
Abstract
People often come to work sick – a prevalent behaviour even during public health crises. Integrating trait activation and social role theories, we examine how organisational sickness preventative practices affect workplace anxiety, approach and avoidance motivation for presenteeism, in turn, contributing to male–female differences in presenteeism. We conducted a time-separated study. The results (N = 86 working adults who completed all four waves of the data) supported our moderated mediation model in that organisational sickness preventative practices were beneficial for reducing avoidance motivation to engage in presenteeism for women, but less so for men. These practices were similarly beneficial for reducing workplace anxiety for women, which explained their lower presenteeism compared to men. We performed a cross-sectional replication using only employees who worked in the traditional office at Time 3 (N = 56) and obtained similar findings. Our results offer steps on how to manage presenteeism.
Keywords
1. Introduction
Public health crises, such as annual respiratory infectious disease outbreaks or global pandemics, may be assumed to encourage employees to engage in health protective behaviours and refrain from spreading the illness to others (Moran and Del Valle, 2016). However, the recent COVID-19 pandemic showed this might not always be the case. People still showed up to work even though they had cold-like symptoms, were tested for the virus and advised to self-isolate until the test results came back (Whiteley, 2020). In other words, they engaged in presenteeism – wherein employees turn up to work despite their illness, injuries and other medical conditions (Johns, 2011). Meta-analytic evidence showed presenteeism to be detrimental to sick employees’ own health and productivity (Miraglia and Johns, 2016). Turning up to work sick also is harmful to co-workers, whose fear of contagion explains why employees become disengaged and demotivated when their colleagues (particularly those of the same sex and race) show up to work sick (Luksyte et al., 2015). Employee presenteeism even adversely affects customers’ repurchase and recommendation intentions (Dietz and Zacher, 2022). Given the negative consequences of presenteeism, both academics and practitioners strive to determine how organisations can prevent presenteeism during normal working days as well as during public health crises when the risks to one’s own health and that of others are particularly dire. Furthermore, although both men and women appear to engage in similar levels of presenteeism (Idris et al., 2023; Miraglia and Johns, 2016), women tend to protect their health more than men (Luksyte et al., 2023; Moran and Del Valle, 2016). Hence, we ask whether the effectiveness of any such measure may differ across men and women? We examined this research question during the recent pandemic. However, the theoretical arguments derived from our framework regarding differential implications of organisational sickness preventative practices in curbing presenteeism and its negative consequences for health and productivity extend to normal workdays as well as other public health outbreaks, crises, epidemics and pandemics (Bolino et al., 2024).
Since the recent pandemic, organisations across the globe have been implementing explicit health measures recommended by the World Health Organization (WHO, 2020a) to curb the spread of the virus. Consistent with prior research, we conceptualise these measures as ‘organisational sickness preventative practices’, which capture the extent to which organisations have enacted WHO-recommended guidelines, such as promoting social distancing, wearing masks, frequently disinfecting surfaces, increasing ventilation and washing hands (Probst et al., 2020). Outside the pandemic context, organisations strive to implement similar practices to not just prevent sickness but to promote health and wellbeing by activating health protective behaviours among their employees (Grant et al., 2007). Indeed, the efficacy of such measures and policies stands to be enhanced by curbing presenteeism, thereby limiting the risk of infection from asymptomatic carriers of the virus. In our research, we integrate trait activation theory (Tett and Burnett, 2003; Tett et al., 2021) and gender-related health research (Lithopoulos et al., 2021; Moran and Del Valle, 2016) with research on presenteeism (Johns, 2010) to examine why organisational sickness preventative practices may differentially influence male and female presenteeism.
In doing so, we build on trait activation theory (Tett and Burnett, 2003), which posits that situational cues can activate or accentuate stable characteristics. This theory also emphasises that ‘trait-relevant situations often have a main effect on behaviour [. . .] because they expose individual differences on relevant traits’ (Tett et al., 2021: 201). We argue that organisational sickness preventative practices serve as an environmental cue to prioritise health and, therefore, are likely to decrease presenteeism. Supporting this view, a study has shown a negative relationship between a workplace climate that emphasised the importance of daily health checks, staying at home while sick as well as those that we capture in our research (washing hands, social distancing and mask-wearing) and presenteeism (Probst et al., 2021). We argue that by enacting sickness preventative practices, organisations send signals to their employees about the importance of health and the need to protect it by staying at home when sick. Yet men and women may interpret such health protection signals differently, with women embracing and men ignoring them. We explain these predictions based on research suggesting that women are generally more health-conscious than men (Lithopoulos et al., 2021; Luksyte et al., 2023; Moran and Del Valle, 2016) and are more likely to comply with health and safety protocols (Sharma et al., 2024). Hence, we examine how organisational sickness preventative practices may accentuate this difference, resulting in greater reductions of presenteeism for women than men.
We also examine ‘why’ these differences occur. Identifying the mechanisms underlying the proposed gendered link between preventative practices and presenteeism is critical for understanding what levers organisations should target to minimise male and female presenteeism. Understanding why certain tactics work better for employees of one gender than those of the other will help companies to identify alternative or complementary approaches to achieve the desired result (i.e. lower presenteeism for everyone). Such theory-informed practice is important for not just preventing sickness but promoting health behaviours of all employees irrespective of their gender. The model of dual systems suggests that behaviour is driven by automatic affective systems and controlled cognitive systems (Evans, 2008). We build on this framework by considering the affective and cognitive mechanisms likely to be important for understanding the impact of preventative practices on presenteeism. We examine the cognitive mechanisms of (1) avoidance motivation for presenteeism, which refers to ‘fear of damaging consequences of seeking sick leaves, thus forcing oneself to report to work’ (Lu et al., 2013: 407); and (2) approach motivation for presenteeism, which captures ‘desire to confront the discomfort to abide by one’s work values and beliefs of achievement and loyalty to the profession and interested parties’ (Lu et al., 2013: 407). In terms of affective processes, we examine workplace anxiety, which refers to ‘feelings of nervousness and apprehension about the accomplishment of job tasks’ (McCarthy et al., 2016: 280). Although scholars have used these variables as mediators to explain other relationships in the organisational sciences (Griep et al., 2024; Hillebrandt and Barclay, 2022), with very few exceptions (Laing and Jones, 2016; Wang et al., 2018), researchers have yet to examine these cognitive or affective constructs as potential explanations as to ‘why’ the organisational sickness preventative practices will substantially minimise presenteeism. Doing so promises to advance our theoretical understanding of preventative practices and presenteeism and inform practice – the significance of which is underscored by our expectation of gender differences. In combination, our predictions constitute a moderated mediation model illustrated in Figure 1.
