
Abstract
During the Second World War (1939–1945), the rate that flour was extracted from wheat to make wholemeal bread was continuously increased to save wheat supplies in Ireland. Once the dangers of eating this bread became known, doctors and scientists advocated that extraction rates be reduced alongside the fortification of flour to counteract the potential side effects. Despite several calls for action, no changes were made until connections were drawn between calcium deficiency, rickets and tuberculosis (TB). This article uses flour as a case study to understand the complexities of introducing health policy at critical periods, such as war. While interest in public health was raised due to the war, the war also ensured that attempts at sound food policies were limited. Higher extraction rates temporarily relieved wartime pressures, but this had severe health effects on the wider population. By mapping flour extraction rates alongside the incidence of disease, this article argues that political short-terminism exacerbated public health problems as symbolised in the black loaf. It was the medical profession that managed to successfully encourage action on the sole basis that flour extraction had created a health crisis among children and the poor.
Introduction
‘Arán an Lae Amáireach’ or its English derivative, ‘Tomorrow's Bread’, was one of few documentary films shown in Irish cinemas and theatres during the Second World War (1939–1945). Produced in connection with the ‘Grow More Wheat!’ campaign and the Department of Agriculture, this film was essentially ‘a story in pictures of the nation's food supply’, urging its viewers to note the severity of the supply situation at hand. 1 This was part of a wider Fianna Fáil propaganda campaign that repeated the slogan ‘Grow More Wheat!’ in political speeches across towns, cities and public memorabilia. 2 Here, Irish farmers were asked to ‘supply the food requirements of Irish men, women and children’ and phrases like ‘Remember the Nation's Bread Supplies depend on you’ were common. 3 Compulsory tillage orders requiring Irish farmers to till wheat and other essential cereal crops were the most aggressive forms of the campaign. The use of tillage inspectors ensured, where possible, that these quotas were met. Not so common in printed public materials, however, was the use of the term ‘black’ in relation to bread. In January 1941, the phrase ‘black bread’ was banned by the censor. 4 This black loaf embodied the contradictions involved in the state's efforts to feed its population during the war.
The black loaf was a result of changes to flour extraction necessitated by wartime shortages. Alongside maximising wheat production, Fianna Fáil sought to minimise the amount of wheat wastage during the Emergency period by increasing rates of extraction. 5 Extraction refers to the flour milling process: the extraction rate describes the portion of the wheat grain that is used to make flour. Before the war, it was normal practice to produce wheaten bread from flour that was extracted at 70–75 per cent. 6 As flour was among the more severe wartime shortages, one resolution to poor wheat supplies was to increase extraction rates. The rate that flour was extracted from wheat was continuously increased, measuring at 100 per cent on some occasions during the war. High extraction flours produced a loaf of a dark, grey-brown colour: the ‘black bread’ that became common in the Irish vernacular. 7 Crucially, close to 100 per cent extraction meant that the government was encouraging millers to create a product that contained matter the human body simply could not digest. In this way, flour supplies were increased by degrading the quality of the flour itself. 8 New findings in medical research showed the detrimental side effects of high extraction rates on public health. As early as 1940, studies in Britain confirmed suspicions that more toxins (phytic acid) were in flour extracted at higher rates. 9 The high phytic acid content reduced human absorption of calcium, thereby reducing intake of a nutrient vital for human growth. Although these findings were known in Ireland, extraction rates were not lowered until December 1943 and flour was not fortified with calcium until June 1946. Meanwhile, the Irish medical profession implicated calcium deficiency as a factor in the rising incidence of rickets and increased tuberculosis mortality which closely followed the increased extraction rates.
By mapping flour extraction rates alongside the incidence of disease, this article argues that political short-terminism exacerbated public health problems as symbolised in the black loaf. While high extraction flour temporarily relieved wartime pressures, it had severe health effects on the wider population, and exacerbated tensions between the Department of Industry and Commerce and Department of Local Government and Public Health. Such was the prioritisation of key supplies that scientific warnings against the use of high extraction flours were ignored. Struggles to reach viable compromises resulted in unnecessary delays that ultimately contributed to a rickets epidemic and a higher tuberculosis (TB) mortality rate. It took a growing health emergency for the Irish government to take action to reduce extraction rates and fortify flour with calcium. These changes were too little too late for those who had already suffered. Nonetheless, the response suggests that rising rickets and TB mortality were treated as public health priorities once they had been proven to exist. An investigation of how this emergency was allowed to occur and what factors encouraged a response reveals the oppositional factors involved in initiating public health policy as well as providing insights into the direction of the newly independent Irish Free State.
