
Abstract
Background
Sturge-Weber syndrome (SWS) is an uncommon etiology of hemiplegic migraine-like (HM-like) attacks, associated with epilepsy and mental retardation.
Case
We report the case of a 40-year-old woman with SWS who has been suffering from HM-like episodes since she was 24, with no history of seizure or mental retardation. Susceptibility weighted imaging (SWI)-MRI and CT scans have shown bilateral calcifications of the choroidal plexuses, a developmental venous anomaly with dilated transmedullary veins and a left parieto-occipital leptomeningeal angioma. 18F-Fluorodeoxyglucose (FDG)-PET/CT revealed a diffuse left-hemisphere hypometabolism. The comparison between the MRI performed at the age of 24 and the one performed at the age of 40 highlighted a progressive unilateral fronto-temporo-parietal atrophy. Surprisingly, even now, cognitive functions of this patient are relatively preserved. Lamotrigine permitted an improvement of HM-like attacks.
Discussion
Explanations for this minimally symptomatic form of SWS may be the absence of seizure, the importance of her deep venous drainage, the absence of cortical calcification and white matter impairment in the affected hemisphere, and, paradoxically, the severely asymmetric cortical metabolism. Furthermore, this case reinforces the hypothesis that alteration of cerebral hemodynamics could precipitate the cortical spreading depression giving rise to migraine with aura.
Conclusion
We propose to consider SWS as a cause of apparently isolated hemiplegic migraine and lamotrigine as a preventive medication in HM-like attacks.
Introduction
Sturge-Weber syndrome (SWS) is a sporadic neurocutaneous disorder involving facial, choroidal and leptomeningeal angioma. Port-wine stain typically affects the first branch of trigeminal nerve and a choroidal angioma could be responsible for congenital glaucoma. The neurological complications of the vascular malformation are seizures, mental retardation and hemiparesis, with varying degrees of severity, and usually occur in early childhood. Three types of SWS are described: type I – facial and leptomeningeal angioma associated with possible glaucoma; type II – facial angioma; and type III – exclusive endocranial involvement.
Here we report an unusual case of SWS to illustrate the possible responsibility of leptomeningeal angioma in (i) migraine-like attacks with hemiplegia, (ii) chronic cortical hypometabolism and (iii) progressive cerebral atrophy with associated neurocognitive impairment. Imaging assessment and therapeutic aspects are also discussed.
The patient’s explicit consent was obtained before publication.
Case report
A 40-year-old, right-handed woman with no mental retardation, had presented a history of right hemiparesis during pregnancy at the age of 24. She had a typical bilateral port-wine stain on the forehead, also involving the left chest and the left hand. At the end of her pregnancy, she suffered from a severe attack with serious disturbance of consciousness requiring intubation. The MRI showed T2-weighted hyperintensities in the left pons and ruled out phlebothrombosis. Furthermore, there were no signs of meningitis on cerebrospinal fluid analysis. Finally, no diagnosis was reached and the neurological examination of the patient after this episode was normal.
During the next 16 years, once or twice a month, she suffered from episodes which began with right arm paresthesia, facial paralysis and dysarthria, appearing progressively over 5 minutes. After 30 minutes, aphasia and right hemiparesis appeared, along with severe throbbing headaches, photophonophobia and nausea. There was no visual aura. Symptoms, which prohibited daily activities, lasted from 2 days to 1 week and were completely reversible. Attacks were more frequent during menstruation. Neurological examination during paroxysmal events confirmed right hemiparesis including facial paralysis, expressive aphasia with paraphrasia, psychomotor slowness and no sensitive impairment. The aphasia was the last symptom to improve.
No migraine with aura in the patient’s family was reported, although her mother suffered from migraines without aura. No mutation was found after exonic sequencing of CACNA1A gene and complete sequencing of ATP1A2 gene, which are involved in familial hemiplegic migraine (FHM1 and FHM2).
Electroencephalographies recorded during an attack showed diffuse slow delta waves of the left hemisphere with no paroxysmal abnormality. MRI, including diffusion sequences, did not show any sign of recent infarct. Nevertheless, susceptibility weighted imaging (SWI)-MRI and angiotomography studies (undertaken when she was 40) showed bilateral calcifications of the choroid plexuses, a developmental venous abnormality with dilated transmedullary veins and a left parieto-occipital leptomeningeal angioma (Figure 1 (c–f)). An ipsilateral fronto-temporo-parietal atrophy was observed, which was not detectable on MRI 16 years before (Figure 1 (a,b)). Interictal 18F-Fluorodeoxyglucose (FDG)-PET/CT showed left thalamic, striatal and cortical hypometabolism (Figure 2). Finally, we diagnosed hemiplegic migraine-like (HM-like) attacks, symptomatic of Sturge-Weber syndrome.