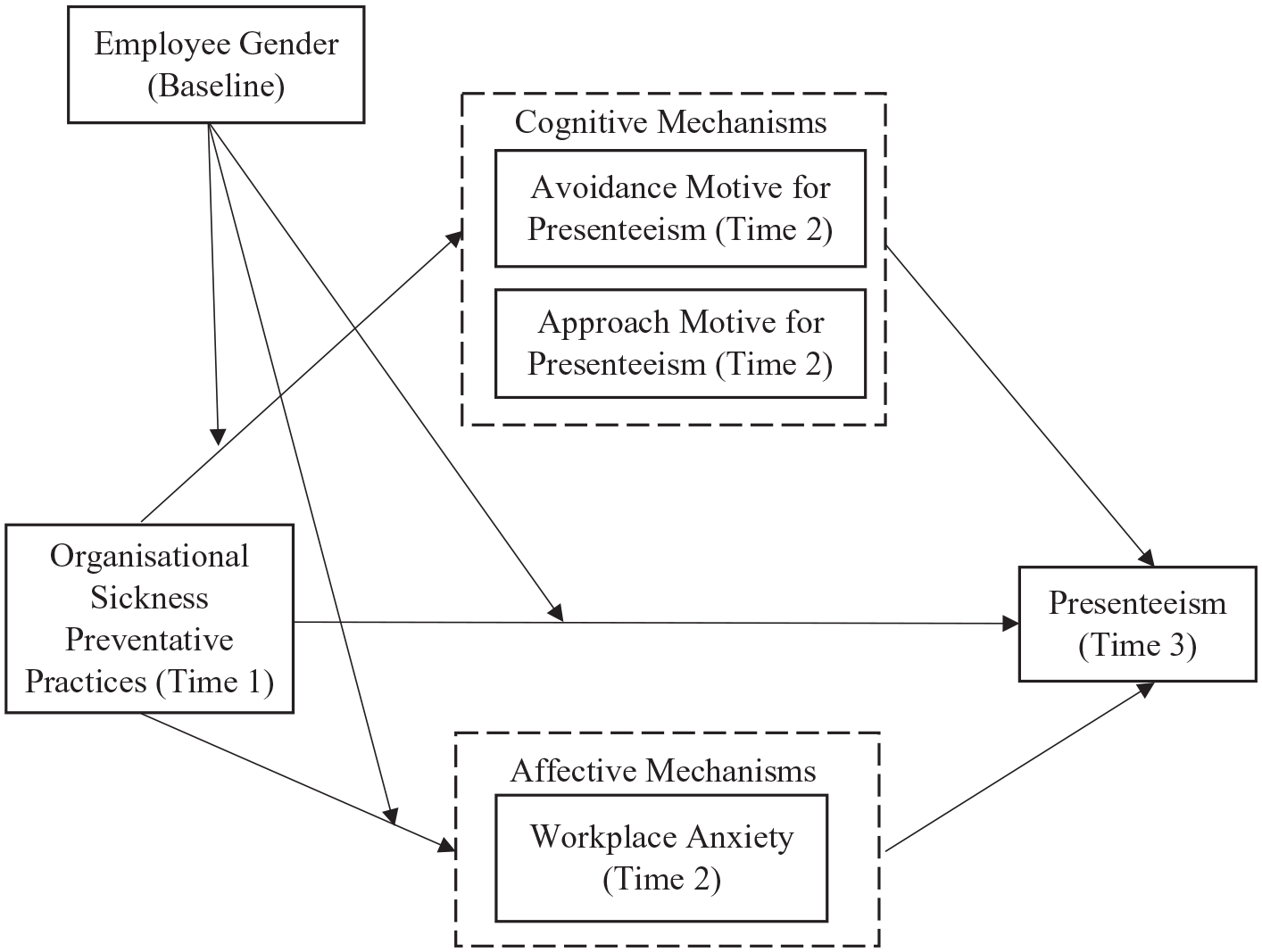
The proposed conceptual model.
2. Theoretical background
Presenteeism is a purposeful and adaptive work behaviour, wherein sick employees must choose between two competing goals, such as ‘preserving health or protecting performance’ (Karanika-Murray and Biron, 2020: 252). Given the risky nature of presenteeism, even under normal circumstances, research has examined its antecedents, including personal, organisational and cultural factors (Ferreira et al., 2015; Lohaus and Habermann, 2019; Miraglia and Johns, 2016). This inquiry has focused on drivers that ‘emphasize the perceived pressure to work despite illness’ (Ruhle et al., 2020: 349) and, thus, can be viewed as prioritisation of performance at work over health. These predictors have proven useful in identifying reasons why people decide to engage in presenteeism: Some are worried about job security, economic loss or burdening co-workers with extra workload (avoidance motivation for presenteeism); whereas others do so because they are passionate about their jobs or believe they should keep up with team schedules (approach motivation for presenteeism; Cooper and Lu, 2019; Lu et al., 2013; Wang et al., 2018). Furthermore, workplace anxiety is expected to be an important motive to engage in presenteeism (Kniffin et al., 2021), particularly during public health crises, when many resources are spent on preserving health while needing to continue to work. We thus specify approach and avoidance motivation for presenteeism and workplace anxiety as cognitive and affective, respectively, mechanisms. We theorise how organisational sickness preventative practices differentially influence these motives for and actual engagement in presenteeism for women versus men.
2.1. Trait activation theory
There are competing goals of preserving health or protecting performance (Karanika-Murray and Biron, 2020) that underlie employee decisions to engage in presenteeism. As such, trait activation theory (Tett and Burnett, 2003; Tett et al., 2021), which explains how environmental cues activate individuals’ underlying aspirations, may help explain how and why organisational sickness preventative practices differentially shape men’s and women’s responses to these practices. Tett and Burnett’s (2003) trait activation theory is based on the interactionist perspective, suggesting that people’s behaviour depends on their individual differences and features of a context that can either suppress or activate the expression of traits. This theory posits that a trait is activated in a work environment that provides trait-relevant cues signalling appropriate behaviour. If a situation offers trait-relevant cues, people behave consistently with their personal preferences (e.g. extroverts will speak up in heated debates). In contrast, when a situation offers trait-irrelevant cues, individuals do not behave according to their predispositions (e.g. conscientiousness is not expressed in higher hierarchy of authority; Luksyte et al., 2024). In addition to trait relevance, the trait activation theory categorises situations based on their potential to shape the expression of traits. The most pertinent categorisation for our inquiry is a facilitating situation, which refers to circumstances that enhance ‘the salience or potency of trait-relevant cues already present’ (Tett et al., 2021: 202). Based on this theory, we conceptualise organisational sickness preventative practices as an environmental cue that activates a health-related goal – that is, such practices will send a strong signal that health, via emphasising sickness preventative practices, is a top priority. We conceptualise these practices as a facilitating situation because they are designed to prevent the transmission of the virus, and thus they are likely to enhance the already present cue about the importance of protecting health (not performance) when it comes to deciding whether to turn up to work while sick. We further argue that this cue will be particularly relevant for women, who (1) are more health-conscious than men (Lithopoulos et al., 2021), (2) prioritise health over performance during presenteeism (Luksyte et al., 2023) and (3) tend to comply with safety protocols more than men (Lithopoulos et al., 2021; Sharma et al., 2024), and as such will more readily respond to such practices.
At face value, the previous arguments suggest that organisational sickness preventative practices – due to their presumed effect on activating a health priority – may dampen performance-related motives for, and in turn, actual engagement in presenteeism. However, we suspect that the process is more complex. Colloquial phrases such as ‘work must go on’ and ‘money must be earned’ emphasise that performance-related goals are still likely to compete with the prioritisation of health. Indeed, research suggests that job insecurity (Lin et al., 2021), disruption of work (van Zoonen and ter Hoeven, 2022), career uncertainty (Howard and Luksyte, 2021) and work pressure (Chong et al., 2020) remain salient (if not accentuated) during public health crises such as global pandemics, and that anxiety and psychological distress is rife (Fu et al., 2021). These issues, combined with the resource intensiveness of organisational sickness preventative practices, wherein employees need to spend additional time and energy cleaning surfaces, maintaining social distance and increasing ventilation, may put further pressure on performance-related goals. We argue that there may be tension between the competing goals of health and performance even when organisational sickness preventative practices are in place. In line with these arguments, research from past pandemics has shown that preventative practices spring women into action more so than men (Moran and Del Valle, 2016). Integrating trait activation theory, emphasising the importance of situational strength and trait relevance on the variability of people’s behaviour under similar circumstances, we argue that the influence of such practices in shaping presenteeism may be moderated by employee gender. We elaborate this argument next, drawing on social role theory.
2.2. Integrating social role theory with trait activation theory
We draw on social role theory (Eagly, 1997) and research related to health prioritisation (Struik et al., 2019), in conjunction with trait activation theory (Tett and Burnett, 2003; Tett et al., 2021) to suggest that organisational sickness preventative practices should be a stronger environmental cue for women than for men and, thus, be more effective at reducing presenteeism and its motives for women. Women are more health-conscious than men (Luksyte et al., 2023; Moran and Del Valle, 2016) – a finding that may be explained by social role theory (Eagly, 1997). This theory explains how gender stereotypes, or generalised beliefs about gender roles, influence others’ perceptions of men and women. Descriptive stereotypes refer to generalised beliefs about how men and women typically ‘act’, whereas prescriptive stereotypes capture generalised beliefs about how men and women ‘should’ behave (Heilman, 2012; Koenig, 2018). As such, women are typically portrayed as communal or nurturing and hence are expected to engage in communal behaviours such as helping, adapting or taking care of others (Carpini et al., 2023). In contrast, men are stereotypically described as agentic or decisive and hence are expected to engage in agentic behaviours such as leading others, innovating and taking risks (Heilman, 2012; Luksyte et al., 2018). According to social role theory, such gender stereotypical expectations influence others’ perceptions of the same work behaviours a man or a woman displays. This theory also assumes that both women and men are aware of and tend to internalise these deeply ingrained and socially shared gender role stereotypes, ‘especially if situational cues make these aspects particularly accessible’ (Eagly and Karau, 2002: 560). Such internalised stereotypes have been shown to shape men’s and women’s own behaviour (Aarntzen et al., 2023; Phuong et al., 2023). For women, internalised communality may be associated with self-care and other care. In contrast, for men, internalised agency and ‘being tough’ have implications for health-compromising behaviours and reticence to seek help. Indeed, women tend to demonstrate more health-protective behaviours than men, such as seeking professional medical health during sickness (Bayram et al., 2016). Women are less likely than men to engage in health-compromising behaviours such as illicit drug use (Struik et al., 2019). Finally, health protection motives are stronger among women than men (Luksyte et al., 2023).
