
Abstract
By the time of his death in September 1921, Peter Johnstone Freyer was an extremely wealthy man. After an education at Queen's College Galway, his medical career had been defined by colonial service in India, and the establishment of a successful surgery and consultancy on London's Harley Street. In public, these hallmarks of his career led to him being described by his contemporaries as amongst medicine's most prominent figures, and as a ‘great surgeon’ by newspapers the length of and breadth of the United Kingdom on the occasion of his death. However, his private papers show that his medical practice was only responsible for a small part of his material success; two-thirds of his wealth was derived from his skill, exercised in private, as an investor in financial markets. By establishing his history as an investor, and comparing it to his public profile in medicine, this article traces the social and cultural histories of professional identity in late-Victorian and Edwardian London. Over the course of its arc, it demonstrates how medicine's public significance in this period was part of a broader, middle-class, professional culture concerned with the accrual of ‘virtual’ wealth, the construction of advantageous social networks, and the tapping of capital in multiple forms. In sum, Freyer's career reflects the symbolic meaning of publicly wielding a scalpel, whilst privately managing a portfolio of financial ledgers.
Keywords
Introduction
When Harold Perkin detected the rise of ‘professional society’ in late-Victorian Britain, he described a public phenomenon, in which professional expertise was part of a political economy that produced new, technocratic forms of public administration. At the same time, professions and their work symbolised bourgeois Victorian ideals concerning civic duty and patriotic public service. 1 Andrew Abbott's theory of professions as expert groups competing over an ecosystem of ‘jurisdictions’ rested on tracing conflicts between professional groups through the public realms of the law, the media and the legislature. 2 Eliot Freidson suggested that professions operate according to their own internal dynamics, beyond capitalistic logic, and the bureaucratic logic of the state. This ‘third logic’ amounted to a monopoly and supported the extension of professional power over discrete fields of expertise in the name of public service. 3
These sorts of arguments make sense. It would be absurd to claim that professional power is not rooted in its public value and performance: professionals are trained at universities, provide services to the public of various sorts, and lay claim to their status by way of appealing to citizenries and the state. 4 What we wish to emphasise here is that less attention has been paid to the forms of expertise that a professional can become proficient in, away from their public identity and practice. These cultivations of expertise in private extend what we can know about the nature of professional fields and their relations to other strands of social and economic history. Our focus here is a case study of Peter Johnstone Freyer (1851–1921), who, in late-Victorian and Edwardian Britain and its empire, was publicly a highly-successful surgeon, but in private was an equally successful financier. 5 Freyer's archive allows us to demonstrate how, when faced with uncertainty in public towards their established field of expertise, professionals can use that uncertainty to further their position in marketplaces for their services. Secondly, professionals respond to it by diversifying into other fields of expertise away from the marketplaces of their formal professions.
In one sense, Freyer was the realisation of professional success through the execution of medical expertise leveraged for economic gain. Especially in the second half of his career, he was a pre-eminent genitourinary surgeon who developed a skill for using a procedure to remove the hypertrophied prostate. The operation became known as Freyer's prostatectomy. 6 One might assume that his fortune at death (£130,000) resulted from accumulating substantial fees for access to his medical expertise. 7
However, this would make too strong a link between his financial success and his proficiency in medicine on the evidence of sources made for public consumption. In his private financial ledgers, we can see that the majority of his wealth came from an extensive portfolio of investments. 8 Shortly after his death, his solicitors estimated that £100,000 (77 per cent) of his wealth at death was accounted for by his investment portfolio. Without examining these private documents, the role finance played in structuring his career has remained hidden. 9 He does not seem to have been publicly associated with this second area of expertise. Why would so successful a medical man cultivate a separate field of expertise for obtaining wealth? Our contention here is that maintaining these two fields of expertise, one in public and the other in private, was an act of diversification taken to confront the conditions of his professional field in medicine. In short, Freyer's professional success became as attributable to his management of a financier's ledger, as it was to his wielding of a surgeon's scalpel.
Our argument proceeds over four core sections, the sections Profiting From Uncertainty: Genitourinary Medicine and Freyer's Making of a Medical Career examine the cultural and economic circumstances that defined Freyer's public standing in medicine. The article's subsequent two sections then complicate our analysis, by examining the content and origins of Freyer's financial investments, and demonstrate how diversifying into this field was a reaction to the uncertainties he faced in medicine. In particular, the Freyer as Investor section establishes Freyer's status as a risk-averse investor, and The Uncertainties of Colonial Employment – Tracing the Origins of Freyer's Financial Investments in his Colonial Service section argues for viewing the origins of his aversion to risk as a consequence of his experiences of professional service in India. The Scalpel and the Ledger – Freyer as Surgeon and Financier in London's Elite Society section then examines how Freyer's expertise in medicine and finance were related, particularly regarding how interactions between the two were shaped by the cultural values of Edwardian Britain's elite socio-economic hierarchies.
Profiting From Uncertainty: Genitourinary Medicine and Freyer's Making of a Medical Career
By the standards of his profession and social class, Sir Peter Freyer had won. On his death in 1921, he was one of the toasts of the medical profession, a position of esteem that he carved out through his professional specialty in genitourinary surgery. At his practice on Harley Street, he had received elite politicians, captains of industry and leading men of science, had been known personally to the late King Edward VII, and was knighted in 1917. 10 Furthermore, in the year leading up to his death, he had overseen his professional specialty being given a space of its own at British medicine's top table by acting as the inaugural president of the Urological Section of the Royal Society of Medicine. 11 Therefore, in the wake of his death he was mourned accordingly by the profession, and the public at large, and left to his family, a personal fortune worth £130,000 that made him an unusually wealthy medical man by the standards of his peers. 12
This wealth and status was no fait accompli within the context of his origins. He had been born into relatively humble circumstances, the son of a Protestant tenant farmer-cum-sub-lessor, Samuel Freyer, and his Catholic wife, Celia, in Connemara, a rural region of county Galway, Ireland in July 1851. 13 Reliant on scholarships to attend university at the newly-founded Queen's College in Galway, after graduation Freyer took a predictable first step into the profession for men of his generation and background, enlisting in the colonial medical service, specifically the Indian Medical Service (IMS). The IMS was, after 1860, re-envisioned as the premier, meritocratic, and professional – if still racially exclusive – medical service under the employ of the Government of India. 14 For a ‘lad o’ pairts’ such as Freyer, drawn from the provincial reaches of the United Kingdom, colonial employment was touted, by medical schools, middle-class commentators, and ex-India hands, as a savvy way of starting a medical career, in spite of the then saturated labour markets for medical employment in Britain. 15
Freyer's Indian employment does not explain his eventual success; Freyer succeeded in spite of his IMS career, which ended in his being pushed from the Service on currents of frustrated ambition on his part, and official rancour on the part of his employers. Furthermore, when he developed a genitourinary practice in the 1880s and 1890s, he positioned himself in a field that engendered fear amongst the public, was the subject of ridicule amongst its therapeutic competitors and, even within its own boundaries, was still seeking answers to fundamental questions about the structure and function of the human genitourinary system. 16 It was the equivocal nature of his field's standing that made Freyer's contributions so noteworthy and garnered him such a rich professional reputation at the turn of the century. In particular, he addressed and ameliorated genitourinary's reputational failings through his innovation in supra-pubic prostatectomy (SPP), raising the field's public profile in the process.
