
Abstract

Genetic disorders characterized by migraine with or without aura as one of the major clinical feature (may be grouped as Migraine attributed to genetic disorder)
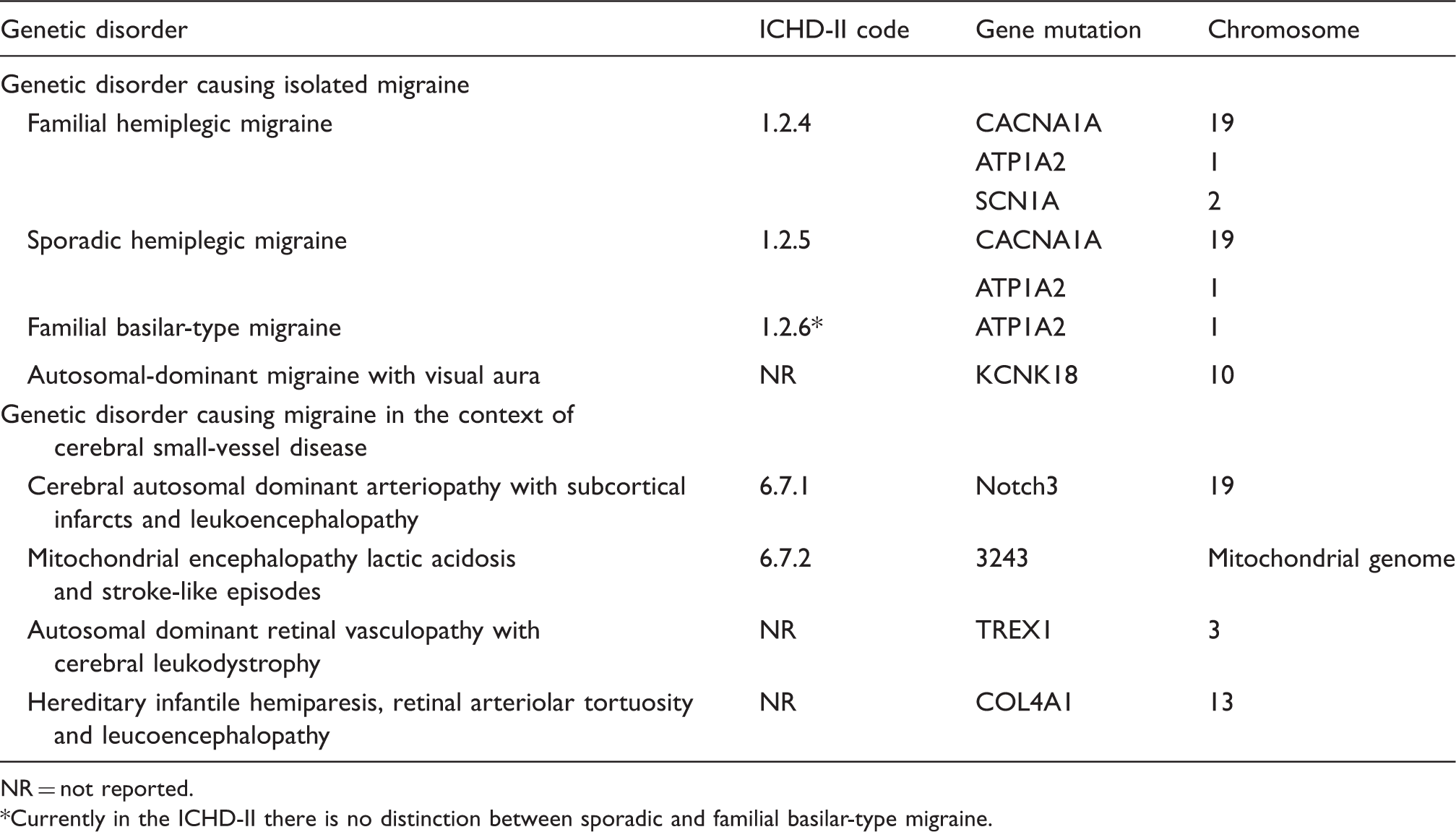
NR = not reported.
Currently in the ICHD-II there is no distinction between sporadic and familial basilar-type migraine.