When integrating this scholarship with trait activation theory – which suggests that trait-relevant situational cues activate stable tendencies, thereby prompting trait-consistent states and behaviour (Tett and Burnett, 2003; Tett et al., 2021) – we argue that organisational sickness preventative practices – as an environmental cue to prioritise health – should be more influential for women than men. These practices should thus be more likely to dampen our theorised explanatory motives for and actual engagement in presenteeism for women relative to men. To our knowledge, previous research has not theorised such a relationship, but empirical data provide indirect support. For instance, women have demonstrated higher participation rates than men in response to workplace wellness programmes (Ott-Holland et al., 2019; Robroek et al., 2009). In the general population, but relevant to pandemics, Moran and Del Valle’s (2016) meta-analysis showed that women were more likely than men to adopt non-pharmaceutical protective behaviours such as avoiding crowds and wearing facemasks in response to public health campaigns for managing respiratory diseases. During the pandemic, women have reported higher intentions to follow government recommendations and engaging in more physical distancing than men (Lithopoulos et al., 2021); there was also a higher correlation between safety protocols and being a female (Sharma et al., 2024).
Trait activation theory (Tett and Burnett, 2003; Tett et al., 2021) emphasises the importance of situational relevance for facilitating trait-relevant behaviours. Social role theory (Eagly, 1997; Eagly et al., 2020) explains how gender stereotypical expectations differentially influence men’s and women’s responses to the same situational cues. Integrating these two theories, we go beyond these empirical data, which concern compliance with health-related initiatives. In doing so, we examine the differential impact of organisational sickness preventative practices for men and women on cognitive and affective motives for turning up at work sick during a pandemic, as well as actual engagement in such risky presenteeism behaviour. From the trait activation theory perspective, these practices should more strongly activate the health priority in women, which should dampen their motives to engage in presenteeism. By triggering the importance of protecting health, these practices will weaken women’s concerns that their supervisors will think badly of them for missing work due to their ill-health – an example of avoidance motivation for presenteeism. Being reminded by these practices of the importance of protecting health, women will also be less likely to engage in presenteeism out of ‘good reasons’ such as showing work commitment and loyalty to their profession or altruistic desire to keep up with team schedule – examples of approach motivation for presenteeism (Lu et al., 2013). Finally, the implementation of organisational sickness preventative practices will likely facilitate the already present environmental cue about health (and not performance) being a priority during the pandemic, and women will likely embrace this cue more readily than men due to health prioritisation of the former than the latter (Luksyte et al., 2023). As such, enacting these practices will decrease women’s workplace anxiety, which stems from internalised pressures to spend more time and energy on disinfecting surfaces, maintain physical distance from others and wash hands instead of accomplishing work tasks. Due to the activation of health prioritisation, women are less likely to experience workplace anxiety than men. For men, who are not expected to prioritise health to the same extent as women, these policies should have a less profound impact on their motives and subsequent presenteeism. Based on these arguments, we propose the following hypotheses:
Hypothesis 1. Employee gender moderates the relationship between organisational sickness preventative practices and presenteeism such that this relationship is more negative for women than for men.
Hypothesis 2. Employee gender moderates the relationship between organisational sickness preventative practices and (a) avoidance motivation for presenteeism, (b) approach motivation for presenteeism and (c) workplace anxiety such that these linkages are more negative for women than for men.
Hypothesis 3. The indirect relationships between organisational sickness preventative practices and presenteeism via (a) avoidance motivation for presenteeism, (b) approach motivation for presenteeism and (c) workplace anxiety, are moderated by employee gender such that these indirect linkages are more negative for women than for men.
3. Method
3.1. Participants and procedure
We recruited 520 employees 1 through Mechanical Turk or MTurk (n = 289) and Microworkers (n = 231) crowdsourcing platforms where participants complete surveys. For the MTurk sub-sample, we specified that participants had to have an approval rate of 95% or higher and had completed at least 100 research studies. Most of our participants (91%) resided in the United States at the time of our data collection, the rest (9%) were in Australia. 2
Our design represents four waves of data collection (Baseline, and Times 1–3). We had serendipitously collected relevant data just prior (i.e. early February 2020) to the declaration of the COVID-19 pandemic, providing an opportunity to control for pre-COVID-19 (this time point is hereafter referred to as ‘Baseline’) presenteeism. We then employed a three-wave design with time-separated measures, starting in May 2020 (i.e. shortly after WHO (2020b) declared the COVID-19 pandemic on March 12th) to examine our relationships of interest during the pandemic as desired, while also reducing common method variance (CMV). We separated measurement occasions by 2 months (Time 1 = May; Time 2 = July; Time 3 = September) to maximise the benefits of time-separated measurements of focal variables for reducing CMV (Baseline = controls; Time 1 = independent variables (IVs); Time 2 = mediators; Time 3 = dependent variables (DVs)), while also collecting data as quickly as possible so we could test our hypotheses during the height of the pandemic. Of the 520 participants who responded at Baseline, 207 responded at Time 1 (May; 40% response rate); 154 responded at Time 2 (July; 74% response rate) and 120 responded at Time 3 (September; 78% response rate). At each time point, we asked participants to provide their MTurk or Microworkers ID, which we used to merge the data across four waves. There were 86 people who completed the surveys at all waves (17% response rate).
All 86 participants 3 were employed with various employment arrangements, including 89.5% full-time and 10.5% part-time. The sample was gender-balanced (52% men) with a mean age of 39 years (SD = 10.10). In terms of race, 79% were White, 8% Black, 8% Asian and 5% other. On average, participants had 16 years of overall work experience (SD = 10.74) and 10 years of industry experience (SD = 8.82); and 7 years (SD = 6.81) of tenure in their current organisation.
3.2. Measures
All measures, if not indicated otherwise, were rated on a 5-point scale (1 = strongly disagree to 5 = strongly agree).
We measured ‘organisational sickness preventative practices’ at Time 1 with nine items we developed for this research based on the Centre of Disease Control and Prevention (CDC CfDCaP, 2020) guidelines on how to prevent the spread of COVID-19. We asked participants to indicate the extent to which their organisation ‘has put the following social distancing and hygiene practices in place in response to the
We dummy-coded ‘gender’ with 0 = male and 1 = female.
We measured ‘avoidance and approach motivation to engage in presenteeism’ at Time 2, with the scales (five and four items, respectively) developed by Lu et al. (2013). This measure asks participants to indicate why they engage in presenteeism, and consistent with our time-separated measurement design, we asked them to respond in relation to the time since the Time 1 survey. Specifically, items were preceded with the following lead-in: ‘Since early May 2020, when you continued working even though you were sick or not feeling well, you did so because . . . ’. Example items are: ‘I worried that I might lose my job’ (avoidance; α = 0.91) and ‘I believed that I should keep up with the team schedule’ (approach; α = 0.84).
We measured ‘workplace anxiety’ at Time 2 with an eight-item scale (McCarthy et al., 2016). As with approach and avoidance motivations, we measured this construct in relation to the time since the Time 1 survey. A sample item is: ‘Since early May 2020, I have felt anxious that I will not be able to perform my job duties in the time allotted’ (α = 0.96).
We measured ‘presenteeism’ at Time 3 with a two-item scale (Lu et al., 2013). Consistent with our time-separated measurement design, we asked participants to respond to the items in relation to the time since the Time 2 survey, that is, ‘Since early July 2020 . . . ’. An example item is: ‘Although I had physical symptoms such as a headache or backache, I still forced myself to continue to work’ (α = 0.86).
