
Abstract
Laparoscopic robot-assisted colorectal surgery can pose significant haemodynamic challenges for patients with severe aortic regurgitation. The increased afterload caused by pneumoperitoneum and aortic compression, along with concurrent factors like hypercarbia, Trendelenburg positioning and ventilatory impairment, can worsen aortic regurgitation, leading to myocardial ischaemia and heart failure. Transoesophageal echocardiography (TOE) assists haemodynamic management intraoperatively but requires subspecialist skills and enables limited inferences to be drawn regarding the impact of afterload on myocardial performance. Minimally invasive haemodynamic monitoring enabling real-time visualisation of a patient’s ‘pressure field’ has been suggested as a potential adjunct or alternative to TOE, with the added advantage of providing continuous quantitative information about both stroke volume and the afterload to ventricular ejection in a single visualisation. We describe an example of successful concurrent use of pressure field haemodynamic monitoring and TOE in a patient with severe aortic regurgitation having a prolonged laparoscopic robot-assisted pelvic exenteration.
Keywords
Introduction
Laparoscopic surgery has multiple benefits, including reduced surgical trauma, reduced postoperative pain and shorter hospital length of stay.1,2 However, pneumoperitoneum and Trendelenburg or reverse Trendelenburg positioning impact haemodynamic stability.1 –3 This may increase the risk of cardiovascular complications in patients with cardiac and pulmonary comorbid disease. 3 In this patient population, careful management of haemodynamics during laparoscopic surgery is of special importance, particularly during robot-assisted surgery, which is associated with longer operative times. 4 The most common approach to managing haemodynamics is to rely on arterial pressure as a surrogate for end-organ perfusion, but in the setting of a patient with valvular pathology undergoing robot-assisted surgery this may pose challenges. Transoesophageal echocardiography (TOE)-guided haemodynamic management is considered optimal and provides information on the structure and performance of the heart; however, it requires subspecialist training and interpretation, and enables limited inferences to be drawn regarding the impact of afterload on myocardial performance and end-organ perfusion.
