
Abstract
Iron deficiency and iron deficiency anaemia are frequently under-recognised in chronic conditions with non-specific symptoms, including fatigue. This study aimed to assess the prevalence of iron deficiency with or without anaemia in chronic pain patients, and the association between iron deficiency status, fatigue and health-related quality of life. Eighty-two patients attending chronic pain outpatient appointments were recruited into this cross-sectional study. Iron studies and haemoglobin were determined from venous blood samples. Participants’ health-related quality of life was assessed with the 36-item short form survey and fatigue with the functional assessment of chronic illness therapy fatigue scale. Iron deficiency was prevalent in 58.8% of patients and 2.5% met the criteria for iron deficiency anaemia. There was no significant association between iron deficiency status and the functional assessment of chronic illness therapy fatigue scale score or 36-item short form survey domain scores. There was a high prevalence of iron deficiency in this group of chronic pain patients, while the prevalence of iron deficiency anaemia was low. There was no statistically significant association found between iron deficiency status and fatigue or quality of life measures.
Introduction
Iron deficiency anaemia (IDA) is a significant risk factor for morbidity and mortality and is recognised as a global health problem. 1 Anaemia, defined as low concentrations of haemoglobin, affects about 23.2% of the global population. 2 While there is substantial geographical variation in the prevalence of anaemia, iron deficiency (ID) remains the leading cause of anaemia worldwide. 2 Data on the prevalence of IDA in the general Australian population is limited; however, the World Health Organization estimates a 17% prevalence of anaemia in non-pregnant Australian women aged 15–49 years. 1 A study in Queensland, Australia, reported that 10.6% of adult women under 50 years had severe ID, 2.8% for women 50 years and above and almost zero for men. 3
Iron deficiency with or without anaemia is often under-diagnosed and under-treated in chronic conditions, including chronic heart failure, 4 inflammatory bowel disease 5 and chronic kidney disease. 6 Iron deficiency, before the development of anaemia, is associated with impaired immune function,7,8 decreased physical work capacity, 9 impaired cognitive function10 –12 and fatigue.13 –15
Chronic pain, defined by the International Association of the Study of Pain, is pain that persists for more than 3 months, 16 and has a prevalence of approximately 20% in developed countries.17 –19 Chronic pain is associated with significant morbidity including depression, 20 fatigue, 21 reduced health-related quality of life 22 and impaired cognitive functioning.23 –25 Creavin et al. reported that 64% of adults in the general population with chronic widespread pain experienced persistent fatigue. 26 It is therefore important to assess the potential contribution of ID to the high burden of fatigue in these patients.
Few studies have assessed the relationship between ID and chronic pain conditions. Ortancil et al. hypothesised that iron deficiency may play a role in the pathophysiology of fibromyalgia as the cerebrospinal fluid of fibromyalgia patients showed decreased concentrations of neurotransmitters synthesised from iron.27,28 However, studies have both supported27,29 and reported no evidence30 –32 of an association between fibromyalgia and ID. The link between IDA and migraine is more consistent, with four studies supporting an association.33 –36
Patient-reported outcome measures have increasingly gained importance in the evaluation of treatment in chronic pain clinics.37 –39 In this study we evaluated the prevalence of ID in the setting of chronic pain patients with the aim of assessing the relationship between ID and health-related quality of life measures.
Methods
This cross-sectional study was conducted at the Royal Brisbane and Women’s Hospital (RBWH), a tertiary level hospital in Queensland, Australia. This study was approved by the Royal Brisbane and Women’s Hospital Human Research Ethics Committee (HREC/2019/QRBW/58663).
Patients presenting to the Professor Tess Cramond Multidisciplinary Pain Centre were screened for eligibility by trained research personnel. Patients over 18 years of age experiencing chronic pain for more than 12 months were included. Patients with known or suspected blood disorders, pregnant patients, patients taking iron supplementation including intravenous iron, or patients who underwent surgery within the past 6 months were excluded from the study.
Patients were recruited from the outpatient clinic or telephoned prior to their visit to obtain informed written consent. Non-fasting venous blood samples were taken on the day of the appointment by trained staff to determine their full blood count, serum iron, serum ferritin and serum transferrin. Iron deficiency anaemia was defined as ferritin less than 100 μg/l and haemoglobin less than 130 g/l in men or less than 120 g/l in women. Iron deficiency was defined as moderate if ferritin was less than 100 μg/l or severe if ferritin was less than 30 μg/l as per Queensland Health definitions.
