
Abstract
Background:
Migraine attacks exclusively felt in the face are very rare, the pain involving the territories supplied by the second and third branches of the trigeminal nerve.
Cases:
Two patients suffering from heminasal pain attacks accompanied with typical migrainous features and responsive to oral or intranasal triptans – but not to intranasal lidocaine or oxymetazoline. In one patient, the attacks could be precipitated upon slight touching on the tip of the nose, in the other attacks were preceded by the nasal sensation typically heralding sneezing.
Discussion:
Migraine pain mostly develops within the innervation territory of the first branch of the trigeminal nerve, which includes the nose. Therefore, episodes of unilateral nasal pain with migrainous features could be considered a migraine with unusual topography (nasal migraine). Painful nasal attacks occasionally preceded by stimulation of trigeminal afferents in the nose, could be conceived of as migraine-tic syndrome.
Introduction
Migraine headaches are usually felt in one hemicranium, with or without shifting sides; reports of bilateral pain are less frequent (1). At times, the pain may extend to the face, the neck, and even towards the arms (2–4). Extracranial spreading of migrainous pain has been attributed to a process of central sensitization that produces an enlargement of the original symptomatic area (4).
Appellations such as lower-half headache and facial migraine have been applied to pain attacks localized below the eye (5). Migraine attacks exclusively felt in the face are very rare; in such instances, the pain has been reported in the territories supplied by the second and third branches of the trigeminal nerve (6,7). Rarely, facial migraine attacks may start in or near the nose, and then spread to the cheek and ear.
There have not yet been any reports of fully developed migraine attacks with pain confined to one side of the nose throughout the time span of the attack. Here, we report two cases of patients suffering from frequent attacks of strictly heminasal pain with typical migrainous features that regularly responded to triptans, strongly suggesting a migraine with a particular topography, that is a nasal migraine.
Materials and methods
Patients
Patient 1 was a 65-year-old female who had suffered from migraines with and without visual aura, since the age of 30. The episodes were described as severe, involving pulsatile pain located in one or both frontotemporal regions, and regularly accompanied by photo- and phonophobia.
