
Abstract
SUNCT syndrome (short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing) is a primary headache characterised by a high frequency of attacks associated with marked autonomic periocular signs and symptoms. Activation of the hypothalamus via the superior salivary nucleus is probably responsible for some of the autonomic involvement observed during SUNCT attacks. We describe a case of SUNCT with unusual autonomic features (e.g., mydriasis) and early onset. Pupillometric studies were performed both in a basal condition (without anisocoria) and after instillation of phenylephrine (a drug with direct sympathomimetic activity) and pilocarpine (a parasympathetic agonist).
The findings in this patient seem to indicate involvement of the ocular sympathetic supply in SUNCT, responsible for the mydriasis, and seem to strengthen the possibility that the autonomic phenomena in this syndrome vary with different levels of pain severity.
Introduction
SUNCT syndrome (short-lasting unilateral neuralgiform headache attacks with conjunctival injection, tearing, sweating and rhinorrhoea) was first described by Sjaastad et al. in 1978 (1). Attacks of SUNCT, in which pain intensity is invariably greatest in the ocular/periocular area, are accompanied by marked unilateral autonomic activation and occur with a frequency of between three and 200 per day (1–3). Conjunctival injection and lacrimation are the most prominent autonomic features. Miosis on the symptomatic side has been described during pain but pupillometry has failed to show changes in pupil diameter (1,2,4), at least in the basal condition. Other associated cranial autonomic signs and symptoms may be present on the headache side: nasal blockage, rhinorrhoea, eyelid oedema, ptosis, hyperventilation, sweating or facial and ear flushing. Cohen et al. (5) mentioned one case of ipsilateral mydriasis, but gave no details.
Case report
A 22-year-old woman came to our observation with a one-year history of headache, but no family history of the disease. The clinical features of her headache suggested a diagnosis of SUNCT, and she indeed fulfilled the International Headache Society (IHS) diagnostic criteria (3), reporting short-lasting (3–5 minutes), left-sided attacks with ocular/periocular localisation of pain, occurring at a rate of 3–15/day and fluctuating in severity. In addition, she reported periodic mild background pain. The autonomic component of the attacks consisted of pronounced ipsilateral tearing and conjunctival injection. In addition, from the onset of the condition, the patient had also experienced concomitant (for the entire duration of the pain) transient pupillary dilation during severe/moderate attacks on the symptomatic side. Over the two months leading up to our observation, the headache had shown a pattern of 2–3 severe attacks/day accompanied by autonomic signs and symptoms and 10–20 mild-to-moderate attacks/day; with both types of attack there was clear-cut paroxysmal mydriasis, conjunctival injection and tearing on the symptomatic side (Figure 1).
Anisocoria with mydriasis on the symptomatic (left) side.
One month before the patient came to our observation, she had also started experiencing, occasionally, short-lasting (1–5 minutes) episodes of scotoma coinciding with severe pain attacks and paroxysmal mydriasis. These episodes were described as the appearance of a grey spot in the centre of the field of vision, followed by luminous zigzag lines. The patient reported no photophobia, phonophobia or nausea.
The neurological examination was normal, as were the results of a series of other examinations: echographic Doppler ultrasound of the supra-aortic vessels, transcranial ultrasound, visual evoked potentials (VEPs), magnetic resonance imaging (MRI) and angio-MRI of the brain.
The indomethacin test (100 mg IM)(6), administered twice interictally, had no effect on attacks or on autonomic signs/symptoms.
The patient had previously used nimesulide to treat the pain, but without benefit. After an ophthalmological examination, she was put on 0.3% tobramycin (eyedrops) three times a day and ketorolac 10 mg on demand for five days; this regime led to the disappearance of the transient scotomas. The patient was prescribed topiramate (150 mg/day) and obtained a significant reduction in the number both of severe attacks and of episodes with paroxysmal mydriasis. After six months, topiramate was reduced to 100 mg/day because of weight loss (13 kg), hair loss and the progressive appearance of other side effects (a sense of ‘shaking objects’ in the symptomatic eye, mental slowing, dysphasia). After a year, topiramate was withdrawn and replaced with lamotrigine 100 mg/day. On this dosage, the patient had 1–2 short-lasting attacks/week associated with mild autonomic signs and symptoms. From November 2008, because of daytime somnolence and difficulty concentrating, oxcarbazepine 900 mg/day was introduced, while the lamotrigine was reduced to 75 mg/day. According to the headache diary kept by the patient, this modification of her therapy led to a reduction in the frequency and duration of the attacks.