Emergency Ireland
Internal changes in the official cabinet throughout the 1940s had a significant impact on food policy. Following the outbreak of the war, the Emergency Powers Act 1939 allowed Fianna Fáil to pass orders without detailed consultations in the Dáil. 10 Bryce Evans has previously noted that security was the main priority of the Irish government at this time. 11 The stabilisation of the Irish economy was central to this security. The Department of Supplies, previously established in 1938 under the auspices of Seán Lemass's Department of Industry and Commerce came into effect following the declaration of war. The main function of this department was to control rationing and maintain supplies. As Minister for Supplies, Lemass controlled the ‘treatment, keeping, storage, movement, distribution, sale, purchase, use and consumption’ of all goods throughout the war. 12 An extension to his ministerial duties as head of the Department of Industry and Commerce prior to the outbreak of war, the scale of additional powers that Lemass assumed during this period cannot be ignored. 13
Established on 20 February 1941 to assist the Department of Supplies, the Emergency Scientific Research Bureau addressed industrial problems faced by agriculture, food, clothing, building and engineering industries. 14 This bureau was advisory and comprised senior businessmen and scientists who examined the possibilities of using indigenous raw materials where shortages existed. 15 Professor J. J. Dowling, the bureau's chairman, was a founding member of the Institute of Physics and had been a fellow student of Éamon de Valera. 16 Other key members included Professor M. A. Hogan and Dr T. S. Wheeler, both of whom were leading scientists in their fields (geology and chemistry). 17 As Bradley has noted, all members were Dublin residents, and this made possible ‘almost daily contact’ with bureau officers and those of the Department of the Taoiseach. 18 Initially proposed for the duration of one year, the bureau continued for a further three years with its members paid ‘an honoraria at the rate of £300 per year’. 19 While it existed independently outside the direct control of the Department of Industry and Commerce, its purpose was to advise, with the Department of the Taoiseach ultimately holding the last say.
In a memorandum addressed to the Department of the Taoiseach, Lemass, conscious of the country's deteriorating food supply, urged that ‘a committee of qualified people, including experts in human and animal nutrition, should be set up to survey the whole question of our present and future food supplies and to make recommendations for their most economic use’. 20 In response, the Medical Association of Éire established the Dietetic Council on 24 October 1941. 21 Consisting of members of the Medical Association of Éire with an interest in nutrition, the council made recommendations to the government on food issues during the Emergency. It continuously liaised with the Seán MacEntee's Department of Local Government and Public Health, as well as both the Department of Supplies and the Emergency Scientific Research Bureau. While MacEntee's department was a spending department in its own right, the extent of funds available for health services depended on finance allocations from the Department of Industry and Commerce. Unlike the Research Bureau, this body was voluntary and its members unpaid, doing this work in addition to their other duties. 22 The council was not a recipient of government support, and relied heavily on the Medical Association of Éire for funding.
The war gave heightened visibility to the vulnerabilities of the young republic. One of the harsh realities of Irish independence was that the economic and social imaginings of pre-independent Ireland did not come to fruition. Instead, poverty increased, and TB and infant mortality were higher than that found in other developed western nations. 23 The toughest indicator of wartime adversity for Irish people was a fall in real wages that coincided with a rise in the cost of living. 24 These conditions worsened in May 1941 when a Wages Standstill Order, outlawing industrial action for greater pay, came into effect. 25 Meanwhile, the Catholic Church discouraged any use of birth control and this found government support in a ban on the sale and importation of contraceptives from 1935. 26 Gerard Fee has noted that Catholic teaching undermined the state's willingness to directly intervene in social matters in the Emergency. 27 This contributed to a situation in which poor families had more children than they could comfortably clothe, feed, and house. 28 Further, extreme shortages of imported goods such as food and fuel exacerbated existing conditions as many families struggled to make ends meet in the face of rising prices. 29 The effect that these shortages had on everyday lives was poignant. Where families lived in one or two rooms, cooking facilities were put under strain due to the loss of coal. 30 In accommodation with small fire-grates, cooking equipment could not be facilitated by alternative fuels such as turf and wood. 31 In some areas, this led to a reliance on ready-cooked foods – bread being among the most notable.
Supply Issues Around Wheat and Flour
Historiography surrounding Irish neutrality has reached consensus on the importance of economic survival to the Irish government during the war. While attempts to ensure the state's economic vitality ‘carried out the best intention: the prevention of starvation’, the means used to achieve this has not been given the same historical coverage. 32 Flour quotas were intimately linked to the country's broader supply question that provoked a constant socio-political tug-of-war between the Irish government and Irish businesses. Each shortage was also linked to a broader supply chain that was severely curtailed due to wartime disruptions. This was hardened by Ireland's vulnerable trade relationship with Britain due to the state's insistence on Irish neutrality. For instance, anxiety surrounding the risk of shortages caused a surge in panic buying and therefore prices of basic foodstuffs increased substantially. 33 This was compounded by economic sanctioning by the British Board of Trade on 2 January 1941 in an attempt to undermine Irish neutrality. Exports to Ireland of food, fertilisers, animal-feed, agricultural machinery, iron and steel, electrical goods and cardboard were rendered subject to licences, and these licences were, as Bryan has argued, deliberately withheld by specific British government departments. 34 In response, coal, kerosene, turf and fuel oil were rationed in Ireland in the same year. 35 The effect that this had alongside a shortage of available Irish ships culminated in a complete system of rationing by May 1942. After all, a severely jeopardised trading relationship with Ireland's leading trade partner (UK) and a lack of Irish charter to import food meant that the Fianna Fáil government had to rely entirely on producing food in Ireland. 36 Petrol and coal were equally indispensable to food distribution and consumption.
