
Abstract
Changing medical workforce demographics emphasise the need to understand and effectively manage pregnancy in the workplace. An Australian survey exploring pregnancy experiences of specialists and trainees working in anaesthesia received 242 responses describing 549 pregnancies. One hundred and sixty-two (67%) of these respondents were aged 31–40 years, 185 (76%) were specialists and 159 (66%) reported one or two pregnancies. Reported pregnancy complication rates were similar to national averages. Potentially harmful exposures included working >40 h per week (n = 298, 55%), ionising radiation and unscavenged gases. Other than ergonomic hazards and stress, exposures were not associated with an increase in self-reported complications. Moving heavy patients on a daily to weekly basis (n = 278, 53%) was associated with an increased risk for any maternal complication; odds ratio (OR) 2.13, 95% confidence interval (CI) 1.37 to 3.33, P < 0.001. High or debilitating stress levels were associated with any maternal complication, OR 2.93, 95% CI 2.06 to 4.17, P < 0.001, and any adverse neonatal/fetal outcome, OR 1.72, 95% CI 1.10 to 2.69, P = 0.018. The most common stress contributors were ‘work-related’, ‘exams’ and ‘pregnancy anxiety’. Ninety-one (38%) respondents reported experiencing stigma or negative attitudes toward their pregnancy from anaesthetic colleagues. Overall, 171 (71%) of respondents were satisfied with their experience of working in anaesthesia whilst pregnant. Thematic analysis of free text comments identified three major themes: workplace culture, maternal and fetal wellbeing, and career impacts on both pregnancy and family planning. Development of multilevel mechanisms to guide and support pregnant trainees and specialists in anaesthesia is recommended to address these findings.
Keywords
Introduction
In the last few decades, females consistently outnumbered males in Australian medical school enrolments; 1 however, the translation to gender parity in specialist training and subsequent practice has lagged in most specialties.1,2 Within anaesthesia, there is increasing gender balance in the trainee cohort, with 42% of anaesthesia trainees in Australia identifying as female in 2019, and near gender parity in younger Fellows of the Australian and New Zealand College of Anaesthetists (ANZCA). 3 Representation within leadership roles is lower, with a mere 24% of anaesthesia heads of department and 29% of ANZCA committee chairs identifying as women. 3 The causes of this low representation are likely multifactorial, and it is postulated that pregnancy and parenting are significant contributors.4,5 With increasing proportions of women working as anaesthesia trainees and new Fellows, it is likely that there will be rising numbers of women working in anaesthesia whilst pregnant or with young families. 6 Workplace conditions have evolved in the context of a male dominated medical workforce. 7 These historical models require continuing modification with specific consideration for the modern medical workforce, with one important consideration being the safe and effective management of pregnancy in the workplace.
Research exploring the association between occupational exposures and pregnancy outcomes relevant to women in anaesthesia have been largely retrospective, observational studies. Articles published since the 1970s have examined medical, anaesthesia, and operating room specific exposures such as ionising radiation, unscavenged gases and chemical and biological agents. Status as a medical doctor alone has been found to be independently associated with increased risk of pregnancy complications in some studies, 8 thought to be mediated by catecholamines and postural effects impacting uterine perfusion. 9 Early studies arising in the United Kingdom evaluating women in anaesthetic practice raised concerns for potential harm to the fetus.9,10 However, applicability has changed over the years, with alterations in anaesthesia practice, including the widespread reduction of nitrous oxide and halothane use in the developed world, and safety standards such as the use of lead aprons during ionising radiation exposure and scavenging systems in operating rooms where volatile anaesthetics are commonly used. Reassuringly there is no evidence for harm from volatile anaesthetics where environmental levels can be maintained below their legal threshold. 11
Occupational hazards relevant to pregnant workers in general include ergonomic hazards, work patterns and psychological stressors. 12 Ergonomic hazards (also known as physical risks) include moving, pushing and pulling heavy objects, and prolonged sitting or standing, and have been associated with increased pregnancy complications.13 –16 Work patterns including long working hours (usually defined as >40 h per week) and working night shifts late in pregnancy have been shown to have detrimental effects. Previous studies have demonstrated increased risk for threatened preterm labour (TPL), preterm birth, and small-for-gestational-age (SGA) or low birth weight (LBW) babies with the listed exposures, albeit with heterogeneous results.10,14,15 A systematic review of pregnant workers in general, including 49 individual studies and 21 cohort studies, identified that long working hours or high physical workload may be associated with an increased risk of preterm birth and SGA. Findings were mostly consistent; however, the pooled results ruled out a more than moderate effect size with an estimated relative risk <1.4, which limited the evidence for any mandatory action to address these risks. 14 The ‘fetal origins of adult disease’ studies link adverse fetal/neonatal outcomes such as preterm birth and SGA/LBW to a range of adult chronic health conditions, including cardiovascular disease, diabetes and stroke.17,18 Psychological risks including exposure to bullying, harassment, discrimination and stigma have been shown to cause harm, often leading to high levels of psychological distress. 19 Stress during pregnancy, even as a single stressful life event, has been shown to have a significant impact on maternal health as well as fetal growth and wellbeing, neonatal health and subsequent neurodevelopmental sequelae.20,21
Literature exploring the pregnancy and parenting experiences of female doctors has reported that career selection may influence subsequent family choices such as the timing and number of children.6,22,23 A recent study of female American anaesthesiologists found 51% reported being discouraged from becoming pregnant or having children, and some female doctors would not recommend a career in their chosen medical specialty due to their experiences of pregnancy and return-to-work.22,24 The self-reported experiences of pregnant female anaesthetists working in Australia have not been previously evaluated, nor has the association between occupational risks and pregnancy outcomes.
Methods
Female Australian specialist anaesthetists and anaesthetic trainees were surveyed on their experiences in the past 10 years of working whilst pregnant. Specific questions on self-reported work patterns, occupational health exposures, work modifications and perceived stress levels during pregnancy were asked. Respondents self-reported maternal and neonatal/fetal health outcomes. Associative analysis examined whether any relationship between occupational exposures (or stress levels) and maternal or neonatal/fetal outcomes could be identified, in addition to whether pregnancy experiences were related to family planning, or the number of pregnancies reported.
