
Abstract
The study objective was to determine the incidence of complications from induced hypertension used to treat delayed cerebral ischaemia (DCI) complicating aneurysmal subarachnoid haemorrhage (aSAH). Induced hypertension (IH) was defined as the use of vasopressors to achieve a supraphysiological systolic blood pressure target. A single-centre retrospective, observational cohort study was undertaken at the Royal Adelaide Hospital intensive care unit. Data are presented as predominantly median (interquartile range (IQR)). All patients admitted with a diagnosis of aSAH between 1 April 2020 and 1 April 2022 were included and analysed according to whether they did or did not receive vasopressors for IH. A total of 109 patients were included, of which 29 (27%) received vasopressors for IH (median age 58 (IQR 52–65) years, 65% female) and 80 did not receive IH (median age 55 (IQR 49–71) years, 62% female). Clinical DCI or radiological evidence of vasospasm were present in all patients given IH and in 16% of non-IH patients. Patients in the IH group had more ischaemic electrocardiogram (ECG) changes (17.2% vs 2.5%, P = 0.01), urine output (4807 (IQR 3186–5720) ml/day vs 2125 (IQR 1650–2760) ml/day, P < 0.001), fluid administration (4895 (IQR 3555–5999) ml/day vs 2704 (IQR 2300–3403) ml/day, P < 0.001) and intravenous potassium replacement (13 (IQR 5–24) mmol/day vs 5 (IQR 0–13) mmol/day, P = 0.001) than those in the non-IH group. IH was also associated with a greater incidence of hyponatraemia (58% vs 34%, P = 0.02). IH was not associated with arrhythmias or rebleeding. Mortality rates were 17% vs 20% (P > 0.9) in the IH and non-IH groups respectively. In conclusion, IH for the treatment of DCI following aSAH was associated with an increased rate of ischaemic ECG changes, increased urine output and hyponatraemia. However, in the IH group there was no increased rate of rebleeding, and 48% of the IH patients had an improvement in their neurological function following commencement of treatment.
Keywords
Introduction
Aneurysmal subarachnoid haemorrhage (aSAH) has an incidence of 10.3 cases per 100,000 person-years or about 2500 cases per year in Australia, and this incidence increases with age. 1 Well-recognised complications of aSAH are radiological cerebral vasospasm and delayed cerebral ischaemia (DCI), which occur in up to 30% of patients and are associated with significant morbidity and mortality
In recent years the mortality associated with aSAH has declined, thought to be predominantly due to improvement in prevention of rebleeding by aneurysm securement and advances in neurocritical care. Despite this, radiological cerebral vasospasm remains a significant issue, with no specific therapy proven to improve patient-centred outcomes. It is thought radiological cerebral vasospasm is triggered by the breakdown of blood products which accumulate in the subarachnoid and perivascular spaces. Specifically, oxyhaemoglobin is believed to cause direct vasoconstriction, release of arachidonic metabolites, promotion of free radical reactions and inhibition of endothelium-dependent vasodilation through nitric oxide scavenging. 2 However, cerebral vasospasm is only one aspect of the complex pathophysiology process which contributes to DCI in these patients. 3 The hypothesis of this multifaceted development of DCI is supported by clinical trials which have shown no clear association between outcomes and the prevention of cerebral vasospasm. In the BRANT study by Pickard et al, prophylactic nimodipine was found to be associated with an improvement in functional outcomes, without showing a decrease in the incidence of vasospasm. 4 Nimodipine is now used routinely in Australia with a view to improve functional outcomes following subarachnoid haemorrhage. The CONSCIOUS trials showed a reduction in the incidence of moderate–severe vasospasm but no significant improvement in patient-centred outcomes.5,6
Current international guidelines for the treatment of DCI are tier based, with the first-line therapy including volume optimisation and induced hypertension (IH). 7 Despite encouraging observational studies suggesting benefit, 8 to our knowledge, there have been no randomised clinical trials demonstrating a mortality or functional outcome benefit with IH. A recent attempt ceased early due to poor recruitment, 9 reportedly owing to a loss of equipoise amongst clinicians, many of whom believe there is benefit from IH. Given that the study was ceased early, the conclusion that there is no clear evidence of improved outcomes and IH can be associated with frequent significant adverse effects 9 should be treated with caution. In this study the reported rate of serious adverse events was 11 (52%) in the IH group versus five (25%) in the non-IH group, with a relative risk of 2.1 (95% confidence interval 0.9 to 5.0). Serious adverse events reported in the IH group compared with the non-IH group included death (6 vs 4), pneumothorax (2 vs 0), atrial fibrillation (1 vs 0), myocardial infarction (2 vs 0) and electrocardiogram (ECG) changes (0 vs 1). This study was ceased after recruiting only 41 patients so was underpowered to demonstrate benefit or accurately quantify adverse effects. Hence complications of IH remain unquantified.
The object of this study was to quantify the incidence of pre-defined complications in patients with aSAH who develop radiological evidence of vasospasm and DCI who subsequently receive induced hypertensive therapy at a single Australian tertiary referral intensive care unit (ICU).
Methods
Study design, setting and population
This is a single-centre retrospective, observational cohort study of patients admitted to the Royal Adelaide Hospital ICU between 1 April 2020 and 1 April 2022 with an admission diagnosis of aSAH. The two-year cohort was chosen based on an estimate of the number of patients admitted each year to the Royal Adelaide Hospital with bleeding from aSAH (75 per year). Of an expected 150 patients, we anticipated 33% would go on to develop DCI and hence about 50 patients would be treated with IH. IH was defined as the use of vasopressors to achieve a pre-specified hypertensive systolic blood pressure target. While no formal power calculation was performed given the multiple complications that were being investigated, the investigators proposed that data from this number of patients would provide useful information on types and frequencies of complications. It was approved by the Central Adelaide Local Health Network Human Research Ethics Committee (CALHN HREC), reference number 17062 on 17 November 2022, with the need for consent waived.
