
Abstract
Objective
The therapeutic response of a patient cannot purely be explained by the method of therapy or the efficacy of a drug. Clinician-patient interaction, psychosocial factors, patients’ expectations, hopes, beliefs and fears are all related to the healing outcome. Malleability and suggestibility are also important in the placebo or nocebo effect. The purpose of this study was to evaluate whether adding brief verbal suggestions for pain relief could change the magnitude of an analgesic’s efficacy.
Methods
This prospective study was performed in the emergency department of a university hospital. Patients who were ordered analgesia with diclofenac sodium for primary headache were divided into three groups. All groups were informed that they would be administered a pain killer by intramuscular injection. The second and third groups were given positive and reduced treatment expectations about the therapeutic efficacy, respectively. Patients were asked to rate their pain on a VAS at 0 and 45 minutes and if they needed any additional analgesic 45 minutes after the injection.
Results
A total of 153 patients were included in the study. The paired univariate analyses showed significant differences for all groups between 0- and 45-minute VAS scores. However, there was no difference between the three groups according to the differences in VAS scores between 45 and 0 minutes and according to the administration of an additional drug.
Conclusion
Simple verbal suggestions did not alter the efficacy of an analgesic agent for headache in an emergency setting. The contributions of suggestibility, desire and expectation in acute primary headache patients should be further investigated.
Introduction
Acute headache is a common condition and accounts for up to 4% of all emergency department (ED) visits (1). The primary task of an emergency physician is to relieve patients’ pain while determining which patients need further diagnostic work-up for serious or life-threatening conditions (2,3).
Most ED patients have benign primary headache syndromes that encompass all forms of migraine, tension-type, and cluster headaches. Approximately 3.8% have serious or secondary pathology (4). Nonsteroidal anti-inflammatory drugs (NSAIDs) are effective in the treatment of acute migraine or tension-type headache (5,6).
Most of the time patients and physicians’ expectation in the ED is to relieve severe pain with strong analgesics. Physicians often prefer to check for any signs of risk for complications and focus on the underlying diagnosis of painful complaints (7). This single-minded attention results in ignoring the pain that prompts the patient to seek care in the first place. ED patients have very high expectations for pain relief, much higher than those with postoperative pain do, and they expect pain relief as soon as possible after arrival (8,9).
The therapeutic response of a patient cannot purely be explained by the method of therapy or the efficacy of a drug. Clinician-patient interaction, psychosocial factors, patients’ expectations, hopes, beliefs and fears are all related to the healing outcome. Malleability and suggestibility are also important in the placebo or nocebo effect. Motivation, personality style, context, belief systems, fear and trust will influence the degree to which an individual edits, filters, or accepts influence and direction from another (10).
Most studies examine the analgesic effects of drugs compared with placebo. Though the placebo effect has long been a source of fascination and speculation, there are some promising claims that help us to understand its effects including Pavlovian conditioning, endogenous opioid release, cultural and social influences that provide meaning to interventions, cognitive variables such as expectancy, and a cluster of psychosocial variables (11,12).
The nocebo effect, which was introduced in 1961, should also be taken into consideration in clinical practice (13). The nocebo effect, or response, follows the administration of an inert substance (the nocebo, or negative placebo) along with the suggestion that the patient will get worse. However, the term nocebo-related effect will also be used to indicate symptom worsening following negative expectations but without the administration of any inert substance (14).
Previous studies concluded that an individual’s expectation of a drug’s effect and positive information about active medication influences the drug’s therapeutic efficacy. However, they suggest further research to investigate the application of their findings to clinical practice (15,16).
To optimize treatment outcomes, it is recommended that physicians integrate patients’ expectations into drug treatment regimens and provide information to patients about the active medication. So, we designed a clinical study to determine whether adding verbal suggestions for pain relief could change the magnitude of the analgesic efficacy of an NSAID for acute primary headache in the ED.
Methods
This prospective study was performed in the ED of a university hospital with an annual census of approximately 72,000 patients. Patients of all ages with any kind of trauma and patients over 15 years old were evaluated in the adult ED area. The study was approved by the institutional ethics committee.
The primary reasons of exclusion from the study.