Following Human Research Ethics Committee approval (LNR/2020/QRBW/60272) an electronic survey was sent to a sample of 1000 Australian trainees and Fellows registered with ANZCA, who self-identified as female and were aged 45 years or less. The sampling approach utilised the national body responsible for the training and education of anaesthetists in Australia and New Zealand—ANZCA. This enabled access to a broad population of trainees and specialists practising anaesthesia in Australia, therefore reducing selection bias. The survey was distributed by ANZCA in April 2021 and responses were invited from those who had experienced pregnancy and/or a return-to-work from parental leave, whilst working in anaesthesia within the previous 10 years. Participants were provided with a link to an anonymous online survey, which the authors created using SurveyMonkey. 25 Completion of the survey implied consent to participate and a single reminder email was sent to the selected group after four weeks. Information was collected about experiences of working while pregnant and returning to work after parental leave. The results of the return-to-work survey are presented separately. 26
Respondent demographic characteristics were sought, including age and level of seniority at the time of survey completion, number of children, number of pregnancies and number of return-to-work episodes, experienced in the past 10 years. For each pregnancy, respondents reported: hours worked per week, changes to usual working patterns, gestational age parental leave commenced, exposures to occupational and ergonomic hazards, whether any work modifications occurred, and satisfaction associated with this and sources of support utilised. Respondents self-reported stress levels and the contributing factors, and maternal and neonatal/fetal health outcomes for each pregnancy. Participants answered ‘yes’ or ‘no’ to the following questions: Did you experience any negative attitudes or stigmatisation from anaesthesia colleagues in relation to your pregnancy? Did you experience any negative attitudes or stigmatisation from non-anaesthesia colleagues in relation to your pregnancy? Overall were you satisfied with your experience of working while pregnant? Did your experiences of working while pregnant influence future family planning decisions? Free text comments were also sought in response to these questions. The survey questionnaire is included in Supplementary material 1 online.
Quantitative data were imported from SurveyMonkey to SPSS (IBM SPSS Statistics, version 23) 27 for data processing and restructuring. Analysis included simple descriptive statistics where all responses have been summarised as frequency (%) for categorical variables, mean (standard deviation) for normally distributed continuous variables, and median (interquartile range) for non-normally distributed variables. For the categorical variables the question either required respondents to select one of multiple options or the question required respondents to select all applicable options. The appropriate denominator is specified, as either number of responses or number of respondents.
Further exploratory analysis of associations between the pregnancy questions was undertaken. The associations were evaluated in response to predefined questions. These examined (for each pregnancy) the relationship between any adverse maternal or fetal/neonatal outcome with the following exposures: hours worked while pregnant; cessation of work or night shifts. For each respondent, the relationship between number of pregnancies and the following exposures were assessed: negative experiences at work during pregnancy; work satisfaction whilst pregnant. Further statistical analyses were performed using R (R: a language and environment for statistical computing, R Core Team, version 4.0.2). 28 Owing to the lack of independence of pregnancy experience responses from the same respondent (for the per-pregnancy associations), generalised estimating equations (GEEs) were carried out with respondent as the clustering variable. All outcomes for the GEEs were binary, thus binomial family and logit link functions were used. The GEEs were calculated in R using the geepack (v.1.3.4) package,29 –31 with an exchangeable correlation structure. Due to the independence in the per-respondent variables, simple chi-square tests (or Fisher’s exact tests in the case of low cell counts) were used.
Qualitative evaluation of the free text comments was completed using conventional content analysis. 32 The free text comments were repeatedly read by two authors (ILC, AFP) to achieve familiarisation, enabling the identification of key concepts and an initial coding scheme. All recurring concepts were subsequently grouped together and organised into major themes. These steps were performed independently to ensure interpretive rigour, with subsequent combined review and agreement by the same two authors on the final concepts and themes, with a third author (VAE) as arbitrator where required. All authors reviewed and agreed on the final analysis. Direct quotes that demonstrated examples of the major themes were provided verbatim, with de-identified respondent numbers provided in brackets. Due to the anonymous nature of the survey, member checking was not possible.
Four authors acknowledge their ‘insider status’ as anaesthetists who trained with ANZCA, worked in Australia as anaesthesia trainees and now are specialists in the field. The experience of pregnancy and return-to-work in this specific context, whilst influencing the choice to study this topic, was seen as valuable in recognising the language used and the experiences described. Self-reflexivity was employed to minimise the impact of insider status on interpretation of the data. Prior to commencing the qualitative analysis the authors reflected on their own experiences of working as anaesthetists whilst pregnant and acknowledged how particular comments evoked personal responses.
Results
Of the 311 surveys returned, only the results for the pregnancy component of the survey are presented. Two hundred and forty-two respondents met the inclusion criteria for having experienced at least one pregnancy whilst working in anaesthesia in the last 10 years. A total of 549 individual pregnancy experiences were described.
Table 1 summarises the survey respondent characteristics. The average hours worked per week was reported as 40 h or less in 248 (45%) pregnancies, 41–50 h in 257 (47%) pregnancies and 51 h or greater in 41 (8%) pregnancies. Cessation of night work (either shifts or on-call) was reported for 406 pregnancies; the median (IQR) gestation at which this occurred was 32 (30–34) weeks. The factors listed as affecting cessation of night work included concerns for maternal and/or fetal wellbeing in 132 (24%), tiredness and concentration in 126 (23%), physical difficulties in 101 (18%), planned leave in 72 (13%), departmental guidance in 65 (12%) and ‘other’ in 91 (17%). Cessation of all work was reported for 420 pregnancies, at a median (IQR, range) gestation of 36 (34–37, 5–40) weeks. This was most commonly due to reaching the planned gestation for leave (237, 44%), followed by physical difficulties (102, 19%), concerns for maternal and/or fetal wellbeing (97, 18%), tiredness and poor concentration (69, 13%), departmental guidance (13, 2%) or ‘other’ (72, 13%). Additional information on work patterns is provided in Supplementary Table 1.
Demographic information of pregnancy survey respondents (N = 242).