Data collection
Eligible patients were identified from the Australian and New Zealand Intensive Care Society – Adult Patient Database (ANZICS-APD), being those with an Acute Physiology and Chronic Health Evaluation (APACHE3) admission diagnosis of subarachnoid haemorrhage, with cases other than acute aSAH excluded (Figure 1). Data were extracted manually by two investigators, who were not blinded to the treatment received, from the Adult Patient Database and the electronic medical record including imaging reports and pathology results. Data included demographic characteristics, documented past medical history of hypertension in the admission note, mechanism of and time to securement of aneurysm, in-hospital mortality, discharge destination, hospital and ICU length of stay (LOS). The highest and lowest values for a number of recorded electrolyte concentrations were collected over the duration of the ICU stay (sodium, potassium and magnesium). Total fluid balance was collected for the duration of the ICU admission and values divided by their LOS to give a daily average. Input included nasogastric feeds, medication infusions and intravenous (IV) fluids, while output was urinary output. Other losses were either incompletely documented such as stool/nasogastric losses or small volumes (e.g. external ventricular drain drainage, routine blood sampling) and it was decided not to include these in the analysis.
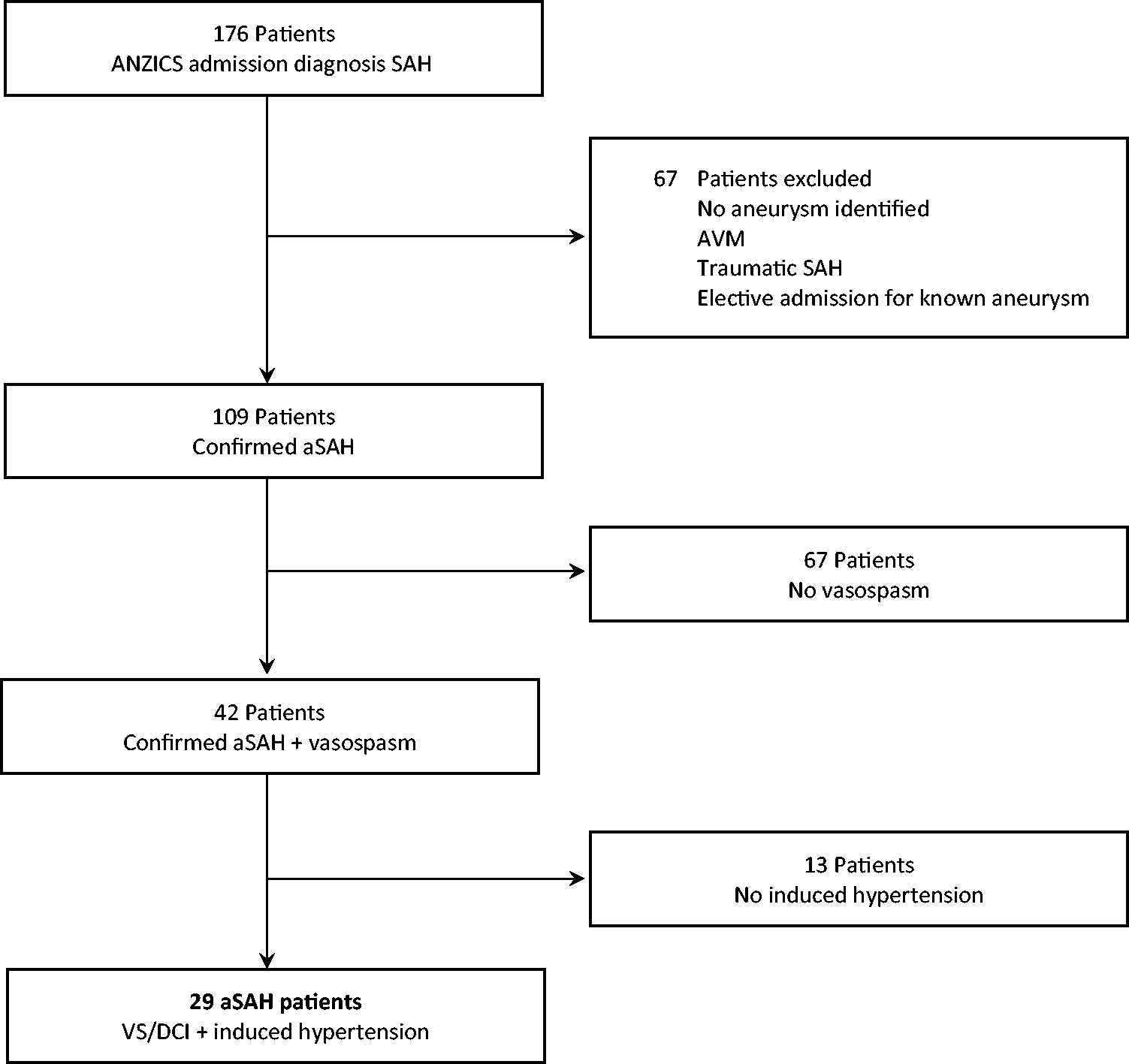
CONSORT flow diagram. ANZICS: Australian and New Zealand Intensive Care Society; SAH: subarachnoid haemorrhage; AVM: arteriovenous malformation; aSAH: aneurysmal subarachnoid haemorrhage; VS: vasospasm; DCI: delayed cerebral ischaemia.