His case diaries make frequent mention of his being required to adapt his practice to fit the mistrust of his patients surrounding their symptoms and his treatments. For example, in January 1905 he was visited by W.H. Wilcox, who was suffering from hypertrophy of the prostate and for whom Freyer opted to perform SPP in order to ‘totally enucleate’ his swollen prostate. Wilcox was, he recorded, ‘one of the most anxious cases I have ever operated on’, which was attributable to the long-standing pain his prostate had caused him; by the time Freyer removed it, it had hardened to the texture of ‘a cricket ball’ and required ‘great physical strength’ to enucleate ‘in equal halves’. 17 In other cases, patients came to him having been on the receiving end of heavy-handedness from other genitourinary consultants. Freyer recorded in J.H. Gartside's case from 1896 that he had been a former patient of the eminent surgeon, Henry Thompson, but would not let Freyer sound him, that is, introduce a bougie into his urethra to establish the scale of his stricture, ‘because Thompson had tortured him so’. 18
Over the course of his career, Freyer's success in performing SPP began changing public perceptions of genitourinary surgery's efficacy. C.H. Izod wrote to Freyer on 25 January 1919, fourteen years after undergoing SPP, to relay to him that ‘I am still a walking & working advertisement of the noble art of surgery … may you live to be in your 82nd year, as this leaves me at present’. 19 The way in which Izod praised Freyer was revealing: he was an ‘advertisement’ for the efficacy of Freyer's practice, which tied technical success to the raising of the operation's profile in an economic marketplace for medical services and allowed its beneficiaries to make a desired return to economic life. In a similar vein, shortly after having his prostate removed in March 1905, 63-year-old John Chapman informed Freyer by letter that ‘The urinary organs are in very good working order. I can quite realise the truth of a remark made to my son by one of the Windsor medical men that “Mr Freyer is giving men a fresh lease of life.”’ 20 Just as in Izod's case, Chapman's successful recovery under Freyer's care was doing the rounds of elite social networks in London, acting as a form of word-of-mouth marketing.
These testimonies from Freyer's patients are a few of several that demonstrate how the economic and epistemic uncertainties of his professional field were transformed into boons through his skill with a scalpel. From a lowly position in the late 1890s – where genitourinary surgery could promise little by way of technical efficacy, was viewed with suspicion by patients and undermined by competitors – Freyer used a previously dangerous surgical technique effectively, and begun to change public narratives about the field's effectiveness. It was out of this managed risk-taking, which made the uncertain more certain, that Freyer created his practice, and raised his profile in the eyes of his contemporaries, and the public.
As much was in evidence by March 1904, at the annual dinner of the Irish Medical Schools and Graduates’ Association. Held at London's prestigious Trocadero Restaurant, Freyer was presented with the Association's Arnott Memorial Medal, which was awarded annually to acknowledge a member's ‘act of heroism or distinguished service or an act performed in the discharge of medical duties either in civil life or in the naval or military services, at home, on the high seas, or abroad …’. 21 More generally the medal was part of the frequently-witnessed practice in middle-class Victorian culture of acknowledging a man's – always a man's – heroism by his being bestowed with an honorific, such as a medal. The Arnott was, therefore, a less well-known and more specialised version of the Victoria Cross and Albert Medal. 22
In Freyer's case, he was being recognised as ‘a hero’ through his perfecting SPP, which although performed since the 1880s he claimed to have made safer and of longer-lasting benefit to patients who underwent the procedure. 23 In presenting him with the Arnott Medal, Freyer's friend and contemporary, the Cork-born Henry MacNaughton Jones, wagered that ‘by his audacity and manipulative skill, by the exercise of his art … he had achieved the ultimate aim of surgery, the relief of human suffering, the saving and prolongation of human life.’ 24 The particular wording of MacNaughton-Jones's oration emphasised a specifically medical version of heroism, which ran counter to the terms of militaristic heroism invoked more broadly in Victorian society, premised as it was on self-sacrifice and glory through death. 25 Although Michael Brown has convincingly argued for medical ‘heroism’ being an extension of these more widespread gendered and militaristic discourses, here Freyer was incorporated into a heroic identity by saving the lives of others, rather than sacrificing his own in the name of the profession and nation. 26 In particular, he attained heroic status through the skilled but also ‘audacious’ application of advanced surgical techniques to allay the suffering of his patients. This style of heroism, premised on the preservation of life through measured risk-taking in the face of uncertainty, rather than the dutiful suffering of death, stood in contrast to the anxious qualms expressed by patients and exploited by patent medicine traders.
In one sense, Freyer's management of his field's failings, and the upsides it provided him within the marketplaces relevant to his services, are fulsome versions of the public economics of medicine. His technical proficiency made SPP safer and more palatable to the cultural tastes of his wealthy clientele, which in turn transformed that proficiency into financial returns and social prestige. However, as intimated above, at the same time as he was carving out this public reputation from a place of professional uncertainty, he was also creating a lucrative financial portfolio, which came to be the bedrock of his social and economic standing. The remainder of this article is given to understanding the contents of those portfolios, and what they reflect about his position in medicine and late-Victorian and Edwardian socio-economic hierarchies more broadly.