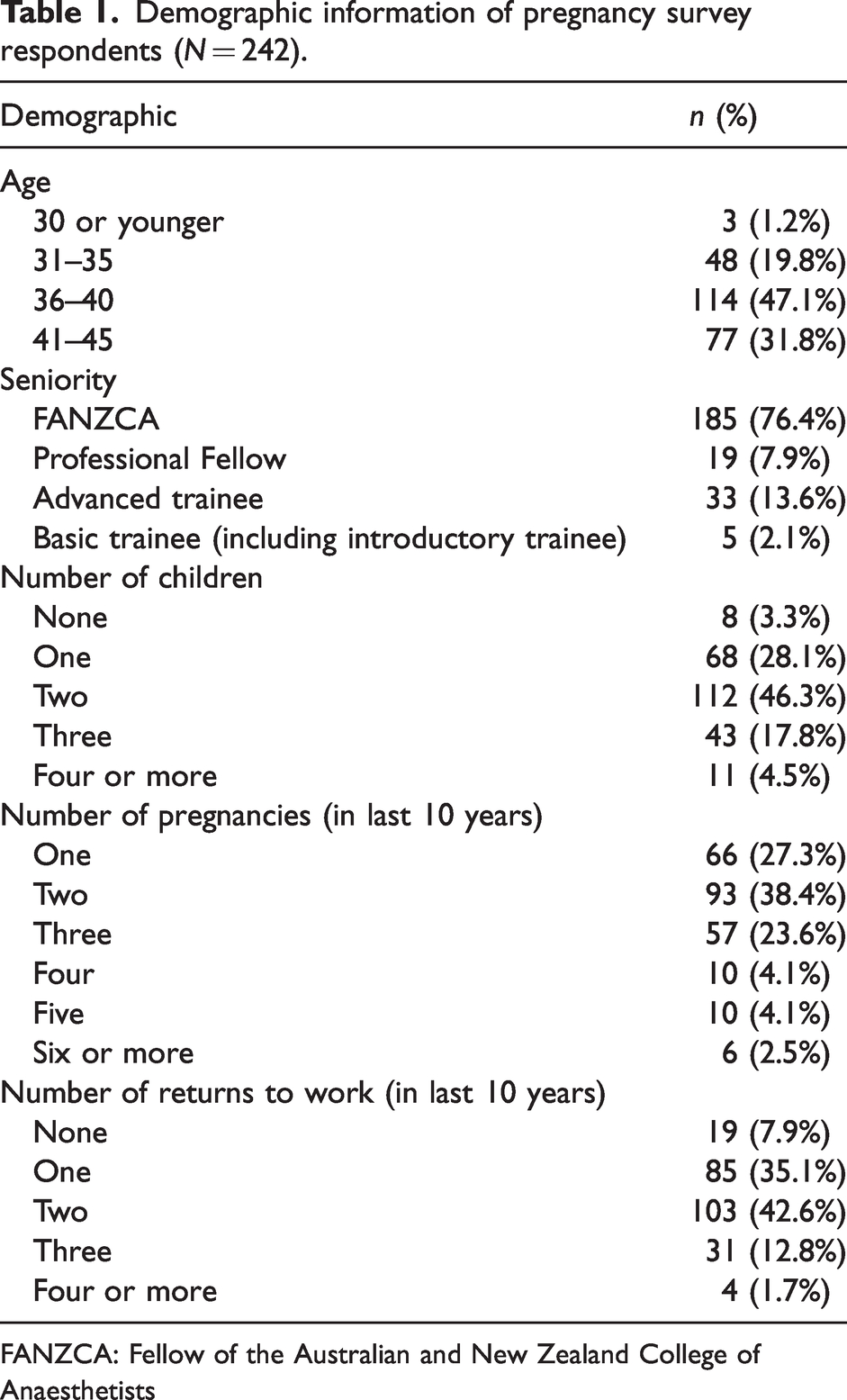
FANZCA: Fellow of the Australian and New Zealand College of Anaesthetists
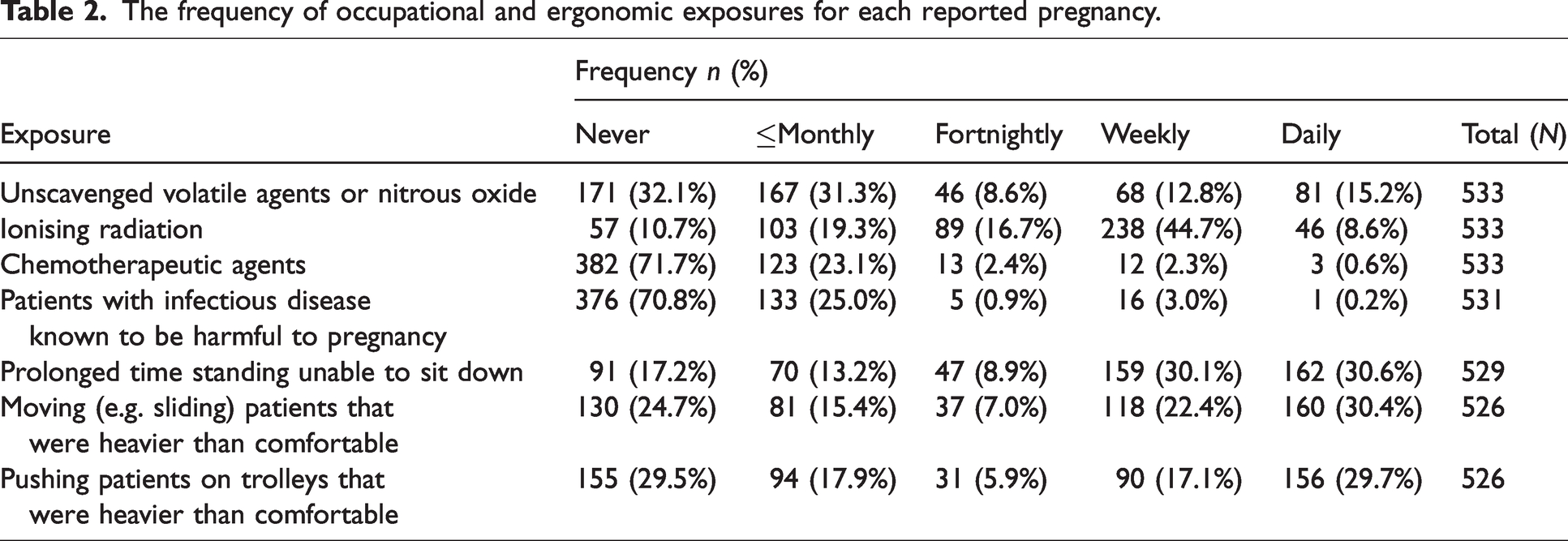
Table 2 reports on occupational and ergonomic exposures. Approximately 30% experienced ergonomic exposures daily, and over half reported exposure to ionising radiation either daily or weekly. Of 535 responses, 271 (51%) reported any work modifications occurring during pregnancy. Radiation avoidance was the most frequent modification, reported in 240 (45%). Fifty-three (10%) had increased clinics, 26 (5%) had increased pain rounds, 12 (2%) avoided unscavenged gases and 40 (8%) reported other modifications. Of the 534 responses reporting on their satisfaction with modifications, 121 (23%) were very satisfied, 119 (22%) were moderately satisfied, 163 (31%) were neutral, 83 (16%) were moderately dissatisfied and 48 (9%) were very dissatisfied.
The frequency of occupational and ergonomic exposures for each reported pregnancy.
Of 533 responses on average stress levels during pregnancy, 10 (2%) were debilitating, 105 (20%) were high, 173 (33%) were moderate, 204 (38%) were mild and 41 (8%) had no stress. Of 529 responses on worst stress levels during pregnancy, 57 (11%) were debilitating, 214 (41%) were high, 149 (28%) were moderate, 89 (17%) were mild and 20 (4%) had no stress.
Sources of stress were most commonly work-related, with 202 (83%) reporting this as one of the top three sources of stress. Professional exams were the greatest source of stress for 51 (21%) respondents, with 79 (34%) ranking them in the top three sources of stress. Anxiety surrounding pregnancy was ranked as the greatest source of stress by 49 (20%) respondents, and it was ranked in the top three causes of stress by 161 (67%) respondents. Figure 1(a) reflects the stress contributing factors by ranking, with further information provided in Supplementary Table 2. Respondents described varied sources of support as illustrated in Figure 1(b) with further information provided in Supplementary Table 3. Informal support from either a colleague or mentor was ranked first by 123 (51%) respondents. Forty-one (17%) ranked a lack of workplace support first.