In regard to complications, specific terms and phrases were sought by manual review to denote certain conditions. Terms sought in medical imaging reports included ‘vasospasm’, ‘perfusion defect’ and ‘pulmonary oedema’. In the patients’ notes, phrases looked for included ‘fluid overload’, ‘pitting oedema’, ‘ischaemic ECG changes’, ‘new T wave inversion’, ‘new ST depression’ or documentation about new arrhythmias (atrial fibrillation, ventricular tachycardia, ventricular fibrillation) or haemorrhage. Vasospasm was considered present radiologically when a computed tomography (CT) angiogram and/or CT perfusion imaging report included the term ‘vasospasm’ or ‘perfusion defect’. DCI was recorded if there was a decrease in Glasgow Coma Score (GCS) by two or more points and/or the development of new focal neurological signs with the treating team assessment being that the cause was vasospasm.
Post commencement of IH, blood pressure was measured via invasive blood pressure monitoring and zeroed at the phlebostatic axis. We also looked for documented evidence of improvement in neurological function, either an improvement in GCS by two or more points or resolution of focal neurological deficit.
Data sharing
The data that support the findings of this study are available from the corresponding author upon reasonable request. Despite the data being de-identified, they are not publicly available owing to privacy or ethical restrictions, as they contain information that could compromise the privacy of research participants. Data can be shared with researchers who meet the criteria for access to confidential data, subject to approval from the CALHN HREC, which provided oversight for this study. Requests for data access should include a brief proposal outlining the intended use of the data.
Statistical analysis
Electronic medical record data were recorded into a purpose-written REDCap electronic data capture tool database.10,11 Summary data are presented as number (%), mean (standard deviation (SD)) or median (interquartile range (IQR)), as indicated. Between-group comparisons were performed by Student’s t-test or rank sum test for continuous variables and by chi-square or Fisher’s exact test for categorical variables respectively. No imputation was undertaken for missing data and missing data are reported only if more than 5% of data was missing. As this study is observational, P-values are provided for perspective without adjustment for multiple comparisons and no specific level of significance was assigned. All analyses were undertaken using Stata MP/17.0 (StataCorp LLC).
Results