Freyer as Investor
As demonstrated in Figure 1, Freyer invested large sums of money over the course of his professional life. The surviving records of his investments visualised here demonstrate that he invested a huge proportion of his wealth (over £150,000) during his post-colonial career on Harley Street (1895–1921). 27 This underwriting of a medical career by financial investments was not unusual for this period. As Greta Jones has indicated for the years 1876–1910, doctors drawn even from well-known families such as the Darwins made the majority of their wealth from industry or finance, rather than their visible profession. 28 Within the context of the medical profession, however, the size of Freyer's estate made him an outlier. Jones has traced only two doctors with estates worth more than £100,000, with the highest proportion dying with an estate worth between £1000 and £2900. 29 By our calculations, for the period 1870–1914, the average wealth at death of Irishmen who enlisted in the IMS was £18,000, far less than Freyer's, which makes his wealth doubly noteworthy. 30
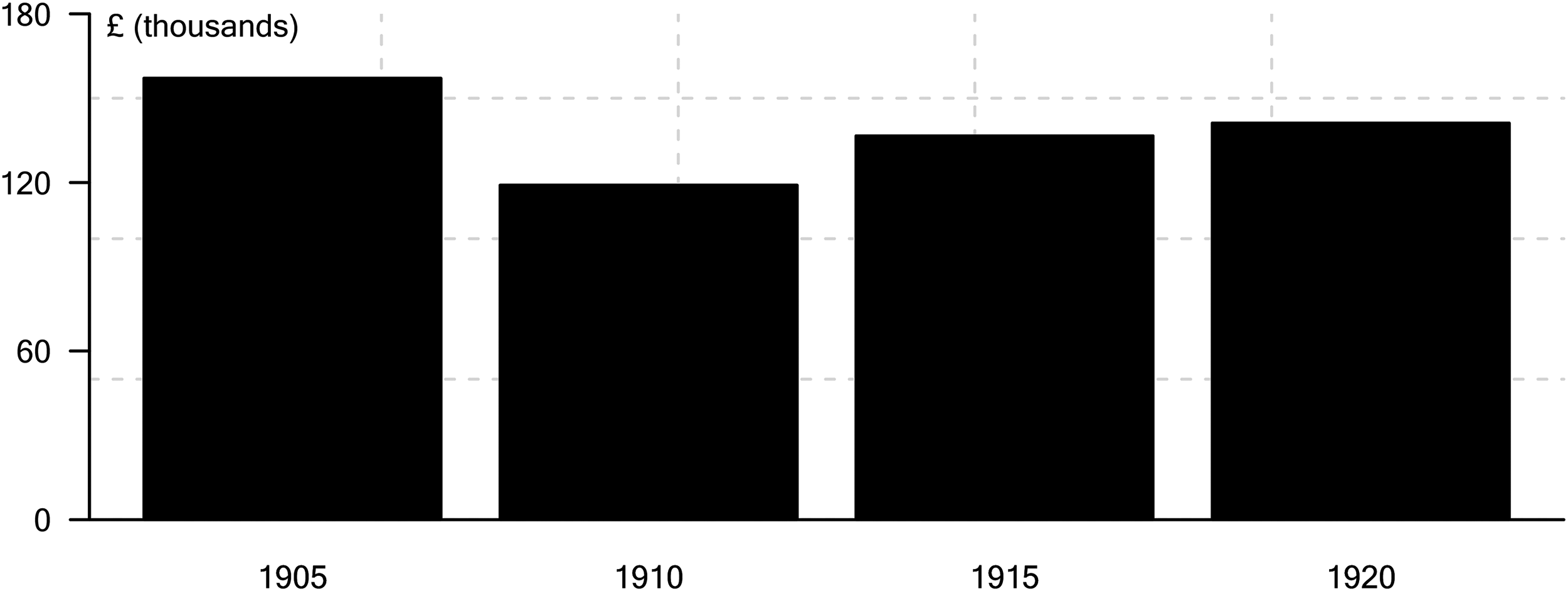
Freyer portfolio value (based on investment cost of purchase).
As shown in Table 1, roughly 74 per cent of Fryer's portfolio was composed of debt instruments, with the remaining 26 per cent in equities. 31 This portfolio composition may indicate that, through his choice of instrument, Freyer was averse to excess risk-taking beyond macroeconomic risks like inflation. Debt instruments have fixed nominal returns relative to equity instruments which are somewhat more exposed to economic fluctuations. A more detailed examination of the portfolio composition provides further confirmation that Freyer was risk-averse. As shown in Table 2, Freyer's largest investments were in government and corporate bonds, constituting on average 55 and 18 per cent respectively of his total portfolio value. Government bonds are typically the safest instruments available to investors, with the yields on these investments often referred to as the risk-free rate. Corporate bonds are subject to higher risk than government bonds, however, they are typically considered safer than equity instruments.
Portfolio decomposition by investment type.
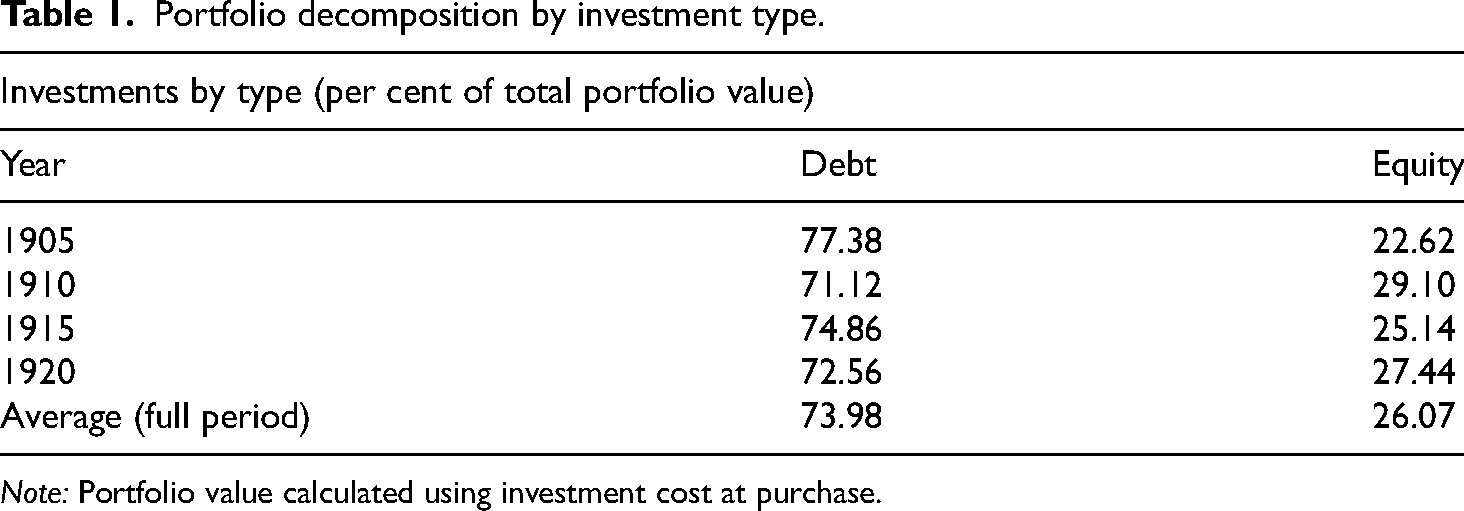
Note: Portfolio value calculated using investment cost at purchase.