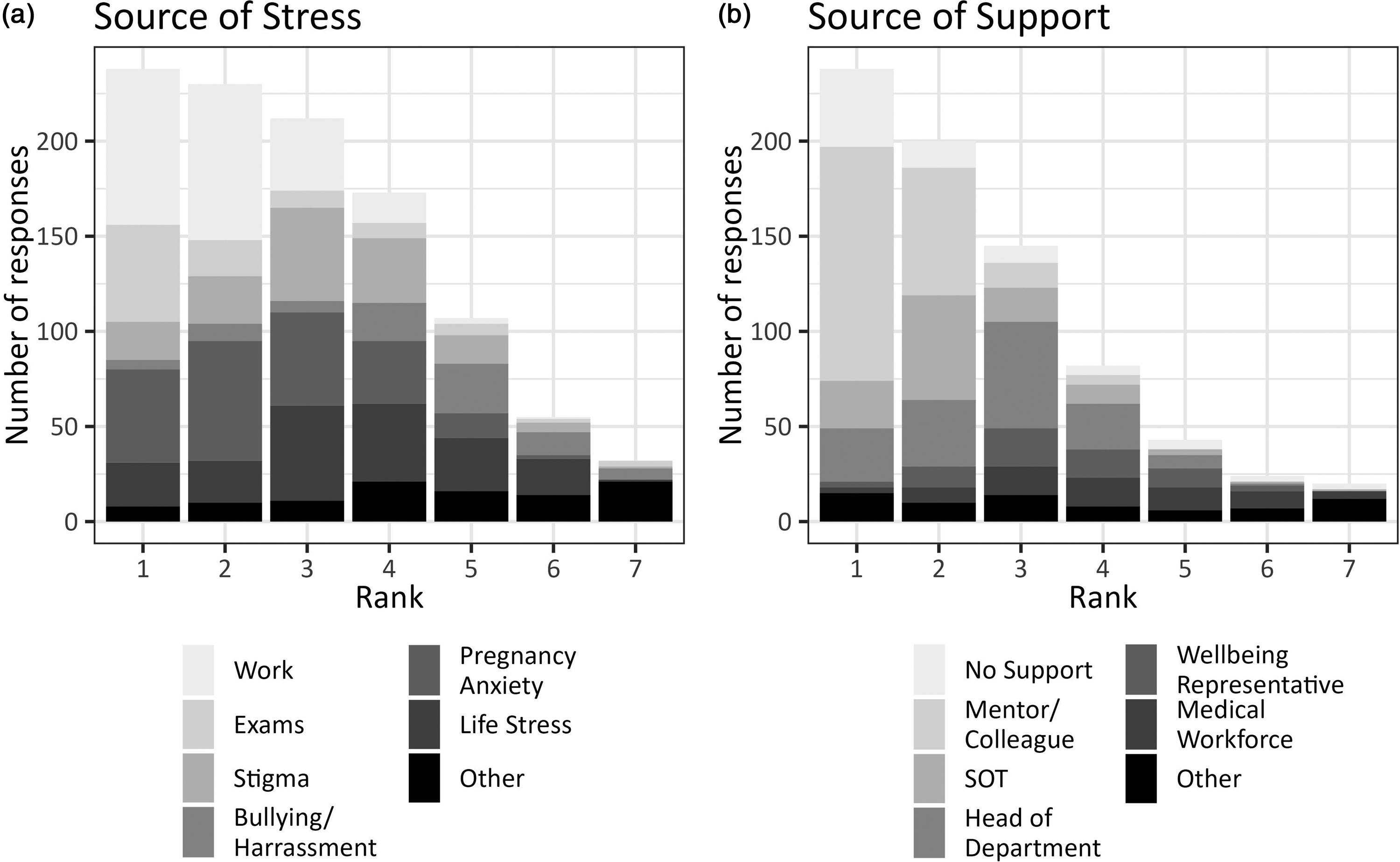
Contributing sources of stress (a) and support (b) during pregnancy. SOT: supervisor of training.
Reported neonatal birth outcomes.
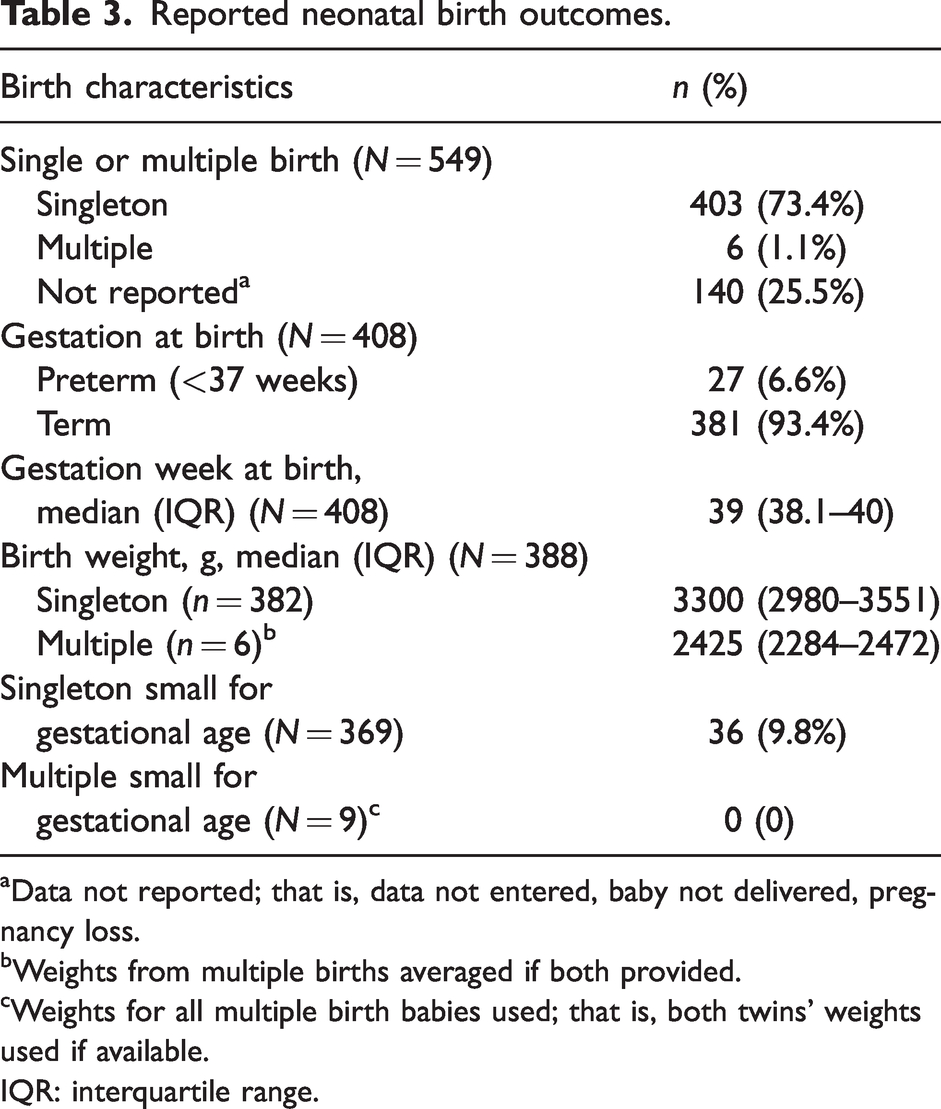
Data not reported; that is, data not entered, baby not delivered, pregnancy loss.