Even as a predominantly agricultural country, there was no quick-fix for Ireland's wheat shortage. As a crop, it could not be produced within six months. Instead, it was a ‘10, 11 or perhaps, 12 month crop’. 37 So acute was the wheat shortage in the 1941 harvest that Ireland had only nine months’ worth of wheat, prompting Lemass to impose export restrictions on the malting of barley. Beer exports were also banned from March 1942. 38 While official bread rationing was not introduced in Ireland until 1947, flour supplies were tightly controlled in Fianna Fáil attempts to ensure fair distribution among the population. 39 The most interventionist of all was the compulsory tillage scheme: a scheme that encouraged farmers to till their land for wheat and cereal crops rather than dairy or grazing use. 40 This involved the Department of Agriculture using inspectors to ensure that the rising tillage quotas were met. 41 Although wheat acreage increased during the first year of the war, the amount of barley and oats fell by 80,000 acres. 42 Malting barley was a notable ingredient in the manufacture of whisky and beer and there was a surge in demand on the British war front for Guinness throughout the war, adding further complexity to the existing wheat problem in Ireland. 43
While scholars such as Bryan, Daly, and Fee have devoted attention to government policy in recent times, the devastating impact that this food campaign had on the lives of the people is deserving of more historical scrutiny. There were bread queues. Some reports detailed waits of over two hours. 44 This was, as one Irish Independent article noted, a ‘soul-destroying hardship’ when it is realised that many people were taking the bicycle to do their weekly shop to conserve their petrol rations. 45 In an attempt to decrease rural consumption, Éamon de Valera urged the country people to eat alternative foods like potatoes instead of bread at the annual meeting of the Irish Countrywomen's Association on 12 March 1942. 46 His reasoning was that bread supplies should be prioritised for the urban population, citing that city people had stood by the farmers during the economic war. 47 Housewives were also targeted by the government-commissioned cookbook, Flour Economy by Maura Laverty. This encouraged Irish women to use flour sparingly within the home. 48 Public and radio talks were held while food production lectures equally sought to disclose the scarcity of food supplies. 49 Rationing aside, initial efforts favoured a bottom-up approach through increased production and by educating the masses of the different methods of production to save supplies. Unbeknownst to the public, however, were the health effects that occurred because of government measures like flour extraction.
Medical Consequences of Extraction Rates
Early successes in the national food campaign were limited as existing shortages worsened. In response, the Department of Supplies issued a series of emergency orders that changed the composition of the bread itself. Baked wholegrain bread contains bran, germ and starch, while white bread contains only starch. Flour becomes more nutritious at higher levels of extraction. However, beyond a 90 per cent extraction rate, its phytic acid content impedes the absorption of necessary calcium into the body. 50 Beyond a 92 per cent extraction rate, there is material in the flour that cannot be digested by the human body. 51 Limited wheat reserves in late 1940 prompted the Department of Supplies to raise extraction rates to 75 per cent and later to 80 per cent. 52 On 27 January 1941, this rate was increased to 90 per cent. 53 Less than three months later, Emergency Powers ordered that flour must be extracted at an even higher 95 per cent rate to conserve supplies. 54 So scarce were wheat supplies that bread or any other wheaten foods could only be served at one course in catering establishments throughout the country from March 1941. 55 Continuous attempts at preservation of supplies culminated at 100 per cent extraction from February 1942 right through to December 1943. 56 Meanwhile, the Dietetic Council warned Lemass on 16 April 1942 that this ‘would be very serious especially in growing children’. 57 The council recommended that calcium carbonate be added to the flour to counteract the side effects of the phytic acid. 58 However, Lemass disregarded these findings because there was no concrete evidence to suggest that a calcium deficiency existed in Ireland. Instead, experiments at the Department of Supplies focused on the aesthetic qualities of the bread, noting no dramatic changes to its flavour, colour or shelf-life when it was made with flour extracted at higher rates. 59
The prevalence of rickets in Ireland increased substantially during wartime. A deficiency disease that occurs in growing infants and children, rickets, is associated with a vitamin D deficiency and a lack of calcium. As the disease develops, skeletal abnormalities occur, leading to disturbances in bone growth. 60 In 1942, Dublin paediatricians observed an increase in cases radiologically diagnosed at children's hospitals. 61 Between 1939 and 1941, studies indicated an increase from 10 cases per 1,000 children to 23 cases per 1,000 children. 62 Following this, another Irish investigation coincided with a rickets survey undertaken in England, Wales, Scotland and Northern Ireland by the British Paediatric Association. Some 365 children were randomly selected for examination from the outpatient departments of Dublin's children's hospitals and welfare centres. Patients were mostly children of the poor, though some benefitted from the remittances of a father who had gone to work in England. 63 The incidence of rickets in Dublin had risen from 10 cases per 1,000 children under four years of age in 1939 to a disturbing high of 230 cases per 1,000 children by 1943. 64 Some reports had cases ‘so bad that [children] required orthopaedic treatment to remedy deformities’. 65 To make matters worse, these figures were four times higher than that found in any English city. 66
To protect children against rickets, calcium and vitamin D intakes had to be optimal, making due allowance for substances which might lessen absorption. 67 The main sources of vitamin D in the diet were milk, butter, and eggs. It was accepted that a child should ingest at least 0.75 g of calcium per day which could be obtained from a little over a pint of milk. 68 Despite the fact that 100 per cent extraction flour contained more calcium than white flour, higher quantities of phytic acid prevented its assimilation into the human digestive system. This proved particularly detrimental to public health when it was placed within a context of severe food shortages. 69 In Dublin alone, 40,000 gallons of milk were consumed daily – the equivalent of about half a pint per head of the population. 70 This, coupled with the fact that eggs were a ‘luxury which few poor families [could] afford’ meant that the quick-fix methods of wartime rationing became visually apparent in the bodies of lower-class children. 71 So marked was its prevalence that the chief medical officer, James Deeny, advised examining all junior classes in city schools for rickets and signs of malnutrition. 72 Because of the high incidence of rickets, the Dietetic Council called for a reduction in flour extraction rates to 85 per cent and to fortify flour with calcium. 73