Patient demographics and clinical information were collected by way of a written questionnaire and collated using REDCap software (Research Electronic Data Capture Vanderbilt) administered by Metro North Hospital and Health Services. 40 Data included the type of chronic pain condition and duration, medical comorbidities, medications, diet and alcohol intake. Pain was rated out of 10 using a visual numerical scale. Health-related quality of life was assessed by the 36-item short form survey (SF-36) and fatigue levels were assessed by the functional assessment of chronic illness therapy fatigue scale (FACIT-Fatigue).
The FACIT-Fatigue scale is a 13-item survey designed to assess the impact of fatigue in chronic disease. This measure has been validated in the chronic disease population and patients with IDA.41 –43 Scores range from 0 to 52, with a higher score indicating less burden from fatigue. The SF-36 is a generic, self-administered questionnaire, which has been validated and used to assess treatment in chronic pain and other diverse populations.37 –39,44,45 The SF-36 provides domain scores rather than an overall score. The eight domains are physical functioning, role limitations due to physical health, role limitations due to emotional problems, fatigue, emotional wellbeing, social functioning, pain and general health. The scores range from 0 to 100, with the maximum score reflecting the highest quality of life. The scores are scaled to represent the average for all eight domains.
Statistical analyses were performed in STATA 15 (StataCorp, 2017. Stata Statistical Software: release 15, College Station, TX, USA: StataCorp LLC). Data were presented as mean and standard deviation (SD) for continuous normally distributed variables, median and interquartile range (IQR) for continuous non-normally distributed variables and frequency and percentage for categorical variables. Associations between categorical variables were assessed using chi-square tests and Fisher’s exact tests were used for small cell counts. To compare continuous normally distributed variables between two groups, the Student’s t-test was used, while a one-way analysis of variance was used to compare three groups. A Mann–Whitney U test (for comparison of two groups) or a