Weights from multiple births averaged if both provided.
Weights for all multiple birth babies used; that is, both twins’ weights used if available.
IQR: interquartile range.
Respondents were asked to report maternal complications, without providing specific definitions due to the assumed knowledge of the medical cohort being surveyed. Uncomplicated pregnancy was recorded for 262 (50%) responses. Of the 262 pregnancies where any complication was reported, the two most frequent were hyperemesis (n = 77, 15%) and threatened preterm labour (n = 42, 8%). Twenty-seven (7%) responses reported preterm birth. A formal mental health diagnosis was disclosed in only 23 (4%). Thirty-one (6%) reported gestational diabetes, 38 (7%) described musculoskeletal complications and 110 (21%) reported ‘other’ complications. No adverse neonatal/fetal outcomes were recorded in 388 (72%) of cases. Early pregnancy loss was reported in 100 (18%) pregnancies, late pregnancy loss in 3 (1%), neonatal complications in 34 (6%) and other reported fetal/neonatal complications in 27 (5%). Thirty-six (10%) small-for-gestational-age (SGA) singleton babies out of 369 were described (using the definition as reported birth weight less than the (non sex-specific) 10th percentile for gestational age). 33 Further detail is provided in Table 3 and Supplementary Table 3. Table 4 summarises the associations between specific exposures and any reported adverse maternal or reported neonatal/fetal outcomes. Reporting of exposure to ionising radiation did not delineate the wearing of appropriate precautions such as lead aprons. This was assumed to be in accordance with Australian standards, but cannot be confirmed. For ergonomic hazards, the moving or pushing of heavy patients on a daily to weekly basis were common (n 278, 53% and n 246, 47% respectively). The associated increased risk for any (combined) reported maternal complication for moving heavy patients was an odds ratio (OR) of 2.13 (95% confidence interval (CI) 1.37 to 3.33, P < 0.001). Similarly, pushing heavy patients on a daily to weekly basis had a corresponding OR of 2.28 (95% CI 1.49 to 3.48, P < 0.001) of any reported maternal complication. There was no association between the average hours worked per week and any reported adverse fetal/neonatal outcome. There was a reduced odds of any adverse maternal outcome when the gestation at which night work ceased was 34 weeks or later compared with <27 weeks (OR 0.52, 95% CI 0.28 to 0.96, P = 0.036), and if the gestation at which all work finished was 34 weeks or later compared with less than 34 weeks (OR 0.50, 95% CI 0.29 to 0.86, P = 0.012). Similarly, there were reduced odds of any reported adverse neonatal/fetal outcome when the gestational age at which all work finished was 34 weeks or later, compared with before 34 weeks (OR 0.45, 95% CI 0.22 to 0.91, P = 0.026). This relationship was not observed for gestation at which night work finished. Specific investigation into potential factors, including working hours, that may increase risk for TPL found no associations. Specific investigation into potential factors, including working hours, that may increase risk for TPL found no associations (see Supplementary Table 4). Self-reported average stress level was high or debilitating for 115 (22%) pregnancies and was associated with greater risk for any reported maternal complication (OR 2.36, 95% CI 1.46 to 3.82, P < 0.001), as described above. Worst stress level being reported as high or debilitating in pregnancy (n 271, 51%) was associated with an increased proportion of any maternal complications (OR 2.93, 95% CI 2.06 to 4.17, P < 0.001) and any reported neonatal/fetal complications (OR 1.72, 95% CI 1.10 to 2.69, P = 0.018). Exposure to infectious diseases known to be harmful in pregnancy showed an association with adverse neonatal outcomes (OR 3.0, 95% CI 1.02 to 8.74, P = 0.047) although numbers were extremely small and should be interpreted with caution.
Associations between the outcomes of any reported maternal and any reported neonatal/fetal outcomes and the factors of occupation/ergonomic exposures, self-reported stress levels, gestational age of cessation of work, and work hours.
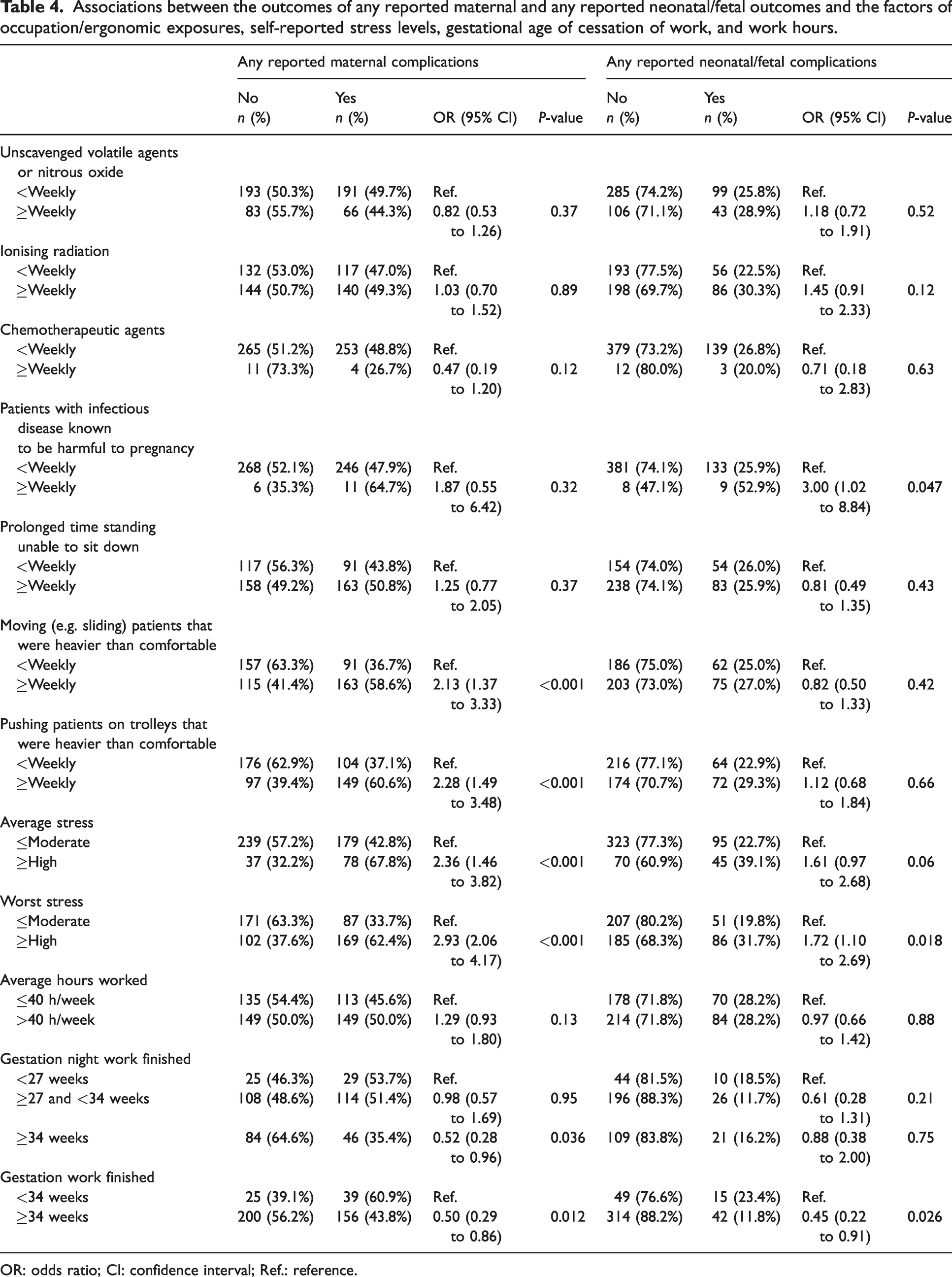
OR: odds ratio; CI: confidence interval; Ref.: reference.