Flour extraction rates also became enmeshed in debates about another growing public health crisis: the rising incidence of tuberculosis. TB is a chronic bacterial disease caused by the growth of bacillus mycobacterium tuberculosis in bodily tissues. 74 While there was a proven epidemiological association between rickets and calcium, there were suggestions as to the possible relationship between calcium and TB. Medical experts Theobald W. T. Dillon and Dr Con Ward asked whether a lack of calcium could weaken one's resistance to a primary TB infection or whether the advanced tertiary case of the disease could be improved by the administration of calcium. 75 Although Greta Jones notes the 1940s as landmark years for the treatment TB, this period also witnessed the swelling of sanatoria at rates that were unmatched by any other. 76 In Dublin alone, numerous doctors were alarmed by an increase in the number of bone fractures in young children while the severity of the onset of TB among the younger age groups proved equally worrying. 77 Both were attributed to calcium deficiency that arose from the removal of calcium from the body by high extraction flour. 78 Home to 20 per cent of the total population, Dublin accounted for over one-quarter of all TB deaths during the war years. 79 This proved alarming when the disease itself was in retreat in most other developed nations. 80
Meanwhile, Britain fortified flour with acid calcium carbonate in 1941. Because of this, the Irish medical profession looked to the advances of the British Ministry of Health as a means of discerning weaknesses found in Ireland. In a letter from Dillon to Dr Ward, Dillon expressed his views on England's rationing system: The rise in the TB death rate which appeared in England during the first two years of this war has in fact been checked with surprising ease during a period of strict rationing, which however was characterised by a determined effort to maintain the calcium intake at the optimum level for all sections of the population by adding calcium to the bread, [and] providing milk for children and expectant mothers.
81
The same cannot be said for Ireland. Extraction rates were not lowered until December 1943 while flour was not fortified with calcium until June 1946. Instead of taking the word of existing British science, both Lemass and MacEntee insisted on doing their own investigations. These investigations took a considerable amount of time. First, the Dietetic Council had to prove a calcium deficiency existed in Ireland. They then had to establish its effects on the incidence of rickets and TB mortality. There were no final conclusions reached as to the whether the increased prevalence of these diseases was because of the flour, a deficiency of vitamin D, a deficient calcium intake or to a combination of these factors. 87 Likewise, the visual precursors of both diseases do not occur overnight while relevant investigations involved a whole host of planning, paperwork and personnel. Although it was not possible to show by animal experiments that calcium influenced the development of TB, apparent links were sufficient to warrant measures that could ensure adequate calcium intake for all sections of the population. Besides, it was believed that the addition of calcium would cause no harmful effects in conditions where deficiency was already apparent. 88 Investigations into appropriate extraction rates and calcium reserves demanded the work of the Dietetic Council and the Emergency Scientific Research Bureau – this also, was time consuming. For instance, the Dietetic Council ran numerous investigations into the dangers of bread made from high extraction flour as well as the use of potatoes in manufacturing bread. This involved surveys of bakeries that were already manufacturing bread with up to 20 per cent potato. 89 Similarly, the Research Bureau awaited results from investigations by the Geological Survey into potential calcium reserves for baking. 90 Even before doing so, both bodies looked to Britain for guidance. 91 The political tensions between Lemass and MacEntee then led to continuous debate over what should be prioritised and when.
Cabinet Debates Surrounding Flour Fortification
Wartime circumstances saw the Department of Industry and Commerce and the Department of Local Government and Public Health attempting to fulfil their basic functions in difficult economic times. The main functions of MacEntee's department lay in health measures designed to combat disease. However, through funding allocations, it was Lemass’ department that was ultimately responsible to fund these measures. Raising extraction rates temporarily relieved the pressures of wartime shortages on Lemass’ department, but this also led to severe health effects on the wider population. Internal struggles to reach compromises on viable solutions resulted in unnecessary delays that ultimately culminated in a rickets epidemic and a higher TB mortality rate. Further, MacEntee himself served as the Minister for Industry and Commerce before Lemass for a short period between 1939 and 1941. Both have been portrayed as continuously at odds with one another, and antagonism between them may have contributed to an inability to find a quick solution, though this view has recently been challenged. 92
In Ireland, the first record of public health concerns raised against high extraction rates was by the Dietetic Council in April 1942 – two months after extraction rates were increased to 100 per cent. From this point onwards, public health arguments in favour of reduced extraction rates were pitched to Lemass in ways that marketed themselves as in the wider interests of the Department of Industry and Commerce. For instance, the Dietetic Council reported that bread made from 100 per cent extraction flour was ‘merely diluted’ as it did not necessarily increase the bread's nutritive value. 93 To get the same nutrition, the consumer would have to eat more of the very thing that Ireland faced difficulties in generating. Additionally, the council noted better keeping properties of bread made from 85 per cent extraction than those of higher extraction. This being so, the council believed that bread made at lower extraction levels was ‘less likely to be wasted’, thereby appeasing demands of the Department of Supplies to conserve wheat reserves in the first place. 94 These arguments were enough to justify reduced flour extraction rates that eventually came about at the end of 1943.
