
Abstract
The experience of suffering is ubiquitous in healthcare facilities, but against this backdrop, is compassion a ‘nice to have’ or does it also affect patient safety? This article uses mixed methods across two studies to understand team compassionate care behaviours as a shared unit property and its association with patient safety outcomes. Using data from 188 healthcare teams, Study 1 finds that team compassionate care behaviours mediated the relationship between team psychological safety and fewer patient hospital-associated infections. Furthermore, the positive relationship between team psychological safety and team compassionate care behaviours was weakened when team workload demands were high. In Study 2, we interviewed 25 nurses to understand the experiences and gain further insights into the relationships between the focal variables. Together, our findings provide evidence that compassion emerges at the team level, is driven by team antecedents, moderated by team environments and tangibly affects patient safety.
1. Introduction
The experience of suffering is ubiquitous in organisations (Dutton et al., 2014; Frost, 2003). Whether the suffering stems from one’s personal life (e.g. financial woes), global events (e.g. the COVID-19 pandemic), is organisationally induced (e.g. workload pressures) or integral to one’s job role (e.g. taking care of sick patients), organisations are emotional arenas. As such, organisations inevitably harbour the suffering of their members and the people they serve (Dutton et al., 2007; Frost, 2003). The ubiquity of suffering and the indispensability of compassion towards those suffering is particularly evident in healthcare settings where patient illness, pain and death are inherent features of the organisational context. The display of compassion towards patients is a cornerstone of the work of healthcare professionals and has been linked to a variety of critical outcomes, such as more accurate diagnosis (Epstein et al., 2005), shorter recovery times for patients (Cole-King and Harding, 2001) and fewer damage claims (Levinson et al., 1997).
Showing compassion to patients is arguably the ‘right thing to do’ in healthcare (Trzeciak and Mazzarelli, 2019: 66). However, in light of increasing levels of staff burnout, concerns about compassion fatigue, increasing medical acuities, funding constraints and chronic staff shortages, questions remain about the extent to which healthcare workers can sustainably practise compassion towards patients (Hooper et al., 2010). Furthermore, with the rise of team-based work and the decreasing reliance on individual contributors, it is questionable whether the continued focus on individuals and their practice of compassion (e.g. Dutton et al., 2014), thus situating compassion as an individual obligation, is practical and sustainable. As acknowledged by compassion scholars, the process of noticing and responding to suffering does not occur within a vacuum (Kanov et al., 2004). Compassion is often a collective rather than an individual response (Lilius et al., 2011) and is more impactful when enacted collectively. Scholars have theorised and described how team and organisational practices can enable reliable patterns of collective compassion among groups of individuals, with distinguishable patterns between groups (Dutton et al., 2014; Lilius et al., 2011). In particular, qualitative evidence highlights the social processes and relational architecture (e.g. shared practices and norms) in developing reliable patterns of compassion within work units (Dutton et al., 2006; Lilius et al., 2011). Yet, to date, the team antecedents that drive team compassion and the collective features of the work environment that moderate the practice of collective compassion are largely described as an ‘amalgam of contextual features’ (Dutton et al., 2006: 62) and remain untested. This article builds on the literature on compassion by focusing on team compassion as a distinct phenomenon and identifies the specific characteristics of the team that drive and moderate team compassion behaviours.
This article provides qualitative and quantitative evidence of compassionate care behaviours as a team phenomenon driven by team antecedents and influencing team outcomes. Drawing on Dutton et al. (2014, 2006) and Lilius et al. (2011) and their theorisation of high-quality relationships enabling collective forms of compassion, we argue that team psychological safety (i.e. the ability for team members to take interpersonal risks, Edmondson and Bransby, 2023; Edmondson and Lei, 2014) drives team compassionate care behaviours towards patients. We argue that team compassionate care behaviours have further downstream effects, influencing tangible team outcomes that directly affect patient safety. This is an important contribution, as studies focusing on the process of team compassion towards the recipients of their service (e.g. clients or consumers) are rare and sorely needed (Dutton et al., 2014; see Wee and Fehr, 2021 for an exception). In this article, we focus on the influence of team compassionate care behaviours on a critical patient safety indicator in hospital teams – healthcare-associated infections (HAIs). Finally, we consider boundary conditions that may prevent the benefits of team compassionate behaviours for patient safety. In doing so, we contribute to the compassion literature in three important ways.
As indicated by Dutton et al. (2014), there is little empirical evidence on how compassion influences outcomes beyond individual (provider or recipient) perceptions. Although many have speculated that collective forms of compassion at work can yield collective benefits (Dutton et al., 2014), others have indicated that the practice of compassion can be effortful and draining (Frost, 2003; Jacobson, 2006). Therefore, our first contribution to the literature is linking team compassionate care behaviours with patient safety, specifically the frequency of HAIs in a hospital unit. HAIs are infections acquired in a healthcare facility by a patient admitted for a reason other than that infection (e.g. an infection of surgical wounds, healthcare-associated pneumonia, sepsis). Hence, an HAI is an infection that the patient acquired after being admitted to the hospital for the treatment of another ailment. HAIs are among the highest-priority patient safety concerns in the world (World Health Organization, 2002) and are estimated to affect 1 in every 10 patients worldwide (World Health Organization, 2016). The 5 most common HAIs in Australia are estimated to occur more than 170,500 times a year, resulting in more than 7500 deaths in public hospitals annually (Lydeamore et al., 2022). In addition, HAIs are costly; they further the suffering of an already ill patient, and a single patient with an HAI is associated with costs of over $37,500 in Australia (ACSQHC, 2018). Reducing the incidence of HAIs is a crucial objective and key team performance effectiveness metric shared by healthcare providers, patients and their families (Johnson et al., 2018a). The ability of healthcare units or teams to effectively treat and discharge patients in better health than when they were admitted is essential, not only for patients and their families but also for the organisation. Our article therefore contributes to the compassion literature by looking beyond individual outcomes and perceptions to show how team compassionate care behaviours towards patients can influence patient safety, demonstrating the utility of team compassionate care behaviours.
Second, we contribute to the compassion literature by empirically examining what drives team compassionate care behaviours. Existing conceptualisations of collective compassion tend to be descriptive and focus on how compassion spreads through the organisation (e.g. Dutton et al. 2006, 2014; Lilius et al., 2011). To date, we are unaware of empirical studies investigating the team antecedents that drive the extent to which teams collectively practise compassionate care behaviours. However, in these conceptualisations, both Dutton et al. (2006, 2014) and Lilius et al. (2011) argued that the relational fabric of work units shapes norms that legitimate discussions of suffering, which enables the collective emergence of reliable patterns of compassion within the team. In particular, Lilius et al. (2011: 889) indicate that ‘fostering a sense that it is safe and appropriate to share . . . makes it more likely that unit members will know enough about the experiences and struggles of others to seek . . . help’. In other words, feeling that it is safe and appropriate to share allows teams to gain insight into the suffering of others, enabling teams to respond compassionately to the needs of the sufferer. Despite this theorisation, the link between team psychological safety and team compassionate care behaviours has not yet been empirically tested. In light of this, we propose that team psychological safety is an antecedent to team compassionate care behaviours.
In addition, our article examines not only team psychological safety as an antecedent of team compassionate care behaviours but also the boundary conditions. Therefore, we also contribute to the compassion literature by examining how the demand or intensity of the work conducted by teams (i.e. team workload demands) could influence the relationship between team psychological safety and team compassionate care behaviours. In other words, how might collectively having too much to do in too little time influence the relationship between team psychological safety and team compassion care behaviours? Drawing on Dutton et al.’s (2006) theory of compassionate organising, we argue that the relational fabric of compassion within work teams is not enough to cultivate team compassion; the context of work and work conditions must also be conducive to directing collective attention to the suffering of patients. Specifically, we argue that team workload demands to shift the focus of the team’s attention away from patient suffering towards the tasks that need to be completed so that the relationship between team psychological safety and patient-directed team compassionate care behaviours is weakened when teams have too much to do.
Finally, the findings of the article make important practical contributions in terms of informing evidence-based interventions to promote team compassionate care behaviours towards patients. To date, most compassion interventions are focused on the individual (e.g. Kirby, 2017), with very little evidence on the effectiveness of team-based interventions aimed at promoting client-directed compassion. Our article provides insights into potential team-level compassionate care interventions that go beyond individual-based interventions and foster more shared responsibility and sustainability.