NSAID: nonsteroidal anti-inflammatory drug; GI: gastrointestinal; PMH: past medical history; BP: blood pressure; HR: heart rate; RR: respiratory rate; temp.: temperature; VAS: visual analog scale; IM: intramuscular. aDiagnosis or suspicion of a secondary etiology of headache (according to the second version of the International Classification of Headache Disorders):
Headache attributed to head and/or neck trauma Headache attributed to cranial or cervical vascular disorder Headache attributed to non-vascular intracranial disorder Headache attributed to a substance or its withdrawal Headache attributed to infection Headache attributed to disorder of homeostasis Headache or facial pain attributed to disorder of cranium, neck, eyes, ears, nose, sinuses, teeth, mouth or other facial or cranial structures Headache attributed to psychiatric disorder
Patients were divided into three groups. Data were gathered in a total of 21 weeks. Patients were enrolled in the study Monday through Friday between 08.00 and midnight because two ED faculty physicians work together and evaluate all patients only during these hours of a week. Consecutive patients presented during the first seven-week period were assigned as Group 1. Patients in Groups 2 and 3 were the consecutive ones presented during the second and third seven-week periods, respectively.
All groups were informed that they would be administered a painkiller by intramuscular injection. Standard information was given by one of the nine ED faculty physicians after their evaluation to limit the number of physicians and to avoid the behavioral inexperience of the ED residents. All faculty physicians were also informed about the study design and educated on how to pronounce the standard sentences.
Group one patients were told that “A nurse is going to administer you a pain killer called Miyadren® by intramuscular injection.” The second and third groups were told the same sentence and additionally given positive and negative verbal suggestions to induce positive and negative treatment expectations about the therapeutic efficacy of the same drug, respectively. The patients in the second group were told “This drug is a powerful pain killer for your headache. Its analgesic effect peaks at about 20 to 30 minutes. We are expecting that your headache will resolve in 45 minutes.” The patients in the third group were told that “If your headache does not resolve in 45 minutes, we can administer you a more potent pain killer.”
Patients were asked to rate their pain on a 100-mm visual analog scale (VAS) at 0 and 45 minutes and if they needed any additional analgesics 45 minutes after the injection.
Data on demographic features were obtained. The primary intention-to-treat analysis included all enrolled patients for whom data were available.
Statistical analysis
The study data were analyzed in Medcalc 11.0.4 and SPSS 15.0 statistical software. The continuous variables were presented as mean ± standard deviation or median (if not normally distributed) with 95% confidence intervals (95% CI) and frequent variable as rates. The normality analysis was performed by Kolmogorov-Smirnov test. The comparison of the three groups for continuous variables were performed by one-way analysis of variance (ANOVA) for the normally distributed data and Kruskal-Wallis tests for the data distributed not normally and Chi-square test for the categorical data. And two group comparisons were performed by Wilcoxon test for paired samples. There was no similar study in the literature. So, when we calculate the sample size according to the findings of our study accepting the mean of the population as 70 and 22 for the standard deviation, the expected sample size is 45 for one group for 99% power. All the hypotheses were constructed as two tailed and an alpha critical value of 0.05 was accepted as significant.
Results
During the study hours of a 21-week period, a total of 972 patients presented to the ED with the primary complaint of headache. A total of 819 patients were excluded according to the exclusion criteria (Table 1) and 153 patients were included in the study.
Comparison of groups according to age, gender and the need for additional medication.

CI: confidence interval. aGroup 1 is significantly different from Group 2 and 3 in post-hoc analysis.
Comparison of VAS scores between 0 and 45 minutes among study groups.