Comparison of T2-weighted MRI at 40 years old (a) and 24 years old (b), showing progressive cortical atrophy. Tomography after injection (c) revealing leptomeningeal and choroidal plexus enhancement. CT-angiography (d) and SWI-MRI (e and f) showing a developmental venous anomaly with dilated transmedullary veins and a left parieto-occipital leptomeningeal angioma. Inter-ictal 18F-FDG-PET/CT showing left striatal, thalamic and hemicortical hypometabolism (Discovery ST, 30 minutes after injection of 121 Mbq of fluorodeoxyglucose).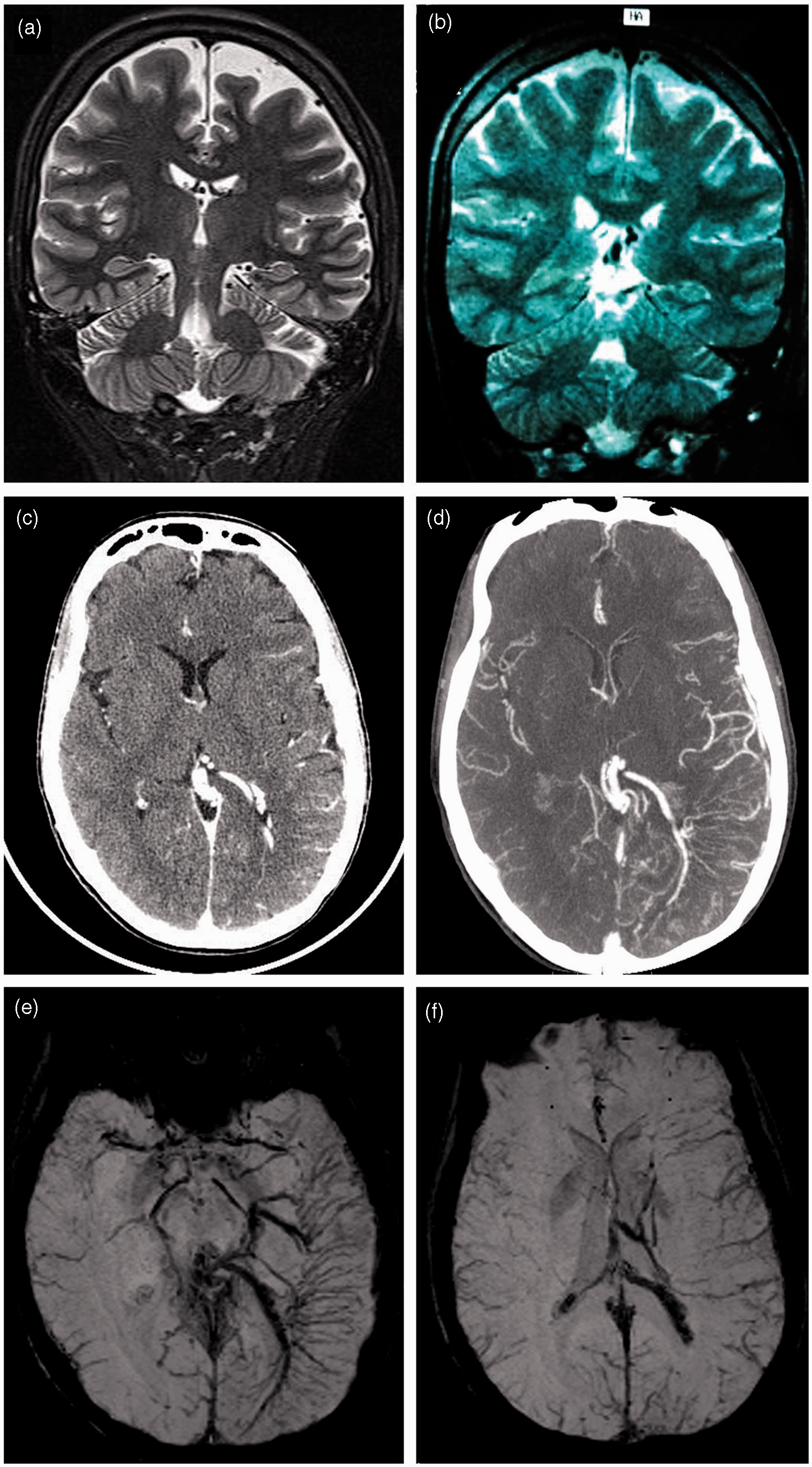

Although she presented no mental retardation (with a good educational level: French baccalaureat) and was employed in a socio-professional role commensurate with her qualifications, the patient complained of progressive memory and language loss. Assessment of cognitive functions showed predominantly attention impairment (more specifically in tense attention with reduced psychomotor activity and fatigability, D2 test), short-term memory, visual and verbal episodic memory impairment (Delayed Matching to Sample (DMS)-48 and French RI-48 test) and a moderate dysexecutive syndrome (in Rey Complex Figure Test and calculation but neither in Stroop color-word test nor in D-KEFS). Language was slightly impaired (LEXIS naming test). Implicit language understanding was affected by short-term memory impairment. These neuropsychological findings have remained stable over the past 2 years.