3.2.1. Control variables
We controlled for pre-COVID-19 presenteeism and COVID-19-responsive leave policies. We controlled for the ‘pre-COVID-19 presenteeism’ in all analyses involving presenteeism so that we could examine the unique impact of organisational sickness preventative practices and proposed mechanisms on presenteeism beyond the level of presenteeism that participants tended to engage in prior to the pandemic. We measured this control variable in the Baseline survey, using the same presenteeism items as used in the Time 3 survey, preceded by the temporal frame of ‘in the past twelve months’ (α = 0.78). We controlled for ‘COVID-19-responsive leave policies’ because such initiatives could also signal a commitment to preventing the spread of COVID-19 and thus relate to presenteeism via the specified mediators. We measured this variable in the Time 1 survey by asking participants to indicate whether their organisation ‘has provided any extra leave allowances or benefits in response to COVID-19’. We also control for the existence of ‘formal paid leave’ by asking participants whether their organisation had ‘a formal paid leave policy that they were eligible for?’ We used the same response options for both these questions such as 0 = no, 1 = yes. Finally, given our sample was both US and Australian, we controlled for location. 4
4. Results
Table 1 reports the descriptive statistics and correlations. First, we examined differences in presenteeism levels before versus during the pandemic. As might be expected, independent samples test showed that presenteeism levels reported during the pandemic (M = 2.39, SD = 1.29) were significantly lower than pre-COVID-19 presenteeism (M = 3.70, SD = 0.98; t (142.66) = 10.19, p < 0.001). This behaviour was still evident, which underscores the importance of examining the relationship between organisational sickness preventative practices and presenteeism. To examine the impact of our sample size (N = 86 complete cases and N = 520 with data at any singular time point), we used G*Power (Faul et al., 2007) to conduct a post hoc power analysis of our ability to detect gender differences of organisational sickness preventative practices for presenteeism. Using these parameters (N = 86, partial η 2 = 0.10, α = 0.05), we calculated the post hoc power being 0.86, which demonstrates sufficient power for our study.
Descriptive statistics and correlations.

N = 520–120. aB = Baseline (February 2020); T1 = Time 1 (May 2020); T2 = Time 2 (July 2020); T3 = Time 3 (September 2020); b0 = Australia, 1 = USA; c0 = male, 1 = female; *p < .05, **p < .01.
Second, we conducted a series of confirmatory factor analyses (CFA) to examine the distinctiveness of the self-reported variables. We used MPlus (Muthén and Muthén and Muthén, 2010) to fit five measurement models. Based on the recommendations for suitable fit indexes (Hu and Bentler, 1999), the six-factor model, wherein all the variables, namely, baseline presenteeism, organisational sickness preventative practices, avoidance and approach motivation to engage in presenteeism, workplace anxiety and presenteeism, loaded onto their respective factors, indicated acceptable fit to the data (χ2 = 830.29, df = 390; root mean square error of approximation (RMSEA) = 0.05; comparative fit index (CFI) = 0.88; Tucker Lewis index (TLI) = 0.86). This model fit the data better than alternative measurement models such as: (1) a five-factor model wherein avoidance and approach motivation were combined into one factor (χ2 = 956.13, df = 395, RMSEA = 0.05, CFI = 0.84, TLI = 0.83; △χ2 = 125.84, df = 5, p < 0.01); (2) a five-factor model wherein avoidance motivation and workplace anxiety were combined into one factor given their sizable correlation of r = 0.73, p < 0.01 (χ2 = 1031.07, df = 395, RMSEA = 0.06, CFI = 0.82, TLI = 0.80; △χ2 = 200.78, df = 5, p < 0.01); (3) a four-factor model in which variables measured at the same time were combined into respective factors (χ2 = 1218.06, df = 399, RMSEA = 0.06, CFI = 0.77, TLI = 0.75; △χ2 = 387.77, df = 9, p < 0.00); and (4) a one-factor model wherein the variables loaded onto one factor (χ2 = 2102.48, df = 405, RMSEA = 0.09, CFI = 0.52, TLI = 0.49; △χ2 = 1272.19, df = 15, p < 0.00).
4.1. Hypothesis testing
We tested our hypotheses using the IBM SPSS Statistics 25 macro (Model 8) developed by Hayes (2017). This approach allows us to examine the conditional indirect effects in moderated mediation models with multiple mediators by obtaining bias-corrected bootstrapped confidence intervals (CIs) for conditional indirect effects. Using this approach, we first examined the top half of the model depicted in Figure 1 (see Table 2), assessing the direct effects of moderation predicting presenteeism (H1) and the proposed mediators (H2a–H2c). Consistent with Hypothesis 1, employee gender moderated the relationship between organisational sickness preventative practices and presenteeism (B = –0.89, SE = 0.38, t = –2.35, p = 0.02). To probe this interaction, we plotted the simple slope regression lines of presenteeism regressed on organisational sickness preventative practices for men and women. As shown in Figure 2, for women, this relationship was more negative (B = –0.68, p = 0.01) than for men (B = 0.21, p = 0.44). Thus, Hypothesis 1 was supported.
Moderated mediation results.

N = 86. aB = Baseline (February 2020); T1 = Time 1 (May 2020); T2 = Time 2 (July 2020); T3 = Time 3 (September 2020); b0 = Australia, 1 = USA; c0 = male, 1 = female; Bootstrap sample size = 5000. *p < .05, **p < .01.
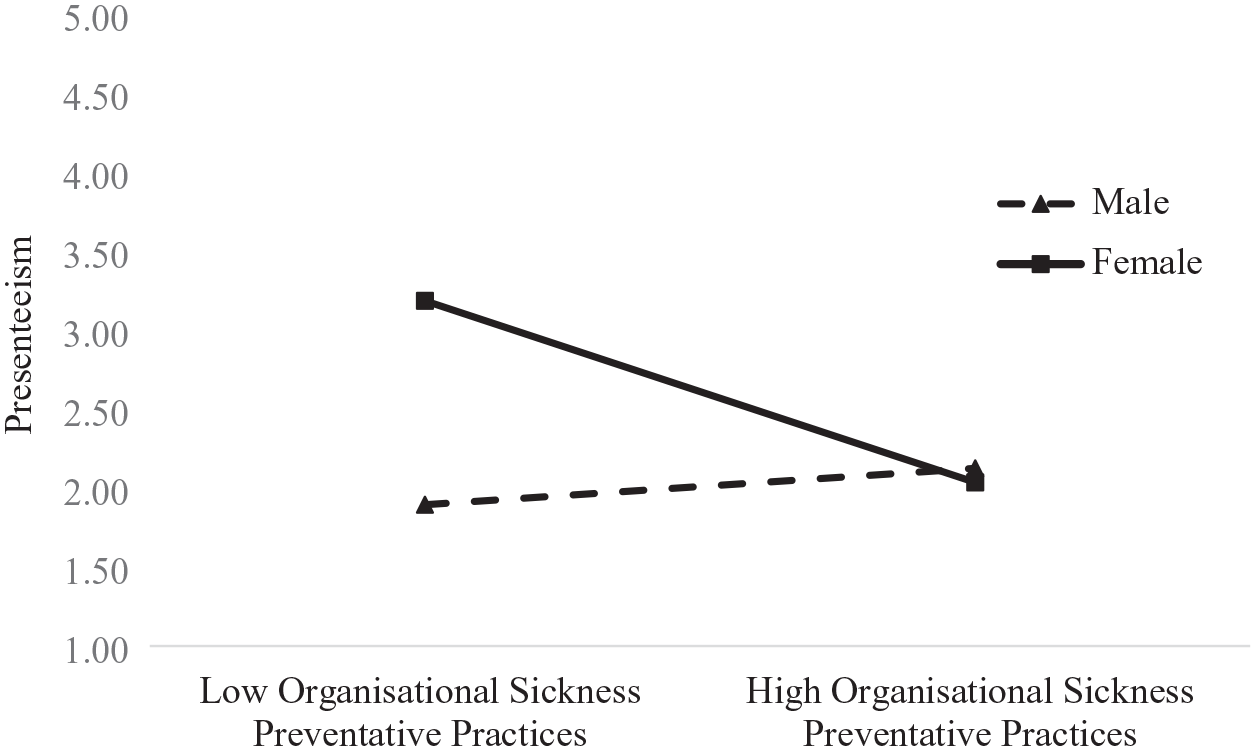
The interactive effects between organisational sickness preventative practices and employee gender in predicting presenteeism.