Together, this article seeks to understand team compassionate care behaviours, including its antecedents, outcomes and boundary conditions at the team level. We conducted two empirical studies with two independent samples of nurses working in acute hospital settings in Australia. The first quantitative study sought to elucidate the relationships between team psychological safety, team workload demands, team compassionate care behaviours and the incidence of HAIs across 188 healthcare teams (see Figure 1). We propose that team compassionate care behaviours mediate the relationship between team psychological safety and HAIs and that team workload demands moderate this mediated relationship. The second study is qualitative and is based on 25 interviews with nurses about the team forces that shape compassionate care behaviours towards patients. We used the qualitative findings to triangulate our quantitative results and gain further insight into the drivers and consequences of team compassion in acute hospital settings.
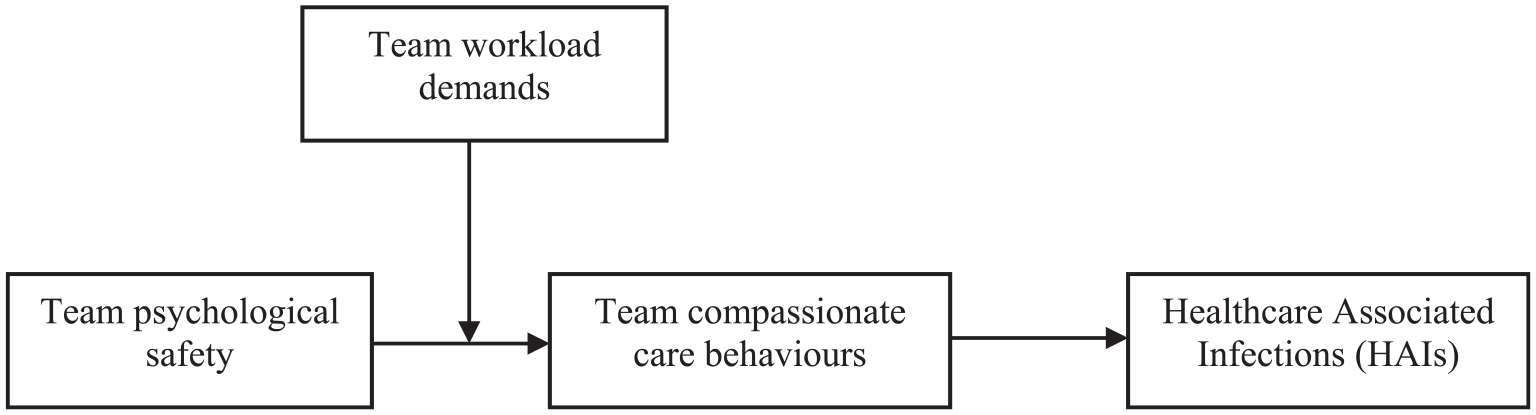
Theoretical model for Study 1.
2. Study 1: a quantitative examination of patient-directed team compassionate care behaviours in healthcare
The provision of high-quality healthcare entails compassion towards patients (Robinson et al., 2008; Stuijfzand et al., 2020). The practice of nursing also requires compliance with legal and clinical obligations (e.g. Nursing and Midwifery Board of Australia, 2006). As such, patients are often characterised by their medical condition, and healthcare personnel are seen to provide clinical expertise to remedy these conditions (Santana et al., 2018). However, high-quality healthcare recognises the person behind the patient and includes care for that individual’s health and well-being that informs the social institution of healthcare (Santana et al., 2018; Simpson et al., 2020). Compassion serves as the bridge that connects healthcare professionals to patients (Nussbaum, 1996) and enables healthcare professionals to care for a patient through some of their most vulnerable moments in life (Trzeciak and Mazzarelli, 2019). Despite this, the practice of compassion by healthcare staff routinely falls short of patient and family expectations ((Friele et al., 2008; Hooper et al., 2010; Sinclair et al., 2016). For instance, Carrese et al. (2017) found that clinicians only greeted or were responsive to patients and visitors approximately 50% of the time. Another study showed that approximately three-quarters of medical professionals failed to recognise a patient’s affective cues and respond effectively to a patient’s emotional state (Levinson et al., 2010).
Research on compassion continues to focus on the focal actor (i.e. the person providing compassion) despite compassion being conceptualised as a process that is embedded throughout the organisation (Dutton et al., 2014). When compassion is conceptualised as a personal characteristic reflected by an individual’s values and traits (e.g. Atkins and Parker, 2012; Dutton et al., 2014), employees might feel that the burden of compassion largely rests on them as individuals. While scholars have highlighted the role of work units as ‘enabling conditions’ for an individual’s compassion, these conceptualisations nevertheless emphasise the role individuals play in the compassion process. In this article, we argue that compassionate care behaviours are not only a reflection of individual caregivers but also a team phenomenon. Building on Dutton et al.’s (2014) theorisation that compassion is nested within the personal, relational and organisational domains, we propose that compassion is also nested within the meso or team context. At the team level, we argue that team compassion is driven by team antecedents, influences team outcomes and is bounded by the team context and conditions. This is supported by Dutton et al. (2002), who found that the compassion of team members is influenced by leadership, as well as Lilius et al. (2011) who highlighted how local practices within a work unit enable reliable patterns of compassion within the team. As such, we propose that compassionate behaviours can be shared at the team level and therefore vary as a function of team membership.
Specifically, we propose that team compassionate care behaviour emerges and varies at the team level, driven by team-level antecedents (team psychological safety) and associated with team-level outcomes (frequency of HAIs in teams). We define team compassionate care behaviours as the extent to which compassionate care towards patients is a shared practice within teams. We adopt a direct-consensus compositional model, or the extent compassionate care behaviours are practised in teams (Chan, 1998; Kozlowski and Klein, 2000). According to Lilius et al. (2011), routine practices and recurrent activities within teams drive relational bonds that legitimate the discussion of suffering and enable collective empathic concern. We propose that these team norms become further reinforced within the team through shared team processes such as attraction–selection–attrition, social comparison, socialisation and leadership (Kozlowski and Klein, 2000). Over time, these practices become legitimised within the team context and are propagated and coordinated between team members to establish collective team compassionate care behaviours whereby the social processes of noticing, feeling and responding to suffering are shared among team members (Dutton et al., 2002). Similar processes have been discussed by Wee and Fehr (2021), who proposed that team compassion behaviours emerge when compassionate individuals within teams provide the social cues to normalise collective compassionate action. Together, these processes enable consistent patterns of collective compassionate care behaviours within teams that are distinguishable between teams.
3. Patient-directed team compassionate care behaviours and patient safety
Patient healthcare outcomes have clinical and humanistic characteristics (Sinclair et al., 2016). These features are considered independent, such that clinical outcomes contribute to a patient’s clinical benefit, whereas humanistic outcomes contribute to a patient’s emotional benefit. This dichotomous approach to healthcare care is prevalent but is also limiting in that it only focuses on the corresponding benefits associated with each approach. This approach neglects the possibility that humanistic features of care can produce positive clinical outcomes and is surprising in light of evidence highlighting the role of compassion in promoting a patient’s physical health and recovery (Cole-King and Harding, 2001).
Evidence indicates that the compassionate care behaviours of healthcare workers can encourage patients to be more forthcoming and openly share information (Bramley and Matiti, 2014). Patients may feel uncomfortable divulging information they deem irrelevant or feel apprehensive about sharing (e.g. personal or family history, new symptoms). Patients may be more forthcoming when treated compassionately, and such information may be clinically important (Wang et al., 2019). As a result, compassionate care behaviours may enable more effective clinical action, resulting in improved clinical outcomes (Epstein et al., 2005). Compassion can also alleviate stress and anxiety among patients, which is associated with faster clinical recovery times (Cole-King and Harding, 2001). Research also indicates that compassionate care encourages patients to participate in healthcare decisions more actively by enhancing collaboration, cooperation and effort between healthcare staff and patients (Cahill, 1996; Thorne et al., 2005). As a result, patients may be more likely to speak up to discuss their care preferences, which can enhance adherence to healthcare plans.