FHM has been associated with mutation in the CACNA1A gene on chromosome 19, in the ATP1A2 gene on chromosome 1 or in the SCN1A on chromosome 2 (4). By contrast, SHM has been associated with mutations in the CACNA1A gene on chromosome 19 and in the ATP1A2 gene on chromosome 1 (5). Clinically, FHM and SHM are characterized by recurrent attacks of migraine with aura including motor weakness; in addition, for the diagnosis of FHM to be made, the patient must have at least one first- or second-degree relative affected by the same condition. FBM has been associated with mutation in the ATP1A2 gene on chromosome 1; it is a subtype of migraine with aura in which the aura symptoms originate from the brainstem or from both hemispheres simultaneously, and is also accompanied by dysarthria, vertigo, tinnitus, hypacusia, diplopia, simultaneous bilateral visual symptoms, ataxia, decreased level of consciousness and bilateral paresthesias (6). AD-MVA is due to a dominant-negative mutation in the KCNK18 gene on chromosome 10 (7). Clinically, AD-MVA is characterized by recurrent typical attacks of migraine with visual aura. CADASIL is due to a mutation of the Notch3 gene on chromosome 19. It is characterized by migraine with or without aura, mood disturbances, transient ischemic attacks (TIAs) or strokes (usually lacunar infarcts) and progressive cognitive decline; other, less common clinical features are epilepsy, acute reversible encephalopathy and myopathy (8). MELAS is due to a mutation at position 3243 of the mitochondrial genome (9). It is characterized by seizures, encephalopathy, stroke-like episodes, migraine mostly associated with vomiting and aura, short stature, cognitive impairment, depression, cardiomyopathy, cardiac conduction defects and diabetes mellitus. AD-RVCL is due to TREX1 mutation on chromosome 3 and is characterized by systemic microvasculopathy with adult-onset retinal vasculopathy and cerebrovascular disease variably associated with migraine, mainly without aura (10). HIHRATL is due to a mutation in the COL4A1 gene on chromosome 13 (11); the disease has some similarities with CADASIL and is characterized by features of cerebral small-vessel disease, including subcortical hemorrhagic and ischemic lacunar strokes and leukoaraiosis. Patients usually suffer also from migraine mostly with aura, seizures, infantile hemiparesis, developmental delay, neuropsychological abnormalities, and ocular, renal and cardiac involvement.
In the ICHD, second edition, FHM, SHM and FBM are coded among the primary headaches (code 1.2.4, 1.2.5 and 1.2.6, respectively); headache in patients with CADASIL and MELAS is coded among the headaches attributed to cranial or cervical vascular disorder (code 6.7.1 and code 6.7.2, respectively); while AD-MVA, AD-RVCL and HIHRATL are not currently included (12). Coding of headache in CADASIL and MELAS is based on the implicit assumption that a vascular disorder is the cause of the headache (8). In our opinion, this interpretation should be reconsidered. In fact, other diseases included in the same chapter are characterized by the presence of macroscopic alterations in brain parenchyma (e.g intracerebral hemorrhage), meninges (e.g. subarachnoid hemorrhage) or blood vessels (e.g. arterial dissection) detectable by currently available examinations (e.g. neuroimaging in most cases and biopsy in some vasculitides), or are closely related to a therapeutic procedure (carotid endarterectomy or angioplasty). In those circumstances, the headache is attributed to the anatomical damage of pain-sensitive brain structures. By contrast, in CADASIL the headache in most cases represents the first symptom of the disease, preceding from months to years the onset of stroke or of TIAs and brain lesions. Nevertheless, evidence supports that the primary pathogenic mechanism is represented by a genetic defect responsible for the functional alterations of the endothelial cells that may predispose to cerebral small-vessel disease and are able to induce migraine. As a result, the primary pathogenic mechanism of the disease seems to be genetic rather than vascular. Moreover, in patients with CADASIL, the headache has features overlapping those of migraine rather than general features of any secondary headache (8). The same remarks referring to the headache in patients with CADASIL may apply to the headache in patients with MELAS, AD-RVCL and HIHRATL.
Some genetic defects causing migraine as an isolated disease (e.g. FHM, SHM, FBM and AD-MVA) or in the context of a cerebral small-vessel involvement were identified and consequently, migraine may be considered either as a primary idiopathic or a primary genetic disease. The inclusion of the new category of migraine attributed to genetic disorder may improve accuracy in the classification of primary headache, assembling together diseases that share as major common features clinical characteristics of the headache attacks matching those of idiopathic migraine and a well-defined genetic alteration.