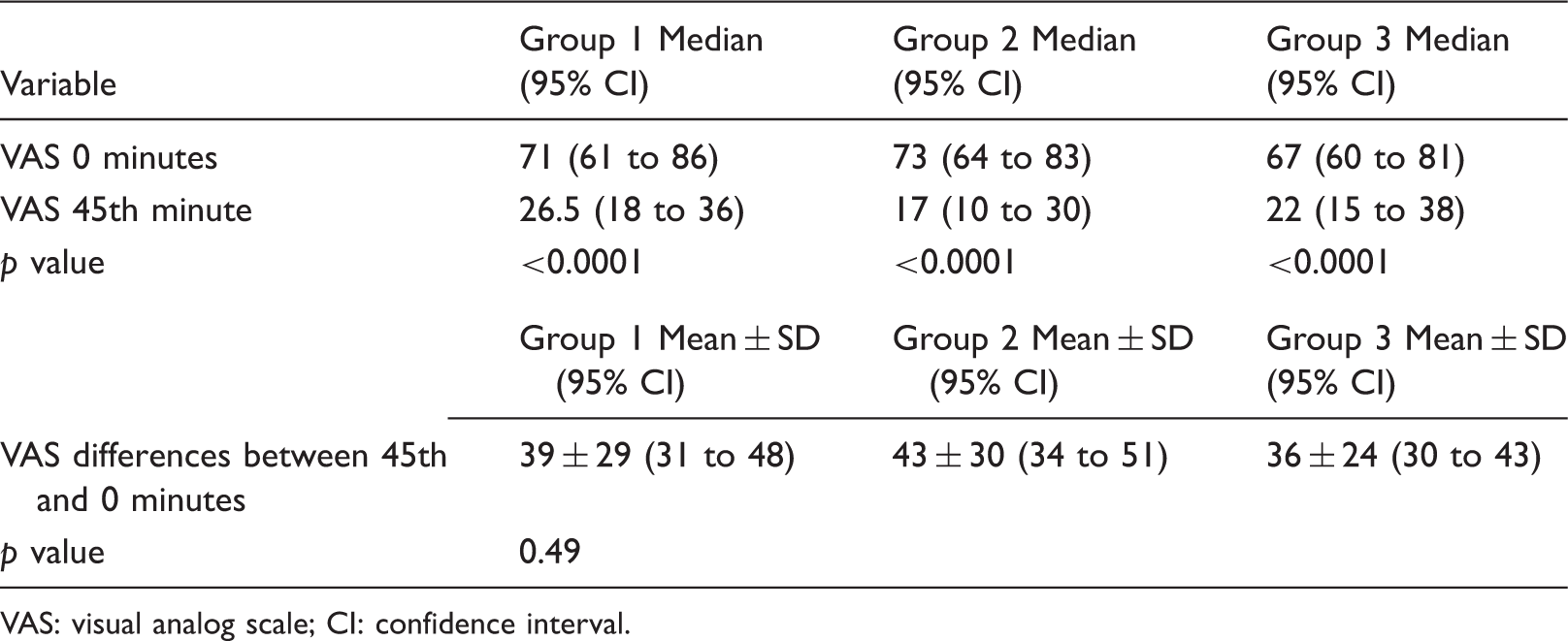
VAS: visual analog scale; CI: confidence interval.
Discussion
Pain management is one of the most important components in patient care. One of the essential objectives of evaluating a patient presenting to the ED with headache is to provide rapid, complete and sustained relief of pain for primary headache syndromes (6). Migraine and tension-type headaches account for almost all primary headaches in the EDs, since cluster headaches are generally rare and very short lived. There is not a clear consensus on the best therapy for migraine headaches, and to date no treatment has been shown to be superior in all respects (17). Dihydroergotamine, triptans, NSAIDs, and antiemetics such as metoclopramide or prochlorperazine are the preferred agents according to the institutional protocols (3,5,6,18). Acute attacks of tension-type headaches respond well to simple analgesics and NSAIDs (6). As NSAIDs are effective, inexpensive, commonly used, and very well tolerated in limited doses, we preferred to use diclofenac sodium for the treatment of primary headache.
Since treatment is given in the context of clinician-patient interaction, a patient who visits a physician with a complaint may start to feel better after receiving a diagnosis and being reassured that the condition will resolve on its own without any treatment. In addition to the power of the doctor to make the patient feel better, the informational context and associated patient expectations regarding treatment may influence the therapeutic efficacy of treatments (19).
In placebo-controlled studies, patients are informed that they are receiving either an active treatment or a disguised placebo or they are told they are to receive a powerful pain killer even though it is a placebo. It is shown that these different verbal instructions about certain and uncertain expectations of analgesia produce different analgesic effects, which in turn trigger a dramatic change of behavior leading to a significant reduction of opioid intake (15,20).
In our study we told all patients that they would receive an analgesic to relieve their pain. We obtained significant pain relief at the 45th minute after the intramuscular injection of diclofenac sodium. However, for the second group we tried to suggest to patients that their pain would be completely relieved in 45 minutes as this expectation would contribute as a placebo effect. The third group was told that more analgesics would be administered if effective pain relief could not be achieved, as this verbal suggestion was expected to induce a reduced treatment expectation.