Extending beyond the literature on individual caregivers and their practice of compassion, we argue that team compassionate care behaviours are associated with better patient safety. Compassion at the group level involves collective noticing, feeling and responding to suffering, including coordination between team members (Dutton et al., 2002). This coordination of compassion is important in acute hospital settings because patients are often cared for by a different nurse each shift, with up to three nurses each day. Over 5 days, up to 15 different nurses may care for a patient. We argue that patients of teams characterised by higher levels of team compassionate care behaviours are likely to receive a coordinated compassionate response between nurses and experience a consistently higher level of compassionate care between nurses in that team. On the contrary, patients of teams characterised by lower levels of team compassionate care behaviours are likely to receive more variable levels of compassionate care, compassionate care of a consistently lower quality or compassionate care that is less coordinated between team members. Therefore, not only are patients’ needs and concerns less likely to be disclosed in the first place, but even if disclosed, such needs and concerns are less likely to be consistently addressed or coordinated by team members.
Given that enhancing the partnership between the patient and the healthcare provider has been recognised as key in reducing the incidence of HAIs (ACSQHC, 2018), we propose that teams with higher levels of team compassionate care behaviours can provide safer and higher-quality patient care as reflected in reduced HAIs. Together, we propose that team compassionate care behaviours are associated with improved patient safety, reflected in the rate of patient HAIs in the team. Therefore:
Hypothesis 1. Team compassionate care behaviours are associated with fewer patient HAIs in the team.
4. Team psychological safety and team compassionate care behaviours
The care of patients in acute hospital settings is becoming increasingly fragmented due to growing clinical specialisation (Rosen et al., 2018). As such, the overall quality of patient care is becoming more dependent on effective collaboration and communication between healthcare workers (Rosen et al., 2018). Nurses provide most of the patients’ bedside care (e.g. attending to the patient and managing patient concerns) and are often tasked with bridging information gaps between patients and healthcare professionals given their proximity and understanding of patients (Bell and Duffy, 2009). However, nurses often experience less power than other healthcare professionals (e.g. doctors) due to differences in clinical training (Green et al., 2017) and often feel constrained in their ability to advocate for patient care (Nembhard and Edmondson, 2006).
Team psychological safety is the collective and shared belief that a team environment is safe for interpersonal risk-taking (Edmondson and Bransby, 2023; Nembhard and Edmondson, 2006). Psychological safety captures perceptions of risk or harm from the environment, particularly negative interpersonal outcomes, from engaging in words or actions (Sherf et al., 2021). Team psychological safety emerges through the patterns of interactions within a team that, over time, act as the collective group norms regarding how safe it feels to engage openly and honestly with others about work-related issues (Edmondson, 2003). When environments are not psychologically safe, employees feel that they are at risk and vulnerable (e.g. threats, dangers, attacks and rejection from peers). As such, they are more likely to be cautious in their interactions with colleagues and more likely to keep insights to themselves.
While psychological safety is associated with fewer adverse incidents and innovation (Newman et al., 2017; Tucker and Edmondson, 2003; see Edmondson and Bransby, 2023, for a review), the relationship between team psychological safety and team compassionate care behaviours remains untested. As indicated by Lilius et al. (2011), not being afraid to speak up forges relational bonds and collective empathic concern by enabling employees to become attuned to one another within the team. In this article, we extend Lilius et al. (2011) by arguing that psychologically safe team environments enable team members to advocate for those outside the team (i.e. patients) to alleviate their suffering.
We propose a positive relationship between team psychological safety and team compassionate care behaviours. By lowering barriers and perceived interpersonal risks, psychological safety invites employees to express different opinions and concerns, thereby prompting more open and authentic discussions (Tucker and Edmondson, 2003). In these psychologically safe teams, nurses are more likely to share their perspectives and observations of patient care and suffering. According to Dutton et al.’s (2014) process model of compassion, this increased sharing within teams about patient observations and perspectives can enhance the noticing or understanding of suffering, which directs the development of empathic concern required for compassion. We propose that team psychological safety can facilitate more comprehensive patient-centred insights across healthcare team members that heighten team compassionate care behaviours. Nurses belonging to psychologically safe teams may feel more comfortable sharing patient suffering and concerns, which can cultivate a collective sense of empathy that directs a coordinated and compassionate team response to patient suffering.
On the contrary, individuals who do not feel psychologically safe often discount the relevance of their newly acquired information and consider it unworthy of broader discussion (Milliken et al., 2003). A lower level of psychological safety is associated with more silence behaviours (Sherf et al., 2021), such as, in the context of nursing, concerns about patient suffering and care. In these environments, nurses may be less likely to advocate for patient suffering. As such, these teams may be less likely to be aware of or notice patient suffering and therefore less coordinated in team compassionate care behaviours to alleviate patient suffering (van der Cingel, 2011). Therefore, we propose the following:
Hypothesis 2. Team psychological safety is associated with higher levels of team compassionate care behaviours.
5. The moderating role of team workload demands
Team workload demands refer to the team’s requirement to work hard and under time pressure (Leicht-Deobald et al., 2022). These team workload demands are often driven by the physical, social and organisational aspects of the team’s work and require sustained physical and/or mental effort and therefore are associated with physical and psychological costs (Demerouti et al., 2001). Although workload has primarily been investigated as an individual experience, the sustained effort that needs to be exerted is often a shared team characteristic (Karasek, 1979) and has been conceptualised as a shared feature of the organisational environment that can vary across work groups (French, Caplan, and Van Harrison, 1982; Lazarus and Folkman, 1984).
Team workload demands are often conceptualised as an unfavourable and stressful work context that reflects the shared experiences of team members (Ni et al., 2020; Razinskas and Hoegl, 2020). Team stressors, such as workload and time pressure, can undermine the performance and effectiveness of teams by inhibiting effective teamwork (Razinskas and Hoegl, 2020). In their review, Razinskas and Hoegl (2020) indicated that team workload demands can affect team information and communication processes and undermine team effectiveness. Specifically, they highlighted that team workload demands can impair the development and accuracy of shared knowledge and learning within teams by narrowing attention towards completing tasks. These teams are more prone to filtering out peripheral information that is less important to task completion, which impairs the team’s access to comprehensive and holistic insights (Razinskas and Hoegl, 2020). With research indicating that healthcare professionals often place more importance on clinical skills than humanistic skills (Attree, 2001; McDonagh et al., 2004), we argue that high team workload demands lead teams to narrow their attention and effort to the most significant clinical problems as opposed to compassionate responding (Hooper et al., 2010; O’Callaghan et al., 2020). Thus, we propose that high team workload demands drain teams of the resources, such as energy, time, effort and information, necessary for team compassionate care behaviours (Ni et al., 2022; Razinskas and Hoegl, 2020).
We propose that higher team workload demands act as an unfavourable context that limits the extent to which team psychological safety enhances team compassionate care behaviours. While members of psychologically safe teams may feel safer in sharing information about patient suffering, teams characterised by high workload demands may be more inclined to focus on clinical or task-related goals. Under high team workload demands, psychologically safe team members may have to prioritise the sharing of task-related information at the expense of sharing observations of patient suffering. This then directs attention away from the collective noticing of patient suffering such that even psychologically safe teams cannot develop a coordinated response to patient suffering (i.e. team compassionate care behaviours). Under high team workload demands, team members may be collectively inclined to direct their limited resources to clinical actions (e.g. quickly administering an injection to scared and vulnerable patients) at the expense of compassionate care behaviours (e.g. soothing a patient’s fear of injections). Under intense workloads, we propose that compassionate care behaviours may be largely considered a ‘nice to have’ but not a high priority (Johnson et al., 2018b; Ni et al., 2022) even when team psychological safety is robust. In contrast, when teams experience lower workload demands, members face fewer competing demands, and therefore there is more shared capacity to assist and provide relief (Schaufeli and Taris, 2014). These teams have more opportunities and are less constrained in time, energy and resources to respond compassionately in light of patient suffering. Therefore, we propose:
Hypothesis 3. Team workload demands moderate the positive impact of team psychological safety on team compassionate care behaviours, such that the relationship is weaker when team workload demands are high.
Integrating the above hypotheses, we propose that team compassionate care behaviours mediate the relationship between team psychological safety and the incidence of HAIs and that this relationship is moderated by team workload demands.
Hypothesis 4. Team workload demands moderate the indirect relationship between team psychological safety and patient healthcare-associated infections via team compassionate care behaviours, such that the indirect relationship is weaker when team workload demands are high versus low.