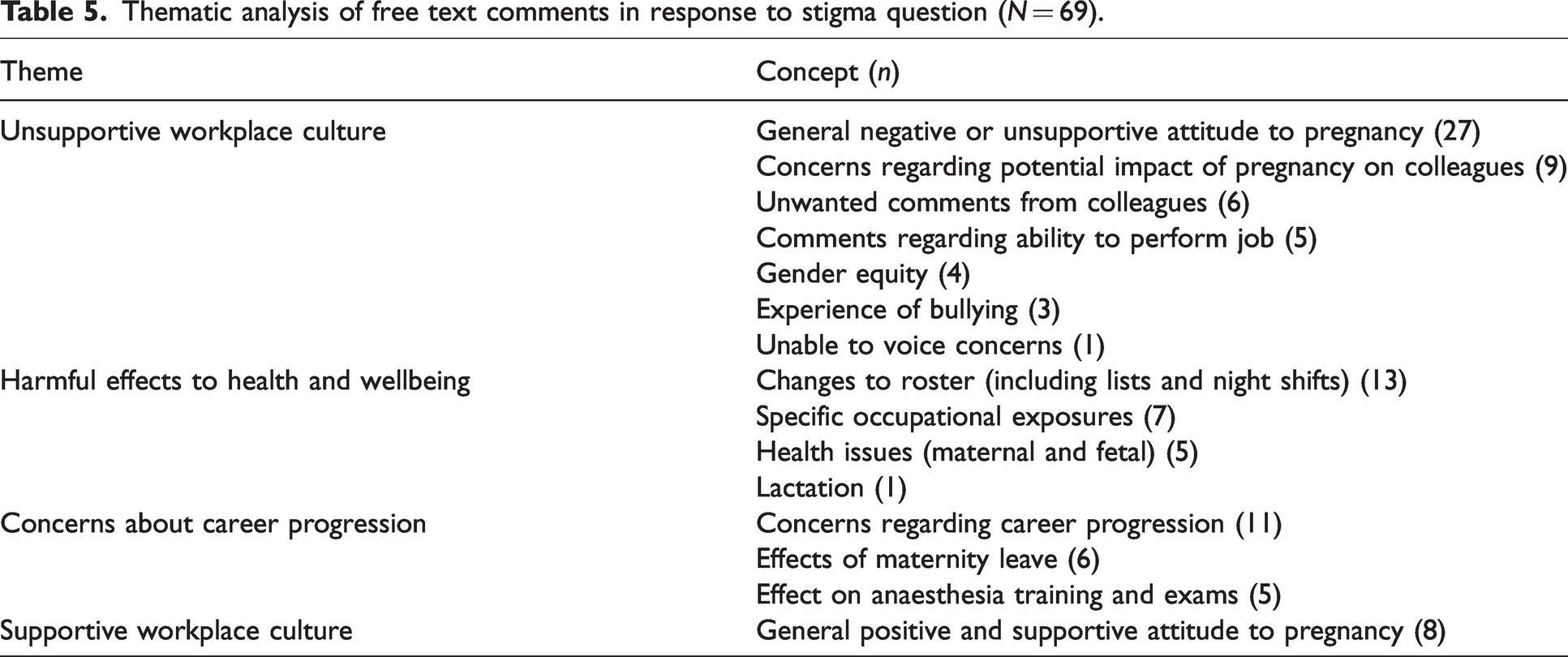
One hundred and forty-one (58%) respondents reported no exposure to stigma or negative attitudes towards pregnancy in the workplace. There were 91 (38%) respondents who reported stigma or negative attitudes from anaesthetic colleagues and 34 (14%) from non-anaesthetic colleagues. Of these, 25 (10%) was from both anaesthetic and non-anaesthetic colleagues. Increasing number of pregnancies experienced by each respondent was significantly associated with negative attitudes or stigma from anaesthetic colleagues (P = 0.005); 18 (69%) of respondents with four or more pregnancies experienced negative attitudes and stigma compared with 20 (30%), 33 (36%) and 20 (35%) for one, two and three pregnancies, respectively. There were 69 free text comments in response to the question ‘Did you encounter any stigmatisation or negative attitudes towards your pregnancy or pregnancies at work from colleagues?’ From these, 15 separate concepts were identified and coded. In total 111 codes were applied to the comments. The concepts, frequency and corresponding theme is summarised in Table 5.
Thematic analysis of free text comments in response to stigma question (N = 69).
Experiences of pregnancy whilst working in anaesthesia affected the family planning and choices about future pregnancies for 112 (46%) respondents. There was no reported effect on family planning for 130 (54%) respondents. There was no significant association between the number of reported pregnancies and satisfaction with experience of pregnancy whilst working in anaesthesia or decisions about future family planning. Further detail is provided in Supplementary Table 5.
Of the 242 respondents, 171 (71%) expressed overall satisfaction with their experience of pregnancy whilst working in anaesthesia.
