
Abstract

It is not the resistance of the material which will be the limit of the aerobatic performance of the artificial bird, but rather the physiological resistance of the man who is its brain.
Louis Blériot, October 1922.
1
In the two decades that followed the first sustained, controlled flights of the Wright Flyer at Kitty Hawk on 17 December 1903, the design of powered, heavier-than-air aircraft advanced rapidly. The development of increasingly powerful engines allowed pilots to fly higher and faster, and begin to perform aerobatic manoeuvres. However, rolls, steep turns, and pullouts from dives exposed aviators to accelerative forces equivalent to many times the force of gravity. Reported effects included the sensation of ‘being forced into the seat’, heaviness of the legs, and occasionally, on pushing ‘the rotatory stimuli up to unusual limits’, narrowing of the visual field, and ‘darkening of the sky’. 2
Introduced in 1916, the Sopwith Triplane saw brief service with fighter squadrons of the Royal Navy Air Service over the Western Front, where it was praised for its phenomenal rate of climb and exceptional manoeuvrability during aerial dogfights.3,4 Quickly superseded by more powerful biplane fighters, surviving aircraft were repatriated to England, where for the remainder of the war they were utilised by the Royal Flying Corps for experimental purposes. In addition to supplying important technical information on airframe design, some of these test flights provided valuable insights to the Air Medical Investigation Committee (AMIC), which had been tasked with examining the medical problems of flying.
In a report published in May 1919, Henry Head, Chairman of the AMIC outlined the experience of ‘Major VB, a highly expert pilot’, who commenced a series of banked turns in a Sopwith Triplane equipped with an accelerometer: On starting the second turn the sky appeared to go grey. A mist gradually arose like going under an anaesthetic, and he fainted … When he came to himself, he was flying over a village about a mile away from the place of the experiment. The unconsciousness must have lasted about 20 seconds. During the first turn g reached 4.5, during the second, 4.6.
Although Head described this phenomenon as ‘fainting in the air’, and postulated that it was ‘not improbably responsible’ for some unexplained accidents, the AMIC made no further effort to investigate the cause, or identify methods of protecting against acceleration-induced visual disturbance, or loss of consciousness. 2
Meanwhile, in Paris, on 22 July 1919, André Broca and Paul Garsaux presented a ‘preliminary note on the study of the effects of centrifugal force on the organism’ at a meeting of the National Academy of Medicine. This research, which subjected dogs to very high g-forces in a 60-cm diameter centrifuge, was precipitated by a fatal crash in which the pilot was presumed to have suffered a ‘physiological accident’ due to radial acceleration. Post-mortem examination of one animal revealed that the abdominal vessels were engorged with ‘almost all the blood of the body’, leading Broca and Garsaux to hypothesise that aviators might benefit from wearing an abdominal belt. 5
Despite this suggestion, it would be more than a decade before elastic and pneumatic belts designed to prevent the pooling of blood in the splanchnic circulation were developed for use in the Coupe d’Aviation Maritime Jacques Schneider.6,7 In the intervening years, pilots participating in air races had learned to contract their abdominal muscles as ‘an instinctive gesture of defence’ during tight turns around course pylons.
8
Nevertheless, as their aircraft became faster and more manoeuvrable, they increasingly experienced ‘dimming of vision’, ‘seeing black’, and transient loss of consciousness.8–11 Testing a Supermarine S.5 seaplane in the run up to the 1929 Schneider Trophy, Flying Officer (later Air Marshal) Richard Atcherley went ‘out’ halfway round a turn. He later recalled: In my lapse of unconsciousness, I dreamt that I was sitting in the housemaster’s garden at Oundle in a deck chair … I could see the flowers – and hear the bees – the noise of which got angrier and angrier, until I started to wonder where I had heard that noise before. Then I realised that it was the Napier engine in the S.5, and gradually came to the frightening realisation that I was going like a bomb and might expect to hit the water at any second … I was a very frightened officer!