Conscious of the detrimental side effects of high extraction rates, Dr Ward attributed the rise of TB to the concurrent increase in flour extraction and used this as a further argument in favour of flour fortification. In a letter addressed to de Valera in March 1945, Dr Ward explored the possible relationship between calcium deficiency and increased TB mortality. 95 Although he acknowledged that more research into this new line of inquiry was required, he noted further investigations were warranted. With calcium levels lower ‘under inferior economic conditions’, he included a list of death rates to correspond with rising flour extraction rates – the highest increase measured at 1,014 at the time of 100 per cent flour extraction (see Figure 1). 96 He linked the lowering of extraction rates with lower death rates from pulmonary TB. Crucially, this letter was penned against a backdrop rife with medical demand to fortify bread. Less than a month later, it was found that the healing of TB depended much upon the laying down of calcium in the form of a lime in the affected areas, thereby ‘walling off the lesion and affecting a cure’. 97 As far as public health officials were concerned, flour should be fortified at once and any increase in cost should be accepted as a necessary production cost. 98 A very different view prevailed in the Department of Industry and Commerce.
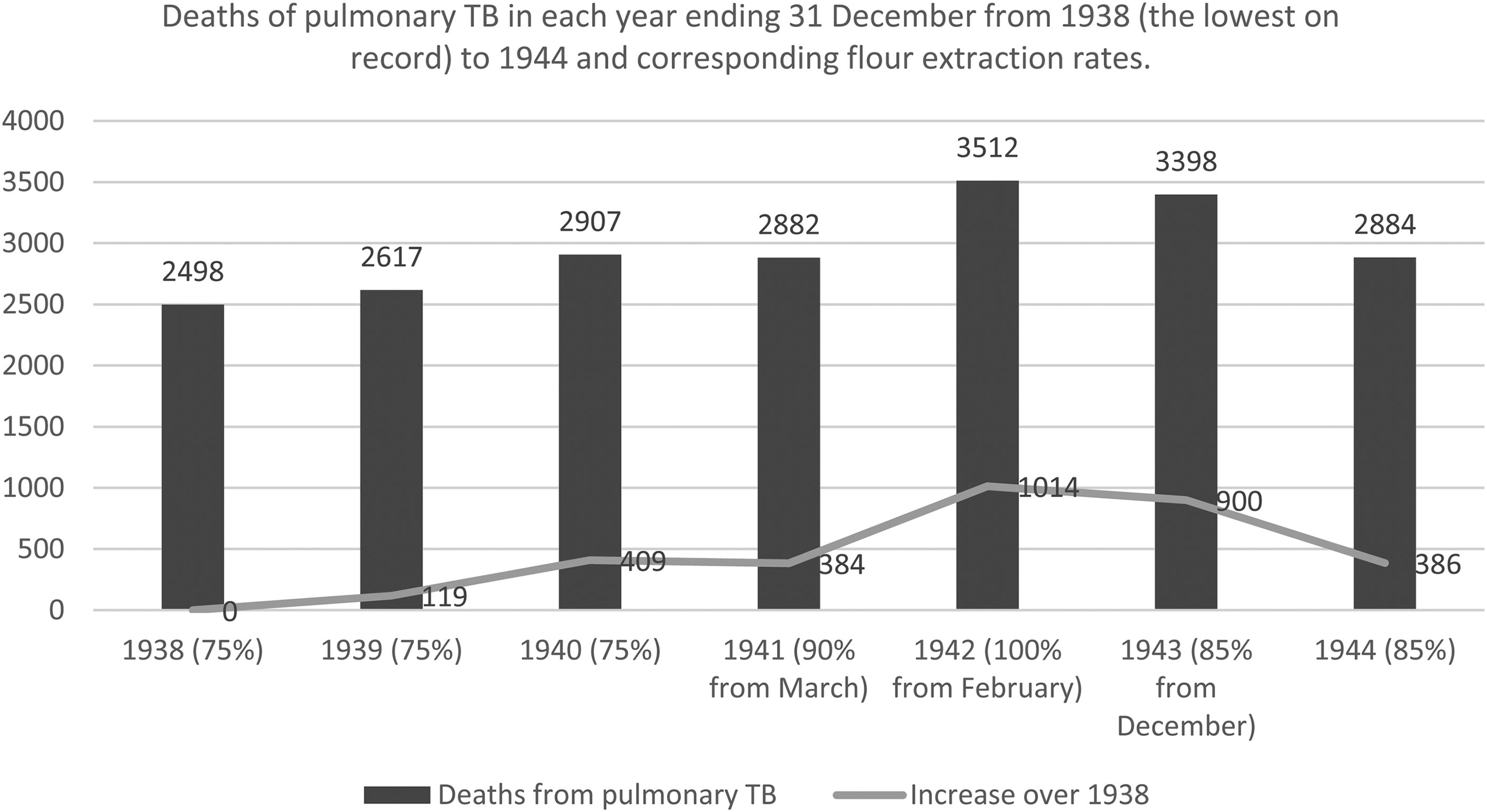
Deaths of pulmonary TB, 1938–1944 and corresponding flour extraction rates.