Portfolio decomposition by instrument type.
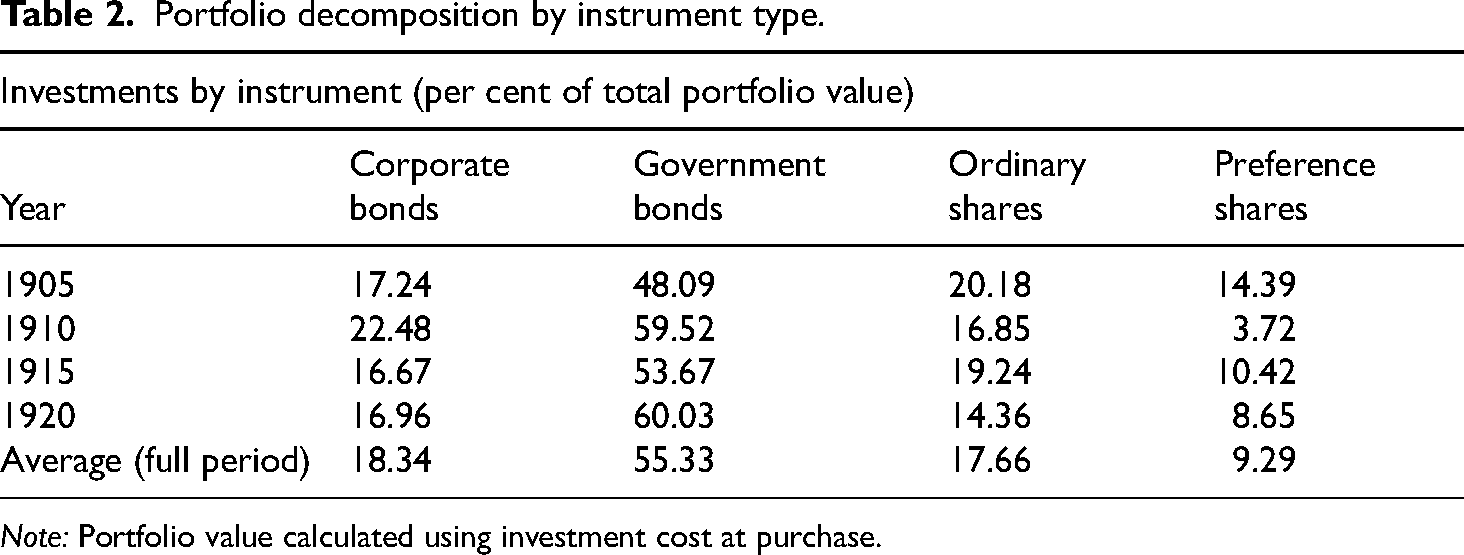
Note: Portfolio value calculated using investment cost at purchase.
Freyer maintained only around 26 per cent of his portfolio in equities, which shows that he was risk averse. However, when you break this proportion down by instrument, we see that Freyer allocated most of his equity capital to ordinary shares. On average Freyer maintained about 18 per cent of his portfolio as ordinary shares and around 9 per cent as preference shares. Given the overall risk-averse structure of Freyer's portfolio, being dominated by debt instruments, a greater share of investment in ordinary shares relative to preference shares among his equity holdings is unusual. Preference shares have fixed returns and are often considered very close in nature to bonds, while ordinary shares are free to fluctuate in value with market conditions, which can also affect dividends. This perhaps shows that Freyer had an appetite for risk in certain elements of his portfolio.
These equity positions do not challenge Freyer's status as a risk-averse investor. Freyer exercised a considerable level of diversification in his portfolio. As shown in Table 3, his investments were spread across several sectors including banking, corporate and semi-state entities, government papers, and railway investments. Furthermore, the geographic spread of his investments, shows that he stuck with what he knew; with British, Irish, and Indian investments respectively accounting for 60, 10, and 7 per cent of his total investments. These were places he had lived and thus probably understood how to estimate their value in accordance with what he knew about the commercial classes, government policy and broader macro-economic trends. As much becomes clear from the fastidious note-taking on the financial press that has been preserved in Freyer's archive. His records are festooned with press clippings that describe offerings of government debt and equities across a global financial market. These clippings often have sections of their text that he found particularly pertinent underlined in blue or red pencil, which were inscriptions that could pre-empt his taking positions in banks, corporations, bonds and railways in both emerging and fully-industrialised economies. 32 Although these investments were predominantly rooted in geographies and cultures that he knew from his personal journey through colonial medical careering, we should also note that he was not blind to opportunities elsewhere. The remaining proportion of his portfolio was spread across global enterprises: 4 per cent in Argentina, 5 in Australia, and 2 in South Africa.
Portfolio decomposition by sector.