Kruskal–Wallis test (for comparing three groups) was implemented if the continuous variable was not normally distributed. Associations between two continuous variables were explored using Pearson’s correlations. When the assumptions of the test did not hold, Spearman’s correlation was used. Statistical significance was defined as a P value less than 0.05 (two-sided).
Results
Eighty-two patients were recruited into this study between June and December 2020. Of these, two did not have ferritin measures available for the classification of ID, and three did not have both ferritin and haemoglobin measures available for the classification of IDA. The prevalence of ID was 58.8% (47/80), of which 37 (46.3%) were moderate in severity and 10 (12.5%) were severe. The prevalence of those with IDA was 2.5% (2/79).
There was no statistically significant association found between ID and age, gender, body mass index, medical comorbidities or medications. Iron deficiency was associated with decreased alcohol intake and eating meat and poultry consumed more than three times a week (Table 1). However, the small sample size and large number of simultaneous comparisons limits the interpretation of these results. No statistical association was found with other dietary factors including the patient’s subjective global assessment of their nutritional status.
Patient characteristics and iron status.
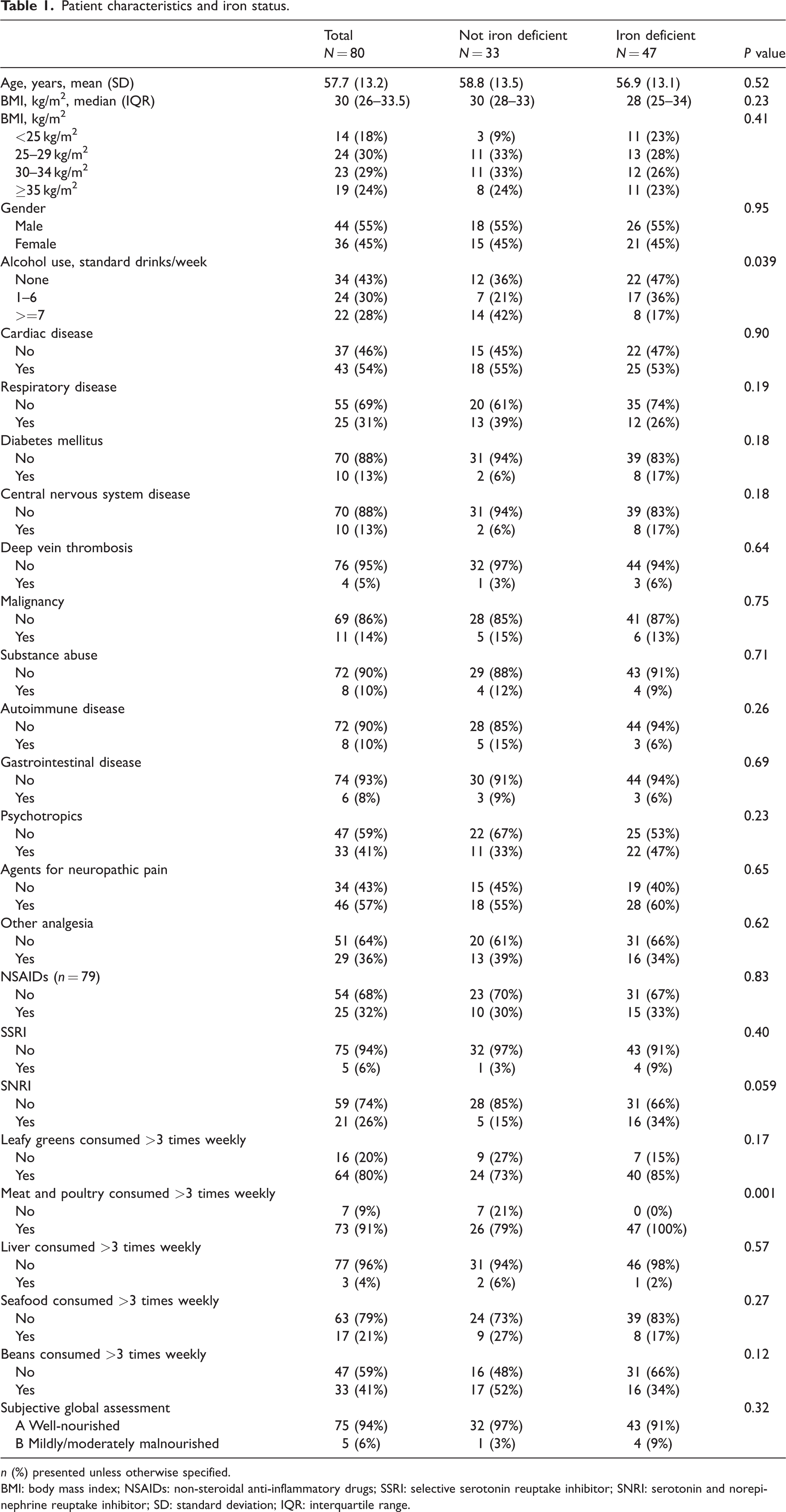
n (%) presented unless otherwise specified.
BMI: body mass index; NSAIDs: non-steroidal anti-inflammatory drugs; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin and norepinephrine reuptake inhibitor; SD: standard deviation; IQR: interquartile range.
The associations between iron deficiency status, patient characteristics and the outcomes of FACIT-Fatigue were explored (Table 2). The presence of central nervous system disease, deep vein thrombosis and psychotropics were associated with lower FACIT-Fatigue scores, demonstrating a higher burden of fatigue. The mean difference in FACIT-Fatigue between ID and non-ID patients was –1.59 (95% confidence interval (CI) –6.46 to 3.28).
Association between iron deficiency and patient characteristics with FACIT-Fatigue.
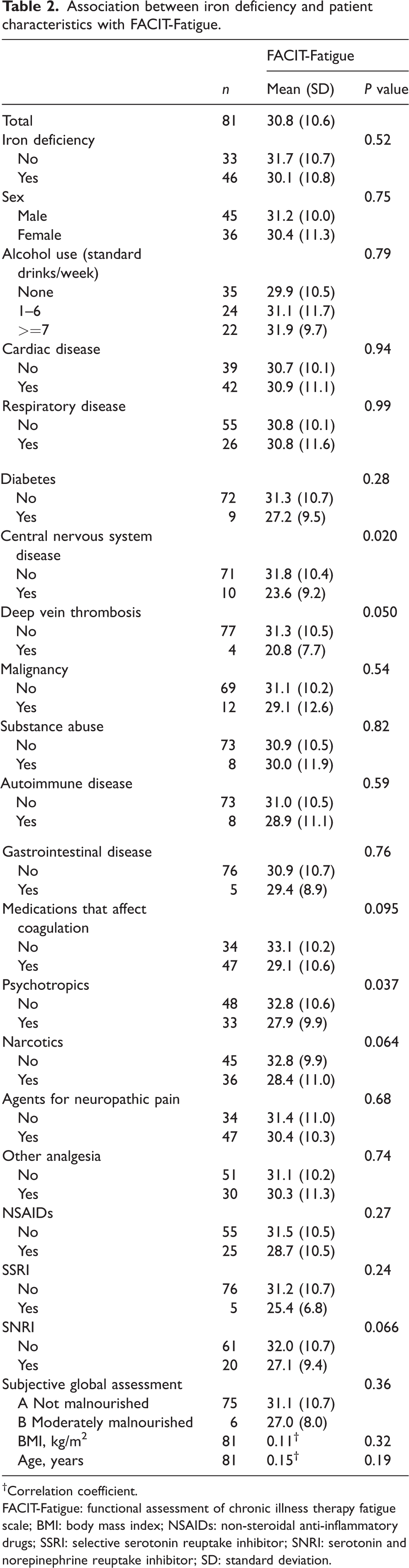
Correlation coefficient.