A pupillary evaluation was carried out to compare the response to sympathomimetic and parasympathomimetic agents.
Pupillary studies
In evaluating this patient, we used a 5.0 megapixel Sony digital camera to estimate mean pupillary diameters (vertical and horizontal). The measurements were taken both in the basal state and after topical stimulation with a sympathomimetic agent (phenylephrine [1%]), an agonist which acts directly on postsynaptic receptors in the dilatator muscle of the iris, and with a parasympathomimetic agent (pilocarpine [2%]). Pupillary dilation was measured at set intervals, comparing the responses of the symptomatic (S) and non-symptomatic (NS) sides. The anisocoria index (100* symptomatic side/symptomatic side + non-symptomatic side) was used for these calculations (7). It would also be interesting to study the response to alpha- and beta-blocking agents and indirectly acting sympathomimetic agents (hydroxyamphetamine, cocaine, tyramine), but these were not available in our setting. Absolute values in millimetres were not used for the calculation due to the relatively low resolution of the camera. The anisocoria index gives results that reflect more closely the clinical situation (Figure 2).
Pupillary measurements in SUNCT. Anisocoria index (AI): 100*(symptomatic side/symptomatic side + non-symptomatic side).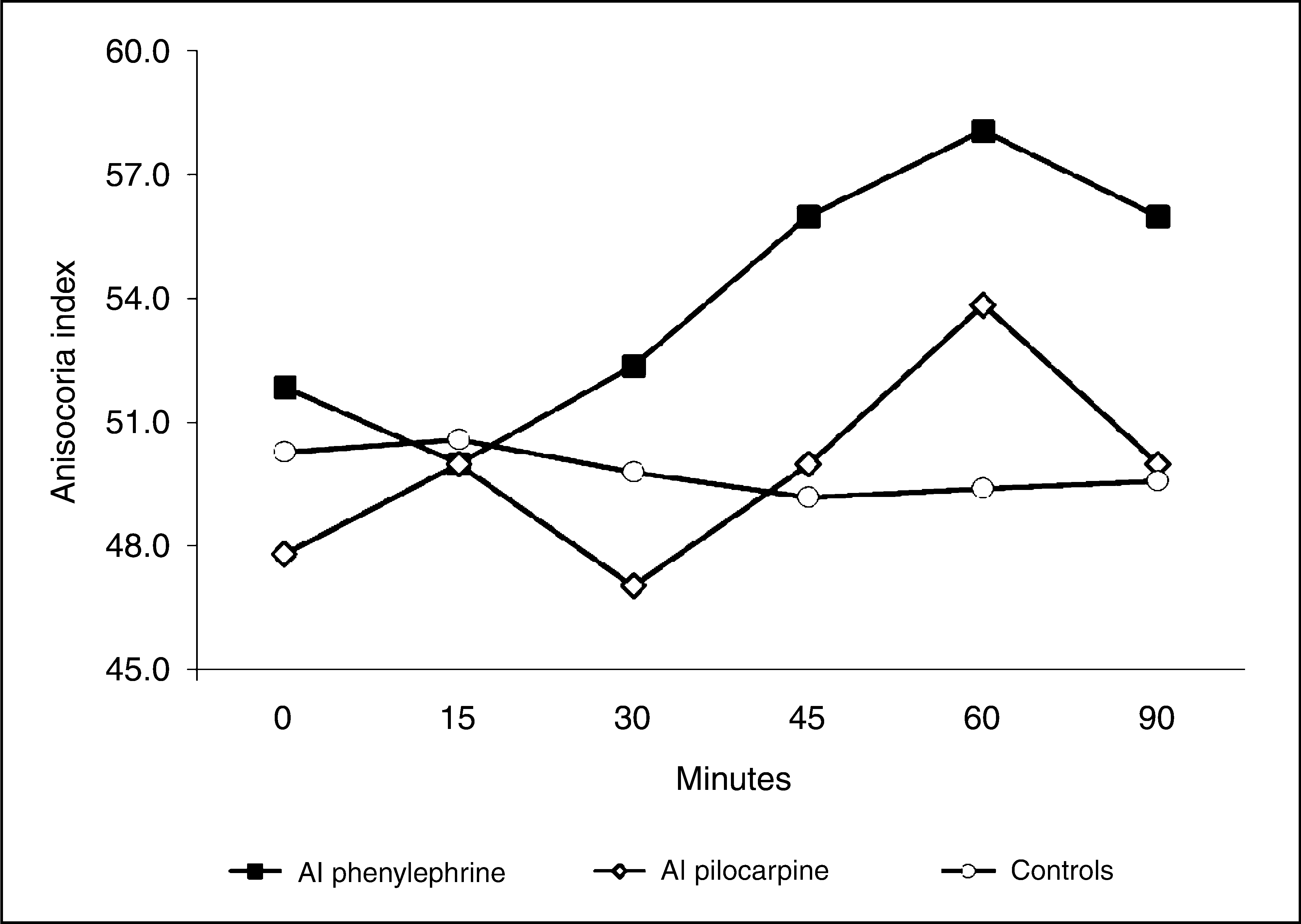
Pupillary measurements after phenylephrine and pilocarpine instillation a

The patient was drug-free at the time of the test. AI (anisocoria index): 100*(symptomatic side/symptomatic + non-symptomatic side).