Qualitative analysis
Thematic analysis in response to the questions ‘Have your experiences of pregnancy whilst working in anaesthesia affected your family planning and choices about future pregnancies?’ (73 comments) and ‘Overall have you been satisfied with your experience of pregnancy at work as an anaesthetist?’ (85 comments) are presented in Supplementary Tables 6 and 7, respectively. Overarching themes identified in the analysis of all three questions included: the influential role of workplace culture in providing both positive and negative experiences, concerns about the impact of work on maternal and fetal wellbeing, and the perceived effects of pregnancy and family planning on career progression and trajectory.
Workplace culture
Some respondents experienced a lack of support from both their departments and individual colleagues. Narratives described situations where pregnant anaesthetists were made to feel that their requests for roster changes were unreasonable. ‘My department decided that the only way I could be allowed off nights, in the late stages of pregnancy and pre-exam was via a group decision that they sent out to all trainees in the department. I felt saddened that my ‘issues’ were perceived to be affecting others’ (Respondent 187). ‘Told I had to do overnight on call while on parental leave. When I questioned this, I was told that it was fine and accepted practice. I had to involve people outside of our department to resolve this’ (Respondent 95).
Other respondents reported progressive departmental attitudes and supportive workplace environments contributing to a positive pregnancy or return-to-work experience in eight of the 69 narratives. Examples included encouragement of the pregnant anaesthetist by colleagues, and expressions of joy for their pregnancy news. ‘Overwhelmingly supportive attitudes from anaesthetic and non-anaesthetic colleagues’ (Respondent 56). ‘Amazing support from all work colleagues, who were delighted for me and supported me at all times’ (Respondent 290).
Health impact of work
Some respondents were concerned that their working conditions were unsafe for both mother and fetus; these were most commonly related to ionising radiation, shift patterns and ergonomics. ‘Told that there was no issue with X rays and pregnancy. Did not feel supported to speak up even though I did. Also, worse back pain from lead wearing wasn’t taken into consideration’ (Respondent 76), ‘Pressure to continue nights, unable to reduce hours, pressure to continue angio lists’ (Respondent 96). It was commonly reported that the onus of moving to a pregnancy-friendly list was placed on the pregnant anaesthetist, and they were made to feel like a burden. ‘Annoyance at having to change lists to non-ionising or just continually “forgetting” to put me on appropriate lists’ (Respondent 103).
Career progression
Some responding consultants described career progression being affected by pregnancy and parental leave. ‘Public hospital lists were changed and never returned to me after coming back from mat leave …’ (Respondent 26). ‘… with the second pregnancy, I was trying really hard to get the public job I wanted against a lot of competition from men who needed no allowances due to pregnancy or breastfeeding, and had no problems with doing extra work instead of family caring responsibilities’ (Respondent 162). ‘I was told by an SOT [supervisor of training] in first year not to think about getting pregnant in training as it would ruin my chances of getting a job at this tertiary facility again. There were casual jokes all the time about women who got pregnant and ruined their trajectory in the program and prospects’ (Respondent 192).
Discussion
Our results provide an extensive exploration of first-hand experiences of anaesthetists working while pregnant in Australia. We identified weekly or more exposure to ergonomic hazards and high levels of stress were the only exposures examined that were associated with poorer reported maternal and neonatal/fetal outcomes compared with those not reporting exposures. Both were commonly reported by respondents. Frequent (daily to weekly) exposures to unscavenged volatile agents, ionising radiation exposure or chemotherapeutic agents did not significantly increase risk. Exposure to stigma towards pregnancy from anaesthetic colleagues is an important finding, given that thematic analysis has highlighted the importance of workplace culture in determining both positive and negative experiences of working while pregnant. Despite these risks, overall perinatal outcomes were similar to the national average, and the majority of respondents expressed satisfaction with their experience of working in anaesthesia while pregnant.
Women working in anaesthesia who responded to our survey were commonly concerned about safe working conditions in pregnancy. Less than half of the anaesthetists surveyed were satisfied with the modifications in their workplace. It is acknowledged that there are unique risks to the mother and fetus associated with maternal work in medicine, and in the operating theatre specifically.12,13 We found a strong association between lifting or pushing patients heavier than comfortable on a regular basis, and any maternal complications. These ergonomic hazards have been identified in other studies of pregnant workers13 –15 and our data provide a focus for achievable improvement in the workplace. The Australasian Faculty of Occupational and Environmental Medicine, of the Royal Australasian College of Physicians, provides a guide for the risk assessment and management of occupational hazards, including gestation-specific ergonomic recommendations. This document is a useful resource for departments seeking guidance in establishing ‘pregnancy-friendly’ workplaces, noting that the development and implementation of policies and procedures concerning pregnancy should be non-discriminatory and flexible, as well as meeting legislative requirements. They propose an evidence-based approach which ensures that women remain integrated and engaged in their workplaces before, during and after pregnancy. 16
One-third of respondents’ pregnancies had average stress levels reported as moderate, with high or debilitating stress levels experienced in about one-fifth of cases. There was more than double the likelihood of any maternal complication when the average stress level was high or debilitating. In those pregnancies where the worst level of stress experienced was high or debilitating, there was an almost threefold likelihood of any maternal complication, and an increase in odds of adverse fetal or neonatal outcomes. Our results found that stress from work, exams and anxiety about the pregnancy were the three most highly ranked stress contributors, respectively, with work-related stress and pregnancy-related anxiety being rated by the majority in the top three causes of stress. Australian anaesthesia trainees have previously rated exams as a major source of stress and almost one-third have reported experiencing high or very high levels of psychosocial distress, with 11% receiving treatment for anxiety or depression.34,35 Pregnancy-specific anxiety is known to be a potent stressor which is associated with complications such as preterm birth.36,37 The number of formal mental health diagnoses was unusually low when compared with national data, where the Australian Institute of Health and Welfare reported a prevalence of 20% for perinatal depression in 2010. 38 The underlying reasons are likely multifactorial and may include limited timely access to mental health professionals, concerns about stigma, and potential impacts on job prospects or medical registration. 35 The Beyondblue survey of the mental health of Australian doctors describes multiple independent risk factors in this study population, who are known to be at a higher risk of psychological distress and mental health disorders. 39 This warrants a proactive approach to the identification of, and support for, perinatal mental health conditions in anaesthetic trainees and specialists. 12
The factors that were not associated with an increased risk for reported maternal complications or reported fetal/neonatal adverse outcomes included frequent exposure to unscavenged volatile agents, ionising radiation (where use of appropriate precautions is unknown), chemotherapeutic agents, prolonged standing, and gestation at which night work finished. Whilst exposure to infectious diseases known to be harmful in pregnancy showed a threefold increase in adverse neonatal outcomes, numbers were extremely small and results should be interpreted with caution. The association between increased risk with earlier cessation of work in anaesthesia is likely to indicate a consequence rather than causation, with a corresponding twofold increase in both reported pregnancy complications and reported adverse neonatal outcomes for those pregnancies where parental leave commenced at less than 34 weeks’ gestation.