There were 176 patients identified from the ANZICS-APD, with 109 confirmed (aSAH), of whom 29 (27%) received vasopressors to induce hypertension (Figure 1). Of the 109 patients with aSAH, 42 (39%) had angiographic vasospasm and 28 (27%) had clinical evidence of DCI (Table 1). Of the 29 patients with IH, 23 (79%) had clinical DCI at commencement, with 70% having a decrease in GCS by two or more points and 39% developing focal neurological deficits. The median age was 58 (IQR 52 to 65] years, 19 (65%) were female and 15 (54%) had a past history of hypertension (Table 1). The procedures performed on patients during their ICU stay are included in Table 2, with external ventricular drain (EVD) insertion being the most common overall. In patients who were treated with IH the average daily dose of noradrenaline was 8 (IQR 5–14) µg/min to achieve the specified systolic blood pressure target throughout the period of IH. The initial targeted systolic blood pressure was greater than 160 mmHg in 68% of cases and greater than 180 mmHg in 32% of cases, with the median highest noradrenaline dose being 35 (IQR 30–44) µg/min. The systolic blood pressure target and the duration of vasopressor therapy (median of 144 (IQR 66–276) h in the IH group) were altered pending clinical response to therapy. In eight (28%) patients who received IH, the blood pressure target was lowered owing to concerns about the high dose of vasopressor required to achieve the blood pressure target. Of patients who were treated with IH, 66% went on to have rescue intra-arterial verapamil owing to persistent DCI. External ventricular drain insertion was more common in those who were treated with IH: 66% vs 30% in the non-IH group.
Patient characteristics with or without treatment with induced hypertension.
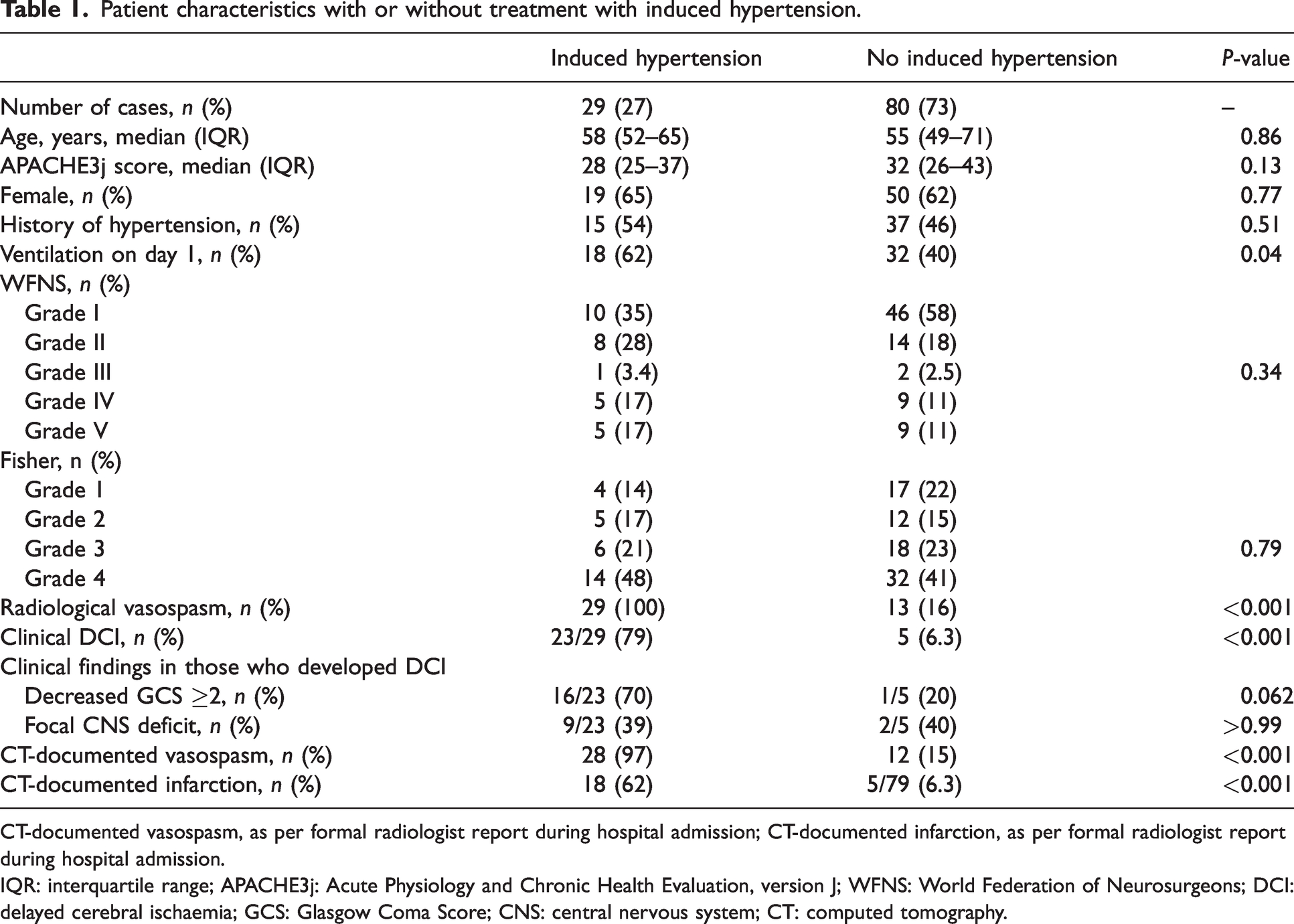
CT-documented vasospasm, as per formal radiologist report during hospital admission; CT-documented infarction, as per formal radiologist report during hospital admission.
IQR: interquartile range; APACHE3j: Acute Physiology and Chronic Health Evaluation, version J; WFNS: World Federation of Neurosurgeons; DCI: delayed cerebral ischaemia; GCS: Glasgow Coma Score; CNS: central nervous system; CT: computed tomography.
Interventions performed.
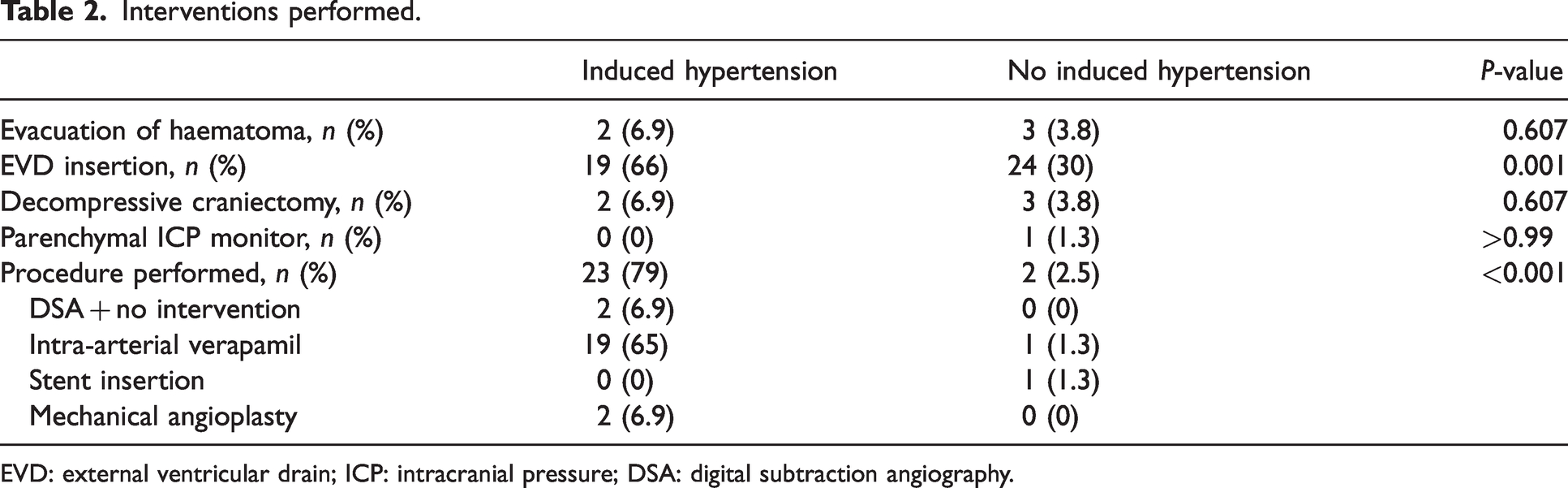
EVD: external ventricular drain; ICP: intracranial pressure; DSA: digital subtraction angiography.
In 11 (48%) cases of clinical DCI there was an association between commencement of IH and documented improvement in neurological function. Thirteen patients (38%) with radiological vasospasm did not receive IH, because either 1) the prescribed systolic blood pressure target was achieved without vasopressors, or 2) they had symptom resolution prior to commencement, or 3) they never developed clinical DCI. Five patients who developed DCI did not go on to have IH owing to symptom resolution without the use of vasopressors.