As predicted by Hypothesis 2a, employee gender moderated the relationship between organisational sickness preventative practices and avoidance motivation to engage in presenteeism (B = –0.83, SE = 0.34, t = –2.47, p = 0.02). As shown in Figure 3, for women, this linkage was more negative (B = –0.50, p = 0.04) than for men (B = 0.33, p = 0.19). Contrary to Hypothesis 2b, employee gender did not moderate the relationship between organisational sickness preventative practices and approach motivation to engage in presenteeism (B = –0.46, SE = 0.30, t = –1.50, p = 0.14). Consistent with Hypothesis 2c, employee gender moderated the relationship between organisational sickness preventative practices and workplace anxiety (B = –1.24, SE = 0.32, t = –3.82, p < 0.01). As illustrated in Figure 4, for women, this linkage was more negative (B = –0.64, p = 0.01) than for men (B = 0.60, p = 0.02). Thus, Hypotheses 2a and 2c received support; Hypothesis 2b was not supported.
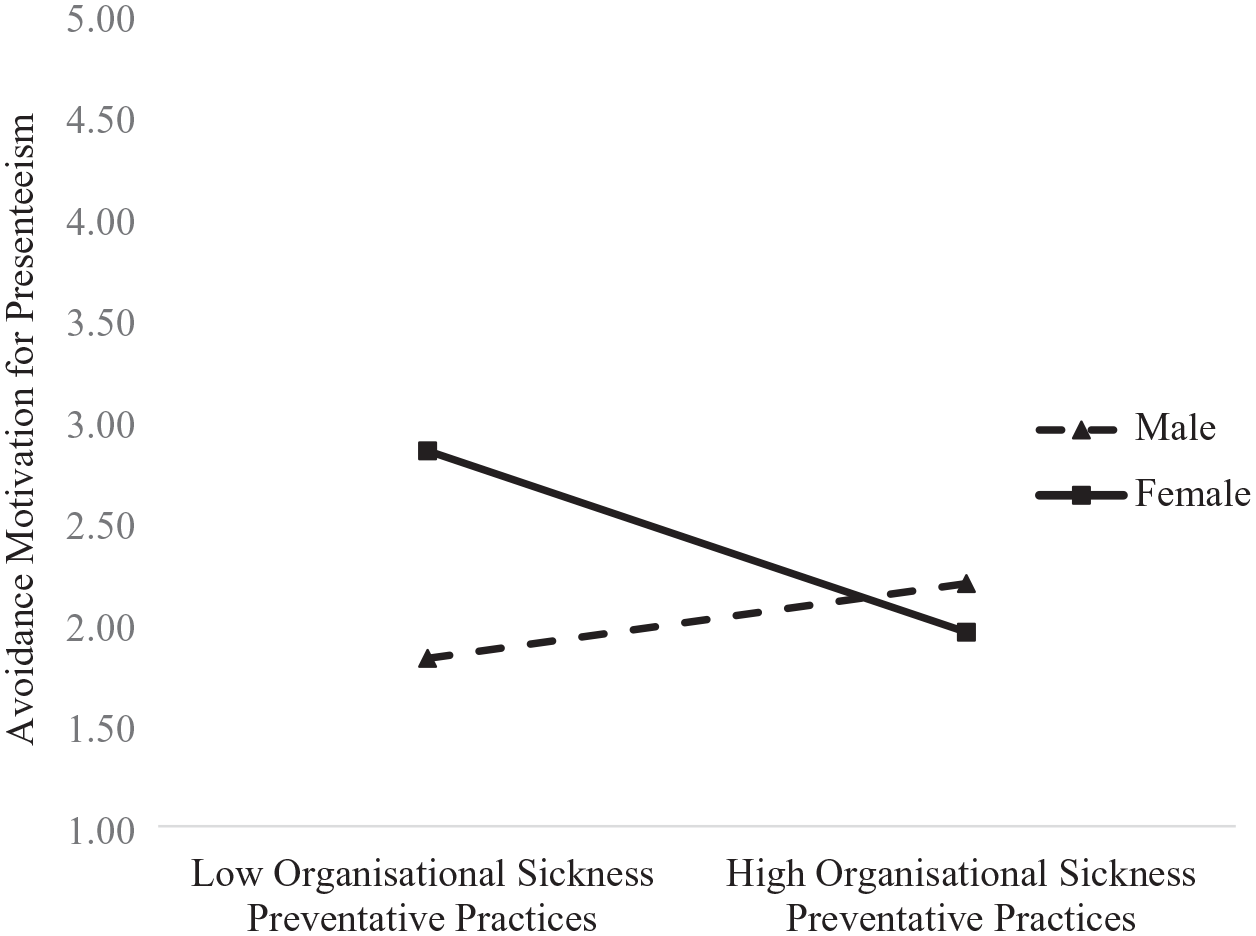
The interactive effects between organisational sickness preventative practices and employee gender in predicting avoidance motivation for presenteeism.
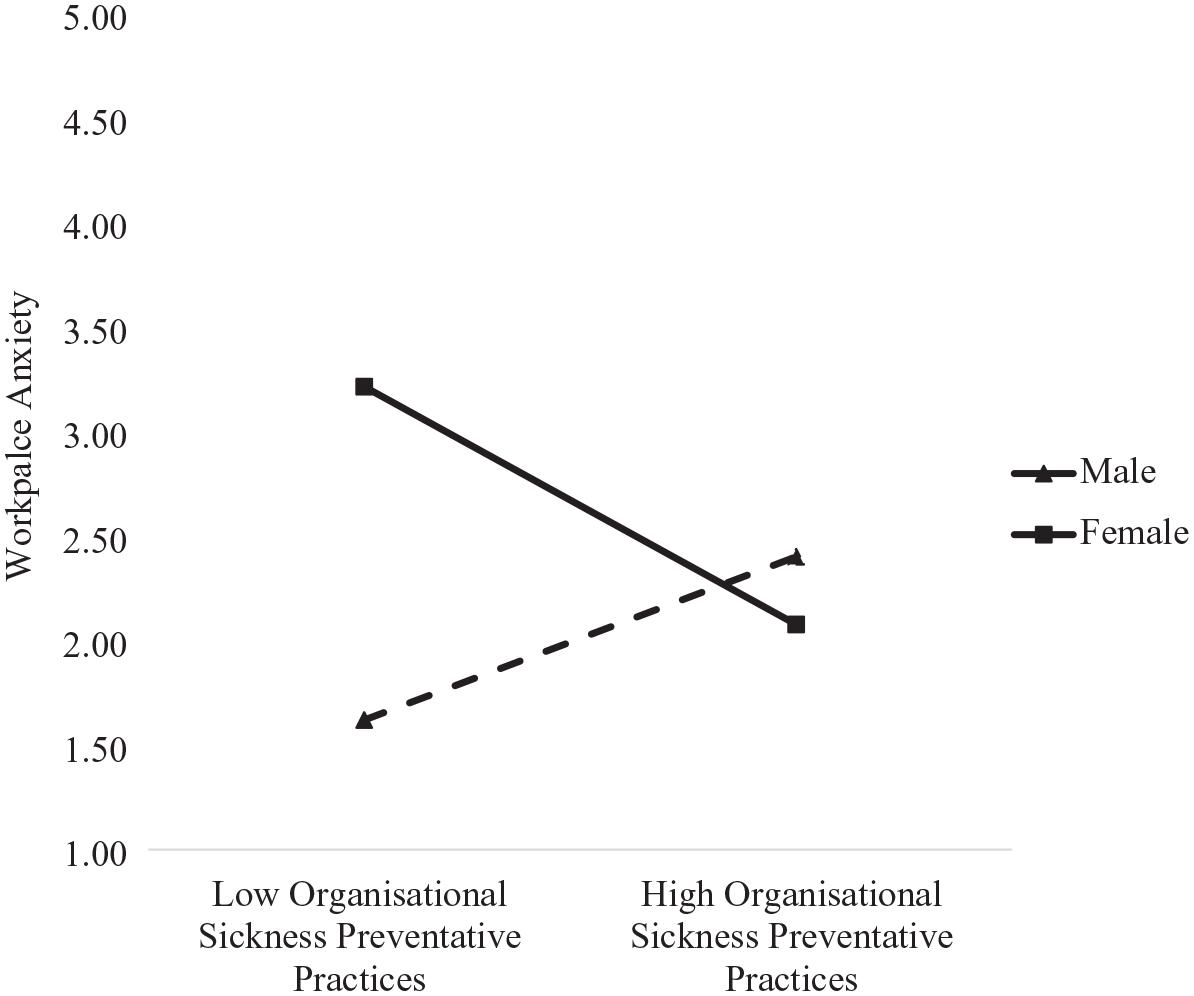
The interactive effects between organisational sickness preventative practices and employee gender in predicting workplace anxiety.