At the age of 57, she started experiencing painful attacks that were exclusively located in the nose. Nasal pain episodes always began in the left part of the tip of the nose (apex nasi), and spread over the left nasal pyramid (dorsum nasi) – up to the internal angle of the left orbit (Figure 1). The pain was moderate to severe in intensity and throbbing. Attacks were accompanied by hypersensitivity to inhaled air along the left nostril, and photo- and phonophobia. The patient denied other accompaniments such as nausea, vomiting, conjunctival injection, nasal obstruction or rhinorrhea. Each attack lasted 1–2 days, or less if effective treatment was provided. The frequency ranged from four to six episodes per month. Between episodes, she remained completely asymptomatic. Pain attacks could be precipitated by slight exteroceptive stimuli in the tip of the nose.
In patient 1, spontaneous or precipitated pain attacks started in the left part of the tip of the nose (shaded area). 117 × 116 mm (96 × 96 DPI).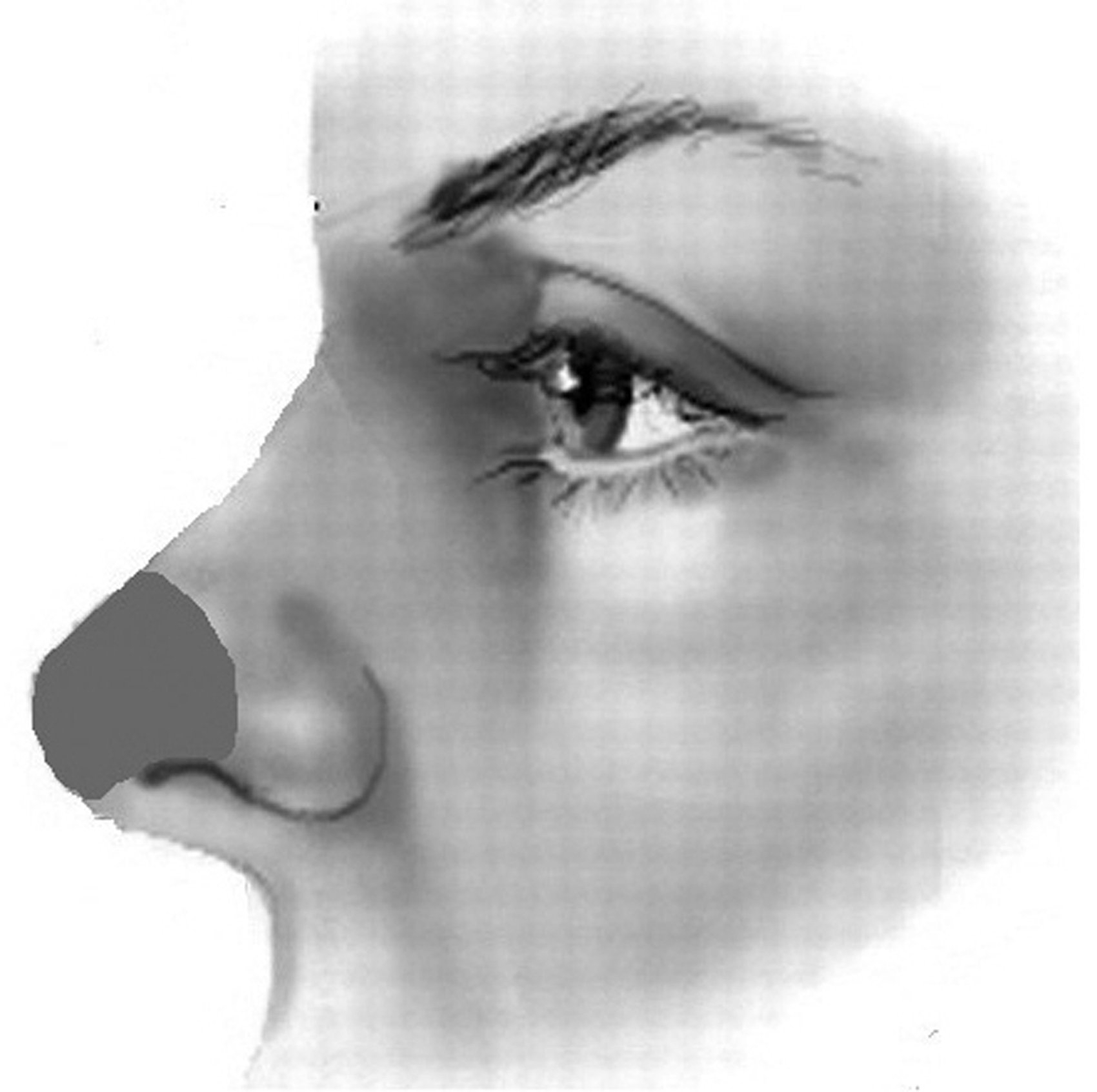
The episodes of nasal pain were refractory to conventional analgesics and non-steroidal anti-inflammatory drugs (NSAIDs), and to treatment with intranasal lidocaine or intranasal oxymetazoline. However, they were completely abated with oral rizatriptan or almotriptan, and with zolmitriptan instilled in either nostril.
Patient 2 was a 48-year-old male. Since the age of 25, he had suffered from severe throbbing headaches, generally preceded by a brief tingling sensation in the vestibulum nasi (Figure 2) that he recognized as the typical symptoms premonitory of sneezing. The pain lasted from several to 24 hours, and was frequently accompanied by photophobia, phonophobia and nausea. Other accompaniments such as conjunctival injection, lacrimation, nasal stuffiness or rhinorrhea were lacking. The episodes recurred weekly. In between attacks, the patient was completely free of symptoms. The patient noted that low quantities of alcohol could trigger the episodes, whereas rest and sleep were mitigative.
In patient 2, the attacks were generally preceded by the nasal sensation typically heralding sneezing (represented in the figure by a gradient of stars). 43 × 41 mm (96 × 96 DPI).
The pain was systematically aborted by zolmitriptan either intranasally or orally. Use of conventional analgesics and NSAIDs, as well as several attempts with intranasal lidocaine, oxymetazoline or fluticasone furoate had no benefit.
Diagnosis
Results of a complete neurological examination were normal in both patients, as were results of additional examinations performed by an ophthalmologist and an ENT surgeon, including nasal endoscopy. Specifically, palpation of the eyeball, trochlear area, and the emergence and trajectory of the supraorbital, infraorbital, supratrochlear, infratrochlear and auriculotemporal nerves was carried out and yielded normal results. Neck motion and results of palpation of both greater and lesser occipital nerves were also recorded as normal.