11
During the early 1930s in Germany, Heinz von Diringshofen was among the first to extensively examine the physiological effects of acceleration on the human cardiovascular system. Initial studies were conducted in the air using an Albatros L 78 biplane, and later, in a 5.4-m diameter human centrifuge constructed at the Aeromedical Research Institute in Berlin. 12 As a result, he deduced that the forces of radial acceleration acting on the upright seated pilot increased the hydrostatic distance between the heart and the head. Consequently, exposure to high g-forces reduced the pressure in the arteries at the level of the brain, leading to disturbances in vison and consciousness. Decreasing the heart–brain hydrostatic distance by crouching forward was found to increase g-tolerance significantly, as did reclining the pilot’s seat backwards, or positioning them prone. Published in 1939, von Diringshofen’s Medical Guide for Flying Personnel of the Luftwaffe contained a detailed chapter on the effects of acceleration and centrifugal force. In June 1940 the book was translated into English by Velyien Henderson, Professor of Pharmacology at the University of Toronto, and distributed to allied airmen. 13
By the outset of World War II, acceleration research programmes had been established in several other countries. Using aircraft and human centrifuges, scientists replicated much of the work carried out in Germany, 14 before moving on to investigate various ways of raising arterial blood pressure at the level of the heart, which facilitated the maintenance of cerebral perfusion in the face of high g. Methods assessed included voluntary self-protective straining manoeuvres, 15 the administration of medications with pressor effects, and the use of hydrostatic and pneumatic anti-g suits to compress dependent parts of the body during positive acceleration. 16
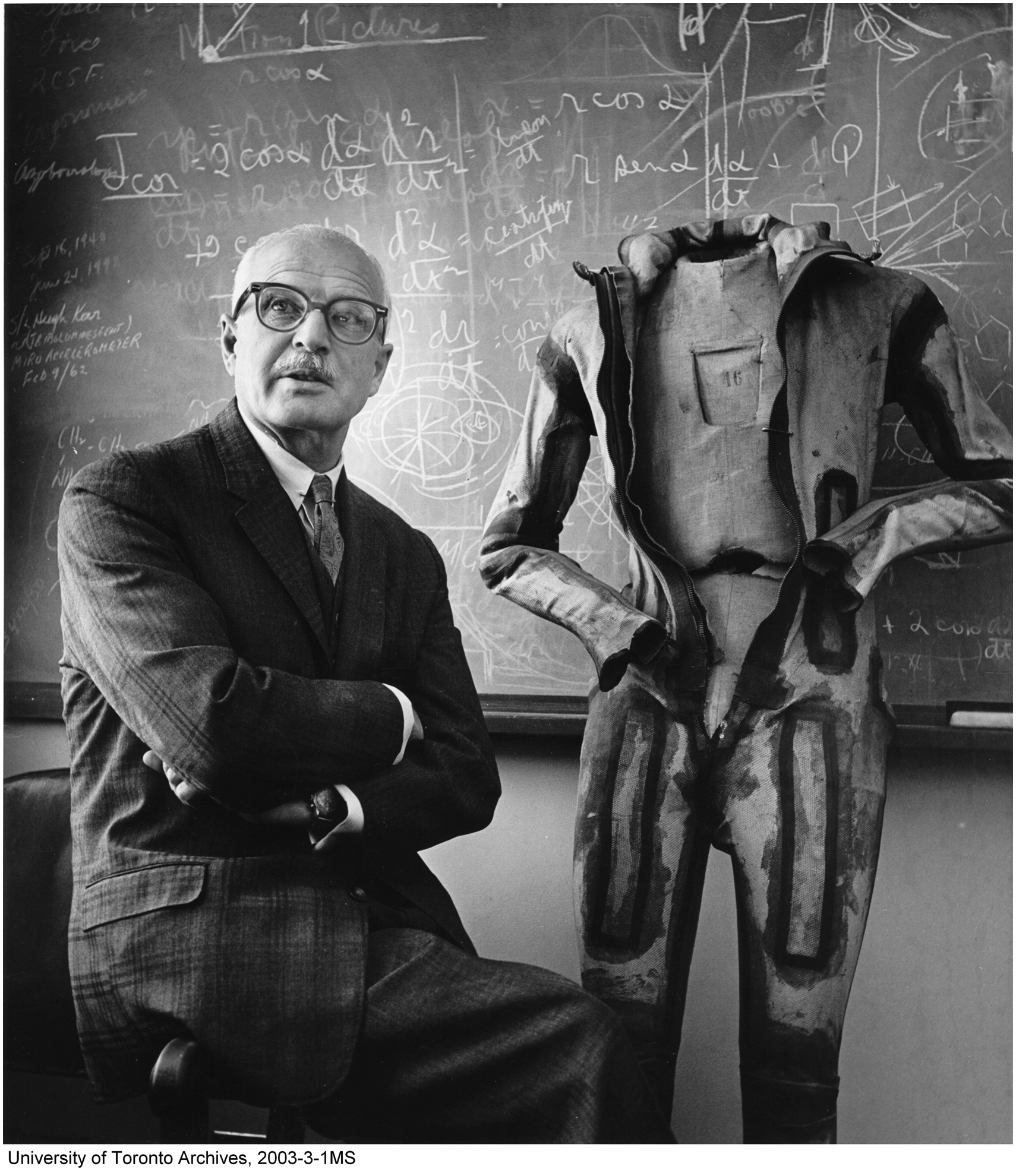
The idea of dressing the pilot in a double-walled fluid-filled anti-g suit in which the outer wall was rigid and the inner distensible had, in fact, been investigated by German researchers in the mid-1930s, but dismissed on the grounds that the ‘weight of the suit … as well as the hindrance to the movements of its wearer would interfere with its effectiveness’. 17 While the water-filled pressure gradient suit developed by Wilbur Franks and colleagues in Canada from 1939 onwards was the first to be trialled in combat, the automatically inflating pneumatic suits devised in Australia and America were quickly found to be superior.
Weighing ‘less than 3 pounds and … as comfortable to wear as conventional flying clothing’, the American G-3 suit was tested by pilots of the Eighth Air Force flying P-51 Mustang aircraft in Europe during the last year of the war. Its use not only reduced the reported incidence of ‘greyout and blackout’, but also increased the number of enemy planes shot down per 1000 sorties.16,18
At the close of hostilities, Frank Cotton, Research Professor of Physiology at the University of Sydney, and developer of the Cotton Aerodynamic Anti-G Suit wrote that the American G-3 garment represented ‘the best yet made as far as present-day aircraft are concerned … however … when much faster aircraft have replaced the present machines, more protection will be required than any present suit can give … and much more research will be required’. 19 By the early 1980s, Cotton’s words proved prescient; acceleration-induced loss of consciousness had become a major threat to crews flying high performance fighter jets, and interest in this field of research was renewed. 20