Hypothesis 3 represents moderated mediation, such that the conditional effects (i.e. moderated by employee gender) of organisational sickness preventative practices on presenteeism are mediated by (1) avoidance motivation for presenteeism (H3a), (2) approach motivation for presenteeism (H3b) and (3) workplace anxiety (H3c). These indirect effects are hypothesised to be more negative for women, representing first-stage and direct effects moderation. When examined together in one model, out of the three proposed mediators, the moderated mediation index was only significant for workplace anxiety as a mediator (Index = –0.47, 95% CI = [–1.23, –0.02]; see Table 3). As expected, the indirect effect (via workplace anxiety) between organisational sickness preventative practices and presenteeism was more negative for women (Estimate = –0.25, 95% CI = [–0.75, –0.004]) than for men (Estimate = 0.23, 95% CI = [0.003, 0.61]). These results indicate that the organisational practices designed to curtail the spread of the sickness proved effective in reducing workplace anxiety for women, who, as a result, engaged in less presenteeism. Contrary to Hypotheses 3a and 3b, the moderated mediation indices were not significant for either avoidance motivation for presenteeism (Index = 0.02, 95% CI = [–0.40, 0.37]) or approach motivation for presenteeism (Index = –0.04, 95% CI = [–0.22, 0.10]) as mediators. Hence, Hypotheses 3a and 3b did not receive support, whereas Hypothesis 3c was supported.
Conditional indirect effects of organisational sickness preventative practices on outcomes.

N = 86. MMI = moderated mediation index. 95% Confidence intervals are in brackets, values in boldface do not overlap with zero.
4.2. Follow-up exploratory analyses
We argue that our conceptual model applies to all employees irrespective of whether they work at home or in the physical workspace. This is because organisational sickness preventative practices send a health prioritisation signal to all employees, irrespective of whether they contemplate physically coming to a workplace or working from home when they are sick. As such, we included both office and non-office workers in the analysis for a more comprehensive test of hypotheses. However, given the pandemic context and associated relevance of contagious disease, one may question whether these would hold for people who continued working in the office through the pandemic given the strong nature of that situation, according to trait activation theory (Tett et al., 2021). Accordingly, we conducted follow-up exploratory analyses using a sub-sample of employees who reported working on site. In particular, at Time 3, we asked our participants: (1) whether they worked from home or in the workplace (traditional office/ shop/ work location) in July (Time 2 data collection); (2) whether that work arrangement changed in September (Time 3 data collection); and (3) if so, to clarify how their work arrangement had changed (work from home vs in the workplace). Based on the answers to these three questions, 56 employees said they worked from the office or a physical workplace at Time 3 (the remaining 58 who responded to these questions indicated that they worked from home). Using this sub-sample of working in the office employees (N = 56), we examined our proposed moderated mediation model. Notably, given the small sample size, we tested each mediator separately and without control variables to preserve power. The moderated mediation index was not significant for avoidance motivation as a mediator (Index = –0.31, 95% CI = [–1.16, 0.24]). Notably, the moderated mediation index was significant for approach motivation as a mediator (Index = –0.43, 95% CI = [–1.07, –0.01]). The indirect relationship between organisational sickness preventative practices was more negative (albeit non-significant) for women (Estimate = –0.07, 95% CI = [–0.32, 0.14]) than for men for whom this link was positive and significant (Estimate = 0.36, 95% CI = [0.01, 0.85]). The moderated mediation model held for workplace anxiety as the mediator, as indicated by the significant moderated mediation index (Index = –0.66, 95% CI = [–1.70, –0.08]). Specifically, for women, the indirect effect (via workplace anxiety) between organisational sickness preventative practices and presenteeism was more negative (Estimate = –0.28, 95% CI = [–0.94, –0.03]) than for men (Estimate = 0.38, 95% CI = [0.02, 0.92]). The significant mediating role of workplace anxiety, based on the sub-sample of employees who worked in the physical location of their work, was consistent with the findings of our full sample of employees, who both work from home and in the workplace. The sub-sample’s findings indicated that the organisational sickness preventative practices increased approach motivation for men, who, in turn, were more likely to engage in presenteeism.
5. Discussion
Integrating trait activation theory (Tett and Burnett, 2003; Tett et al., 2021) and research on gender differences in health-related behaviours (Luksyte et al., 2023; Moran and Del Valle, 2016; Struik et al., 2019), we examined how organisational sickness preventative practices might differentially influence male and female motives for, and engagement in presenteeism. Using a time-separated measurement design, spanning four waves of data starting in February 2020 (before WHO declared COVID-19 a pandemic) and ending in September 2020, when countries across the world experienced second waves of infection, we showed that the impact of these practices on curtailing presenteeism depended on employee gender. Organisational sickness preventative practices reduced avoidance motivation to engage in presenteeism and workplace anxiety for women more so than for men. Furthermore, the latter affective mechanism explained why the sickness preventative practices reduced presenteeism more so for women. Notably, these results held in a sub-sample of employees who continued working in the workplace throughout the pandemic.
5.1. Theoretical implications
Trait activation theory (Tett and Burnett, 2003; Tett et al., 2021) proved useful for understanding how and why organisational sickness preventative practices can differentially influence male and female presenteeism. This theory explains how environmental cues can encourage the expression of certain traits (Mohr et al., 2022), particularly if these situations are trait relevant. This theory also distinguishes between various types of contextual features depending on their activation potential (Tett et al., 2021). Using the logic of this theory, we conceptualised sickness preventative practices as a facilitating situation because such practices enhance the already salient cue – the importance of health (as opposed to performance). When sick, employees need to decide whether to prioritise performance by engaging in presenteeism, or protect their health by staying home (Miraglia and Johns, 2021). Integrating these competing motives underlying presenteeism with trait activation theory, we showed that, although organisational practices such as promoting social distancing, disinfecting surfaces and wearing face masks are designed to curtail the spread of the sickness for all employees, they proved more effective for those whose preferences were likely aligned with the underlying cues. Women were particularly responsive to these practices, which is consistent with the conjecture that the practices activated an internalised focus on health that is more salient for women than men (Luksyte et al., 2023; Moran and Del Valle, 2016). Extending this situational trait relevance tenet (Tett et al., 2021) to public health crises, our research unpacked why organisational practices may differentially influence presenteeism – a potentially risky behaviour under normal circumstances and particularly during public health crises such as epidemics and pandemics. This suggests public policy campaigns should be aware of these differential effects for men and women, who, in accordance with their different social roles, may prioritise health differently.
Our results may also contribute to research and scholarship on presenteeism (Cooper and Lu, 2019) by unpacking why these organisational practices differentially influenced presenteeism of men and women. Building on and extending scholarship that argues people engage in presenteeism either out of job concerns or job commitment (Lu et al., 2013), we showed that worry about not getting work done (McCarthy et al., 2016) was a powerful motive for why people engaged in presenteeism even during the pandemic. Notably, when examined separately, both avoidance motivation for presenteeism and workplace anxiety explained how and why the organisational sickness preventative practices reduced presenteeism of women. Yet when examined together, workplace anxiety was the sole significant mediator. When sick people contemplate presenteeism, they need to choose whether they preserve health or protect performance (Cooper and Lu, 2019; Karanika-Murray and Biron, 2020; Lohaus and Habermann, 2019). It appears that during a public health crisis such as a pandemic, these competing goals and motives are still salient – by staying at home, sick people preserve health, yet they risk losing a job or falling behind in work, which is a widely held concern during a pandemic (Lin et al., 2021). Our findings were consistent with our arguments that organisational sickness preventative practices signal to employees the importance of prioritising health. We also conjecture that women tend to be more health-conscious than men and thus should be particularly sensitive to this environmental signal. The reduced workplace anxiety in response to the implementation of these practices for women, and subsequent reduction in presenteeism, highlights the importance of aligning public health campaigns with individual health priorities.