6. Method
6.1. Design and participants
Study 1 examined the hypothesised relationships between nurses and midwives from eight hospitals across a major healthcare network in Australia. Nurses and midwives working within a hospital unit share patients and work throughout the day and night to provide care to patients with similar clinical needs. As a result, the teams are characterised by high task interdependence and coordination needs (Wageman, 1995).
We first surveyed the nurses and midwives across the eight acute healthcare facilities. The survey was voluntary and could be completed on paper or online. The paper survey packs consisted of a participant information sheet, consent form and survey and were placed on workstations and break rooms, along with posters about the research. All completed paper surveys were sealed and returned to the researchers in a reply-paid envelope. The online link to the survey, including the participant information sheet and consent form, was distributed by email from the healthcare facility’s director of nursing and midwifery services.
All 4925 nursing and midwifery staff across the facilities were invited to participate in the survey. The final sample consisted of 2437 nurses and midwives (average age = 39 years, SD = 12.01; 86% female) in 188 teams, representing a response rate of 49%. On average, participants had worked as a nurse or midwife for 15 years (SD = 11.96).
6.2. Measures
Our study was concerned with theory and analysis at the team level, and so we followed the recommendations of Kozlowski and Klein (2000) and Chan (1998) in conceptualising our team-level constructs. Psychological safety is an emergent team property, and we captured team psychological safety through the referent-shift consensus approach, where respondents were asked to respond to their team’s psychological safety and therefore reflect on its collective experience.
On the contrary, team workload demands and team compassionate behaviours were created using the direct-consensus compositional model (Chan, 1998) to represent them as unit properties (Kozlowski and Klein, 2000). We adopted the direct-consensus compositional model for two reasons. First, these constructs reflect an important phenomenon at the team level. Each unit or ward (team) within the hospital has specific and unique care responsibilities reflecting the unique medical profile of patients (i.e. obstetrics vs palliative care). Consequently, the workload demands and compassionate care behaviours reflect the context of the team and individual experiences.
Second, we found sufficient consistency or within-group agreement and between-group differences to index consensus and justify aggregation to the team level (Chan, 1998; Kozlowski and Klein, 2000). Under both the referent-shift and direct-consensus compositional model, within-group agreements among team member perceptions indicated shared team perceptions and justified aggregation of individual responses to represent scores at the team level. We ran a series of analyses before aggregating our variables to the team level by following the recommendations of Bliese (2000) and James et al. (1993) to determine the agreement between team members. In general, all team variables had acceptable ICC(1) > 0.05, ICC(2) > 0.40 (Bliese, 2000) and rwgs > 0.70 (James et al., 1993), indicating suitability for aggregation of ratings from an individual to a team level of analysis. The mean rwg for psychological safety was 0.73, for workload demands was 0.73 and for compassionate care behaviours was 0.91. To assess the between-group variance, we conducted a one-way analysis of variance (ANOVA) and calculated the ICC1 and ICC2 (Chen, Bliese, and Mathieu, 2005). For psychological safety, we found ICC[1] = 0.09 and ICC[2] = 0.54 (F = 2.17; p < 0.01), for workload demands, we found ICC[1] = 0.10 and ICC[2] = 0.58 (F = 2.62; p < 0.01) and for compassionate care behaviours, we found ICC[1] = 0.05 and ICC[2] = 0.40 (F = 1.97; p < 0.05). These results suggest that a significant proportion of psychological safety, workload and compassionate care behaviours can be attributed to team membership. We averaged team member ratings and aggregated them to the team level. HAIs were captured by the hospital incident management system and are only reported at the team level. All aggregation indices are reported in the description of the measures below.
Team psychological safety was measured using four items adapted from Edmondson’s (1999) psychological safety scale. The items indexed the extent to which healthcare workers felt valued by others in their unit or ward and were safe to raise problems and ask for help from their team members. An example item is ‘members of my team are able to bring up problems and tough issues’ (see full list of items in Appendix 1). Items were rated using a Likert-type scale, from 1 = does not apply at all to 5 = applies entirely. The aggregation indices were rwg(j) 0.73, ICC(1) of 0.09 and ICC(2) of 0.54.
Team workload demands were measured using three items from the Caplan et al. (1975) workload scale. The measure indexes healthcare workers’ perceptions of the amount and pace of their workload. For example, participants were asked to measure the extent to which ‘work piles up faster than you can complete it’. The items were rated from 1 = to no extent, to 5 = to a very large extent. Team aggregation indices were rwg(j) of 0.73, ICC(1) of 0.10 and ICC(2) of 0.58.
Team compassionate care behaviours were measured using two items. We asked the extent to which healthcare workers reported displaying compassionate behaviour towards their patients over the past week. The items were used from a scale developed by the authors (Johnson et al., manuscript in preparation) from adaptations of other measures of compassion in healthcare (e.g. Lown et al., 2015). For example, participants were asked the extent to which they ‘treated patients with compassion’. Both items were rated from 1 = never to 5 = always. Team aggregation indices were rwg(j) of 0.91, ICC(1) of 0.05 and ICC(2) of 0.40.
HAIs were collected across the 12 months after the survey’s close (i.e. lagged data). HAIs refer to an infection acquired in a healthcare setting by a patient admitted for a reason other than that infection (e.g. surgical wound infection, cannula infection, hospital-associated pneumonia). There are legislative requirements for healthcare facilities to collect and report safety and quality indicators, including HAIs (see Clinical Excellence Commission, 2021). We were provided access to hospital HAIs through the critical incident management system, as part of these legislative reporting requirements. We collected total HAI incidents across 12 months to ensure that the data were not affected by well-established seasonal variations in hospitalisations, most notably during winter months, that may result in poorer healthcare outcomes for patients (Fullerton and Crawford, 1999; Richardson and Mountain, 2009).
6.3. Results
Means, standard deviations, reliabilities and intercorrelations among variables are reported in Table 1. We used Mplus (version 8.0) to test all hypotheses and controlled for team size. We mean-centred team psychological safety and team workload demands in the calculation of interaction product terms to mitigate potential multicollinearity and improve the interpretability of moderating effects (Aiken and West, 1991).
Means, standard deviations, reliabilities and inter-correlations of Study 1 variables.
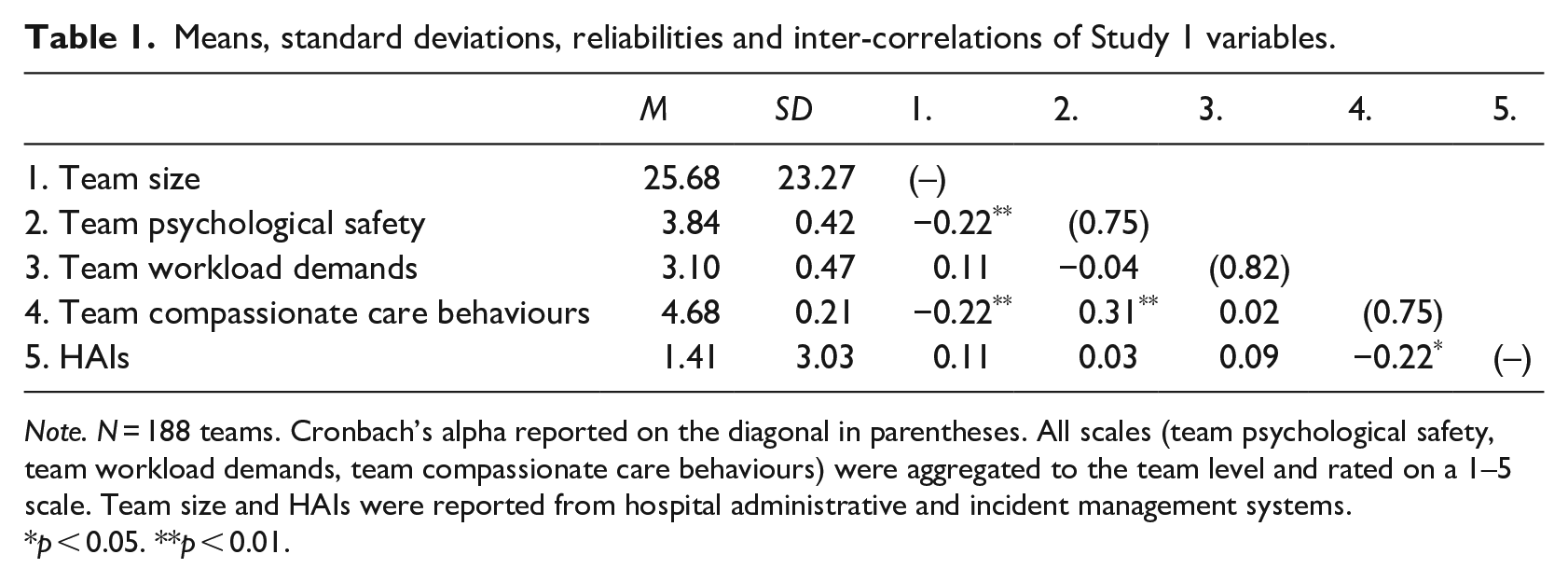
Note. N = 188 teams. Cronbach’s alpha reported on the diagonal in parentheses. All scales (team psychological safety, team workload demands, team compassionate care behaviours) were aggregated to the team level and rated on a 1–5 scale. Team size and HAIs were reported from hospital administrative and incident management systems.
p < 0.05. **p < 0.01.