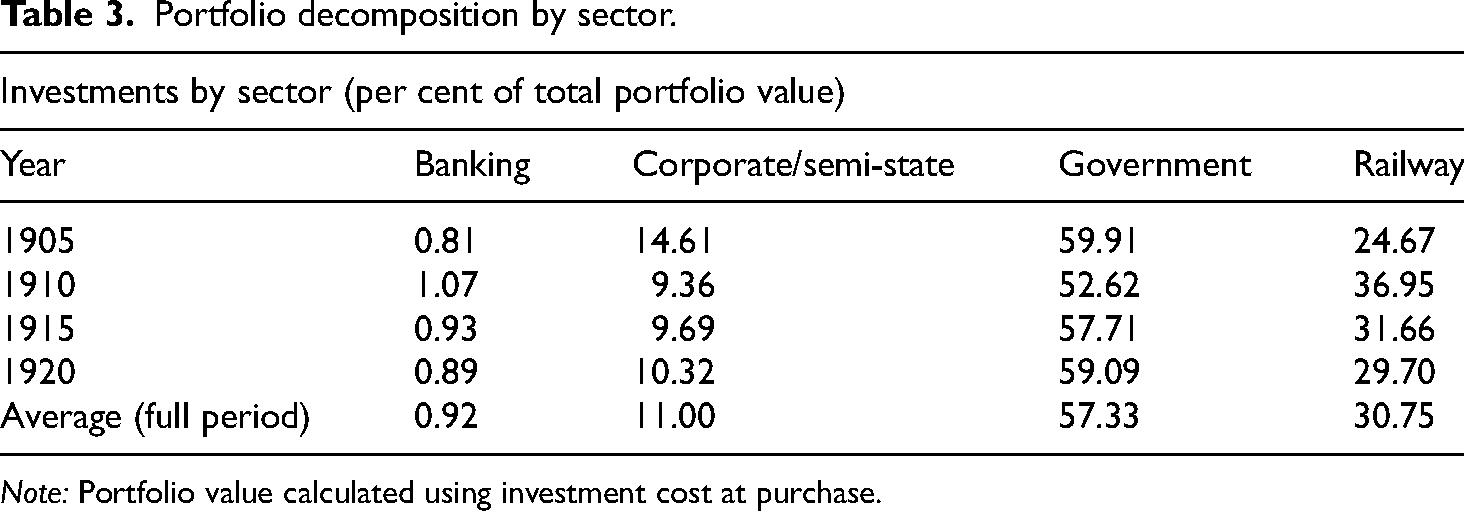
Note: Portfolio value calculated using investment cost at purchase.
Freyer's diversification strategies were largely in line with the investment diversification trends described by Sotiropoulos and Rutterford in 2016. 33 As they demonstrated for the period 1887–1902, the average British investor based 71 per cent of their portfolio in U.K. securities. A further 29 per cent was placed in overseas securities, with roughly half each of that proportion split between colonial and foreign (i.e., non-British colonial) securities. The same proportions hold true in Freyer's archive for his portfolio, with 70 per cent in the United Kingdom, 14 per cent in the colonies and 10.37 per cent in foreign securities. The striking deviation from Rutterford and Sotiropoulos’ average was in foreign securities, which would again indicate that he was financially risk-averse, and preferred holding positions in businesses and institutions with which he was culturally familiar. Overall, these diversification trends reveal investment patterns that were driven by regions and institutions with which he was personally familiar. Our reconstruction and description of Freyer's investment portfolio suggest that overall, he was a risk-averse investor. His investment and diversification strategies helped him to navigate broader economic fluctuations, and provided him with access to fixed nominal returns provided by debt instruments.
The Uncertainties of Colonial Employment – Tracing the Origins of Freyer's Financial Investments in His Colonial Service
Why did Freyer turn to finance as a way of underwriting his medical career, and how can we explain his aversion to taking financial risks? Freyer's interest in investment dated from before he began his career on Harley Street, and were attributable to the uncertainties of his colonial medical employment between 1875 and 1895. Although uncertainty and frustrated ambitions have been featured in scholarship concerned with the making of medical careers in Britain's empire during this period, we as yet have little sense of how doctors responded to this uncertainty, and offer the interpretation of Freyer's investments as a study of one such strategy. 34
As traced in the introduction section, IMS enlistment was common for men of Freyer's social class and ethnicity in the second half of the nineteenth-century, a period when medical migration to the empire from the United Kingdom became a given. 35 Irish, English and Scottish medical schools consistently over-produced medical graduates, meaning 53 per cent of their graduates circulated around the United Kingdom between 1860 and 1910. 36 A second substantial proportion, estimated by Douglas Haynes to be as extensive as 2000 graduates, or nearly 10 per cent of the British profession by the turn of the century, migrated further to occupy posts in colonial medical services across India, Africa and South-East Asia. 37
However, Freyer's investment patterns were contiguous with public employment reflects that professional jobs in the colonies, whilst lionised in public discourse as a route to professional success, were often a far more uncertain and riskier enterprise for those who partook in it. At the very least they did not live up to the expectations of medical students, who had been encouraged by their lecturers and mentors ‘to strike out boldly for the prizes available to them’ through colonial employment, safe in the knowledge that ‘once an entrance is gained [to the IMS], the doctor is forthwith relieved of all anxiety as to his being a success in practice’. 38 As a result, the half-century prior to c. 1920 was also a period defined by expressions of gloom about medical employment on the subcontinent. Between c. 1870–1920, numerous fraught letters of complaint from colonial surgeons were relayed back to the BMJ in London, lamenting a lack of prestige, poor pay and conditions, worse prospects for the future amongst IMS surgeons, and their consternation towards the better fortunes enjoyed by their colleagues in the Army Medical Department.