In regard to specific complications, documented dynamic ECG changes were more common in the IH group. These changes were new T wave inversion or ST depression. Peak troponin levels were recorded for 15 (52%) patients in the IH group vs 24 (30%) patients in the non-IH group (Table 3). The troponin values were abnormal in seven (24%) patients with IH and eight (10%) in the non-IH group. There was no difference in the documented rates of rebleed, pulmonary oedema, fluid overload or arrhythmias (Table 3).
Defined complications with or without treatment with induced hypertension.
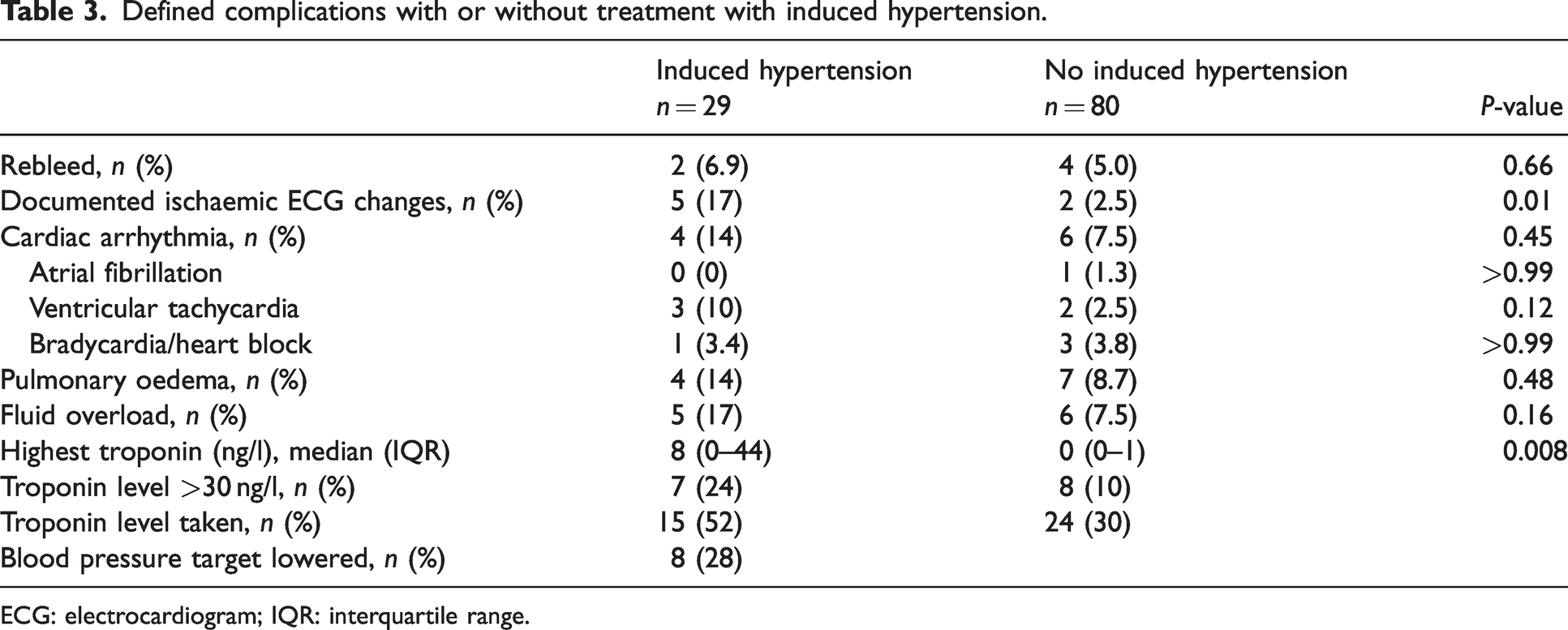
ECG: electrocardiogram; IQR: interquartile range.
Two patients in the IH group developed new haemorrhage as a complication. One of these originated from the region of a clipped aneurysm; however, it was unclear whether this bleeding was from residual aneurysm or haemorrhage in nearby infarcted tissue. The other occurred in a patient whose aneurysm could not be identified on presentation CT angiogram or digital subtraction angiography but subsequently developed DCI. While receiving 40 µg/min of noradrenaline to achieve IH, neuroimaging revealed an aneurysm. The patient went on to have a coiling procedure, while receiving IH, which was complicated by further bleeding from the aneurysm.
One patient undergoing IH had a clinically significant bleed from a femoral artery access site which had previously had an arterial sheath to facilitate intra-arterial verapamil administration.
Of the four patients who had a rebleed in the non-IH group, two occurred during the coiling procedure; one was in the context of a complex aneurysm which required stenting and coils then subsequent anticoagulation; and the other occurred shortly after arrival to hospital prior to aneurysm securement.
The IH group had a number of complications related to fluid and electrolytes. The urine output was higher in the IH group compared with the non-IH group, 4807 (IQR 3186–5720) ml/day vs 2125 (IQR 1650–2760) ml/day (P < 0.001). The IH group daily fluid intake and IV potassium replacement were also significantly greater, with mean fluid administration of 4895 (IQR 3555–5999) ml/day versus 2704 (IQR 2300–3403) ml/day (P < 0.001) and mean IV potassium replacement of 13 (IQR 5–24) mmol/day vs 5 (IQR 0–13) mmol/day (P = 0.001), not including the potassium in any maintenance fluid or enteral potassium replacement. There was also an increase in patients with hyponatraemia, lower urea and creatinine levels. More patients received hypertonic saline in the IH group (Table 4). Eleven patients received a dose of frusemide while in ICU, four (14%) in the IH and seven (9%) in the non-IH group.
Fluid balance and electrolyte levels for patients with or without treatment with induced hypertension.