The patient was treated with lamotrigine (200 mg per day) for 2 years. Although she continued to suffer from one attack per month, the aura symptoms and headaches lasted no more than 5 hours. Prior to the administration of lamotrigine therapy these attacks had lasted from 24 hours to 7 days. The headaches were also less severe: recording 9/10 initially to 6–7/10 on the visual analog scale. Symptomatic treatments during attacks such as acetaminophen, ketoprofen or tramadol failed to improve headaches. Triptans have not been tested because of her severe and prolonged auras.
Discussion
We report here the first case of SWS with late onset (24 years old) HM-like attacks, without epilepsy and/or mental retardation. Diagnoses of SWS with late-onset epilepsy in the fifth or the sixth decade have been previously described (1,2). Some authors have presented the association between SWS and HM, but only for patients with mental retardation (3) and/or early (3,4) or late-onset (5) epilepsy. A case of SWS with a prolonged attack of hemiplegia during pregnancy has also been reported, but with authentic seizures (6).
Our patient presents all the International Classification of Headaches Disorders III (ICHD III) criteria for hemiplegic migraine except for the duration of her motor weakness (more than 72 hours) and the presence of a vascular lesion. Therefore, we prefer to use the terminology ‘hemiplegic migraine-like attacks’. We hypothesize that vasomotor disturbances within and around the angioma are responsible for oligemia, which could trigger left hemisphere cortical spreading depression (CSD), explaining the right hemibody symptoms. The fact that aura symptoms have always been located on the same side strongly supports this view. CSD was indirectly demonstrated by slow waves on EEG, and oligemia by hypometabolism on 18F-FDG-PET/CT. Finally, SWS must be considered as an etiology of hemiplegic migraine-like attacks (or ‘symptomatic’ hemiplegic migraine) as meningioma, meningitis, encephalitis, some metabolic disorders and arteriovenous malformations (7,8).
Sporadic or familial hemiplegic migraine can include severe attacks (coma and encephalopathy) frequently in the first years of the disease (7). The episode during the patient’s pregnancy may have been one of these severe attacks or a mere consequence of pronounced regional oligemia.
This case supports previous studies highlighting the usefulness of SWI-MRI in SWS (9,10). Indeed, it seems to be the best MRI sequence to identify prominent transmedullary veins. It is also the most accurate in identifying cortical calcifications usually associated with severe epilepsy and neuropsychological complication in SWS patients (11).
As a result of the chronic hypometabolism demonstrated in 18F-FDG-PET/CT, a progressive cortical atrophy developed in the leptomeningeal angioma region, as previously observed (10,11). This case report tends to suggest that slow atrophy (even with severe hypometabolism on PET) is paradoxically correlated to a non-severe form of the disease (12,13). Several clinico-radiological data may explain our patient’s relatively preserved cognitive functions: (i) no seizure in her childhood, (ii) important deep venous drainage, allowing a small increase in pressure under the angiomatosis (10), (iii) no cortical calcification on SWI-MRI (9), (iv) no white matter impairment in the affected hemisphere on classical MRI sequences (10), (v) severely asymmetric cortical metabolism, known to facilitate effective interhemispheric reorganizational processes resulting in less cognitive impairment in children (13,14). As no cognitive evaluation was conducted at a younger age, it seems difficult to link with certainty her cognitive impairment to a neurodegenerative origin because of progressive atrophy or to a poor basic neurodevelopmental process. Her complaint of progressive memory and language loss, however, and the semiology of her cognitive impairment (corresponding to the topography of the atrophic regions) support the neurodegenerative hypothesis.
We report that lamotrigine appears to be a possible treatment for HM-like attacks in SWS as it is known to be efficient in sporadic HM and familial HM (7) and in epilepsy control in SWS (1).
Conclusion
Sturge-Weber syndrome should be considered in any case of hemiplegic migraine, as some classic features of SWS such as mental retardation, epilepsy or facial angioma (Sturge-Weber type 3) may be lacking (11,12). This case reinforces the hypothesis that alteration of cerebral hemodynamics could precipitate the CSD giving rise to migraine with aura, especially in a predisposed individual. Finally, lamotrigine might be an effective treatment in HM and HM-like attacks but further randomized studies are necessary.
Clinical implications
Sturge-Weber syndrome (SWS) is a cause of apparently isolated hemiplegic migraine-like attacks. Chronic hypometabolism can lead to progressive cerebral atrophy in SWS. SWI-MRI seems to be the best MRI sequence to identify prominent transmedullary veins in SWS. Lamotrigine allows hemiplegic crises improvement in SWS.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgements
The authors express their thanks to Drs Serge Akono, Joseph Nkodo and Cecile Charpy for proofreading the manuscript and Dr Emmanuel Chabert for performing MRI studies.