By the early decades of the twentieth century, the specific complaints of medical officers about pay and conditions had metastasised into a more general malaise about the status of medicine in India. In the midst of the dissatisfaction, the medical services were assaulted by precipitous falls in recruitment, the lobbying of middle-class Muslim nationalists for greater representation of their brethren in the Indian public services, and a version of these demands being realised in the wide-ranging Minto-Morley reforms (1919). 39 This cauldron of factors led ex-India hands, such as an Irish contemporary of Freyer's in the IMS, Patrick Hehir, to diagnose a ‘crisis’ of ‘western medicine in India’. 40 The effects of this crisis were, according to Hehir, ‘retrogression’ and ‘a decline in the efficiency and skill with which orthodox medicine and surgery will be practised in our Indian Empire in the future’. 41
Freyer's experience of employment in the IMS came to resonate with this symphony of discontent, decline and uncertainty. In March 1888, he was seconded by the Government to the principality of Rampur in order to treat the state's Nawab, Kalb Ali Khan, and his sickly son and successor, Muhammad. 42 For this service, he was paid 100,000 rupees (a lakh) by the younger Khan, who had ascended to the principality's throne after his father's death in March 1888 having recovered from ‘an advanced case of paralysis’ under Freyer's medical attendance. By contemporary valuations, the sum was worth £10,000, or approximately £820,493 today. 43
The public nature of the sum's bestowal, its size, and Freyer's acceptance of it was interpreted by the Government as Freyer having contravened the purpose of public service – enriching himself, rather than serving the colonial state – and that he should leave ‘the value of his services to the judgement of the Government in whose employ he is serving’. 44 The Lieutenant-Governor of the North-Western Frontier Provinces, Auckland Colvin, who first voiced the official interpretation of his remuneration, subsequently requested Freyer to turn the fee over to the exchequer, and on Freyer's refusal, changed his position to requesting Freyer return half to the state. If, Freyer was told, he continued to refuse, he could expect a bar to be placed on his further promotion through the IMS. 45 Freyer maintained his position, on the grounds that there was no rule preventing his accepting the money, and that other public officials had also received similar fees for their work but had not been treated as he had. 46 In consequence, the Government made good on its threat and he languished in his position as a Lieutenant-Colonel for seven years, the official stance on the matter being repeatedly enforced by civil servants in Lucknow, Calcutta and London. 47
Freyer's Rampur controversy was an illustration of how professional jurisdictions were brought into conflict during the late-nineteenth century, and the consequences for an individual's status of running counter to the values and principles of the institution they served. 48 In this case, the public services of India, populated as they were by lawyers, professional civil servants, and increasingly, through the piecemeal meritocratic reforms of imperial administrations, ‘parvenus’ in medicine and engineering, fractured along inter-professional lines. The interests of doctors, Freyer and his supporters within the IMS, were pitched against those of lawyers and civil servants, such as Colvin and senior administrators within the Government and the India Office in London, with the battles between them waged in terms of discourses concerned with the moral meaning of public service in the colonies, a topic well-established in British imperial and colonial history. 49
However, we must bear in mind that there were limits to the power of these discourses to shape the careers of those involved; uncertainty in the wake of official sanction was certainly not the death knell for Freyer's professional status, but forced him to adapt his personal finances beyond those made possible by his medical career. Thus, his archive reflects that one of the ways in which he responded to this obstructing of his career's progress was to either extend pre-existing income streams or create new ones beyond public employment, which included a roving private practice for genitourinary diseases to European and indigenous elites, and his earliest financial investment in local Indian businesses. His diversification into private practice was not directly induced by his being barred from promotion in the IMS; he had gained a reputation amongst, in his own words, ‘local native gentlemen’ prior to beginning his secondment in Rampur. 50 However, his ledgers for the early 1890s contain particular mention of the fees he charged ‘Birhan Pershad’, ‘Rev. A.E. Vivian’ and ‘Mrs Granger’ for private medical practice that supplemented his IMS income.
In addition to private practice, Freyer was a medical bureaucrat to emigration agents for assessing the health of Indian indentured labourers probably bound for one of a number of locations around the Indian Ocean, and British South Africa. He recorded three sums received for examining ‘emigration coolies’ between 1894 and 1895, which amounted to the small sum of 400 rupees. However, aside from their small amount, these payments demonstrated the forms in which he provided medical services beyond his formal employment in the IMS. No doubt, the extent to which flows of indentured labourers left India during this period, and the increased status of medicine as an official arbiter of public health, would have created earning opportunities for well-placed and savvy medical officers such as Freyer. As estimated by Thomas Metcalfe, between 1830 and 1920, 1.3 million Indians were contracted as indentured labourers on sugar plantations in a system of labour that has been termed ‘a second slavery’. 51 By the turn of the twentieth century, procuring medical knowledge and opinion had become one of the fixed economic costs of these indentured labour schemes and, in tandem with changing political and military circumstances in some of these ports of arrival, more sophisticated diagnostic technologies were used to assess the fitness of labourers recruited by agents in India. 52
Aside from his status as a bureaucrat and private practitioner, the period of his frustrations within the IMS also coincided with the first surviving records of his career as an investor in financial markets. Whilst the data above reflects his portfolio's eventual character as a record of truly global patterns of investment – from his acting as a creditor to the Prussian government, a shareholder in Guinness, and an investor in the Buenos Aires and Pacific Railway – at the start, Indian employment was a useful conduit for gathering information about local, Indian markets.
As has been argued by Bishnupriya Gupta, investment patterns in India were tethered to social networks in particular places and amongst particular ethnicities. According to Gupta, industrial investment in Bombay was the preserve of ethnic Indians trading in textiles, whereas British-owned businesses dominated Calcutta through investment in tea, jute and coal. 53 Gupta's thesis holds true in Freyer's case, at least as regards place. However, the types of business into which Freyer invested bore a greater resemblance to Gupta's ‘Bombay’ model. He held stakes across a range of Calcutta-based textile mills in this period, with no mention of coal or tea, and this pattern is congruent with what we know of who invested in Indian textiles. Jute and cotton, for example, were particularly ‘British Indian’ investments, with both gaining the vast majority of their investment capital from rupees rather than sterling. 54 As Gupta argued, jute had been a staple of the Indian economy for centuries, and offered an opportunity for British residents in India to make a profitable investment in a commodity to which domestic British investors did not have access in the same degree or quantity. 55 When Freyer was on the ground in India, jute was a particularly attractive prospect, as its production experienced a return to profitability after a contraction in the mid-1880s due to the market's inability to cope with the effects of an increase in supply. 56 He was alert to the commodity's change in fortunes and, in May 1892, the ledgers describe his taking shares in the Budge Jute Mill Company. 57
What this profile of Freyer's economic activity during his Indian career, and particularly during the dispute with the Government over Nawab's fee, represents is a broadening of our awareness about medicine's economics in the late-nineteenth century, and the place of professional uncertainty in determining the markets through which a medical man moved. Freyer, and most probably others like him, were not ‘rational actors’, buying medical goods and selling medical services by way of their professional credentials alone. They were partaking in these forms of economic activity but also had their careers defined by the effects of institutional attitudes towards their work and its proceeds. Although it is useful to think in terms of, for example, the jurisdictional battles that take place between professionals in given historical settings, there is important analytical work to be done in asking what happens after those battles have played out. What do the actors who have taken part in them do next, and how does their professional status change accordingly? Our overall point in this article is that one of the results for those who have their jurisdiction limited within their established field of expertise is to evolve multiple ways of working, which provide them with a more diverse spread of income and opportunities. For Freyer, his frustrated relations with the Government of India pushed him to partake in different forms of economic activity in an attempt to maintain his professional status, practice and income. Additionally, the fallout from events in Rampur drove him to become more reliant on safe positions in financial markets than was previously the case.