Although Kam-Hansen and colleagues investigated how variations in medication labeling modified placebo and drug effects in patients with episodic migraine attacks and concluded that positive information about active medication contributed to successful treatment of episodic migraine (16), this the first study of its kind investigating the effect of different verbal suggestions on the analgesic efficacy of diclofenac in patients with a primary headache disorder presenting to the ED.
Suggestions to patients may have either psychological or physiological effects like placebo, which has been proven to cause endogenous opioid release since the opiate antagonist naloxone is capable of reversing placebo analgesia (21,22). As verbal suggestion for pain relief was suggested to increase the magnitude of placebo analgesia, suggestions may also have an important role on nocebo effect (23).
Expectations of analgesia also lead to a significant placebo analgesic effect (24). Additionally, all unconscious conditioning may play a role in patients’ response to pain medicine. A Pavlovian conditioning model could be valid if the patient receives analgesics over and over (25,26).
Benedetti analyzed the effects of opposing verbal suggestions on experimental ischemic arm pain in healthy volunteers and on motor performance in Parkinsonian patients and found that verbally induced expectations of analgesia/hyperalgesia and motor improvement or worsening antagonized completely the effects of a conditioning procedure. They also measured the effects of opposing verbal suggestions on hormonal secretion and found that verbally induced expectations of increase/decrease of growth hormone and cortisol did not have any effect on the secretion of these hormones. They found that verbally induced expectations have no effect on hormonal secretion, whereas they affect pain and motor performance (27). This study demonstrates that conscious expectations and unconscious conditioning are involved in different circumstances and that this is true not only for placebos but for nocebos as well.
Bingel and colleagues also investigated how divergent expectancies alter the analgesic efficacy of an opioid in healthy volunteers by using brain imaging. They assessed the effect of a fixed concentration of remifentanil on constant heat pain. They contended that an individual’s expectation of a drug’s effect critically influences its therapeutic efficacy and that regulatory brain mechanisms differ as a function of expectancy (15).
On the other hand, we hypothesized that verbal instruction about the effect of a drug could change its efficacy as creating a suggestion. We did not administer an inert agent as a placebo or nocebo drug. We extrapolated that patients could be influenced by the explanation of the effect of the analgesic agent; however, no statistically significant changes occurred.
Excluding almost 85% of patients presenting with headache could be interpreted as a limitation of the study; however, the main reason was that we desired to include patients with primary headache syndromes. In ED practice, it is not always possible to use International Headache Society Criteria (IHSC) to make the definitive diagnosis of the headache. Besides, ED physicians mostly consider selecting patients for emergency investigation and treatment of suspected critical secondary headache causes and providing effective treatment for primary headache syndromes. It was also declared that only 46% of patients with a prior migraine diagnosis and/or final emergency discharge diagnosis of acute migraine met IHSC (28). Although a detailed structured interview in the ED and adherence to the IHSC resulted in reproducible classification of headache patients, more than one-third of acute headache patients could not readily be given a specific diagnosis in the ED (29). There were concerns about the utility of the IHSC for future ED research, and modification of IHSC should be considered (28).
Another limitation of our study is the time of asking the need for additional medication 45 minutes after diclofenac treatment. Although the peak plasma concentration of 2.15 micrograms/ml was determined to be achieved in 20–30 minutes, analgesic efficacy may differ clinically (30). It might be possible to achieve significant differences, if different end points such as two or four hours were used. However, it is generally difficult to monitor patients for longer periods in an overcrowded ED.
Conclusions
Contrary to our hypothesis, simple verbal suggestions before administering an analgesic agent did not alter its efficacy for primary headache in an emergency setting. The contributions of suggestibility, desire and expectation in acute primary headache patients should be further investigated.
Clinical implications
The therapeutic response of a patient cannot purely be explained by the method of therapy or the efficacy of a drug. During clinical practice many physicians give suggestions to patients as to expecting better outcomes, especially for pain relief. Simple verbal suggestions before administering an analgesic agent did not alter its efficacy for primary headache in an emergency setting.
Footnotes
Funding
This study was supported by the Akdeniz University Scientific Research Project Unit.
Conflict of interest
None declared.