
Abstract

The Australian and New Zealand College of Anaesthetists (ANZCA) curriculum states a minimum volume of practice (VOP) required to complete each subspecialty unit. We performed a prospective study of seven trainees who undertook their cardiothoracic anaesthesia subspecialty rotation at The Prince Charles Hospital, Queensland. The results were presented at the 2023 ANZCA Annual Scientific Meeting and are summarised in Table 1.
Fellow and Trainee experience by cases.
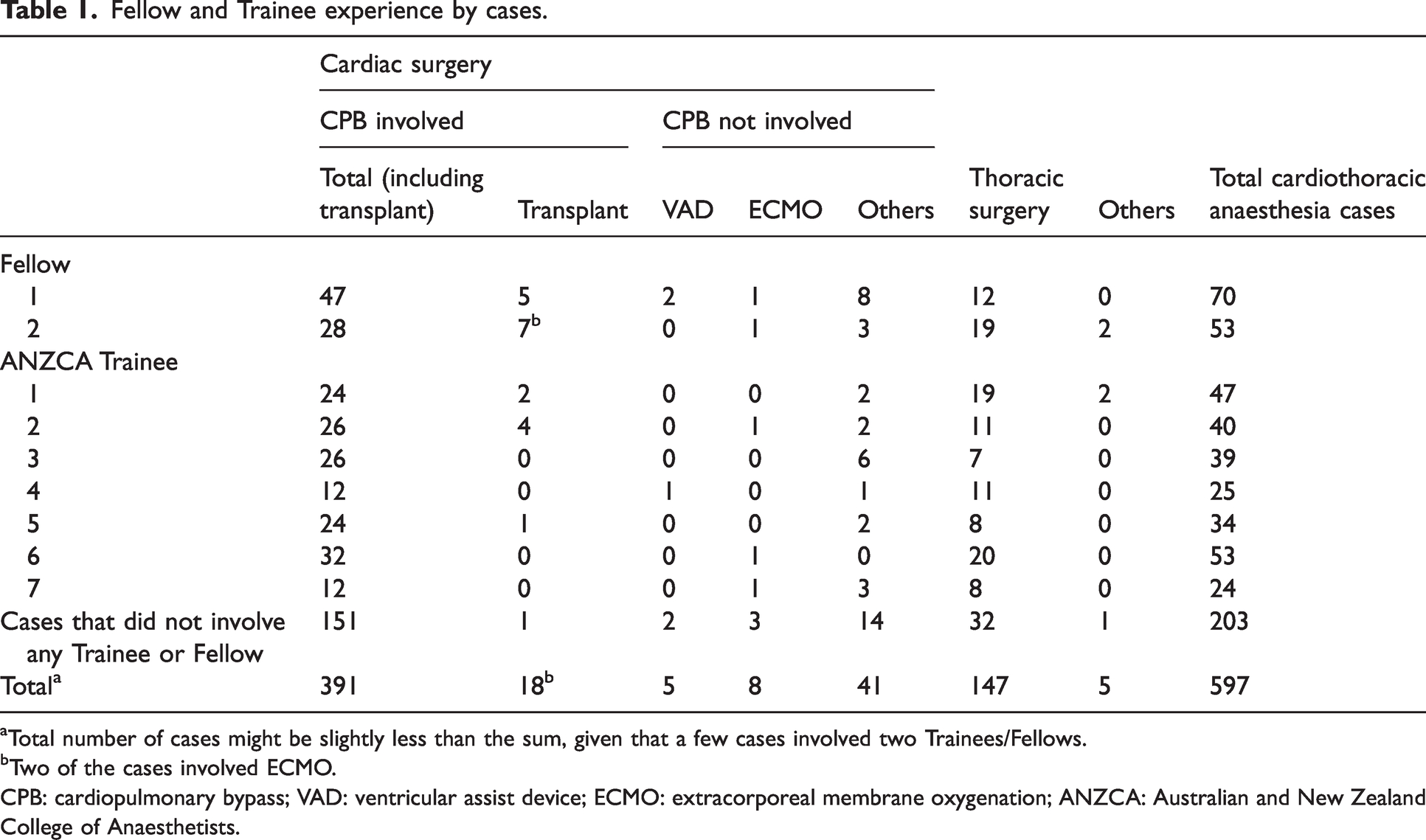
Total number of cases might be slightly less than the sum, given that a few cases involved two Trainees/Fellows.
