
Abstract

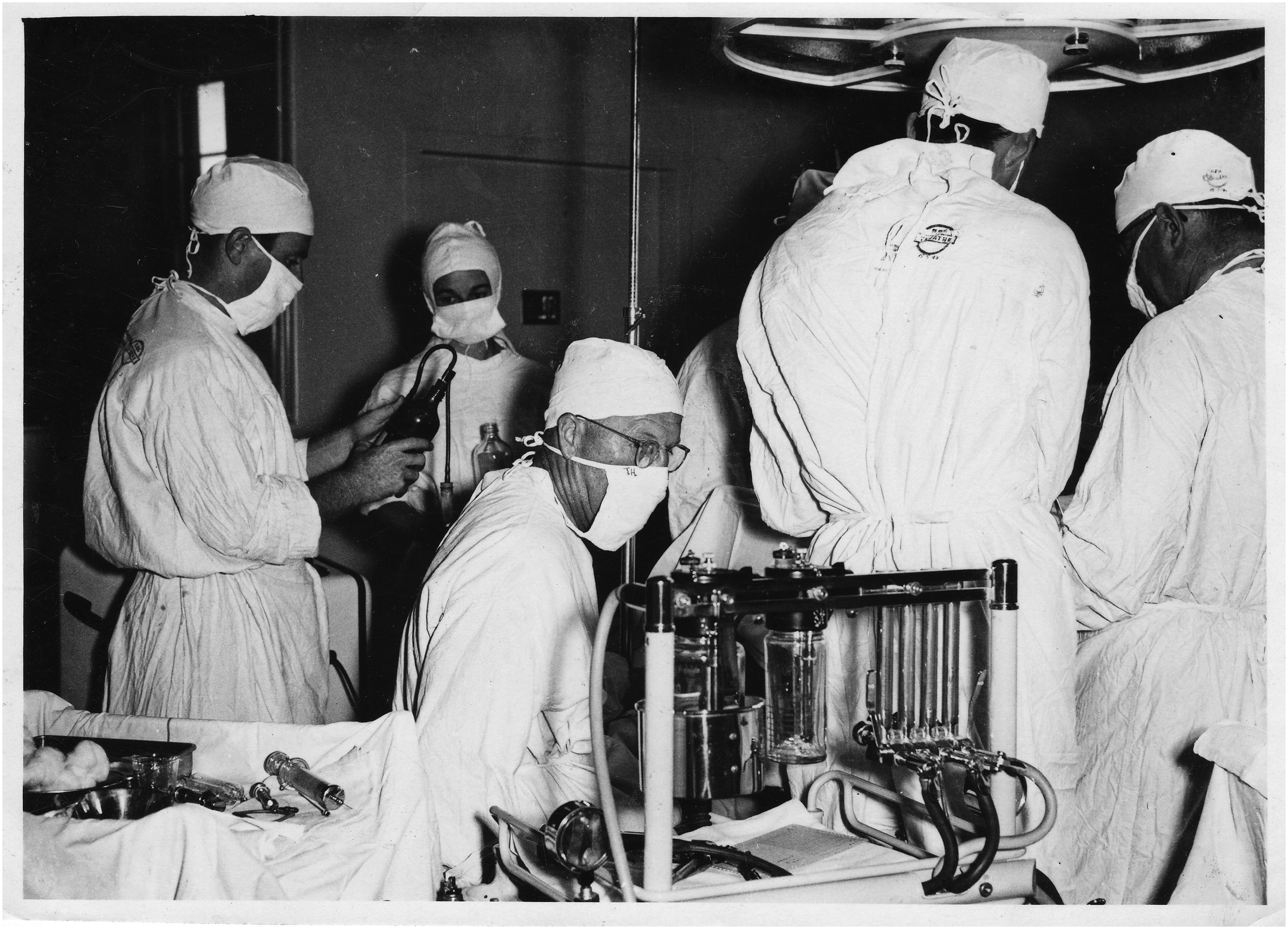
Dr Gilbert Troup, Operating Theatres, Royal Perth Hospital, c. 1953. He is seated at a Boyles machine which has two Boyles bottles—one in a water bath. There are four flowmeters, which were for oxygen, nitrous oxide, cyclopropane and carbon dioxide. Note the tray of glass syringes and needles for drug administration to his right. Image courtesy of Dr Toby Nichols FANZCA and Dr Fiona Nichols PhD (Dr Troup’s grandchildren).