FACIT-Fatigue: functional assessment of chronic illness therapy fatigue scale; BMI: body mass index; NSAIDs: non-steroidal anti-inflammatory drugs; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin and norepinephrine reuptake inhibitor; SD: standard deviation.
There was no statistically significant difference between the SF-36 domain scores of iron and non-iron deficient patients (Table 3). Multiple patient characteristics were associated with SF-36 domains (see Supplementary Table 1 available online). Agents for neuropathic pain were associated with decreased energy and emotional wellbeing. Psychotropics were associated with role limitations due to emotional problems, poorer emotional wellbeing and social functioning. Serotonin-norepinephrine reuptake inhibitor (SNRI) usage was associated with role limitations due to physical and emotional problems, poorer emotional wellbeing and decreased general health. Medications that affect coagulation were linked to poorer physical functioning and energy. Various domains were significantly associated with substance abuse, central nervous system comorbidity, deep vein thrombosis comorbidity, medications that possibly affect coagulation, selective serotonin reuptake inhibitors (SSRIs) and subjective global assessment, although most had small group sizes and should be interpreted with caution.
Association between iron deficiency and SF-36 domains.
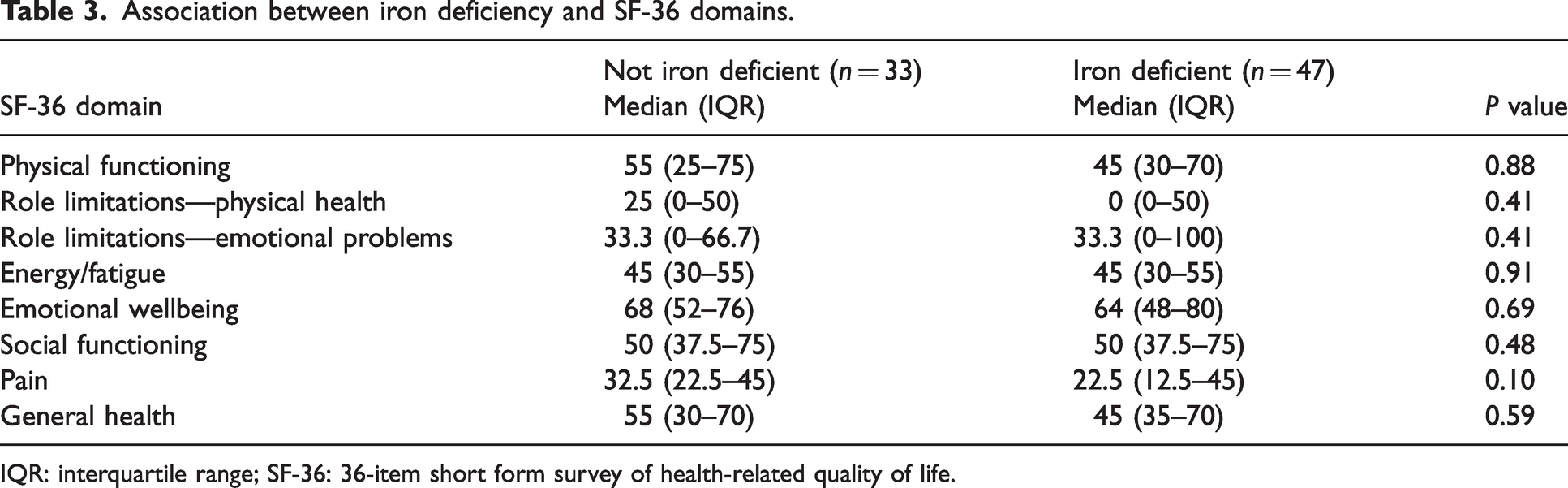
IQR: interquartile range; SF-36: 36-item short form survey of health-related quality of life.