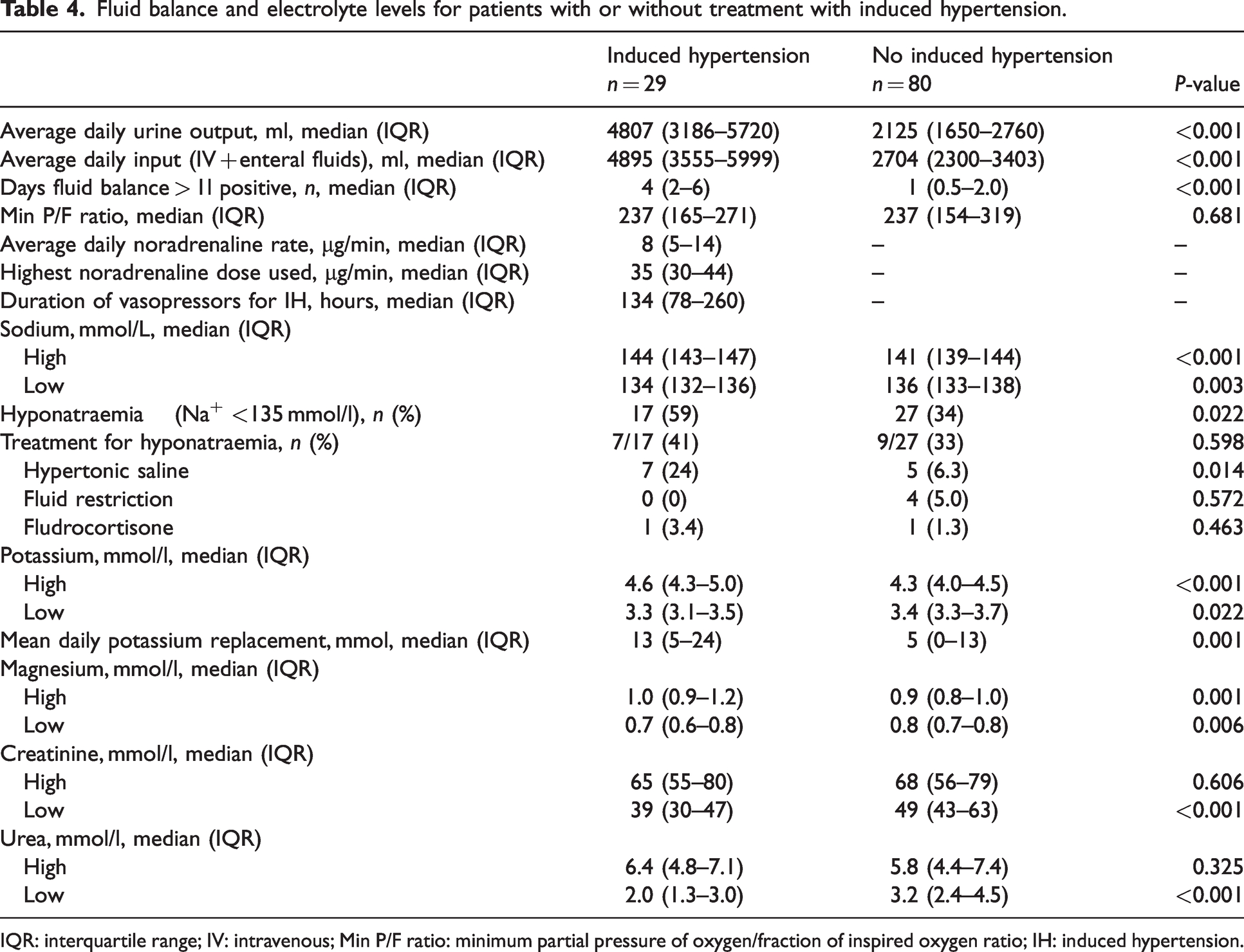
IQR: interquartile range; IV: intravenous; Min P/F ratio: minimum partial pressure of oxygen/fraction of inspired oxygen ratio; IH: induced hypertension.
The patient group who received IH had a longer LOS in ICU and hospital (Table 5) and were more likely to be discharged to a rehabilitation facility rather than home (rehabilitation facility 72% vs 33% for the non-IH group, home 10% vs 47% for the non-IH group).
Outcomes for patients with or without treatment with induced hypertension.