Two of the cases involved ECMO.
CPB: cardiopulmonary bypass; VAD: ventricular assist device; ECMO: extracorporeal membrane oxygenation; ANZCA: Australian and New Zealand College of Anaesthetists.
By crosschecking with the operating theatre lists, our study showed that nearly 40% of the cardiothoracic anaesthesia cases did not involve a Trainee or Fellow. It could be hoped that with meticulous planning and rostering more of these cases could be assigned to ANZCA trainees, thus maximising their clinical exposure during the limited time spent in this subspecialty rotation.
Our results also demonstrate the potential to allow additional ANZCA Advanced Trainees (ATs) to complete a cardiothoracic anaesthesia rotation at our institution simultaneously. For example, 151 cases for additional trainees over a six-month period would be able to accommodate about 10 more ATs. The thoracic cases available would be the limiting factor—this can potentially be addressed by cooperation with private hospitals to increase case availability, and by simulation.
Given that approximately half of the thoracic surgeries are performed in the private sector, it could be possible to arrange for ATs to undertake a portion of their training in private hospitals to gain more experience in thoracic anaesthesia. Second, in-house simulation training would be of great value and offer a realistic experience in the techniques of lung isolation (insertion of double-lumen endotracheal tubes or bronchial blockers) essential for thoracic surgery. Moderated by experienced thoracic anaesthetists, multiple case scenarios can be practised, simulating typical emergencies in thoracic anaesthesia. This provides a safe environment for trainees to think about and troubleshoot potential intra- and postoperative crises and learn with the highest efficiency.1 –3
Further research is needed to explore proficiency in trainees after the set VOP is achieved, and to query the need to modify the VOP requirement. In the USA, Markin et al from the University of Nebraska Medical Centre reported an average exposure of 40 to 50 cardiac anaesthesia cases per trainee during the two-month cardiac anaesthesia rotation during anaesthesiology residency. 4 A cumulative 60 critical care echocardiography scans needed to be performed to arrive at a state of consistent performance where the learner can be judged as possessing the technical skills, knowledge and clinical judgement essential for competency.5 –7 As for gastrointestinal endoscopic procedures, which demand a high level of manual dexterity, precision and visuospatial skills, an average of 200 gastroscopies and 150 colonoscopies was required to obtain competency.8,9 These statistics prompted the authors to raise the question, ‘Does the VOP for cardiac anaesthesia need to be increased?’.
Paediatric residents who spent longer periods in the neonatal intensive care unit report relatively higher self-perceived competency in performing neonatal resuscitation and procedures. 10 We believe that trainees getting higher caseload, above the recommended VOP requirements, is beneficial. Cardiothoracic anaesthesia involves a deep understanding of applied cardiopulmonary physiology and of the pharmacology of various inotropes, vasopressors and vasodilators. Owing to the nature of the surgeries and patient population, cardiac surgery often calls for advanced critical care skills such as timely management of intraoperative arrhythmia, including cardiac arrest, as well as massive transfusion and real-time interpretation of viscoelastic point-of-care coagulation results. Trainees receive invaluable exposure in the perioperative management of critically unwell heart failure patients and applied knowledge of cardiac pacing. Skillsets and clinical exposure to cardiothoracic anaesthesia can be extrapolated and prove useful when trainees start their independent clinical practice. This is especially important in the setting of Australian and New Zealand anaesthesia training, in which anaesthesia and intensive care training are separated—governed by two different Colleges, with only 13 weeks of intensive care experience required in the ANZCA curriculum for anaesthetists in training.
Our findings apply to our institution only, and discussions and suggestions are based on the opinions of the authors. However, it is likely that these opportunities identified in our centre would also be available in other cardiothoracic centres in Australia and New Zealand, allowing an increase in the caseload for trainees and/or in the number of trainees. Options for obtaining this exposure through private hospitals’ thoracic anaesthesia lists and designing innovative simulation workshops for cardiothoracic anaesthesia crisis management are worthy of further discussion. We propose that more exposure to cardiothoracic anaesthesia be encouraged by making full use of the remaining unrostered cases to improve critical care skills for soon-to-be independent practising anaesthetists.
Footnotes
Author Contribution(s)
Acknowledgement
We express our gratitude to Department of Anaesthesia at The Prince Charles Hospital and participating ANZCA trainees for supporting this project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.