Standardised coefficient estimates for the model are presented in Table 2. In support of Hypothesis 1, we found that team compassionate care behaviours were associated with fewer HAIs in the team (β = –0.21, SE = 0.10, p < 0.05). In support of Hypothesis 2, we found that team psychological safety predicted higher levels of team compassionate care behaviour (β = 0.26, SE = 0.07, p < 0.01).
Analysis results (coefficients and standard errors).
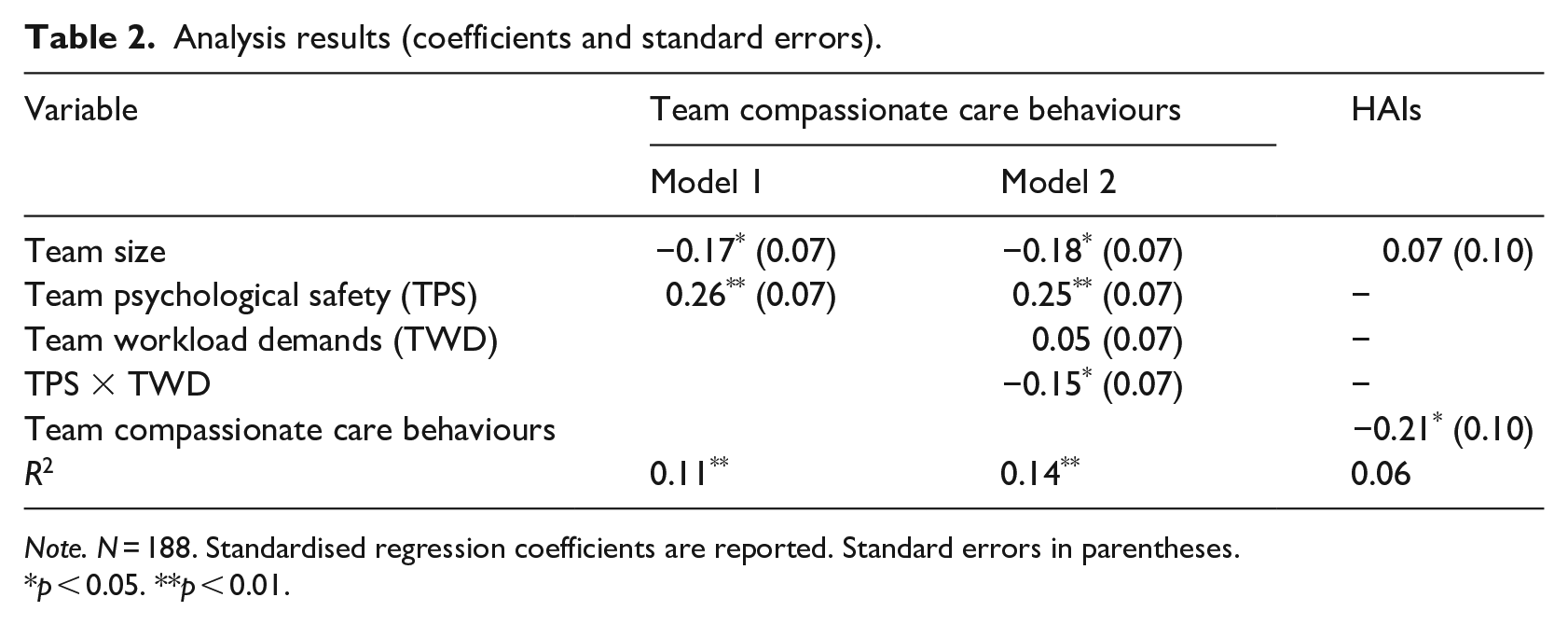
Note. N = 188. Standardised regression coefficients are reported. Standard errors in parentheses.
p < 0.05. **p < 0.01.
In support of Hypothesis 3, we found a significant interaction between team psychological safety and team workload demands on team compassionate care behaviours (β = –0.15, SE = 0.07, p < 0.05). We graphed the interaction to better understand the pattern of the significant interaction and conducted a simple slopes test. As indicated in Figure 2, there was a significant and positive association between team psychological safety and team compassionate care behaviour at lower (–1SD) values of team workload demands (b = 0.08, p < 0.01). The relationship between team psychological safety and team compassionate care behaviours became non-significant at higher (+1SD) values of team workload demands (b = 0.02, p > 0.05). Therefore, Hypothesis 3 was supported.
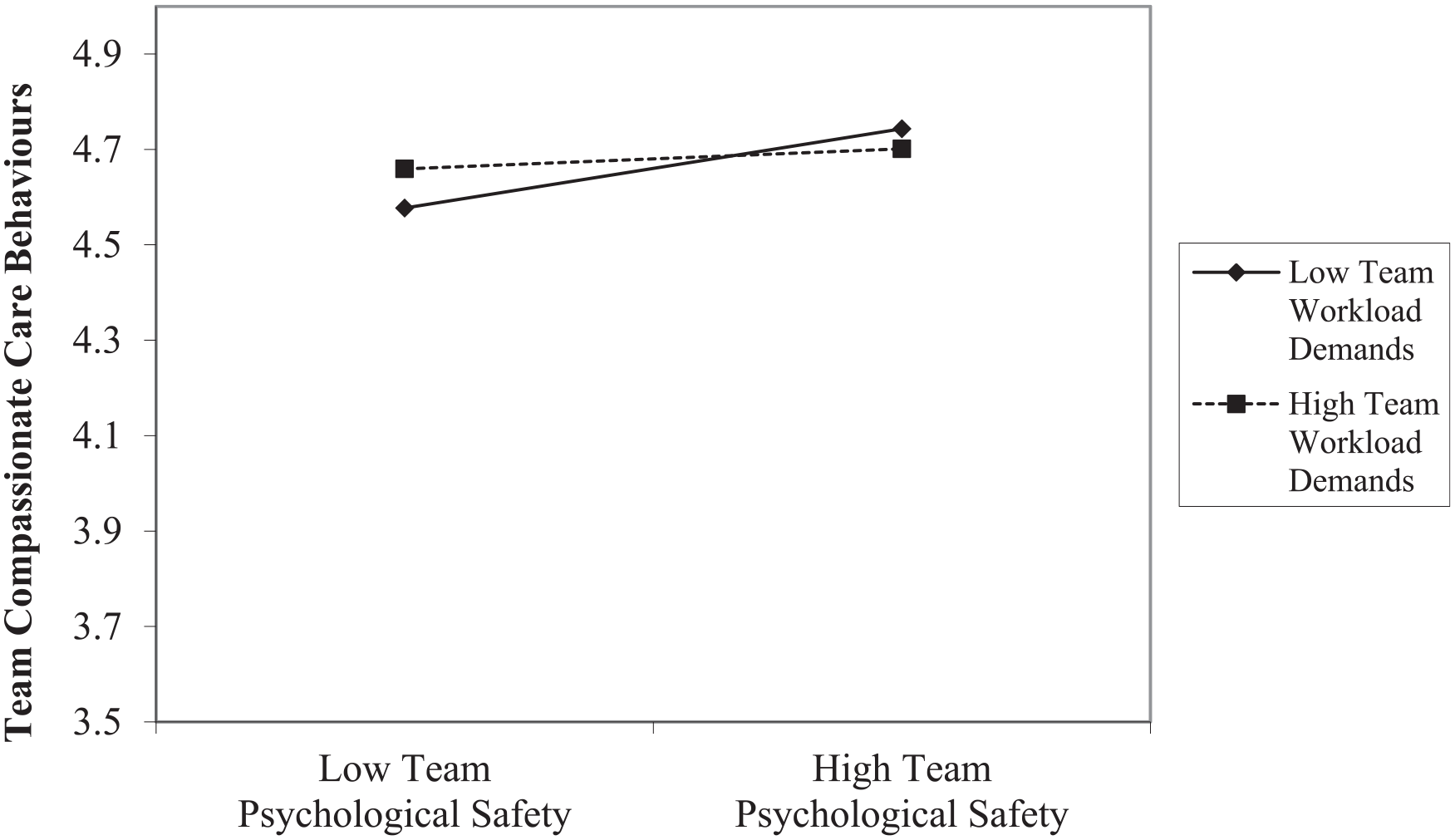
The interaction between team psychological safety and team workload demands in predicting team compassionate care behaviours.