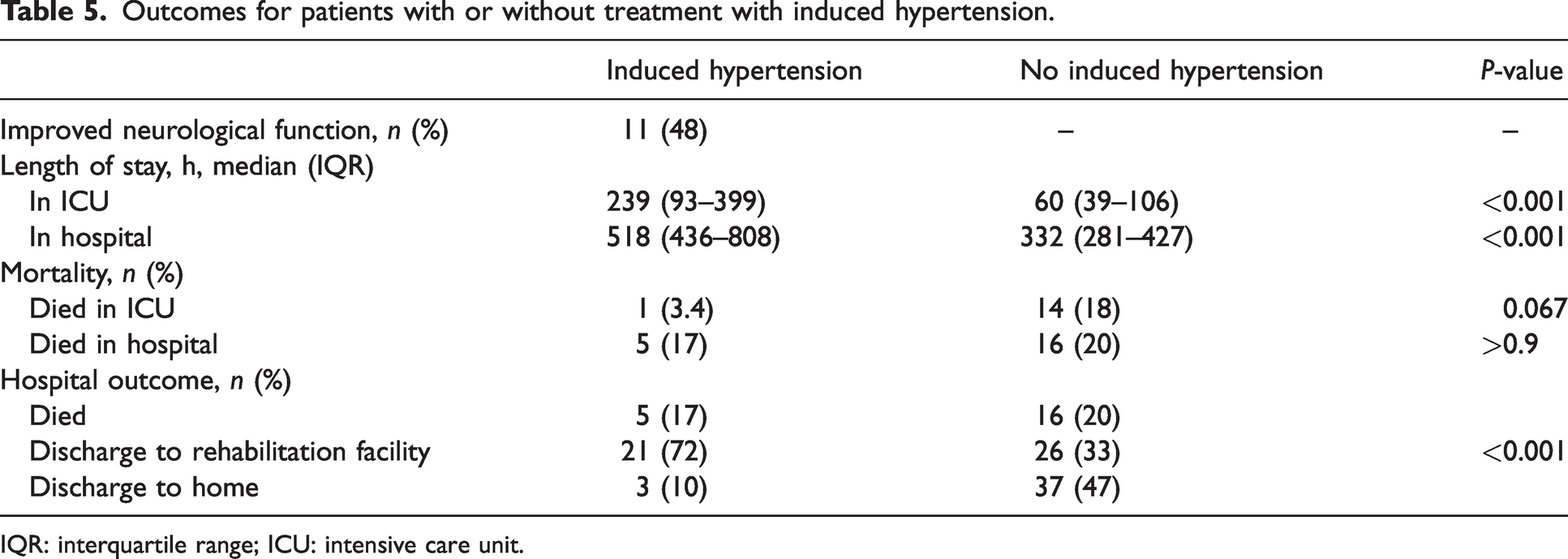
IQR: interquartile range; ICU: intensive care unit.
The majority of patients, 99 (91%), had their aneurysms secured: 68 (69%) coiled, 27 (27%) clipped and four (4%) stented. Endovascular coiling occurred earlier than craniotomy and clipping (Figure 2).
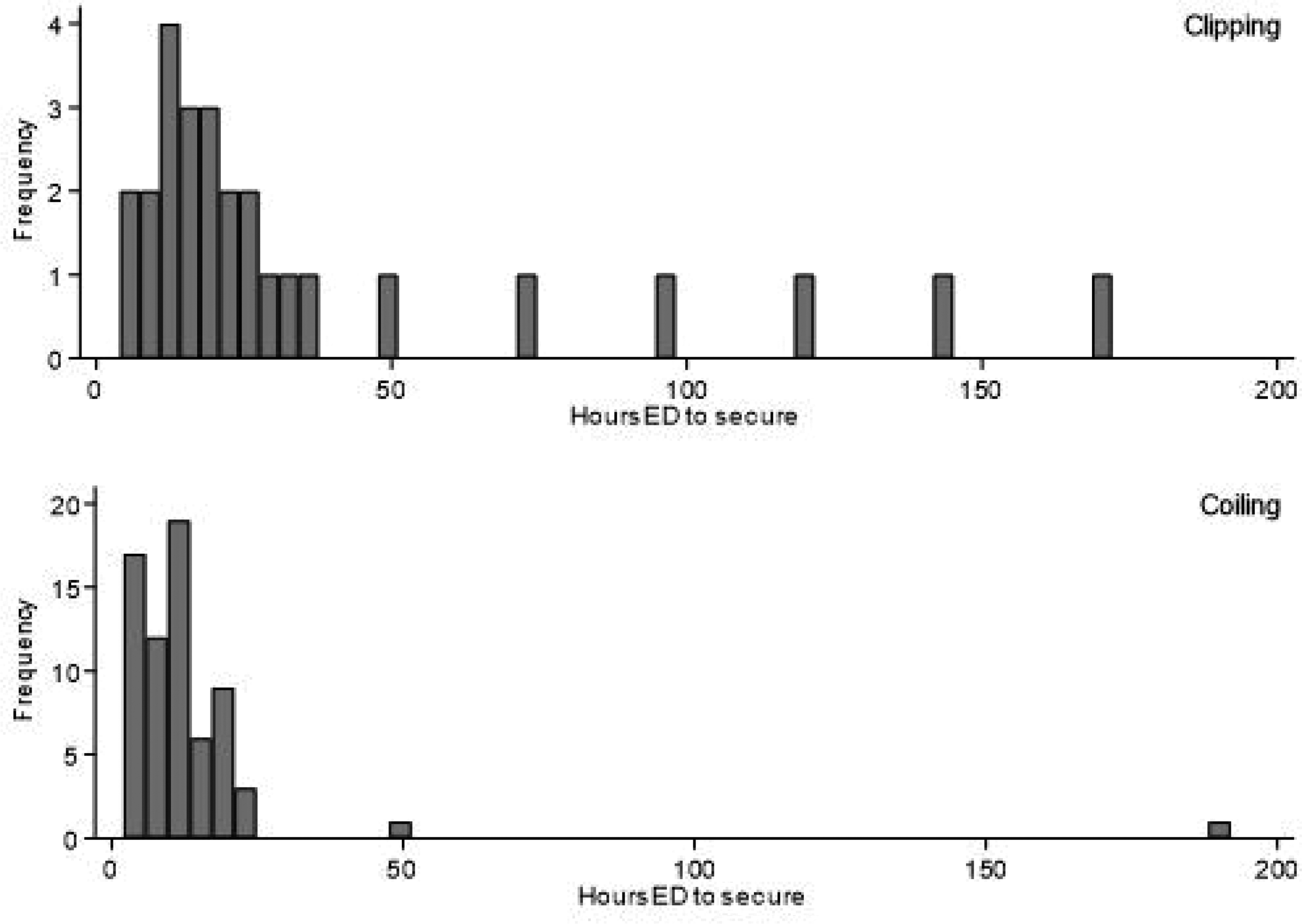
Time in hours from emergency department (ED) presentation to securement of aneurysm, clipping versus coiling.