Overall, this patient group had the poorest quality of life in the domain of role limitations due to physical health (median 0, IQR 0–50), followed by pain (median 22.5, IQR 22.5–45). There was no statistically significant difference in domain scores between male and female patients. There was a weak relationship between increasing age and decreasing physical functioning (r −0.22, P = 0.044), and a weakly positive relationship between increasing age and energy (r 0.26, P = 0.018).
Discussion
There was a substantial proportion of patients with ID (58.8%) in this sample of chronic pain patients. There was no significant difference found in the FACIT-Fatigue score between iron deficient and non-iron deficient groups. Overall, there was a high burden of fatigue (mean FACIT-Fatigue 30.8) in this group. We were unable to compare fatigue scores between iron deficient patients without anaemia and those with IDA due to the low percentage of anaemic patients. Health-related quality of life as measured by SF-36 domain scores was not significantly diminished in iron deficient patients. There was no significant relationship between SF-36 pain scores and ID, although the median score was lower in the ID group.
The study by Ahmed et al. of iron status in Australian adults reported an ID prevalence of 20.3% of pre-menopausal women, 5% of women 50 years or older, and 1.5% of men. 3 It should be noted that there is significant variation in the diagnostic criteria of ID, with Ahmed et al. employing a definition of serum ferritin less than 20 μg/l. The prevalence of IDA (2.5%) in our study was low and is likely to be related to the smaller proportion of pre-menopausal women in this sample.
There have been limited studies examining the relationship between pain and ID in selected chronic pain conditions including fibromyalgia and migraine. Ortancil et al. hypothesised that ID may play a role in the pathophysiology of fibromyalgia as iron is essential for the formation of neurotransmitters such as dopamine, which have been found to be of a lower concentration in the cerebrospinal fluid of patients with fibromyalgia. 27 The aetiology of chronic pain is diverse in the patients presenting to chronic pain clinics. Our sample included only two patients with fibromyalgia and two with migraine. Further research into the role of ID in the pathophysiology of these conditions may lead to targeted treatment options in the future.
SF-36 scores in domains related to emotional wellbeing were lower in patients using SNRIs, psychotropic drugs and medications to manage neuropathic pain. Identification of patients in these groups may allow for focused treatment in chronic pain clinics.
The main limitations of this study were the small sample size and lack of a healthy population control group. The cohort was heterogeneous in terms of the aetiology of their chronic pain. Due to the small sample size, multivariable modelling was not performed to investigate further the independent effect of iron deficiency on SF-36 and FACIT-Fatigue. At the univariable level, some variables had small group sizes and should be interpreted with caution. While multiple factors were associated with SF-36 domains, many groups had small sizes requiring caution in their interpretation. As this was a cross-sectional study, we did not measure the effect of iron replacement therapy. Serum ferritin is frequently used as a single measure of iron status but is only an estimation of iron status, given it may be raised in conditions such as inflammation, malignancy and increased alcohol intake. FACIT-Fatigue and SF-36 scores were not compared with norms for the Australian general population.
Conclusion
Only 2.5% of the study population had IDA, but there was a high prevalence of iron deficiency without anaemia in patients presenting to this chronic pain clinic. There was no statistically significant difference in FACIT-Fatigue or SF-36 scores between the iron deficient and non-iron deficient groups. However, there was a high burden of fatigue overall in our study population. The data collected from this study may help inform the evaluation of treatment at chronic pain clinics using patient-reported health-related outcome measures and iron supplementation in the future.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X241263612 - Supplemental material for A cross-sectional study of the relationship between iron deficiency anaemia and chronic pain
Supplemental material, sj-pdf-1-aic-10.1177_0310057X241263612 for A cross-sectional study of the relationship between iron deficiency anaemia and chronic pain by Kerstin H Wyssusek, Christine AWoods, Emily T Minard, Julie Lee, Anita Pelecanos and Paul Gray in Anaesthesia and Intensive Care
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.