Finally, we tested our moderated-mediation constructing bias-corrected 95% confidence intervals (CIs) on 10,000 bootstrap samples. Effects are considered significant when the bootstrapped 95% CI around the indirect effect does not contain zero. First, we found that team psychological safety had a significant indirect effect on HAIs through team compassionate care behaviours (95% CI (–1.24, –0.05)). In support of Hypothesis 4, we found that team workload demands moderated the indirect effect of team psychological safety on HAIs via team compassionate care behaviours. The conditional indirect effect was significant when team workload demands were lower (–1SD) (95% CI (–0.81, –0.06)) and non-significant when team workload demands were higher (+1SD) (95% CI (–0.44, 0.04)).
6.3.1 Supplementary analysis
In addition to our theoretical model, we assessed the direct relationships between team psychological safety and team workload demands on HAIs. We did not find a significant association between team psychological safety (β = 0.05, SE = 0.10, p = 0.59) nor a significant association between team workload demands (β = 0.12, SE = 0.10, p = 0.24) and HAIs. Together, our findings indicate that the indirect relationship between team psychological safety and future HAIs is mediated by team compassionate care behaviours.
7. Study 1: summary of findings
The findings of the first study show that team compassionate care behaviours can reside at the team level and reflect a shared unit property of the team. This extends Dutton et al. (2002), who argued that leader behaviours can promote compassion in team members. In Study 1, we provide quantitative evidence that team members vary in the level of compassionate behaviour as a function of their team membership. Our findings establish that team compassionate care behaviours are driven by team antecedents, affect team outcomes and are bounded by the team workload demands. Our study, therefore, represents one of the first steps in uncovering the nomological network of team compassionate care behaviours.
Consistent with the literature (Dutton et al., 2014), we find that the social fabric of organisations characteristic of high-quality relationships (i.e. team psychological safety) predicts team compassionate care behaviours. This represents one of the first studies to uncover the drivers of team compassionate care behaviours. Furthermore, we found that team workload demands weakened the positive relationship between team psychological safety and team compassionate care behaviours. This finding highlights potential differences in the conceptualisation of work stressors, such as workload, between levels of analysis. While workload has primarily been examined at the individual level, it is commonly described as a challenge stressor capable of fuelling engagement (Crawford et al., 2010). We find that team workload demands weaken the positive relationships between team psychological safety and team compassionate care behaviours. This supports the idea that high team workload demands can impact how team resources (e.g. psychological safety) relate to compassionate care behaviours (Ni et al., 2022; Razinskas and Hoegl, 2020).
Finally, we highlight the practical utility of team compassionate care behaviours by examining their impact on tangible metrics of team effectiveness and patient safety. This is a critical extension to the literature by demonstrating the broader impact of compassionate behaviours beyond the perceptions of the people providing and receiving compassion, which has attracted limited scholarly attention to date. Furthermore, by investigating HAIs as a metric of team effectiveness, we highlight how team compassionate care behaviours can prevent further suffering by treating and discharging patients in better health than when they were admitted.
While this quantitative study provides insights into the nomological network of team compassionate care, they must also be interpreted cautiously given the static nature of the analysis (please see General Discussion). In particular, the analysis provides limited insight into process of team compassion, how it develops and how it affects team effectiveness, patient care and patient safety. Therefore, we decided to conduct a second study to better understand the direction and nature of relationships between variables and complement and extend our understanding of team compassionate care behaviours.
8. Study 2: a qualitative examination of team compassion
We used a qualitative research design in Study 2 to gain further insights into the forces that shape team compassionate care behaviours towards patients (Kivunja and Kuyini, 2017). Semi-structured interviews allowed participants to elaborate on experiences they believed to be most significant, which is advantageous when there is little in the existing literature on team compassionate care (Brinkmann, 2014). Furthermore, this qualitative approach allowed us to triangulate the quantitative findings of the first study.
9. Method
9.1. Participants and design
The second study aimed to generate experience-focused insights into the findings of Study 1. We interviewed 25 nurses from all positions and levels of seniority from the operating theatre (including pre-admission and post-anaesthesia care/recovery units) of a major metropolitan hospital in Australia (see Table 3). Nurses in this unit were tasked with ensuring that patients were informed and ready for the surgical procedure. During surgery, nurses are responsible for the sterilisation and responsibility of all surgical equipment. Other nurses coordinate the activities of the operating room and advocate for the patient during the surgical procedure. After surgery, nurses monitor patient recovery, including emergence from anaesthesia and pain management.
Study 2 participant sample.

Operating theatre and associated pre-admission and recovery units provide unique insights for studying team compassionate care behaviours and patient care. The surgical setting perhaps represents one of the most vulnerable experiences where patients have limited opportunities to give feedback during their care. Nurses and patients often have more time to develop relationships in standard hospital unit or ward settings compared with the transient flow of patients entering and exiting the operating theatre. In the operating theatre setting, patients and their families often have a limited window to discuss concerns, anxieties and preferences in the pre-admission unit before surgery. During surgery, patients are often heavily sedated, restrained and/or medicated in a closed setting, so nurses must provide care and advocate for patients according to previous wishes without direct patient involvement. After surgery, patients are often confused and can be in distress or pain. In these settings, nurses are tasked with balancing the clinical recovery of patients with patients’ prior wishes and their experience of confusion, anxiety and pain. As such, the compassionate care behaviours provided by nurses in these settings are often highly proactive and discretionary and require them to act according to the wishes of patients and their families without their direct visibility. Operating theatre nurses therefore provide unique perspectives on the role of compassionate care for vulnerable patients.
9.1.1 Interview and data analysis procedure
All interviews, approximately 25 minutes long, were voluntary and conducted in a private setting with only the interviewer and participant present. We developed an interview protocol with five semi-structured questions, which were endorsed by the ethics committee. The five questions provided consistency and a basis for comparing emergent themes between participants. The semi-structured nature of the interview also allowed for unforeseen avenues of discussion to be investigated. Specifically, the five structured interview questions were designed to elicit insights into the relationships between variables identified in the quantitative analysis, such as the participant’s involvement in psychologically safe teams and how that has influenced compassion towards patients. All interviews were audio recorded and subsequently transcribed verbatim. The audio transcriptions were then systematically analysed and reviewed to identify emergent themes articulated by the interviewees. Furthermore, the transcripts were triangulated with the quantitative findings to provide insight into the observed relationships reported in Study 1. These findings resulted in the development of themes, coded alongside the corresponding relationships between variables in Study 1.
9.2. Findings
9.2.1 The relationship between team psychological safety and team compassionate care behaviours
Nurses described a patient’s physical or clinical needs as objective and easier to voice in team settings. The physical or clinical characteristics of the patient were often supported with observable physical evidence, such as medical imaging or tests, that nurses could refer to. Communicating information of a purely clinical nature was considered safe because limited interpretation was required. However, nurses indicated a lack of confidence when speaking to healthcare teams about patients’ emotional well-being and suffering: ‘Emotions are something you perceive, and they might not be true, but physical problems are something you see . . . you can’t always tell with emotional pain because it’s more vague’ (SCRUB2). Nurses indicated that the nature of these subjective assessments was risky to voice to others, given that such sentiments may not be shared or endorsed: ‘I might feel like, emotionally this . . . I’m seeing that patient in one way, but another person might feel [sic] in a different way to you’ (SCRUB2).