In a 2014 review, one in two Australian women reported discrimination while pregnant, during parental leave or upon returning-to-work. 40 Consistent with this, our study demonstrated that approximately one in three female Australian anaesthetists experienced stigma or negative attitudes towards their pregnancy from anaesthetic colleagues. Stigma surrounding pregnancy has been reported to be as high as 60% amongst anaesthetists in the United States. 22 The stigma associated with pregnancy follows mothers throughout their professional lives and may be reflected by the gender wage gap, lower numbers of mothers in leadership roles and by women exiting the workforce. This phenomenon has been termed the ‘motherhood penalty’ and it describes the workplace discrimination mothers experience relative to women without children or males (with or without children). 41 Our thematic analysis demonstrates the extent to which workplace culture can positively and negatively influence an anaesthetist’s experience of pregnancy. Discriminatory behaviour was demonstrated in the free text comments, with negative experiences significantly outweighing the positive. Discrimination during pregnancy can have a detrimental long-term effect due to the negative impact on women’s mental and physical health, career and job opportunities, engagement with the workforce and attachment to the workplace. 40 A study exploring parental leave and return to work experiences in trainees and recently graduated Fellows of the Royal Australian and New Zealand College of Obstetricians and Gynaecologists from 2012 mirrored concerns about job opportunities and career progression. 42 Due to their large proportion of women in training and in specialist practice, recommendations from this survey included a proactive approach to workforce planning, particularly in relation to parental leave by individual departments, state health organisations and at a college level. The Australian Medical Association held a gender equity summit in 2019, identifying nine key action areas to address gender inequity. 43 These included addressing the impact of gender bias on job opportunities and career progression, improving access to leave entitlements, ensuring appropriate workplace support for pregnant and breastfeeding women, establishing gender diversity targets for representation and leadership, and promoting transparent reporting of gender equity data.
Our study revealed that whilst half of the pregnancies described at least one maternal complication, the reported perinatal outcomes, including preterm birth and SGA babies, were similar to the reported national average (7.4% and 8.2%, respectively for those with the least socioeconomic disadvantage). 44 The incidence of early pregnancy loss mirrors the estimated prevalence of miscarriage, which is greater than 15% in confirmed pregnancy. 45 Despite the high incidence of unfavourable working conditions reported, other factors (such as smoking and socioeconomic status) are likely to have been more favourable and could potentially influence the incidence of preterm birth and SGA neonates.
Although a number of concerns have been raised in our study, 71% of respondents reported that they were satisfied overall with the experience of working in anaesthesia while pregnant. Similarly, in a survey of pregnant surgical residents in the United States, 95% reported that they would still become parents again during residency, despite the significant challenges they experienced. 46 We suggest that without a widely promulgated ‘gold standard’ for ‘pregnancy-friendly’ workplaces, it is impossible to gauge how respondents may have set expectations for their pregnancy work experience.
This study had some limitations. We were unable to determine how many survey recipients met our inclusion criteria, because of the anonymous method of distribution, nor are we able to accurately estimate this, preventing an accurate calculation of the response rate. The nature of the questions precluded the discrimination between experiences that occurred during anaesthesia training and those that occurred while working as a specialist. Similarly, we were unable to discriminate between those that occurred in public versus in private practice. This limits our ability to accurately identify potentially remedial factors. ANZCA is a bi-national college, but we did not include New Zealand anaesthetists or trainees within our survey. The existing processes around pregnancy and return-to-work in New Zealand are considered more progressive and not directly comparable to Australian conditions. We have not surveyed the experiences of anaesthetists with primary infertility or those who have left the profession. Selection bias may have occurred, with over-representation of respondents with highly positive or highly negative experiences. The long survey time frame may contribute to recall bias, and respondents report their perceptions which are unable to be confirmed independently, with associated possibility of response bias. We did not clarify the level of training or seniority for each individual pregnancy experience so are unable to accurately perform sub-analysis of these groups. The sample size is relatively small when considering the comparison of outcomes reported. It is acknowledged that the maternal and neonatal outcomes in this survey were self-reported, rather than formal diagnoses supported by objective evidence. Therefore, the associations identified should be interpreted with caution, particularly in the instances of infrequent adverse outcomes.
While these results are specific to anaesthesia trainees and specialists working in Australia, there are similarities with studies undertaken in other specialties and overseas, broadening the relevance and transferability of results within medicine. Future contributions to research in this field could be directed towards a deeper understanding of the aspects of this study that have not been fully elucidated, given that this is an exploratory study. This includes further sub-analysis of the data collected in the survey. Further to this, the impact of level of training or seniority and nature of work (public vs. private practice) could be explored. The interaction between stress and the risks for perinatal mental illness within this demographic appears to be an important relationship that has yet to be explored. Further consideration of the factors that increase risk of maternal and fetal/neonatal complications, including ergonomic risks, and strategies for managing these risks safely in pregnant workers would be valuable.
Conclusion
These important findings highlight the generalised inadequacy of departmental policies and procedures relating to pregnancy in the Australian medical workplaces described in this survey. The onus of occupational safety is often placed principally on the pregnant worker. The authors, along with peak advisory bodies encourage a proactive approach to enable the provision of individualised support for pregnant workers. This study draws attention to the potential harms associated with ergonomic hazards and high levels of stress during pregnancy. The authors suggest the use of existing resources to address speciality-specific, predictable occupational hazards. Reassuringly, overall self-reported pregnancy complication rates and adverse neonatal outcomes were similar to national averages. While overall 71% of respondents were satisfied with their experience of working in anaesthesia while pregnant, ideally 100% should be satisfied. Reflection on the prevailing attitudes and standards within the medical profession, and within anaesthesia specifically, is essential. This must occur at the individual, departmental, national and college levels, to drive a change in workplace culture where it is required, and address the need for implementation of relevant, evidence-based policies in this field.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X241263116 - Supplemental material for Experiences of Australian anaesthetists and anaesthetic trainees of working whilst pregnant: Results of a national survey
Supplemental material, sj-pdf-1-aic-10.1177_0310057X241263116 for Experiences of Australian anaesthetists and anaesthetic trainees of working whilst pregnant: Results of a national survey by Rosmarin Zacher, Isabelle L Cooper, Anna F Pietzsch, Lachlan Webb, Anita M Pelecanos and Victoria A Eley in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X241263116 - Supplemental material for Experiences of Australian anaesthetists and anaesthetic trainees of working whilst pregnant: Results of a national survey
Supplemental material, sj-pdf-2-aic-10.1177_0310057X241263116 for Experiences of Australian anaesthetists and anaesthetic trainees of working whilst pregnant: Results of a national survey by Rosmarin Zacher, Isabelle L Cooper, Anna F Pietzsch, Lachlan Webb, Anita M Pelecanos and Victoria A Eley in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the search, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.