The ‘pressure field software’ is haemodynamic monitoring software which continuously resolves blood pressure into its cardiac and vascular components, displaying this relationship visually to guide clinical decision-making (Figure 1). The software continuously visualises the parameters of the pressure field equation,
5
which states that the mean perfusion pressure (MPP) of each cardiac cycle can be defined such that

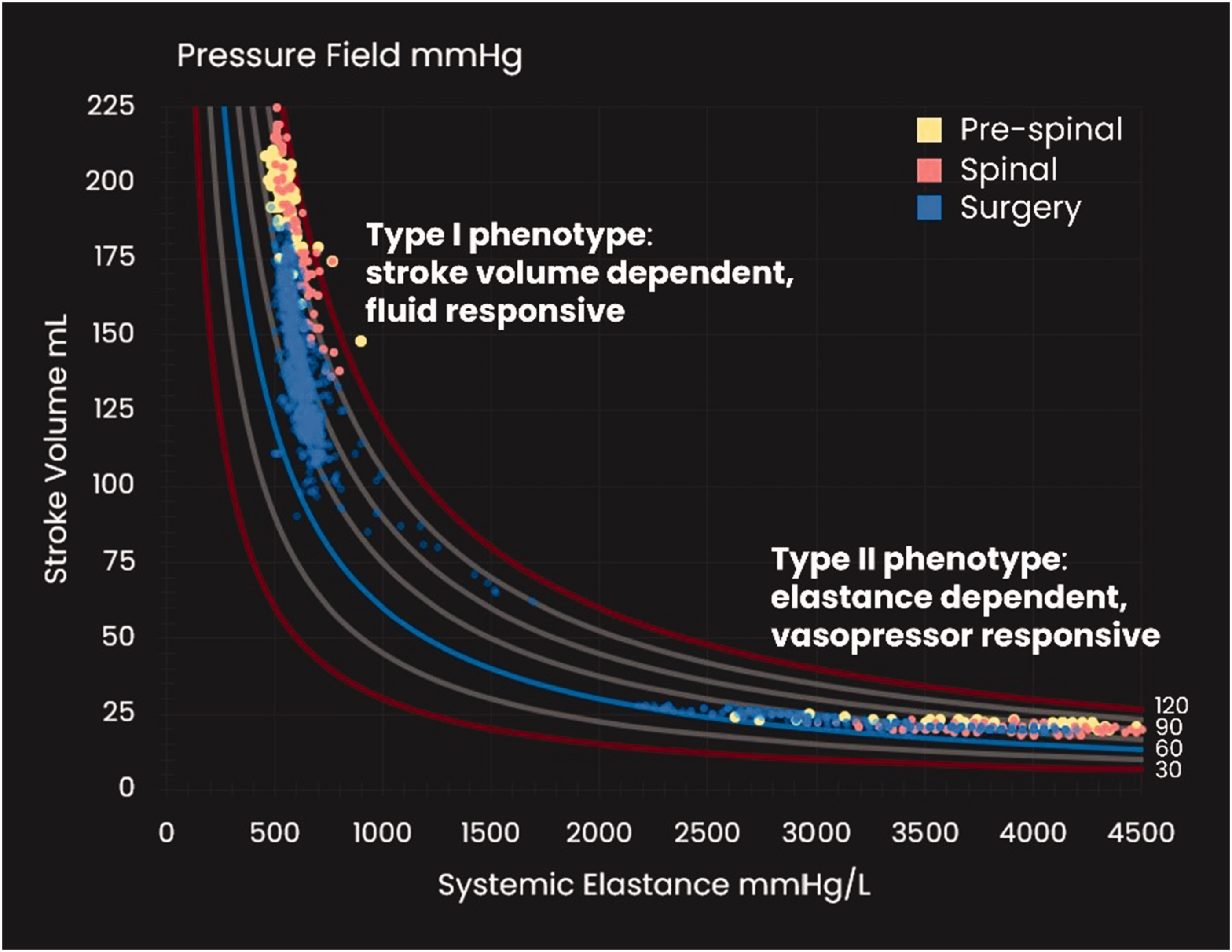
Pressure field illustrating the two types of circulation.
We describe the concurrent use of the pressure field software and TOE in a patient with severe aortic regurgitation having a prolonged (11-h) laparoscopic robot-assisted pelvic exenteration in the steep Trendelenburg position. Haemodynamic monitoring with the pressure field software was utilised to continuously interrogate the performance of both the heart and vasculature, in addition to TOE being used to intermittently interrogate the structure and performance of the heart.
Report
A 65-year-old 46-kg female presented for a laparoscopic robot-assisted pelvic exenteration for a large locally invasive rectal adenocarcinoma, complicated by a rectovaginal fistula with pelvic side-wall lymphadenopathy. She consented to the use of the pressure field software and the publication of this report.
The patient had a history of hypertension, mild coronary artery disease and severe asymptomatic aortic regurgitation. Preoperative medications included telmisartan and frusemide. On preoperative examination, the patient had a blood pressure of 140/60 mmHg and heart rate of 70 beats/min. A water-hammer pulse and a Grade 3 early diastolic murmur loudest at the left lower sternal edge were present and consistent with severe aortic regurgitation. There were no inspiratory crepitations and no peripheral oedema. Her recent transthoracic echocardiogram showed a moderately dilated left ventricle (LV) with normal systolic function, Grade 1 diastolic dysfunction and severe aortic regurgitation with a pressure half-time of 200 ms. Furthermore, the right coronary cusp prolapsed with a posteriorly directed jet. Diastolic flow reversal was seen in the descending thoracic aorta.
After multidisciplinary discussion between the colorectal surgeons, anaesthetists and cardiologists, it was decided that cancer surgery with a laparoscopic robot-assisted approach would proceed prior to valve intervention, and that both TOE and pressure field monitoring would be utilised perioperatively. The decision to convert to an open approach would be made early using TOE-based guidance, dependent on haemodynamic instability occurring.