Our research also provided theoretical insights about why men tended to engage in more presenteeism than women. The results of our follow-up exploratory analyses, which were based on a sub-sample of employees who worked in the physical workspace, showed that men responded to organisational sickness preventative practices with more presenteeism because of approach motivation, which captures beliefs that despite sickness, men should ‘persevere’, ‘be loyal to the customers or profession’ or ‘keep up with the team’ (Lu et al., 2013). From the social role theory perspective, organisations may inadvertently encourage male presenteeism by activating their internalised agentic gender expectations of ‘being tough and a loyal team player’. Such internalised external pressures driving behaviours are similar to introjected motivation, which refers to regulation that ‘is within the person but is a relatively controlled form of internalised extrinsic motivation (e.g. I work because it makes me feel like a worthy person)’ (Gagné and Deci, 2005: 334). If organisations strive to discourage male presenteeism they may need to explicitly address this approach motivation for presenteeism as well as conceptually similar but novel, unexplored mechanisms such as introjected motivation. To minimise approach motivation for presenteeism of all employees (and of men in particular), managers ‘need to affirm their work ethics but at the same time resocialize them the value of rest and recovery’ (Lu et al., 2013: 414). Furthermore, reasons for introjected regulations are to avoid guilt or feel worthy (Gagné and Deci, 2005). As such, organisations may focus on addressing these feelings of guilt that men may experience by feeling pressured to come to work. They may do so because it has been theorised that during presenteeism men strive to protect their performance even at the expense of their health (Luksyte et al., 2023). So, organisations can discourage presenteeism among men by explicitly addressing attendance pressure as well as emphasising that work goals can be accomplished while working from home.
Recent developments in this domain have proposed that presenteeism can be functional if those engaging in it can achieve good performance without ‘further taxing the presentee’s health’ (Karanika-Murray and Biron, 2020: 247). Considering public health crises such as annual respiratory infectious outbreaks, the presumed functionality of presenteeism depends on the context in which presenteeism occurs. The decision about the functionality of presenteeism should be based not just on the performance and health of the presentees, but on that of their co-workers (Luksyte et al., 2015), which is particularly important during public health crises as well as for organisational efforts and interventions to promote health of all employees. Furthermore, we build on and extend research on presenteeism by highlighting the importance of environmental cues for influencing individual decisions to engage in presenteeism (Ruhle and Suss, 2020). Prior research has shown how organisations can inadvertently encourage presenteeism by creating a ‘presenteeism climate’ by not having sick leave policies or putting pressure (even implicitly) on employees to work long hours and engage in ‘face time’ irrespective of one’s health (Ferreira et al., 2015). Such climates may also result from poor leadership, whose lack of concern for employee wellbeing, may promote presenteeism (Wang et al., 2018). Given the negative consequences of presenteeism on organisational outcomes, such as customers’ repurchase and recommendations intentions (Dietz and Zacher, 2022), organisations will benefit from knowing how to curb presenteeism. Our results further emphasised the critical role organisational practices play in combating presenteeism, yet they also underscored how and why these practices may not work equally well for all employees, even during public health crises. Our results are applicable outside the pandemic context because they highlighted the importance of implementing sickness preventative practices that will activate health protective behaviours. Although some of the organisational sickness preventative practices (e.g. social distancing) are no longer mandatory in public places, such practices are still effective in sending signals to all employees about the importance of prioritising health (and not performance) when deciding to come to work sick. This is because when organisations continue implementing measures such as increasing ventilation, providing disinfectants and sanitisers, emphasising good hygiene practices at work (e.g. washing hands), they promote health prioritisation motives as organisational norms that get shared and embraced as organisational culture of health and wellbeing (as opposed to presenteeism climate; Ferreira et al., 2015; Troth et al., 2024). The critical role of organisational practices in curbing presenteeism, particularly among women, has highlighted the importance of having such practices for prioritising health. For example, health leadership is designed to promote ‘physical, mental, and social wellbeing, and not just the absence of disease’ (Rudolph et al., 2020: 1). Consistent with this focus on promoting health, not just preventing sickness, our results highlight the importance of organisational practices to minimise presenteeism for women, presumably via activating a health protection motive – a key feature for creating an organisational culture of health.
Finally, our model held regardless of whether employees worked from home or in a workplace such as an office, shop or work location. These findings further supported the potential benefits of organisational sickness preventative practices for the reduction of presenteeism in general and not just when there is potential for contagion. By putting in place preventative practices, organisations send signals that they value the health and wellbeing of their employees, who should prioritise their health and not engage in presenteeism regardless of whether they work from home or in a physical workspace. These findings are particularly relevant in light of recent research showing how presenteeism is prevalent even when people work from home, a phenomenon coined as workahomeism (Brosi and Gerpott, 2023). Our results suggest that organisational sickness preventative practices are likely to reduce workahomeism, particularly for women, because they are designed not only to prevent sickness but to promote health. Our findings are also important considering increased mental health issues related to stress and anxiety, amplified by public health crises, wherein a challenge to balance work and health is acutely experienced (Wu et al., 2021).
5.2. Practical implications
Our research has important implications for understanding how and why men and women may react differently to organisational health initiatives during public health crises and provides levers for helping organisations to reduce presenteeism. First, organisations should be aware of the potential for differential effects of preventative practices for men and women considering documented differences in health prioritisation. Organisations could proactively address and emphasise the importance of these practices for all employees, but men in particular, who tend to be reticent to engage in health-protective and health-promoting behaviours (Moran and Del Valle, 2016; Struik et al., 2019). Second, although absenteeism is costly because workers do not contribute to organisations (Nguyen et al., 2016), its opposite – presenteeism – is even costlier due to its negative effects on employees and their co-workers. As such, we agree it is important to drop our ‘soldier on’ mind-set and stop going to work sick, as has been suggested by the Australian Chief Medical Officer Brendan Murphy (Meixner, 2020). This advice is particularly relevant for women who are more responsive to organisational practices to minimise this risky behaviour. This advice is also relevant for men, who were less responsive to the organisational sickness preventative practices, which our theory argues is due to a lower priority placed on health. Organisations may be able to discourage presenteeism by emphasising the importance of complying with the sickness preventative practices and other health promoting measures and staying at home while sick for all employees. In doing so, employees will not only protect their own health but the health of others – a vital step in curtailing the spread of the sickness during public health crises as well as promoting health culture.
We replicated our model with employees who work from home and in the traditional office space. These findings suggest that organisations can manage presenteeism without implementing ‘daily health checks’ that have been recommended as a potential measure to ‘mitigate and guard against presenteeism’ (Kniffin et al., 2021: 68). Yet, these health checks may interfere with employees’ privacy rights. Our findings suggest that organisations can minimise presenteeism without such intrusive measures that could potentially erode organisational trust and commitment. Organisations can achieve this goal by implementing sickness preventative measures and/or other health-promoting interventions, and in doing so, they will signal to their employees the importance of their health and wellbeing, which in turn, minimises presenteeism.
5.3. Limitations
Despite the potential strengths of our research, which is based on the four waves of data spanning the various stages of the global pandemic, we should note limitations. We discuss these limitations here, along with associated implications for future research; as well as additional avenues for research that show promise for building upon the current findings.
We begin by acknowledging methodological limitations that may have influenced our results. First, the self-reported nature of our data suggests that CMV may have influenced our results. We attempted to minimise this concern by using a time-separated measurement design and controlling for the baseline levels of the DV (i.e. presenteeism). However, this design does not allow us to examine other lagged effects, for which longitudinal, panel studies are needed (Demerouti et al., 2009; Lu et al., 2013). Future research could strengthen our findings by utilising experimental vignette scenarios that have been used to manipulate socially undesirable work behaviours such as lateness (Luksyte et al., 2013), absenteeism (Patton, 2011) and presenteeism (Luksyte et al., 2023).