Nurses indicated that psychologically safe team environments made them feel more confident in sharing and advocating for subjective assessments of a patient’s emotional needs and suffering. Nurses remarked that when they felt psychologically safe in the team, they felt more confident in sharing and acting on their subjective interpretations of the patient’s emotional state and needs. In these environments, it was: easier to talk about the patient . . . there’s no obstacles along the way, knowing that I’m safe and that I’m able to do what I needed to do, because I feel like I’m supported. (SCRUB1) you can say what you feel needs to be said at any time, no matter who is around you. (SCRUB7) you can say exactly what the patient needs without fear of being judged. (PACU1)
In addition, nurses indicated that psychologically safe teams often translated into greater confidence in the team’s capability and its processes. Psychologically safe teams enabled nurses to feel ‘confident in their skills, their experience, and . . . I feel like we work well as a team together’ (PACU3). This increased confidence in the team provided nurses with the ‘space’ to focus on cultivating compassionate attitudes towards patients because when you know what your teammates are doing, you know that you can rely on them, you haven’t got to watch to make sure somebody is doing this, or somebody is doing that. If it works like clockwork, then compassion just kind of happens. (ANAES7)
9.2.2 The influence of workload demands
Overwhelmingly, nurses indicated that higher workload demands impacted compassionate care behaviours. As summarised by one nurse, ‘compassion isn’t hard, it’s the situation that’s hard’ (SCRUB2). When caring for patients, nurses often appealed to differences between the more clinical and humanistic aspects of care: I can deal with a deteriorating patient with, like a heart rate or a systolic blood pressure or whatever, I don’t mind dealing with that. But I find pain makes me quite stressed . . . I don’t like seeing people in pain at all. (PACU2)
When workloads were higher, nurses reported focusing on the fundamentals of clinical care where ‘there is this emphasis on speed rather than care . . . I have been in environments where patients have expressed to me that they feel that it’s a factory, they feel that they’re just one of the numbers’ (ANAES6). Nurses indicated that despite feelings of empathy and compassion, high team workload demands made them feel ‘squeezed’. As a result, nurses reported compressing the development of feelings towards patients and their corresponding compassionate care behaviours: Time constraints are something which always hinder you from being able to take [good] care of the patient. You want to do so much but you have no time. (SCRUB2) Time stops you from being [able] to individualise your care . . . to properly care for your patients as you would like to. (ANAES9)
Environments characterised by high workload demands not only created an emphasis on speed but also exacerbated feelings of staff fatigue and exhaustion. This fatigue made it more difficult for nurses to engage in compassionate care: ‘fatigue makes it harder to work to the best of your abilities. You will still try your best . . . but it’s just a battle, showing up with your fatigue and then trying to still care for patients’ (PACU1). In these high workload environments, fatigued nurses often reported making a conscious choice to withdraw from the compassionate elements of care: ‘I deliberately make the choice. I’m really shattered. I’m so tired. I really don’t have the energy to be feeling the feelings. I deliberately have to make the decision’ (ANAES3). Such strategies represent a form of ‘self-protection’ (ANAES6) and as ‘one way of coping. It’s either gonna [sic] crush you mentally or . . . you become . . . detached’ (SCRUB3).
9.2.3 The relationship between compassionate care behaviours and patient outcomes
Nurses believed that ‘being more compassionate means extending your care beyond what other people deliver, or what you think you can deliver. So, it’s bringing your top-of-the-game type of care’ (PACU1). Nurses indicated that compassionate care enabled stronger relationships with patients: ‘they’ll never remember that you gave them their medications on time, but they’ll always remember if you fluffed their pillow and you cared’ (PACU4).
Nurses indicated that showing compassion signalled their commitment to patients. As a result, nurses felt that patients were more likely to share information they may have withheld from others: ‘tell you stuff, they’ll disclose stuff, they’ll tell you how they really feel’ (PACU4). Compassion provided a safe ‘window with your patient. . .and they’ll come out with stuff that they haven’t told anybody’ (ANAES6). Nurses indicated that compassion enabled them to possess a greater pool of knowledge about patients, which was critical in providing care and preventing adverse clinical outcomes. Such patients were easier to care for . . . because they can let you know more about the pain or they might say ‘that’s funny, you mentioned this earlier and now my foot feels a bit different’ . . . I don’t think they’re always forthcoming with that information, which may be important. (PACU4)
Furthermore, nurses indicated that compassion allowed patients to take more ownership of their care and maintain their independence and self-identity. Nurses indicated that compassion provides patients with a ‘semblance of control that enhances their experience’ when ‘coming into hospital, when they get sick . . . they lose control’ (ANAES9). This input into their care and control ‘helps their recovery; I think it also helps them decrease their anxiety, which will help with their recovery, decreasing anxiety helps with them recovering from their operation’ (SCRUB9).
10. Discussion
Research on compassion typically focuses on the role of individual differences with little attention to how team forces can shape the process of compassion. In addition, there is little empirical evidence on the broader objective impact of compassionate behaviours beyond the perceptions of the person providing and receiving compassion. This article contributes to the compassion literature by examining team compassionate care behaviours in healthcare settings. We found support for team compassionate care behaviours as a team phenomenon, with team antecedents and downstream impacts on objective measures of team patient safety.
Our article establishes that team compassionate care behaviours are driven by shared unit properties and can vary between teams. In doing so, we show that work teams are not simply an ‘enabling’ condition that drives an individual practice of compassion (Dutton et al., 2014) but also a source of compassion. Critically, we establish that team compassion has benefits on an objective downstream indicator of enhancing patient safety outcomes. Quantitatively, we show that team compassionate care behaviours were associated with fewer patient safety incidents (HAIs) over 12 months. Our qualitative findings enriched the quantitative findings by revealing how compassionate care can engender feelings of trust, enabling healthcare professionals to be proactive in their clinical decision-making for the benefit of patients. Therefore, these teams were more likely to treat and discharge patients in better health than when they were admitted, which is not only a core mission of healthcare facilities but also contributes to the broader objective metrics of care and hospital effectiveness. Compassionate care behaviours, therefore, are not only a reaction to suffering but can also prevent further suffering.
Second, we contribute to the literature by identifying the specific team forces driving compassion within teams, which extends Dutton et al.’s (2014) theorisation of the organisational context in cultivating compassion. While Dutton et al. (2014) highlighted the value of high-quality relationships between individuals in creating the values and norms for organisational compassion, these high-quality relationships can take many forms. We find that the emergent state of team psychological safety (i.e. the pattern of interactions between team members that enable them to take interpersonal risks because they feel safe) is a critical factor in what constitutes these high-quality relationships. Our quantitative findings reinforce Lilius et al. (2011), who reported that feelings of safety within teams enabled norms of collective empathic concern. Furthermore, our qualitative findings highlight how team psychological safety drives team compassion. Nurses reported that feeling safe within the team enabled them to speak honestly and candidly about subjective elements of patient care, which led to the collective team noticing and acting on patient suffering. Our findings therefore contribute to the compassion literature by extending the work of Dutton et al. (2006, 2014) and Lilius et al. (2011) by identifying and empirically testing the specific team antecedent that promotes collective compassion beyond individuals.
However, the positive relationship between team psychological safety and team compassionate care behaviours was weakened by high team workload demands. Studies examining the influence of team work pace and intensity have attracted less scholarly attention, which is surprising given that workload demands are a feature of the organisational environment (French et al., 1982; Karasek, 1979; Lazarus and Folkman, 1984). Specifically, our findings indicate that team psychological safety leads to lower HAIs via team compassionate care behaviours, but only when team workload demands are low.
Our findings on team psychological safety in driving team compassion behaviours and the critical role of team workload demands in buffering this relationship speak to recent developments in the conservation of resource (COR) literature (Hobfoll et al., 2018). Although COR is primarily examined at the individual level, recent developments in the team literature argue that interactions between team members enable resources to cross over from one individual to another (Stoverink et al., 2020). Within healthcare, compassionate behaviours are likely to be perceived by teams as a valuable resource that helps achieve work goals (e.g. Halbesleben et al., 2014; Hobfoll et al., 2018). These compassionate resources likely ‘cross over’ to other team members and act as a recursive foundation for the emergence of shared compassionate team resources and the development of normative team-level behaviours. Furthermore, COR indicates that resources enable further resource gains and the development of positive-gain spirals (Hobfoll, 1989). To this end, team psychological safety, which has previously been conceptualised as a key team resource (Stoverink et al., 2020), helps cultivate the development of team compassion resources and its associations with patient safety.