Discussion
This retrospective observational study reports the complications of IH via vasopressors used to treat vasospasm complicating aSAH in all patients from a single site over a two-year period. The results suggest a relationship between IH and ECG changes consistent with ischaemia as well as polyuria, hyponatraemia and hypokalaemia.
Myocardial ischaemia has previously been reported during IH and is an expected serious complication given the increased afterload owing to noradrenaline resulting in increased myocardial oxygen demand. Our data showed a higher incidence of ECG changes consistent with myocardial ischaemia in the IH group compared with the non-IH group (17% vs 2%). Troponin concentrations were available in only a small subgroup and hence are difficult to interpret, but a higher percentage of patients in the IH group had troponin levels above the normal range. This is in keeping with the study published by Gathier et al, which reported a 10% incidence of myocardial infarction in the group who received IH compared with zero in their control group. 9 Similarly, Roy et al reported ECG changes in 46% of patients and troponin elevation in 13% of patients who received IH when phenylephrine was the predominant vasopressor used. 12 This suggests an increased rate of myocardial ischaemia which in a prospective study could be further quantified with the use of echocardiography to look for regional wall motion abnormalities. With this suggested increased rate of myocardial ischaemia, we would expect an increased risk of arrhythmia and acute pulmonary oedema. While this study did not find the incidence of these complications to be significantly greater than in the non-IH group, the study was too small to detect a clinically significant result.
In this patient cohort, IH was associated with an increase in urine output, fluid administration, IV potassium replacement, episodes of hyponatraemia and hypertonic saline use. To our knowledge no other studies have previously explored the relationship between IH and fluid balance. As this study is retrospective in nature, the reasons for the increased fluid administration are uncertain. However, it is possible that IH causes a pressure naturesis. This can occur as the increased blood pressure produces an increase in renal perfusion, causing an increase in renal interstitial hydrostatic pressure. This affects tubular reabsorption of sodium in the proximal tubule and results in an increase in urine output and urinary sodium loss. 13 Both the resultant hypovolaemia and hyponatraemia would be potentially deleterious to aSAH patients. In this patient cohort, euvolaemia was maintained and negative respiratory effects of fluid overload such as pulmonary oedema were not observed. Nevertheless, further investigation of the relationship between IH and excessive diuresis with resultant difficulties in fluid and electrolyte management are warranted as these may influence outcomes.
We observed no increase in rebleed rates with IH following aSAH; however, this is in a population who largely underwent early securement of their aneurysm. This finding is consistent with a previous study in which patients underwent IH for vasospasm; however, the sample size was only 12 patients. 14 Patients who underwent coiling of their aneurysm achieved securement faster than those patients who required clipping.
Induced hypertension was used in most patients who developed DCI in this centre. There was also a high rate of interventional radiological procedures both to diagnose and treat vasospasm. Improvement in neurological function was documented in 48% of patients following the commencement of IH. This is lower than rates previously documented, which have ranged from 50% to 100%. 9
As this is not a randomised controlled trial the clinically important outcomes (survival, discharge destination) are provided for interest only and cannot be related in any meaningful way to the use or otherwise of IH. Nevertheless, the high rate of discharge to a rehabilitation facility rather than home suggests poor functional outcomes are still associated with the onset of DCI in these patients and behoves us to further investigate the benefits as well as limitations of this treatment. Vasospasm alone has previously been reported to be associated with a 50% risk of a poor outcome as defined by a modified Rankin Score of greater than 3. 9
Strengths of this study include the large and complete dataset that has been collected over a two-year period. The group of patients with IH is small, but this is an uncommon group of patients, and the previous largest patient group in which the incidence of complications of IH was collected was 21 patients in the Gathier study. 9 Weaknesses include the retrospective and observational nature of this study limiting interpretation of the results which should be considered hypothesis-generating. Furthermore, as it is a single-centre study generalisability to other centres could be questioned. In this study all patients who required IH received noradrenaline via a central venous catheter. We did not collect specific data in regard to line-associated complications in this study; however, previous evidence suggests that mechanical complications occur in 2.1% of patients, a 1% risk of blood stream infections and a 1% risk of catheter-associated deep venous thrombosis. 15 This should be considered when discussing complications of IH therapy as this may be the only indication for central access in this patient group.
These findings contribute to the literature by quantifying the incidence of common complications of IH therapy for aSAH in a contemporary cohort. In the absence of additional data from larger datasets or randomised controlled trials these data can be used to help weigh risks and benefits of using IH for aSAH in individual patients. A temporal improvement in neurological function was noted following the initiation of IH in 48% of patients, which supports continued investigation into this treatment modality. However, it remains uncertain how to determine optimal blood pressure goals, how to optimise benefit versus risk, and the medium- and long-term effects of this treatment. The poor functional outcome in this patient group (72% discharged to a rehabilitation facility) emphasises the need for further investigation and improvement in treatment modalities. If reproduced in a larger population then there may be sufficient evidence of risk that equipoise is returned, and a randomised controlled trial may be justified to address mortality and functional outcomes of IH.
Conclusion
In this retrospective single-centre study of IH for the treatment of DCI following aSAH, IH was associated with an increased rate of ischaemic ECG changes along with the expected physiological response of increased urine output and hyponatraemia. However, there was no increased rate of rebleeding. Of patients managed with IH, 48% had some associated improvement in neurological function. Further pre-clinical and prospective clinical trials investigating IH for DCI and the ideal method to titrate this therapy are warranted.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.