These arguments and the coincidence of increased TB mortality and higher flour extraction may seem convincing in retrospect, but Lemass was not immediately in favour of flour fortification. From the outset, he placed rickets and TB in a much wider context and asked why the public health regime was so fixated on these diseases over others. He pointed out that mortality rates from heart disease far exceeded the number who died from TB yet he ‘knows no medical authority is in favour of increased calcium intake for persons suffering from heart disease’. 99 There were still over 1,000 small millers whose plants were only capable of producing wheaten meal at the equivalent of 100 per cent extraction. There were also a number of smaller mills used by wheat growers in their own homes. 100 In short, Lemass argued that lowering extraction rates and calcium fortification would impact many firms that did not possess the capacity to change their methods. Further, he was dubious of the benefit in terms of reducing TB mortality and of the insistent prioritisation of TB and rickets as opposed to other diseases.
In response, MacEntee compared fortification to the addition of chemical substances known as ‘improvers’ to flour to improve its appearance without regard for nutritional quality before the war. He argued that calcium, ‘a mineral essential to human life’, should be added to flour without question. 101 In relation to smaller operations, he noted that much of the flour consumed by smaller farmers was consumed by the farmers themselves. 102 The calcium intake of this social group was ‘generally regarded as adequate’. 103 Besides, the popular use of buttermilk and oatmeal among this class meant they were not considered at risk of any deficiency that would necessitate special action. 104 Here, MacEntee's reasoning was that any calcium shortage arising from 100 per cent extraction would be offset by the small farmer's access to other calcium-rich foods.
Rickets and TB were only two of a number of public health concerns during the Emergency, yet their incidence dominated Irish cabinet debates. With little having changed throughout the 1940s, heart disease was the main cause of death accounting for 21.9 per cent of all deaths during the war period (see Table 1). 105 This was followed by senility (14.3 per cent) and cancer (9.2 per cent). 106 As shown, mortality from heart disease rose significantly throughout the war period and would continue to do so for the remainder of the decade. 107 TB mortality figures also rose substantially during the war. Even more specifically, they peaked during 1942–1944. These also happened to be the years when flour was extracted at higher rates (see Table 1). With little done by way of tackling heart disease, Lemass was justified in his bafflement at the public health preoccupation with flour fortification. However, state action only occurred as a delayed response to rising rates of rickets and TB. Evidenced by the rising extraction rates, Lemass was shown to be more interested in dealing with problems directly flared by wartime conditions. In response, MacEntee assumed the role of examining the health effects that this had on the wider population, and this took away from even bigger problems like heart disease. This created a situation in which Fianna Fáil were effectively firefighting in public health as opposed to orchestrating a long-term plan.
Causes of death in Éire, 1939–1945. Figures are taken from the Annual Report of the Registrar-General, 1938–1945.
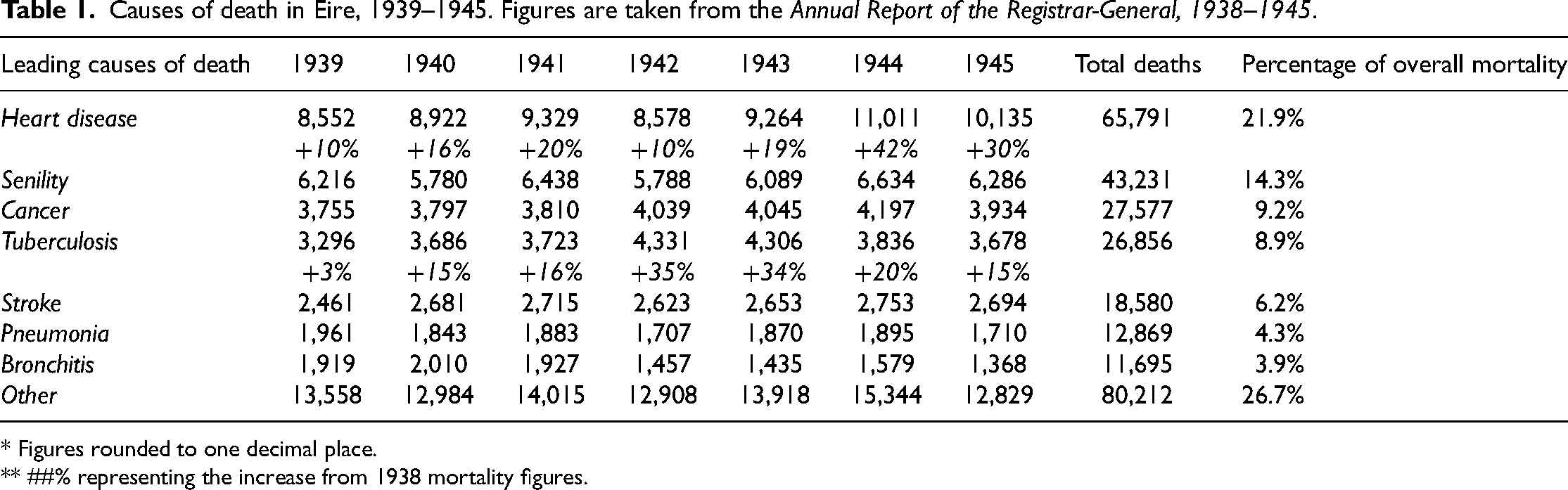
* Figures rounded to one decimal place.