In the operating room, a radial arterial cannula was placed and connected via a FloTrac sensor (FloTrac System 4.0, Edwards Lifesciences, Irvine, CA, USA) to the EV1000 monitoring system (Edwards Lifesciences, Irvine, CA, USA). A three-lumen central venous line was inserted in the right internal jugular vein, and the distal lumen connected via the TruWave transducer to the EV1000 monitoring system. The EV1000 monitoring system was connected to a laptop with the pressure field software via a serial-to-USB cable, data was transmitted every 20s from the EV1000 monitor, and the patient’s pressure field was calculated and displayed in synchrony. The patient’s resting pressure field was monitored before induction of anaesthesia to guide intraoperative management (Figure 2(a)).
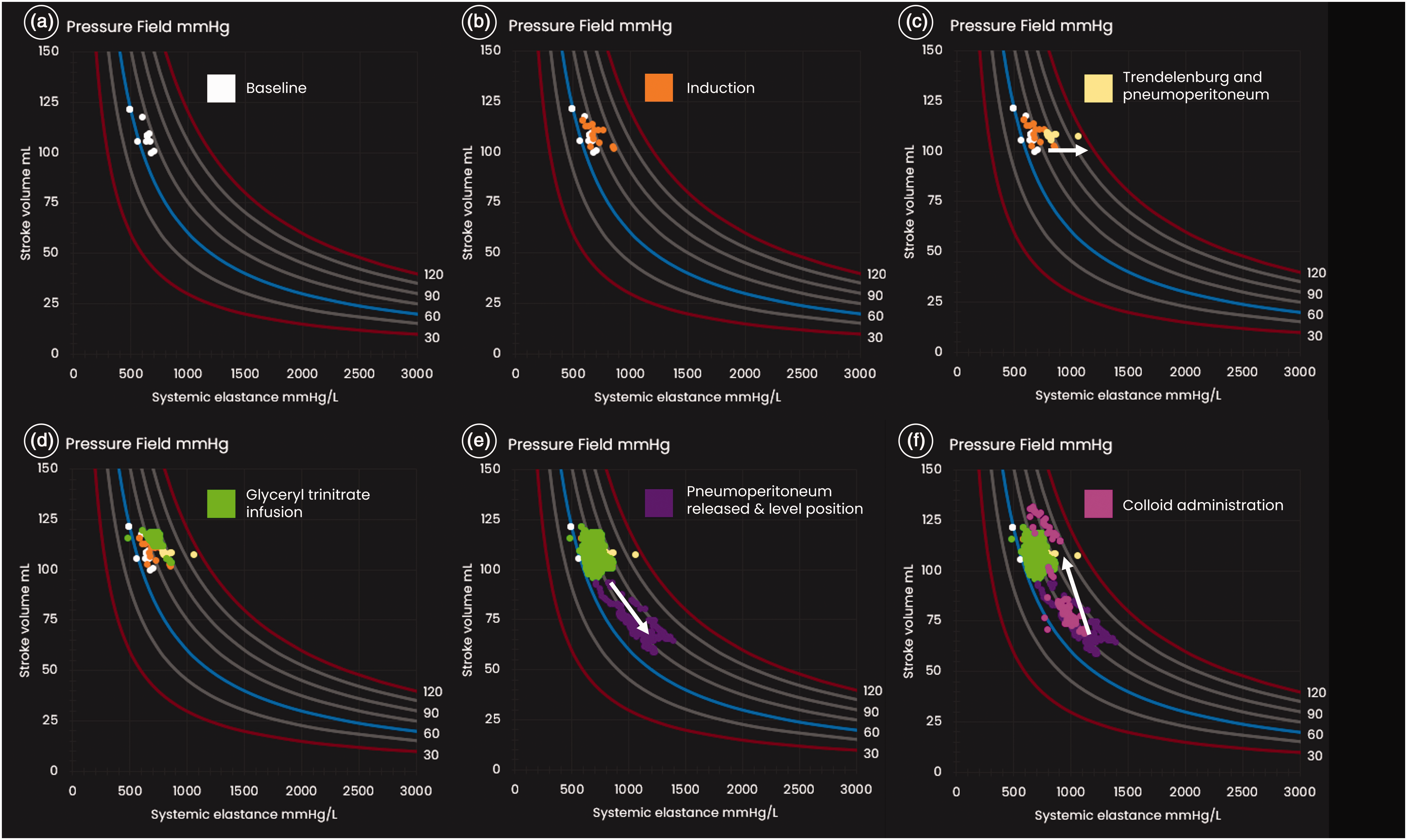
The pressure field visualisation. The X-axis represents systemic elastance as a measure of vasomotor tone; the Y-axis represents stroke volume, which varies with preload and contractility. The curved lines represent mean perfusion pressure, with pressure fields at intervals of 15 mmHg, between 30 mmHg and 120 mmHg. Mean perfusion pressure (that is, MPP = MAP – CVP) is at the intersection of these two coordinates. Each dot on the pressure field visualisation represents a time/data point. Each of the six diagrams displays the time/data points for part of the perioperative care period. (a) Pressure field at baseline; (b) induction; (c) during