Routine blood tests (including erythrocyte sedimentation rate and immunological screening), and urine tests, chest X-rays, as well as brain and orbital/facial magnetic resonance image (MRI) examinations were also performed and rendered normal results. The scores of inventories of Beck Depression Inventory (BECK) and State-Trait AnxietyInventory (STAI) (feature and situation) were within normal ranges.
The clinical features, differential responses to systemic and intranasal therapies, and the generally negative outcome of the supplementary examinations ruled out a symptomatic headache – including post-traumatic nasal pain (8), and primary nasal disorders, such as rhinosinusitis (1), mucosal contact point headache (1,9), nasociliary neuralgia (1,10), persistent idiopathic facial pain (1) and idiopathic rhinalgia (11).
Comments
Our patients complained of recurrent episodes of heminasal pain, and results of physical and supplementary examinations were normal thus indicating they were suffering from a primary pain disorder. Additionally, many features were reminiscent of migraine – namely, unilaterality of the pain, duration and frequency of attacks, accompaniments, and response to triptans. Altogether, these features indicate that we may be facing a migraine with unusual heminasal topography.
Despite such precise localization, the process seems to be central in nature, as indicated by the ineffectiveness of intranasal treatments with vasoconstrictors and anesthetics. On the contrary, treatment with oral (and intranasal) triptans systematically provided rapid and complete relief. Efficacy of triptans via a possible vasoconstrictor action in the nasal mucosa is unlikely, as powerful topic vasoconstrictors (oxymetazoline) instilled in the symptomatic nostril failed to provide relief.
The ICHD-2 diagnostic criteria for a migraine (1) includes unilateral localization of the head pain without stating any particular topography of the symptomatic area. Although the nose anatomically belongs to the face, it can functionally be conceived of as part of the innervated territory of the ophthalmic division (V-1) of the trigeminal nerve. Accordingly, it is possible that our patients could suffer migraine attacks with pain felt within a facial area supplied by the V-1 nerve. Nevertheless, particular traits in each patient warrant further comments.
Patient 1 could trigger attacks by gently touching the tip of the nose. Such precipitating mechanism presumably activates nasal afferents of the trigeminal nerve, thus bringing to mind a trigeminal neuralgia, and a migraine-tic syndrome (12). Attacks of trigeminal neuralgia are triggereable, but they typically last for only a few seconds, lack autonomic features and are unresponsive to triptans. To date, only one case of migraine-tic syndrome has been reported (12); it included attacks presenting with the two components in a consecutive fashion: the neuralgic pain involving the cheek (second branch of the trigeminal nerve) followed by the migrainous pain developing in the ipsilateral hemicranium.
Patient 2 reported that most attacks were preceded by the nasal discomfort typically heralding sneezing. Although such a nasal sensation could originate in the peripheral territory of the trigeminal nerve, both the preceding symptoms and ensuing migraine attacks could also be central in nature. Sneezing is a complex reflex mediated by the trigeminal and facial nerves and brainstem respiratory centers. Such a reflex may be subject to supranuclear modulation.
Patient 2, suffered from nasal migraine attacks from the onset of symptoms. Conversely, patient 1 experienced a topographic change of her migraines from 57 years of age and onwards, with the typical cranial migraine attacks being replaced by exclusively nasal attacks. Such a topographic change is certainly enigmatic. Theoretically, a plastic change in the central somatotopy of the migrainous process could have occurred.
Migraine pain is mostly felt within the innervation territory of the V-1 nerve, which includes not only the forehead and orbit but also the nose. Therefore, episodes of unilateral nasal pain with migrainous features could be considered a migraine with unusual topography. Migraines are thought to be centrally driven. It is also possible that a migrainous dysfunction of the parietal lobe could produce alloesthesia with displacement of the perception away from the correct location to another site. Finally, precipitating mechanisms acting on trigeminal afferents in the nose invest the nasal migraine with a neuralgic tinge, which might be decisive in the determination of the topography.
Clinical implications
This is the first description of migraine attacks with pain exclusively felt in the nose. Novel precipitating mechanisms of migraine attacks with important pathophysiologic implications are described. Differential response to treatment given orally or intranasally is of paramount importance in the diagnostic work-up of primary nasal pain.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.