Second, although we focused on organisational sickness preventative practices, we explored employees’ perceptions about the enactment of such practices at the individual level. Such an approach is consistent with prior research that utilised employees’ perceptions to assess organisational practices in general (Baker et al., 2019) and during public health crises in particular (Lin et al., 2021). Yet future research could use multilevel modelling to validate our model across different levels of analyses (Beus et al., 2019).
Third, we collected most of our data from the United States, with some participants from Australia. Notably, our participants across these two countries reported similar levels of how their organisations implemented sickness preventative practices. They also did not differ in their responses regarding other safety net indicators, such as the existence of and access to formal paid leave during the pandemic and COVID-19-responsive leave policies. However, countries across the world differed in how they have implemented WHO recommendations to manage the recent pandemic (Islam et al., 2020). Hence, employees in other Western and non-Western countries may have various levels of compliance with the organisational sickness preventative practices.
Fourth, it is also important to discuss the generalisability of the current results, given that we collected data in the context of the recent COVID-19 pandemic and operationalised the organisational preventative practices to address that virus. Notably, the hypotheses generated from our theoretical framework extend to other organisational health practices and non-pandemic periods. We speculate, however, that the effects may be more pronounced during non-pandemic time due to their being higher mean levels of and variability in presenteeism (as evidenced by our baseline data). Nonetheless, the findings that presenteeism still occurred during the pandemic, and that our results point to actionable levers for reducing such behaviour, sets the stage for preventative actions for other public health crises such as annual respiratory infectious outbreaks and/or future pandemics.
Although we examined theory-based mediators, we have not empirically incorporated our conceptual pairing of gender with health consciousness into the moderation aspect of our model. Recent research showed that women tended to prioritise and protect their health more than men (Luksyte et al., 2023). Future research could incorporate this health protection motive into the testing of our model.
A final limitation of our study is the small sample size for our follow-up exploratory analyses. Using the G*Power programme, we conducted post hoc power analyses to detect gender differences for our proposed model. Using these parameters (N = 56, partial η 2 = 0.10, α = 0.05), we calculated post hoc power being 0.69, meaning that our sub-sample was underpowered and thus caution must be taken when interpreting the results. However, we note that workahomeism is positively related to traditional forms of presenteeism (Brosi and Gerpott, 2023). Hence, we urge future research to examine the applicability of our model with different types of presenteeism including workahomeism, by using larger sample sizes than the one we utilised in our follow-up exploratory analyses.
5.4. Future research directions
This research also sets the stage for extending knowledge about presenteeism beyond the current focus. First, future scholars could examine other organisational practices that could minimise presenteeism. Research has shown that leaders play a crucial role in modelling presenteeism for their followers: Those leaders who come to work sick signal to their employees’ norms and expectations about health-related behaviours, thereby encouraging presenteeism among their followers (Dietz et al., 2020). It is possible that leader presenteeism may have a stronger effect on men’s than women’s presenteeism, given that women are more likely to prioritise health than men and thus could be less susceptible to the impact of their leaders’ presenteeism on their own decision to engage in presenteeism.
Second, our research has implications for future research regarding cognitive and affective motives for engaging in presenteeism. Past research has considered such motives either as specifically related to the behaviour in question or at a more general level of specificity. Indeed, we conceptualised and operationalised our specified motives in line with past research (Lu et al., 2013), such that we measured the approach/avoidance motivation in reference to presenteeism behaviour, and we measured workplace anxiety in relation to work in general. Future research could advance theoretical understanding of these motives by considering the potential implications of the level of specificity. For example, one might wonder whether motives assessed in relation to the specific behaviour in question conflate the operationalisation with the behaviour. Notably, the correlation between workplace anxiety and presenteeism (r = 0.51) in these data was stronger than the correlations involving the approach/avoidance motivation (r = 0.30 and r = 0.40, respectively). This empirical pattern suggests that conflation between the approach/avoidance motivation measures and presenteeism is unlikely to be a concern in these data but points to an opportunity for future work to consider the theoretical and empirical implications of conceptualising and operationalising motives at different levels of specificity.
Another opportunity for future research relates to the measurement breadth of such motives. Despite our CFAs confirming the empirical distinction of workplace anxiety and avoidance motivation for presenteeism, their strong positive correlation is noteworthy. Workplace anxiety refers to the extent to which employees feel nervous and apprehensive about fulfilling their work goals (McCarthy et al., 2016). Avoidance motivation for presenteeism refers to deciding to turn up to work while sick due to ‘worries about being punished, blamed, or leaving a bad impression on important others’ (Lu et al., 2013: 410). As such, workplace anxiety captures concerns over work in general, whereas avoidance motivation for presenteeism is specifically related to the act of presenteeism. In terms of operationalisation, however, it is noteworthy that the established measure of avoidance motivation (Lu et al., 2013) captures anxiety-related motives. Thus, future research may benefit from operationalising this construct with greater breadth.
Third, our theorising was based on the idea that women prioritise health more than men, who focus on protecting their performance rather than health when contemplating whether to come to work being sick. Future research could build on and extend this idea, supported by our findings, about what organisations can do to minimise this theorised focus on protecting performance, which is believed to lead to more presenteeism for men. Organisations should explicitly recognise that presenteeism, even if it is done for good, approach (not avoidance) reasons such as out of a commitment to work, desire not to overburden colleagues (Lu et al., 2013), is not a welcomed work behaviour. Future research could contrast and compare the effectiveness of sickness preventative practices with other organisational measures that proved influential in either reducing or aggravating presenteeism during the pre-pandemic times (Lohaus and Habermann, 2019). It is worthwhile noting that in our study, there were no gender differences in baseline presenteeism; yet presenteeism measured at Time 3 was higher among women than men. These mixed results are consistent with prior research that failed to show strong and conclusive evidence of women reporting higher levels of presenteeism (Idris et al., 2023; Luksyte et al., 2023; Miraglia and Johns, 2016). Interpreting the current findings from this angle indicates that the main effect of gender on presenteeism is qualified by the extent to which the organisation implements health practices, and moreover, that motives explain that interaction. These data suggest that women engaged in more presenteeism than men when there were lower levels of organisational health practice intervention due to higher levels of workplace anxiety. Our findings, therefore, extend our understanding of when and why women may sometimes engage in higher levels of presenteeism; even though often both men and women display similar levels of presenteeism.
Also related to gender, future research could consider additional and more specific motives for engaging in presenteeism, particularly those that may be even more gendered (i.e. tied to theoretically presumed social roles). For example, social role theory points to specific motives such as the expectation to financially provide for dependents as particularly motivating for men; and specific motives such as the expectation to care for dependents (e.g. children or elderly parents) as particularly motivating for women. Honing in on these specific motives has the potential to add further nuance to understanding the mechanisms that underlie the impact of organisational practices on presenteeism.
Finally, we examined gender as one demographic that may shape the effectiveness of organisational strategies in minimising presenteeism. Other characteristics may be of equal importance. Research has shown that older workers are motivated to protect their naturally declining health by staying at home when they are sick (Jensen et al., 2019); this finding is supported meta-analytically (Miraglia and Johns, 2016). Furthermore, research has shown that younger people reported being less likely to comply with public health measures during public health crises (Brankston et al., 2021). Extrapolating from these studies and our research findings, we encourage future scholars to explore how organisations may tailor their strategies to address younger employees’ compliance with these strategies and subsequently minimising their presenteeism.
Key practical and research implications
Managers should be aware of how and why women and men may react differently to sickness preventative measures that organisations implement to minimise presenteeism behaviours.
Employers could proactively emphasise and focus on tailoring health-protective and health-promoting behaviours to avoid the ‘soldier on’ mindset of sick employees who contemplate whether to engage in presenteeism.
The implementation of organisational preventative sickness practices signals to employees (particularly to women) the importance of prioritising their health, which in turn minimises presenteeism.
Footnotes
Appendix 1
We measured ‘Organisational sickness preventative practices’ with the nine items that were rated on a 5-point frequency scale ranging from 1 = very little to 5 = a great deal.
Instructions: Please use the scale provided to indicate the extent to which your organisation has put the following social distancing and hygiene practices in place in response to the COVID-19 pandemic:
Final transcript accepted on 19 December 2024 by Ashlea Troth (AE Organisational Behaviour).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the University of Western Australia’s Business School Grant, and an Australian Research Council’s Discovery Early Career Researcher Award (DE170100182) for the first author.