Trendelenburg and pneumoperitoneum; (d) after commencement of glyceryl trinitrate infusion; (e) after release of pneumoperitoneum and out of Trendelenburg to level position and (f) after fluid administration. CVP: central venous pressure; MAP: mean arterial pressure; MPP: mean perfusion pressure.
In the sitting position, a spinal anaesthetic with 0.5% plain bupivacaine 2 ml and intrathecal morphine 300 µg was administered. General anaesthesia was induced using fentanyl 150 µg, propofol 5 µg/ml using target-controlled infusion (Schnider model, effect site) and rocuronium 50 mg. The trachea was intubated. Anaesthesia was maintained with propofol (target concentration 2.5–3.5 µg/ml). Intraoperative TOE was performed. The TOE performed post-induction confirmed severe aortic regurgitation with pressure half-time of 190 ms, and a posterior directed regurgitant jet across the anterior leaflet of the mitral valve during diastole with a vena contracta width of 0.7 cm (Figure 3).
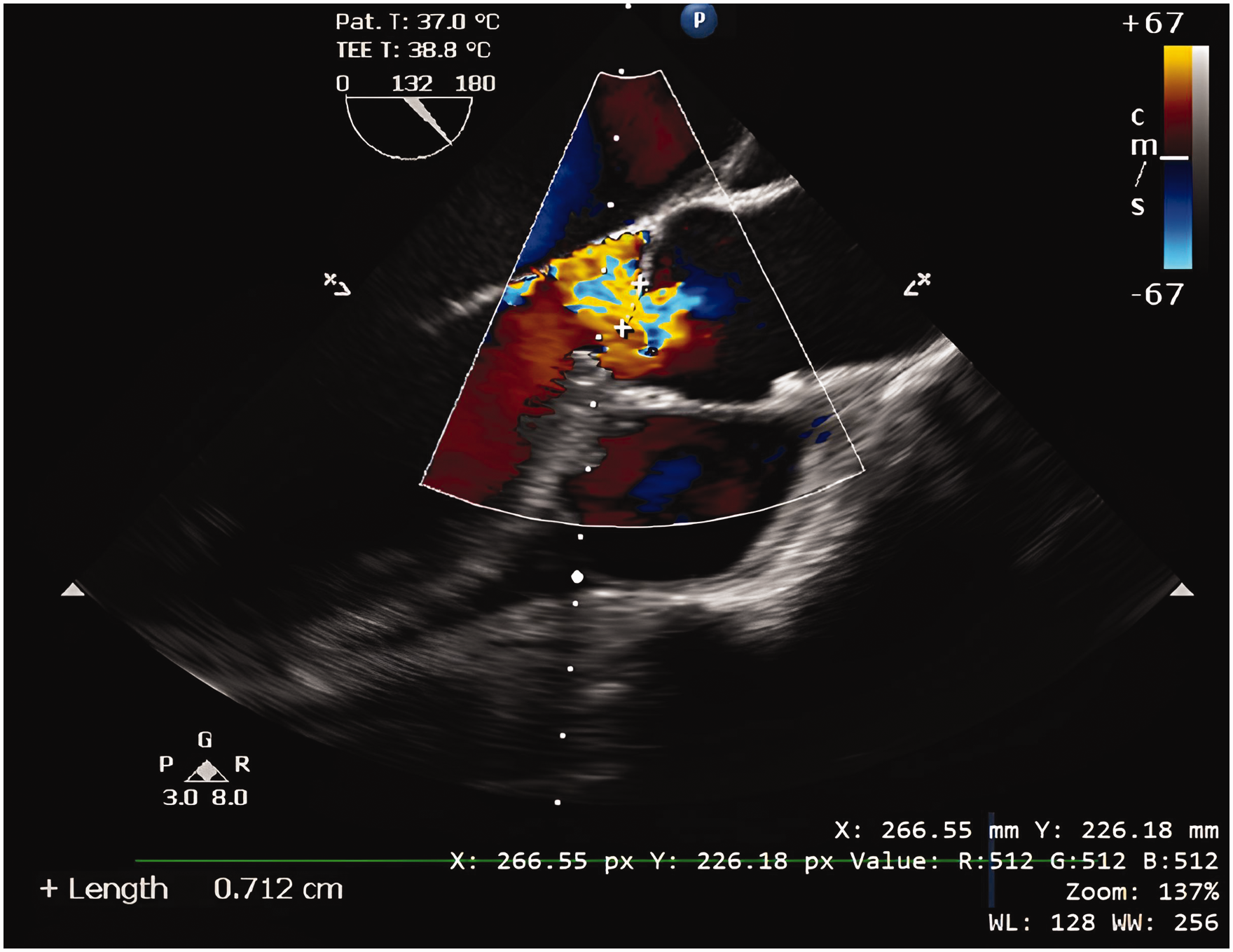
Pre-pneumoperitoneum transoesophageal echocardiography with a mid-oesophageal long axis view showing severe aortic regurgitation, with vena contracta width of 0.7 cm.
Following Trendelenburg of 24° and pneumoperitoneum of 15 mmHg, the patient became hypertensive to 190/60 mmHg with worsening of aortic regurgitation on TOE, with a vena contracta width of 0.9 cm. The inferior wall of the LV became hypokinetic. The