Discussion
Sophisticated neuroimaging provides evidence that the posterior hypothalamus is involved in the pathophysiology of SUNCT, as is also suggested by the finding that it shares clinical characteristics with other headaches such as cluster headache (CH) and chronic paroxysmal hemicrania (CPH) (8); this hypothesis is further supported by evidence from functional imaging and deep brain stimulation studies (9). It has also been suggested that the pathophysiology of SUNCT, CH and CPH revolves around activation of the trigeminal-autonomic reflex (8), which consists of a brainstem connection between the trigeminal nerve and facial (VII cranial nerve) parasympathetic outflow. Benjamin et al. (10) have suggested that the prominent cranial autonomic symptoms that we encounter in these syndromes may be due to a central disinhibition of the trigeminal-autonomic reflex by the hypothalamus. Experimental data in rats show the existence of direct hypothalamic-trigeminal connections (11) and corroborate the idea that the hypothalamus exerts a modulatory role on nociceptive and autonomic pathways, specifically the trigeminovascular nociceptive pathway (12). The autonomic picture may be more complicated in SUNCT, whose impressive set of local autonomic signs (conjunctival injection, lacrimation, rhinorrhoea) are probably due to additional recruitment of the parasympathetic system.
The pupillometric findings described in this case of SUNCT seem to indicate involvement of the ocular sympathetic supply, possibly responsible for the mydriasis, and to strengthen the possibility that the autonomic phenomena in this syndrome may vary according to different levels of pain severity. It might be suggested that the key feature of trigeminal autonomic syndromes such as SUNCT is the severity of their expression and not the presence per se of autonomic dysfunction (13). Fanciullacci et al. (14,15) demonstrated impaired pupillary sympathetic responses in CH patients between attacks, within cluster periods. A comparison of CH patients with a relatively large control series showed that the pupil on the symptomatic side frequently, though not always, has a Horner-like appearance in CH (7,16). In the presence of unilateral lesions of the postganglionic sympathetic nerve fibres to the pupil, the affected pupil will, upon direct sympathetic stimulation, dilate more because of denervation hypersensitivity. Fanciullacci et al. (17) suggested that adrenergic transmission may be disrupted in headache sufferers generally, hypothesising a deficiency of noradrenaline in the iris adrenergic nerve terminals. The third neuron also exhibited reduced capacity of neurotransmitter synthesis and adrenoceptor hypersensitivity (17).
The results we obtained in this case with the available pupillary tests are consistent with sympathomimetic stimulation during the attack; however, there was a difference in response between the two eyes. If the origin of the stimulus is ‘central’, this could be due to a difference in stimulation magnitude.
However, the underlying mechanism is, in all probability, much more complex than simple stimulation of the parasympathetic or sympathetic nervous system suggest.
This issue aside, this patient nevertheless appears to be a genuine case of SUNCT with additional clinical features: paroxysmal mydriasis and transient scotoma episodes. Parasympathetic block and/or sympathetic stimulation, when separately used, produce a mydriatic response and might result in the clinical expression of a mydriatic eye. Our data in this SUNCT patient seem to raise more problems than they solve; in CH, on the other hand, the pupillary reaction is more consistent and easier to interpret (16).
Footnotes
Acknowledgements
This work was supported by Italian Ministry of Public Health grant 2007/RC.