** ##% representing the increase from 1938 mortality figures.
Lemass may have been baffled by the focus on flour fortification and its relationship to TB and rickets but these public health issues had more visibility than heart disease or other senile diseases. In both diseases, physical ill-health was visible. The clinical symptoms of rickets include a bowing of the long bones and short stature. 108 More broadly, the rickets epidemic proved emotive in a country that experienced a proportionately higher infant mortality than most other European countries. 109 Between 1940 and 1944, the infant mortality rate in Dublin increased from 91 deaths per 1,000 births in 1940 to 117 per 1,000 in 1944. 110 In 1943 – the year that flour was extracted at 100 per cent, infant mortality was particularly high at 126 deaths per 1,000 births. 111 This is not to say that rickets was a causative factor in rising infant mortality rates; this has been attributed to premature birth, gastro-enteritis, bronchial disorders and injury at birth. 112 Notwithstanding, any childhood disease proved controversial in a state with relatively high infant mortality. While rickets was not directly associated with child mortality, its presence was recorded in 90 per cent of children worldwide who had died before the age of four in the early twentieth century. 113 Because of this, emphasis was placed on foodstuffs that were essential to the growth of children. This was further alluded to in the nutrition survey. 114 The idea that children represented the future generation may explain why little by way of state action occurred for those suffering from heart disease – a disease that is mostly associated with ageing. Senility and heart disease together accounted for over one-third of all deaths at the time but, as Lemass identified, provoked much less advocacy from the Department of Local Government and Public Health.
TB, a prominent public health concern since the late nineteenth-century, was continuously monitored by the Irish medical profession during the war. Declining in other countries such as Britain and the US, TB mortality in Ireland rose to 147 deaths per 100,000 of the population during the Emergency, levels not seen since the First World War. 115 TB causes weight loss, restricted movement and deformity of the affected joint. 116 For instance, sufferers of pulmonary TB experienced substantial weight loss, sustained coughing, chest pain, episodic chills and sweats. Similarly, a person with spinal TB made sure to guard his movements which would later underpin the ‘hunch-back’ deformity. 117 Like rickets, TB was particularly prominent among children and young people. Listed as the most common cause of death in older children aged between five and fifteen, TB was a major cause of death among adolescents and young adults under the age of 45. 118 When a visible crisis emerged, such as that of rising rickets and TB, the Irish medical profession rallied behind a solution only to find themselves firmly confined by the constraints of rigid government funding strictures.
Both a reduction in extraction rates and the fortification of flour were enacted after several years of advocacy by the Dietetic Council, Deeny and MacEntee. Yet these stories exemplify how economic concerns competed with public health interests in Ireland. Calls for the fortification of flour with calcium were first voiced by the Dietetic Council in 1942, but the issue was shelved for the duration of the war. Lemass only belatedly sanctioned a reduction of flour extraction rates in December 1943 – the easiest of the two options at that time. Reducing extraction rates primarily involved the work of two acting parties: Fianna Fáil and the flour millers. On the other hand, flour fortification not only relied on Fianna Fáil and the compliance of flour millers, but it equally required the identification and testing of existing calcium reserves, the co-operation of relevant businesses and a set of rigid price controls. Notwithstanding, acid calcium phosphate was added at a rate of 24 ounces per 280 lb sack of flour from June 1946 – four years after concerns were first voiced. 119 In the interim, there was a known risk to public health (phytic acid) which resulted in avoidable morbidity and even mortality.
Historically, fortification is a top-down method used to address a population or sub-group population deficiency. Crucially, it is a form of preventative medicine that aims to minimise malnutrition at a future stage. A blanket measure designed to target the entire population, it nevertheless reminds us of just how serious this crisis was. Fortification contrasts, for instance, with the infomercials and flour economy cookbooks issued at the beginning of the war, which prioritised the maintenance of public resources over public health. The consequences of this were warned of, but the Department of Supplies had to balance economic demands with health. Crucial decisions in this juggling act had significant consequences for the health of the poor. Introduced only after the identification of a serious rickets epidemic and a higher TB mortality rate, flour fortification in Ireland's case was unique – introduced instead as a reactionary measure to correct the mishaps made under wartime rationing.