The Scalpel and the Ledger – Freyer as Surgeon and Financier in London's Elite Society
Freyer's ability to adapt to the economic uncertainties of colonial employment did not save his career in the IMS: by 1895, he had decided to retire from Indian service, and used the proceeds of his work in Rampur, coupled with his other earnings from private practice and financial markets, to purchase the lease on No. 27 Harley Street, the address from which he founded his elite genitourinary practice. Over the next twenty-five years, he established a formidable reputation in medicine with which we are by now familiar, and furthered the extent of his private career as a successful financier. The work of this section is to map the extent to which these two composite parts of Freyer's expertise were inter-related, and what the similarities and differences between them denote about both his public status in medicine, and his position in the elite socio-economic orders of Edwardian Britain.
Freyer was, on occasion, explicit about the influence of finance – and particularly financial risk – on shaping his medical career, and did so by way of the logic he applied to his medical practice, and also the language he used to describe himself. Whilst working in Rampur, Freyer produced a number of documents in which he assessed Nawab's health for the benefit of the government's strategic interests in the principality. In one of these documents, which was addressed to Auckland Colvin, he assessed Nawab's present and future health in the following terms: ‘Perhaps I can put this case most clearly if we judge of him [the Nawab] by the practical standard of a Life Assurance Company. Judged by this standard he cannot be regarded as either a first or second-class life. In fact, no Insurance Company would be certified in accepting his life for insurance at all.’ 58
This was the period in which life insurance emerged as a form of risk management in both Britain and the United States. Life insurance corporations were founded in the middle of the eighteenth-century, to assess the risks associated with maritime trade and notably that which dealt with the transport of slaves. However, it was not until after 1860, with the advent of actuarial science and its promise of more accurate and representative mortality tables for the calculation of probabilities concerning policy-holders’ longevity, that these firms and their products began to spread extensively through Britain and America. 59 Taking the United States as an example, William Rothstein plotted the number of life assurance companies increasing from forty-three in 1860 to 84 in 1900, and by 1911 he estimated that little over half of American and Canadian physicians were medical examiners of applicants for life insurance policies. 60
Uncovering here the intersection of medicine and life insurance in circumstances defined by colonialism's hard, strategic edge offers an additional layer to this history. Freyer's memorandum did not include any mortality tables or other sorts of quantitative evidence to lend formal verification of his assessment concerning Nawab's health. Instead, the memorandum served a rhetorical purpose: to provide Colvin and his fellow civil servants with a heuristic of Nawab's present and future health. The forms in which capitalism provided colonialism with an engine to expand and maintain its presence beyond Europe in the eighteenth- and nineteenth-centuries have long been noted by both contemporary commentators and historians. 61 But here we have a very specific example, in which discrete modes of professional identity – medicine and finance – converged to form a conduit for colonial power. Freyer, as a medical doctor, aped the language of an actuary to assess and exploit the health of an indigenous elite in the interests of colonial rule. Could there be a neater example of medicine acting as, to borrow Bridie Andrews’ and Andrew Cunningham's formulation, a ‘tool of empire’? 62
However, we should hesitate before pushing that metaphor too far. In the second instance of Freyer's invoking finance, this time linguistically as a form of self-description, he illuminated how his actions in Rampur exposed him to types of uncertainty and risk in the making of his career that were related to extensive, cultural discussions about the moral rectitude of money and its earning. Shortly after accepting the Nawab's fee he wrote to a colleague and self-identified as ‘a gambler playing for high stakes … if I have the good fortune to win, it must not be forgotten that there was long odds [sic] on my losing.’ 63 Freyer's self-identification as a ‘gambler’, coupled with his identity as a financier, is a pertinent illustration of the way in which Victorian Britain's burgeoning financial economy transcended the markets and exchanges in late-Victorian society and came to form an important form of social and cultural orientation for those who partook in its commerce. As opined by Tamara Wagner, writing of stock-market crises in Victorian literature, the stock market did not merely reflect contemporary financial crises but ‘formed a new cultural imaginary that expressed changing ideas of moral probity and indeterminate identity, creditworthiness and the management of financial risks’. 64
In a parallel study of ‘gambling’, as both an activity and a form of identity politics, David Itzkowitz has demonstrated the ways in which Wagner's ‘cultural imaginary’ operated in line with the creation of new distinctions between the middle- and working classes. 65 By his reckoning, after mid-century and through to the 1920s the middle classes sought to distance their relationships with risk in financial markets, mediated through stock exchanges, from the forms of risk in which the working classes partook in betting shops and the unregulated financial trading spaces. 66 The products were false distinctions that siphoned interpretations of ‘gambling’ away from the apparently more legitimate forms of practice known as ‘speculation’ and ‘investment’. Therefore, in describing himself as a ‘gambler’ to his colleague, he was indicating that his trust and reliability as a professional were placed under scrutiny because of his practice in Rampur.
Drawing upon these interpretations of finance in late-Victorian culture provides valuable context for why Freyer was, firstly, conservative in the markets and, secondly, why this form of expertise, remained private and divorced from his professional reputation as a medical practitioner: the taking of financial risks and being identified as partaking in the financial economy posed a threat not only of material, but also cultural, ruin. This is where we should bear in mind his status as a ‘first generation’ medical professional, operating in a context on Harley Street where his clients cared deeply about the reliability of those from whom they sought medical treatment. As Christopher Lawrence once noted in relation to this period, ‘what counted for the rich in choosing a doctor was whether he was a gentleman’, that he symbolised opposition to any suggestion that medicine was ‘reducible to a body of knowledge which had precise rules for its implementation’, and that as an individual he embodied claims ‘to moral and cultural leadership of professional and national life.’ 67 Freyer's professional field existed against a cultural backdrop where ‘character’ was a vital idea in public discourse. Accordingly, then, it was necessary for Freyer to jettison any associations with the ‘gambler’ he had been in Rampur, and become a reliable medical expert in the view of the elite clientele he served.