In contrast, team workload demands likely represent a threat to resources. Nurses in our qualitative study reported the need to prioritise their time, energy and effort. Others reported feeling ‘squeezed’, having to focus on speed, or withdrawing from compassionate elements of care and detaching themselves from patients to focus on task completion. According to COR, this threat of resource loss leads the team to adopt a protection strategy to conserve resources. Therefore, under conditions of low workload demands, psychologically safe teams are likely to invest resources (e.g. time, energy and effort) to cultivate team compassionate care. But when team workload demands are high, resources are threatened and the team may not have the capacity to cultivate compassionate responding (Ni et al., 2020; Razinskas and Hoegl, 2020).
In the healthcare context, tasks completed under high workload demands are likely to encompass action directly associated with patient mortality outcomes. Under these circumstances, compassion can be seen as a ‘nice to have’, relegated when workload demands are high (Sinclair et al., 2016). While this narrowing of attention to focus on tasks is understandable, our findings indicate that this may be associated with future adverse patient safety incidents such as HAIs. This speaks to the idea of loss spirals in COR, whereby those who lack resources are susceptible to more resource loss (Hobfoll, 1989). In our research context, when resources are threatened by high team workload demands, the team may be less inclined to invest in the development of shared team resources that enable compassionate responding, ironically leading to teams expending more resources in the care of patients adversely affected by HAIs. On the contrary, teams with lower workload demands can invest resources to engage in compassionate care behaviours, reducing the incidence of HAIs and leading to faster recovery and discharge of patients. Ironically, the investment of resources reduces the workload demands of the team.
10.1. Practical implications and future research
Work is being increasingly conducted in teams whereby team members are interchangeable (Kozlowski and Ilgen, 2006). Repeated interactions between customers and employees are rarely characterised by one-to-one, but instead by one-to-many. Therefore, it is practically important to examine the compassionate behaviours practised by the team as a collective unit to assess the overall quality and consistency of care received by patients. Our findings indicate that compassion is not just a ‘nice to have’, but critical in safeguarding patient safety. Together, both studies show that team compassionate care behaviours not only alleviate emotional suffering but are also associated with tangible benefits in providing safer patient care. Our findings indicate that team compassionate care behaviours are higher when teams are psychologically safe. The higher quality of relationships between members of psychologically safe teams may be associated with ripple effects on the way members of teams interact with their patients. One practical way to promote psychological safety in healthcare teams is to introduce and embed the practice of daily safety huddles (Shaikh, 2020). Regular and structured safety huddles, also referred to as daily safety briefings, daily check-ins or daily safety calls, allow healthcare teams to voice concerns and risks from both the patient and staff perspectives. Such initiatives have been shown to facilitate team communication (Shaikh, 2020). These regular safety huddles can encourage psychological safety by empowering healthcare teams to build a culture of collaboration that improves patient safety, including rates of medication errors, unrecognised clinical deterioration and other serious safety events (Brady et al., 2013; Goldenhar et al., 2013; Stapley et al., 2018).
Leadership is often a key driver of team psychological safety (Edmondson and Lei, 2014). Furthermore, research indicates that leaders can help develop a culture of patient-centred compassionate care by exemplifying compassion in their leadership (Shipton et al., 2008; The King’s Fund, 2014). In teams with high levels of psychological safety, leaders facilitate rather than direct, ensuring that all voices are heard and valued (West, 2021). Compassionate leadership is also associated with beneficial workforce outcomes such as reduced staff stress and absenteeism (Lyubovnikova et al., 2015; West et al., 2014), which can alleviate workload pressures. Healthcare organisations may look to create person-centred compassionate care leadership programmes to equip healthcare leaders with the skills to create psychologically safe team environments and embed a shared team vision around how to provide patient-centred compassionate care (Murray and Tuqiri, 2020).
Our findings highlight the critical role of manageable workload demands. Our research shows that team psychological safety led to fewer patient safety incidents, namely HAIs, via team compassionate care behaviours, but only when team workload demands were low. This finding is supported by Hunsaker et al. (2015), who found that work environments shaped nurses’ provision of compassionate care behaviours. In particular, most people who enter nursing are already highly motivated to provide compassionate care (Horsburgh and Ross, 2013). As such, high workload demands appear to be a key barrier to the valued practice of compassionate care behaviours and patient safety. Healthcare managers should be mindful of the impact of high workload demands, which are more acute than ever given pressing challenges such as increasing rates of nurse burnout and challenges in recruitment and retention in nursing (Haddad et al., 2022).).
One notable limitation of our studies is our conceptualisation of compassionate care behaviours in teams. Compassion towards another is a construct contingent on an interaction between two or more people (in this study, nurses and patients). However, our measure of team compassionate care behaviours in Study 1 and our interviews in Study 2 captured only the views of nurses rather than triangulating perceptions of both nurses and patients. Despite this, our findings indicate that the perceptions of healthcare teams predict objective indicators of patient safety. Future research may benefit from acquiring survey and interview data from both provider and recipient of compassion. Likewise, this article focuses on HAIs as a critical indicator of team effectiveness and patient safety. Future research should consider the impact of compassionate care behaviours on other forms of adverse patient safety outcomes. The Australian Commission on Safety and Quality in Health Care (ACSQHC, 2018) recognises 15 other complications acquired in healthcare. The impact of team compassion care behaviours on these other types of adverse patient safety incidents is currently unknown.
We proposed a positive relationship between team psychological safety and team compassionate care by drawing on the extant literature (see Edmondson and Bransby, 2023 for review). Psychological safety is inextricably associated with voice and sharing of perspectives in team settings because psychological safety is characterised by assessments of interpersonal risk-taking. We argued that team psychological safety was positively associated with team compassionate care behaviours because it allowed nurses to share their perspectives on patient suffering, which then afforded the team a shared understanding to alleviate patient suffering. However, we did not measure these intermediate processes, namely, the extent to which nurses voiced as a result of team psychological safety or the extent to which team members developed more comprehensive insights due to team voice. However, our qualitative interviews indicated that nurses felt less safe sharing their observations about patient suffering due to the subjective nature of these assessments (compared with diagnostic reports), but that psychological safety allowed them to take these risks and disclose such insights without the fear of being ‘judged’. Although we were unable to quantitatively map how team psychological safety specifically translates into more team compassionate team behaviours, insights from existing theory along with our qualitative interviews support our claims. Compassion theories, however, will benefit from future studies that demonstrate how emergent states transform into compassionate behaviours.
It is also worth noting that the cross-sectional design of the survey in Study 1 fails to capture how team psychological safety, team compassionate care behaviours and team workload demands might relate to each other over time. For example, without longitudinal analyses, this study cannot offer insight into how team psychological safety at one point in time may impact team compassionate care behaviours at a later point in time. Our interviews suggest that these variables unfold over time, but future quantitative studies may benefit by considering a time-lagged series approach.
Furthermore, there are no archetypal contexts representative of all healthcare team environments. Medical practices, aged care homes, disability support workers, at home care and different hospital departments represent different clinical settings, all with a potentially different interpretation of workload demands, team psychological safety and compassionate care. Furthermore, while Study 1 attempted to obtain a representative sample by collecting survey data from eight health facilities in a local health district, the qualitative explanations in Study 2 were only conducted in an operating theatre context, potentially limiting the explanation of the findings. Future research should therefore seek to triangulate these qualitative explanations between different healthcare settings.
Overall, this article highlights that compassion is more than just a ‘nice to have’ in the workplace. Our article provides evidence that compassion emerges at the team level, is driven by team antecedents, is moderated by team environments and influences team outcomes. Specifically, we find that teams characterised by high psychological safety engage in more team compassionate care behaviours, which highlights the role of emergent team processes. Within healthcare settings, team compassionate care behaviours appear to safeguard patients from experiencing further suffering post-admission. Together, the findings highlight that engaging in compassion is a critical force in shaping team effectiveness and enhancing an organisation’s ability to meet its purpose and objectives, especially when the organisation strives to alleviate the suffering of others.
Footnotes
Appendix 1
Acknowledgements
We thank all the participants and supporters for their engagement with the study.
Final transcript accepted on 27 June 2024 by Lynne Reeder (AE Special Issue).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Australian Research Council’s Linkage (project number LP160100505) funding scheme.