pressure field concurrently displayed an increase in Esys with preservation of SV (Figure 2(c)), indicating a significant increase in afterload. Magnesium (10 mmol) was administered to reduce the blood pressure by vasodilation to 160/65 mmHg. LV regional wall motion improved and the pressure field concurrently normalised, displaying a reduction in Esys back to baseline levels with preservation of SV.
There was subsequently a progressive increase in Esys as the spinal anaesthetic wore off, and a glyceryl trinitrate (GTN) infusion was started at 5 µg/min and increased to 15 µg/min to counteract this (Figure 2(d)). The trend in Esys in the pressure field informed titration. Prior to starting the GTN infusion, TOE demonstrated worsening of the aortic regurgitation jet, which improved substantially upon up-titration of GTN.
Seven hours later, the pneumoperitoneum was released, and the patient was levelled out from the Trendelenburg position. The blood pressure reduced to 90/40 mmHg, and the pressure field showed a reduction in SV and increase in Esys (Figure 2(e)). The decrease in SV in the pressure field suggested an acute reduction in ventricular preload, which was visualised on TOE with a reduction in the LV diastolic volume, and so the GTN infusion was stopped and 100 ml of balanced crystalloid solution with 20% albumin was administered. The blood pressure rapidly improved to 140/70 mmHg with a recovery in SV and reduction of Esys.