Dr Gilbert Reynolds Troup (1896–1962) was initially a physician with special interest in cardiology but also had interest and expertise in anaesthesia, becoming a major contributor to the specialty in Western Australia (WA) and nationally. He was one of the founders of the Australian Society of Anaesthetists (ASA) 90 years ago in 1934 and, in 1950, a foundation Fellow of the Faculty of Anaesthetists, Royal Australasian College of Surgeons. He was the second President of the ASA. His life and many contributions to medicine have been well documented.1 –4
In 1929 or 1930, Troup worked with Ivan Magill in England and later, in 1935, with John Lundy, Ralph Waters and Arthur Guedel in the USA. He returned with drugs, equipment and techniques to improve anaesthesia in Australia, and worked on the development of portable anaesthetic equipment. Troup was the first to use cyclopropane in Australia. 4
Troup was very much an ambassador for Australian anaesthesia—presenting wherever he went. In the USA, he presented on ‘Anesthesia in Australia’ 5 and on his return home, he presented on ‘Anaesthesia in America’ in Australia. 6 All travel then was by ship, which meant many months away from Perth, one of Australia’s remotest state capitals. However, Troup managed to attend many major national meetings, especially in the early days of the ASA—all of this combined with a busy practice as an anaesthetist and physician. Troup served during WW2, ultimately being Lieutenant-Colonel of the 2/12 Australian General Hospital in Ceylon. Troup became Honorary Director of the anaesthetic department at Royal Perth Hospital in 1948. 7
Troup had a major involvement in thoracic anaesthesia and at this time was one of the pioneers of curare use in Australia. The initial use of curare in Australia had been at St Vincent’s Hospital in Sydney by Daly and Marshall in August 1945. 8 Harry Daly was a contemporary and fellow founder of the ASA. Troup used curare manufactured by both Squibb (Intocostrin) and Burroughs Wellcome and Co. (d-tubocurarine), very soon after Daly, and described its use in 65 cases for mainly upper abdominal and some thoracic surgery. Based on the brief self-experimentation literature at the time, Troup recognised that curare did not have any central effect and he mentioned that he had not had to call upon using the antidote ‘prostigmin’! He also called for urgent international standardisation of curare preparations. 9
Tuberculosis (TB) was a major problem in this era, with significant thoracic surgery occurring in all centres in Australia. Troup, with his friend and surgical colleague, Mr Fred Clark, undertook the first TB surgical visit to Papua and New Guinea (P&NG) in July 1956 under the auspices of the Commonwealth Health Department. 10 At this time Australia had civil administration of the Territory of Papua and the United Nations Trust Territory of New Guinea.
TB was a major health problem in P&NG at that time and remains so today. TB was more common in the coastal areas compared with the highlands and spread had supposedly increased after workers returned from the cane fields of Queensland early in the 1900s. The National TB Control Program was implemented in 1950.11,12
The thoracic surgery was performed in Port Moresby, at the Native Hospital at Ela Beach with some pre- and postoperative care occurring at Gemo Island in Fairfax Harbour—this was an early isolation centre for TB, leprosy and other diseases established in 1937 by the London Missionary Society.1,12,13
Initially the indigenous patients were reluctant to have this major TB surgery as earlier surgery on Gemo Island had had unfavourable results, but once anaesthetic and surgical outcomes were seen to be good, many were keen for operative treatment. 12 Several other thoracic teams were to follow from WA and later a team from St Vincent’s in Sydney also travelled to P&NG, led by Mr Harry Windsor and Dr Brian Dwyer. 14
Troup delivered the EH Embley Memorial Lecture in 1954, discussing many aspects of anaesthesia. This included education regarding modern more complex anaesthetic techniques, the dire need to establish anaesthetic departments throughout Australia, the transition from inhalational agents to intravenous barbiturates, simple adaption of a draw-over apparatus to avoid hypercarbia and the development of one-lung anaesthesia. 15
He continued working until shortly before his death in 1962.
Footnotes
Author Contribution(s)
Acknowledgements
Dr Toby Nichols, FANZCA, and Dr Fiona Nichols, PhD, grandchildren of Gilbert Troup; Sarah Toohey, Museum Curator, Royal Perth Bentley Group, WA; Medical Library, St George Hospital, Sydney, NSW.