But in addition to the necessity for him to manage this cultural politics of expertise, we also know that his professional standing was also tethered to his ethnic origins in Ireland. This was evident in how he was presented with the Arnott medal in 1904, but even after a quarter of a century on Harley Street, the obituaries written on his death identified Freyer, erroneously, as ‘“he man from Roundstone [a village to the south of his actual birthplace, Cleggan]” who had retained his “Irish brogue” throughout his career at the pinnacle of British medicine’. 68 His distinctions of accent and place of birth would, when coupled with his management of risk in the markets, have been particularly acute in British high society in the Edwardian era, a time when presumptions of Irish unreliability inflected acutely in imperial politics. The trope of the ‘unreliable Irishman’ coursed through Parliament as a result of heated debates about the application of Home Rule to Ireland, and fears amongst Conservative parliamentarians that Home Rule for Ireland might inspire dreams of independence amongst nationalists elsewhere, not least in India. 69
Freyer was woven into émigré social networks that put him in touch with individuals invested in the cultural and political separation of Ireland from the United Kingdom. In March 1905 he was referred a patient by Johnstone Redmond, a cousin of John Redmond, the leader of the Irish Parliamentary Party and Home Rule movement. 70 Freyer was later listed as amongst the chief mourners at Redmond's funeral, held at Westminster Cathedral. Furthermore, a close reading of his financial ledgers shows his support for the cultural project of the Irish literary revival at the turn of the century: between 1897 and 1902, he subscribed to the Irish Literary Society, which had been founded in 1892 by revivalists such as W.B. Yeats. 71 Within his professional milieu, then, we can well imagine Freyer's chasing of high returns on risky investments being interpreted amongst his professional neighbours and clientele as evidence that the Irish were as risky in the markets and the clinic as they were in Parliament and the parlour room. Whilst there is little evidence in his case diaries that his politics determined his clientele, the snapshots we have of his various associations with Irish culture in London would have needed to be curated in step with how these, as well as any financial risk he exposed himself to, might have damaged his professional reputation. Therefore, his pursuit of steady returns in the markets was likely part of a broader hedging of reputational damage within elite society, against suspicions about Irish moral and political reliability in British culture.
Lastly, we should bear in mind that, between the growth of his professional reputation in medicine and his private cultivation of a financial fortune, lay his orchestrating a move from provincial obscurity to metropolitan acceptance for him and his family. Sections of his ledgers provide glimpses of the social mobility that his various economic activities and professional successes supported, in terms of where and how his children were educated. Freyer noted how much he paid for his son Dermot's tuition at Temple Grove preparatory school in East Sheen, an elite school for boys. 72 Later, he was paying for Dermot's tuition at Wellington College, one of Britain's elite public schools, and at Trinity College, Cambridge. 73 These are indications of the social history that Freyer was living out, and that were attached to proficiencies as a doctor and financier that were underwriting a shift in his family's social position. His direct funding of Dermot's attendance at elite institutions symbolised a shift from his experience of reliance on scholarships to attend a new, provincial university a generation before. Additionally, there are scattered entries in his debit columns to the remittances that he sent back to his parents in Cleggan. 74 These outgoings provide us with a sense of what was at stake for Freyer. The economic choices he made and the professional reputation he maintained were directly connected to his children's ascent into elite society, and his parents' comfort in old age.
Therefore, Freyer's private career in finance, and his conservative style of management, was not only a form of economic diversification to counter professional uncertainty. In addition, his managing a portfolio of expertise was connected to broader social realities. Given his self-identification as a gambler in Rampur, and his obvious ability to assess risks in financial marketplaces and in treating patients, he would have been conscious of the ways in which his own professional standing was uncertain, too, and the threats that uncertainty posed to his and his dependents’ position in British society.
Conclusion
When Freyer died in September 1921, British and Irish newspapers marked his passing by mourning a ‘great surgeon’. The Times in London wrote of his exploits in India, and how he had spent the time since intervening in the lives of elderly men and endowing them with a new lease of life. Smaller newspapers relayed this same message through towns and villages across the United Kingdom, not least the Tuam Herald, the local newspaper serving a small market town sixty miles to the east of Freyer's birthplace in Connemara. 75
This article has been an exercise in demonstrating how Freyer's historical significance was far more extensive than just being the medical protagonist of these public stories, which were ultimately ways of expressing contemporary hopes about the power of scientific progress. We have argued here that Freyer's undoubted acuity in medicine was not the sole determining factor in his successful navigation of Edwardian Britain's elite socio-economic orders. Rather, he had to deploy acumen away from medicine, to maximise the success he could achieve in his formal, public professional field.
We hope to have demonstrated through this argument that there is a benefit to small-scale studies that question the extents of and adaptations to the exercise of professional power when particular types of professionals have been confronted with uncertainties in their formal field of work. We have very many sophisticated and extensive theories of why professionals create and sustain their fields: to claim ‘jurisdiction’; to exercise sovereignty by way of ‘biopower’; to perform a particular public ethic, or ‘logic’. 76 We also increasingly have sophisticated and more detailed accounts of where professional power is located, not only in professional associations, qualifications or marketplaces for services, but in successfully performing a role that resonates with culture more broadly. 77
However, here we have provided an insight into a professional adapting to socio-economic circumstances throughout his career, in public as well as private, and doing so in such a way that put him in touch with economic phenomena relevant to his needs beyond the terms and conditions of his formal profession. This is a far more unusual insight into how professionals function and adapt strategies to the socio-economic conditions of both their own lives and also those of their professional field. We think it creates the possibility for interesting future inquiries: how representative was Freyer's maintaining two realms of expertise for other members of liberal professions in this period, not only in Britain but on the Continent and in the United States? To what extent did other colonial professionals employed by European empires underpin their careers as lawyers, civil servants or doctors with shadow careers as financiers? If Freyer was able to successfully maintain these two careers, what of those who failed? How did failure in the markets impact upon professional life of his contemporaries who maintained financial portfolios, too? Given the scale of financial investment amongst the middle classes at the turn of the twentieth century it would be unsurprising to find that many of Freyer's contemporaries were also professionals-cum-financiers, and that this relationship between two seemingly distinct types of expertise was a key factor in the shaping of professional work and fortunes.
Footnotes
Acknowledgement
Our thanks to the staff of Special Collection and Archives, James Hardiman Library, University of Galway.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Author Biographies
Dr
Dr