A period of brisk blood loss (estimated blood loss of 500 ml with a haemoglobin drop from 101 g/l to 78 g/l) necessitated transfusion with two units of allogeneic red blood cells along with 200 ml of balanced crystalloid solution with 20% albumin, with SV increasing in response (Figure 2(f)). Real-time visualisation of the changes in SV in the pressure field informed the titration of fluids. TOE demonstrated a reduction in the LV diastolic volume during the period of brisk blood loss, with subsequent recovery during fluid therapy.
The total duration of the procedure was 11 h, the noradrenaline requirement was between 2 µg/min and 4 µg/min, the lactate remained below 2 mmol/l, and the urine output was greater than 0.5 ml/kg per h throughout. The patient was transferred ventilated to the intensive care unit. She was extubated the following day and transferred to the surgical ward. The next day, she developed a transient acute kidney injury with creatinine rise from 56 µmol/l to 119 µmol/l, and she was given 1 l of balanced crystalloid solution. This resolved completely over the subsequent three days. She did not have any signs of peripheral oedema. She was discharged from hospital after two weeks.
Discussion
Prolonged laparoscopic surgery in the steep Trendelenburg position has significant haemodynamic implications, especially in the setting of severe aortic regurgitation. The pneumoperitoneum-associated increase in afterload as a result of aortic compression and neurohormonal factors can result in worsening of aortic regurgitation and an increase in myocardial oxygen consumption.1 –3 This can cause myocardial ischaemia, and in the setting of increasing preload this could precipitate pulmonary oedema and heart failure. The concurrent hypercarbia and ventilatory impairment caused by the Trendelenburg position adds further insult, leading to progressive reduction in perfusion pressure and acidaemia.1 –3 Robot-assisted surgery generally requires higher pneumoperitoneum pressures and longer operating times, 4 compounding these cardiovascular and respiratory consequences. 1 For these reasons, severe valvular disease is considered a relative contraindication for laparoscopic robot-assisted intra-abdominal surgery; 7 and where undertaken, careful haemodynamic management is especially important. TOE-guided haemodynamic management is considered optimal and provides information on the structure and performance of the heart; however, it requires subspecialist training not commonly encountered in the non-cardiac anaesthetist, enables limited inferences to be drawn regarding the performance of the vasculature, and is most commonly used as an intermittent form of monitoring. 8
The pressure field is a novel approach to haemodynamic monitoring. It extends the work of Sunagawa et al., who in 1984 proposed that elastance is a better beat-by-beat measure of afterload than SVR. 5 SVR represents resistance to steady flow, but the human circulation is pulsatile with the arterioles the major source of resistance. Elastance is a pulsatile measure of afterload and a better measure of ventricular afterload because it is independent of varying heart rate.5,6 The application of Sunagawa and colleagues’ seminal laboratory work to critical care is nascent and has focused on validating various approaches to estimating elastance in the intact circulation.9 –13 The pressure field equation utilises Sunagawa’s concept of elastance to simplify Starling’s pressure equation to the relationship between SV and Esys (see Supplementary material online for the derivation of the pressure field equation). Where the pressure field equation is measured and visualised at high frequency, it provides a unique method for understanding the circulation and informs haemodynamic management. The beat-to-beat change in blood pressure is deconstructed into Esys on the X-axis and SV on the Y-axis (Figure 1), where Esys reflects vascular tone and SV reflects both preload and contractility. Initiating pressure field monitoring before induction enables a personalised template (baseline) to be identified, and this enables management to be guided by changes in the patient’s underlying physiologic state. The software interface is simple and intuitive, with a 1-h clinical education session sufficient to enable interpretation.