On paper, the calcium deficiency was going to be resolved via flour fortification, albeit a little later than expected. Paradoxically, fortification in Ireland resulted in the ‘medicine’ being moved further away from the population group that needed it most. Poorer households were more likely to consume bread in a higher proportion of their diet than any other class. This is because bread was a ready-cooked food and many poor households had very limited cooking facilities. While the calcium deficiency that arose was most pronounced among this population group, and the health problems of rising rickets and tuberculosis were cited as the main reasons for calcium fortification, doing so naturally increased the cost of the flour. Between 1939 and 1947, the price of flour per stone increased from 2/6 to 4/– (a 60 per cent increase), only to reduce to 2/10 a couple of years later. 120 To make matters worse, pre-war wage levels were not restored until 1949. 121 Here, rising flour costs ultimately reduced access to the ‘treatment’ for the problems that high flour extraction had caused. Fortification was likewise referred to by the wider medical profession as a type of ‘shot-gun’ treatment. 122 The idea was that by ‘scattering shots over the entire population, you hope that a few pellets will hit the individuals needing them’. 123 However, fortification increased the cost of food production and therefore did not prevent the possibility of ‘pointing the gun in the wrong direction and missing the bird entirely’. 124 Nevertheless, its path to the statute books signifies a triumph in medical circles as they were given increased authority in negotiating government policy.
Conclusion
Constrained by financial pressures and the very real threat of war, Fianna Fáil focused on short-term gains (the management of the immediate supply situation) at the expense of long-term public health. The outbreak of war plunged Ireland into a state of economic emergency, and the prioritisation of rickets and TB as opposed to diseases of the elderly may simply be attributed to Fianna Fáil's reaction to issues exacerbated by wartime conditions. Ironically, wheat supplies could have been saved if people ate smaller amounts of bread that had lower rates of flour extraction as opposed to producing high quantities of high extraction brown bread that was neither nutritious nor nice to eat. Here, the Department of Industry and Commerce were reluctant to invest funding into health problems that did not have a quick-fix solution. First, they needed proof that the issue existed. Second, they needed concrete evidence of the severity of the problem. And third, they required a viable working solution before making any decisions on funding allocations. In part, this explains why the Department of Supplies tried to tackle the most visible problems as opposed to engaging in long-term planning. While the Dietetic Council belatedly succeeded with fortification, this was only after the ‘Emergency Proper’ had concluded (1946).
The fact that decisions to reduce extraction rates and fortify flour were only made following proven associations between calcium deficiency, rickets, and TB does incidentally provide us with an effective marker of government strategy. During the early years of the war, the most ‘vivid’ concern for Fianna Fáil was food shortages as the expert medical opinion was consistently side-lined in favour of managing the country's supply chain. Because of this, the advocacy of the medical profession was required to make the consequences of this public health policy more ‘vivid’ by producing evidence of the increased incidence of disease. It was the Dietetic Council that demonstrated the links between calcium deficiency, TB mortality, and the growing crisis of rickets among children. This was embarrassing because it was part of a larger set of health problems among the younger population that made the state look rather backwards compared to the UK that it had recently left. It is only with this information that Fianna Fáil took action to extract flour at lower rates and fortify flour, albeit belatedly. Once wartime pressures eased, Lemass moved his focus back to stabilising supplies. Distancing themselves from what was once a serious health concern, Fianna Fáil appeased the demands of millers through a reduction in flour fortification and reverted to bottom-up methods of encouraging calcium intake like those found in the results of the National Nutrition Survey. 125
Removed from direct combat, wartime nutrition in Ireland posed a different type of problem than that found in other countries. Questions of food proved particularly emotive in a country that was experiencing first-hand the long-lasting impact of the Great Famine less than a century earlier. 126 After the Famine, the consumption of a varied diet was increasingly understood as progress toward civilising the Irish and ‘raising them into more sophisticated beings’. 127 The fact that bread dominated cabinet debates was partly influenced by earlier arguments that the Irish poor were poorly fed following the Famine and reflected the age-old idea of disease as most vividly manifesting among the poor. Ironically, the fortification of bread with calcium increased its cost, thereby moving it further away from poorer population groups.
Then, as now, official healthcare policy struggled to strike a balance between crisis management and effective allocations of public health resources. An insight into the balancing act of public health during a time of crisis seems particularly relevant now as the COVID-19 pandemic continues to distort the public health system with consequences for the prevention and treatment of other diseases. This paper has shown how political short-termism can exacerbate public health problems as symbolised in the black loaf of Emergency Ireland. Rising extraction rates may have provided an immediate pay-off to the management of the country's wheat supply in the short term, but this had devastating effects on long-term health planning. The debates that ensued in Ireland's economic and health departments on what should be spent and where are nonetheless revealing in terms of what constituted ‘health’ and ‘ill-health’. Rickets and TB were two diseases that were strongly linked to existing concerns with childhood and poverty, and so sensitive was the issue of the bread that the words ‘black bread’ were even banned by the censor. While these health issues were eventually addressed by the lowering of extraction rates and flour fortification, this was at the expense of a number of other health issues. Heart disease, rather poignantly, remains the leading cause of death in Ireland.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
I am grateful to acknowledge that this work was jointly supported by Dublin City University's School of History and Geography PhD Studentship and the Irish Research Council, grant number GOIPG/2021/1460; Irish Research Council for the Humanities and Social Sciences (grant number GOIPG/2021/1460).