
Abstract
Many studies have reported prolonged fasting times in children, associated with negative metabolic and behavioural outcomes. We felt that although our paediatric preoperative clear fluid fasting guideline was only for 2 hours, prolonged fasting still occurred for some patients. We conducted an audit of paediatric fasting times, before and after introducing a new protocol of ‘apple juice on arrival’, in which, on arrival to the children’s ward, all children received 3 ml/kg of apple juice. Data were collected prospectively from patients and their parents for two 4-week periods (before and after introduction of the protocol). Data included fasting time (solids and clear fluids), capillary blood glucose levels, knowledge of fasting requirements and sources of fasting information before surgery. Thirty-nine and 40 children, respectively, were included in each group before and after protocol introduction. Clear fluid fasting times reduced from an average of 9.9 hours pre-intervention to 3.5 hours post intervention (P < 0.01). In addition, mean preoperative blood sugar levels increased from 4.9 mmol/L (pre-intervention group) to 5.6 mmol/L in the post-intervention group (P < 0.001). The implementation of an apple juice on arrival protocol appeared to be an effective method to reduce clear fluid fasting times in children in our institution.
Introduction
During anaesthesia, the loss of protective airway reflexes and consequent risk of aspirating gastric contents means preoperative fasting is a universal practice. 1 Traditionally, ‘fast from midnight’ was a common approach to reduce the risk of pulmonary aspiration during both adult and paediatric anaesthesia. Acknowledging that this could result in excessive fasting times with risks of dehydration, hypoglycaemia and hypotension, North American and European associations of anaesthesia adopted new guidelines in the early 2000s.2 –4 These recommended fasting from solid foods for 6 hours, breast milk for 4 hours and clear fluids for 2 hours (6-4-2 rule) prior to anaesthesia. The Australian and New Zealand College of Anaesthesia (ANZCA) adopted these guidelines, and they remained in place for many years. 3 More recently, anaesthetic societies of Australia, New Zealand, Canada and Europe, have endorsed a one-hour clear fluid fasting time guideline in paediatric anaesthesia practice.5,6
Studies investigating more liberal fluid fasting have demonstrated benefits including reduced ketone production, reduced rates of post-induction hypotension, 5 reduced length of stay, earlier return of bowel function and lower incidence of postoperative nausea and vomiting.7 –9 Research indicates that pulmonary aspiration in children is relatively rare, including a multicentre study of over 118,000 patients in the UK, where aspiration occurred in only 2.0 to 2.2 cases per 10,000 anaesthetics. 10 The Anaesthesia Practice in Children Observational Trial (APRICOT) reported an incidence of nine cases per 10,000, with no aspiration events associated with long-term morbidity or mortality. 11
In 2022, ANZCA updated its fasting guidelines, which now recommend children older than 6 months of age fast from solids for 6 hours, breast milk for 4 hours and clear fluids for one hour. 12 However, these changes have not been universally adopted and at Peninsula Health, Melbourne, where the current study took place, paediatric fasting times remained as 6 hours solids—4 hours breast milk—2 hours clear fluids until recently. The primary aim of our study was to audit paediatric fasting times before and after the introduction of a new ‘apple juice on arrival’ protocol for our paediatric patients. A secondary aim was to determine admission blood glucose levels in the fasting paediatric population, given these data were routinely collected.
We postulated that offering children preoperative apple juice on arrival to the paediatric ward would be an effective, safe, and feasible way to reduce prolonged clear fluid fasting, while aligning more closely with the new ANZCA paediatric fasting guidelines. However, we felt that simply changing to the one-hour rule may still result in prolonged fasting, as other hospitals had reported that actual mean fasting times with this strategy were 2.5 hours at best, and 6 hours at worst. 5 Moreover, because parents may receive their fasting instructions from a variety of clinical craft-groups (surgeons/anaesthetists/emergency department clinicians/paediatricians), new guidelines may require a significant investment in educational resources and time to disseminate and fully implement. Because the paediatric ward and its nursing staff are the common pathway for all paediatric admissions, an apple juice on arrival protocol is an alternative approach in which education may be focused on paediatric nursing staff as a priority; potentially implementing the new one-hour guideline quickly and efficiently. In addition, it was hypothesised the apple juice intervention would increase average admission blood glucose levels.