In our case, we found both TOE and pressure field monitoring useful in managing our patient. For example, although TOE demonstrated a worsening of regurgitation with Trendelenburg positioning, an increase in afterload as the primary cause and the quantum of this was only surmised from TOE; the pressure field supported this diagnosis. Similarly, TOE demonstrated a worsening of the aortic regurgitation jet as the spinal anaesthetic wore off, while the pressure field monitoring supported a diagnosis of increasing afterload and assisted in the precise titration of GTN in response; and TOE was useful in visualising the decreases in LV diastolic volume associated with levelling out and blood loss, while pressure field monitoring supported the diagnosis of decreased SV and also informed the titration of fluids in response. Further, whereas in this case TOE monitoring was intermittent (that is, ‘on and off’), an advantage of pressure field monitoring in this case resulted from its being ‘always on’: with each change in blood pressure, the pressure field provided in real-time an indication of the underlying cause, which usefully informed both the choice of intervention and, importantly, its dose and duration. The ability to visualise in a single picture the changes in the contribution of both the heart (SV) and the vasculature (Esys) to changes in blood pressure was of particular assistance in quick and timely decision-making, and represents an application of the human factors engineering principle of proximity compatibility. 14
In summary, magnesium, GTN, and fluids comprising 300 ml of 20% albumin, 2 units of red blood cells and 2 l of crystalloid were administered. There was 500 ml of blood loss, which was substantial for our patient as she was only 46 kg. Following surgery, she did not have signs of fluid overload; however, she did develop a transient acute kidney injury despite having a satisfactory urine output throughout. This could be explained by the long duration of pneumoperitoneum causing a reduction in renal blood flow. Reassuringly, there was no elevation in lactate throughout the case, which suggests that end-organ perfusion was satisfactory.
Pressure field monitoring relies on SV values estimated by arterial waveform pulse contour analysis. In this case, the pressure field monitoring was based on SV values provided by the current generation of the FloTrac algorithm, which is considered to be generally accurate in surgical and critically ill patients. 15 Its accuracy may be reduced in the presence of aortic valvular disease;16,17 however, in this case trends in SV values aligned well with TOE observations and informed management. Further, although the pulmonary artery catheter has been referred to as a gold standard for flow measurement, it does not enable continuous beat-by-beat estimation of SV (and thus does not enable continuous estimation of Esys), it is a more invasive form of monitoring with the associated risks, its availability may be limited in centres without a cardiac anaesthesia service, and there is equipoise in the literature regarding its use. 18 In addition, whereas the use of TOE requires substantial training, interpretation of the pressure field leverages the existing physiological knowledge of clinicians.
To date, use of pressure field monitoring to inform haemodynamic management has been described in a series of case studies, 5 including of a patient undergoing renal transplantation. 19 An ambidirectional study of patients undergoing cardiac surgery concluded that haemodynamic management based on pressure field monitoring led to a lower red cell transfusion rate due to decreased perioperative fluid loading. 20
In conclusion, we describe an example of the concurrent use of pressure field monitoring and TOE for haemodynamic management in the setting of severe aortic regurgitation. Pressure field monitoring may have a role in goal-directed therapy and enable lengthy steep Trendelenburg surgery to be performed in a safer manner in patients with severe valvular pathology. Pressure field monitoring may also be generalisable to all complex patients having major surgery in whom minimally invasive haemodynamic monitoring is clinically appropriate. Pressure field monitoring was helpful as adjunct monitoring in this patient. Its role as an adjunct or alternative to TOE monitoring should be formally evaluated in prospective clinical studies.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X241263115 - Supplemental material for Intraoperative ‘pressure field’ haemodynamic monitoring in a patient with severe aortic regurgitation having laparoscopic robot-assisted colorectal surgery
Supplemental material, sj-pdf-1-aic-10.1177_0310057X241263115 for Intraoperative ‘pressure field’ haemodynamic monitoring in a patient with severe aortic regurgitation having laparoscopic robot-assisted colorectal surgery by Walston R Martis, Charles Allen, Rajib Ahmed, Hilmy Ismail, StephenWoodford and Bernhard Riedel in Anaesthesia and Intensive Care
Footnotes
Patient Consent
This case report was published with the written consent of the patient.
Author Contribution(s)
Declaration of conflicting interests
S Woodford has received honoraria from Edwards Lifesciences. This author holds patents related to the pressure field.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.