier studies examined the presence of any abnormalities, while we included only those with Fazekas ≥1.
Strengths and limitations
The present study has several strengths. First, it is the only population-based study to examine the association between intracranial abnormalities on MRI and headache, and we were able to categorize sufferers into distinct groups based on validated primary headache diagnoses (26). Second, the participants were selected at random to minimize selection bias, and a comparison showed that the headache rate and the majority of demographic data recorded for participants in HUNT MRI were similar to those of non-invited and non-participants, except that the participants had fewer cardiovascular risk factors and a higher educational level (24). However, differences in terms of risk factors and, therefore, their potential effect on our estimates, were small.
The study does have some limitations. Headache status was measured using a questionnaire, which allows only one primary headache diagnosis per responder, and estimating headache using such a questionnaire is inferior to a clinical interview. However, the “any headache” criteria were validated and show fair sensitivity and specificity (26). While the migraine diagnosis was highly specific (95%), but had low sensitivity (51%), the opposite was true for TTH; however, repeating the analyses on the migraine groups using the more sensitive “probable migraine” criteria did not alter the results. One should bear in mind that the participants were selected randomly, and that the low prevalence of most intracranial abnormalities is reflected in our estimates. Such rare findings are not effectively evaluated in a population-based study design. The fact that the participants in the HUNT MRI had slightly fewer cardiovascular risk factors than the general population (24) may have led to a lower prevalence of infarctions and WMH.
Clinical implications and further research
This study provides a baseline estimate of the presence of intracranial abnormalities among headache sufferers and headache-free individuals drawn from the general population. The possible relationship between TTH and WMH warrants further research.
Conclusion
This population-based neuroimaging study showed that the prevalence of minor intracranial abnormalities was significantly higher among headache sufferers than among headache-free individuals. However, there was no significant association between headache and major abnormalities. Thus, neuroimaging of headache sufferers in the general population yields few findings of clinical importance.
Article highlights
In a random sample of the general population, 29% of headache sufferers and 22% of headache-free individuals had intracranial abnormalities. Headache sufferers did not have significantly more major abnormalities (e.g. tumors, aneurysms, and infarctions) than headache-free individuals; however, they had more minor abnormalities (e.g. cysts, white matter abnormalities, and calcifications). When comparing headache sub-groups with headache-free individuals, only the tension-type headache (TTH) group had more minor abnormalities. The increase in minor abnormalities was primarily related to the amount of white matter hyperintensities (WMH).
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgments
The Nord-Trøndelag Health Study (HUNT) is a collaboration between the HUNT Research Centre, the Faculty of Medicine at the Norwegian University of Science and Technology (NTNU), the Norwegian Institute of Public Health, and the Nord-Trøndelag County Council. The authors thank the staff at the Department of Medical Imaging, Levanger Hospital, and neuroradiologists Kjell Arne Kvistad and Jana Rydland.