Methods
This was a pre and post-interventional audit, conducted at Peninsula Health (Frankston Hospital), a Monash University-affiliated teaching hospital situated in suburban Melbourne, Victoria, Australia. A variety of adult and paediatric (non-neonatal) surgery is performed at the hospital, with paediatric surgery predominantly being elective general surgical and ear/nose/throat cases, plus orthopaedic and plastic surgery emergency cases. Peninsula Health Human Research and Ethics Committee approval was obtained on 9 February 2023 (QA/9439/PH-2023). Only verbal consent for data collection on the day of surgery was required. The two audit periods were 4 weeks each: February/March 2023 for the pre-intervention period and April/May 2023 for the post intervention period. Due to availability of data collectors, only cases on lists between Monday to Friday, 08:00 to 17:00 hours were included. Parents of all patients younger than 18 years of age having elective or emergency surgery were approached for data collection during these times. Data were collected in the preoperative holding area of the Frankston Hospital theatre complex, a 10-bay room adjacent to the operating theatres which includes a dedicated paediatric area. Exclusion criteria were cases occurring at weekends or after-hours (weekdays), and patients with intra-abdominal pathology (strictly ‘nil orally’), including nauseated/vomiting children. Included emergency cases were semi-elective in nature: minor plastic or orthopaedic surgery occurring on planned plastic/orthopaedic trauma lists. Such children did not present directly from the emergency department (ED) to theatre but were discharged from the ED to either home or the paediatric ward for overnight stays prior to transfer to theatres on the following day.
Data collection
Data collection was identical in the pre and post-intervention periods and took place in the preoperative holding bay of the theatre complex. Paediatric patients or their carers were asked for the time of last solid food, clear fluid, and breast/formula milk (if relevant). Time of patient arrival in the paediatric ward, time of being called for theatre, and time of entry into the operating room for surgery was recorded from the hospital’s patient administration system, iPM (Dedalus, Milan, Italy). Fasting times were calculated as the difference between the self-reported times of last consumption of solids and fluids and the time of entry into the operating room, for both the pre and post-intervention groups. Patients/carers were asked who provided the fasting instructions, if any: paediatric ward staff, surgical staff, the emergency department staff, anaesthetists, or other.
Other data collected included patient age, sex, and operation details (the procedure being performed, whether elective or emergency). Capillary blood glucose levels on admission were recorded as the paediatric ward routinely performs this test on fasting children and records it on the anaesthesia chart. Morbidity or other harms, including aspiration or surgical delay were collected through the anaesthesia department’s morbidity/mortality reporting system.
Intervention
Following the initial audit, apple juice on arrival was given to all paediatric patients undergoing surgery as soon as they arrived on the paediatric ward. Single-serve Ripe Road apple juice (Just Squeezed Juices, Campbellfield, VIC, Australia) containing 0.3 g of sugar per 3 ml was given at a volume of 3 ml/kg. Education was provided to paediatric nursing staff, with the focus on apple juice being provided immediately on children arriving in the ward, allowing there to be at least one hour between patient arrival and the 08:00 scheduled theatre commencement time for the first patients. Consequently, nursing staff were asked to perform other tasks, such as weighing children, recording vital signs, and assisting children with theatre attire after the apple juice was offered. During the intervention period, blood glucose levels were determined after apple juice administration, following other vital sign observations. This was generally 20 to 30 minutes after children arrived in the ward. There were no associated changes during the intervention period, such as patient/carer educational campaigns, education of ED/surgical staff, or changes to fasting-relevant printed information.
Data analysis
Data were de-identified prior to analysis. Data was entered into a database and exported to STATA (version 13: StataCorp 2013. Stata Statistical Software: Release 13. College Station, TX, USA: StataCorp LP). Continuous data were summarised with mean, standard deviation (SD), median and interquartile range. Categorical data were summarised as counts and percentages. Continuous data were analysed using an unpaired two-tailed t-test assuming unequal variance and Wilcoxon rank sum test for skewed data. Categorical data were analysed with Fisher’s exact test. The level of statistical significance was set at a P-value less than 0.05.
Results
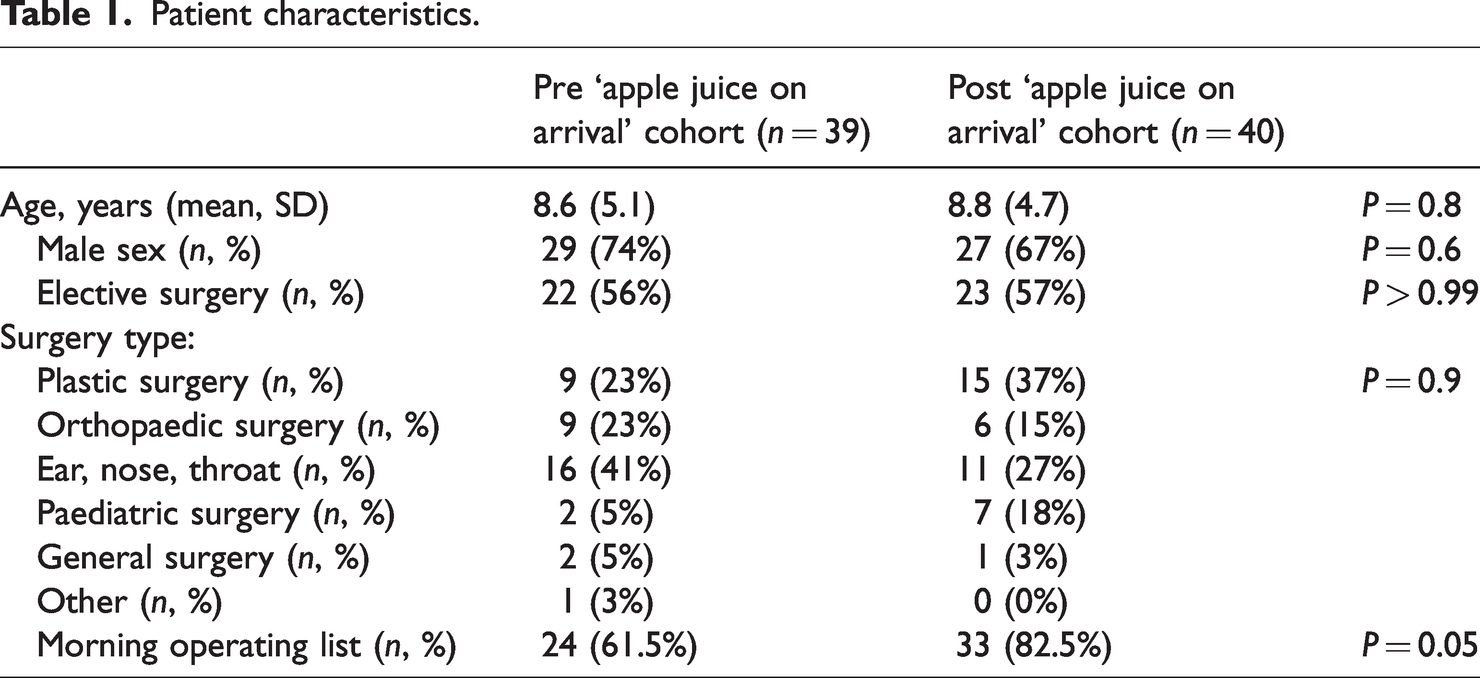
Data were collected on 79 patients in total; 39 prior to and 40 after the initiation of the apple juice on arrival protocol. Patient and surgery characteristics are displayed in Table 1, showing most of the paediatric surgery at the health service were minor plastics, orthopaedic or otolaryngology (ENT) procedures. The two groups were well balanced, apart from the post-intervention period having significantly fewer afternoon cases, which just reached statistical significance (Table 1).
Patient characteristics.
The time (mean, SD) between theatre staff calling the paediatric ward for the patient to be transferred from ward until theatre arrival was the same between pre-intervention (0.94 hours (0.5)) and post-intervention periods (0.94 hours (0.5)) (P > 0.99). The major fasting outcomes are shown in Table 2.
Major fasting outcomes.
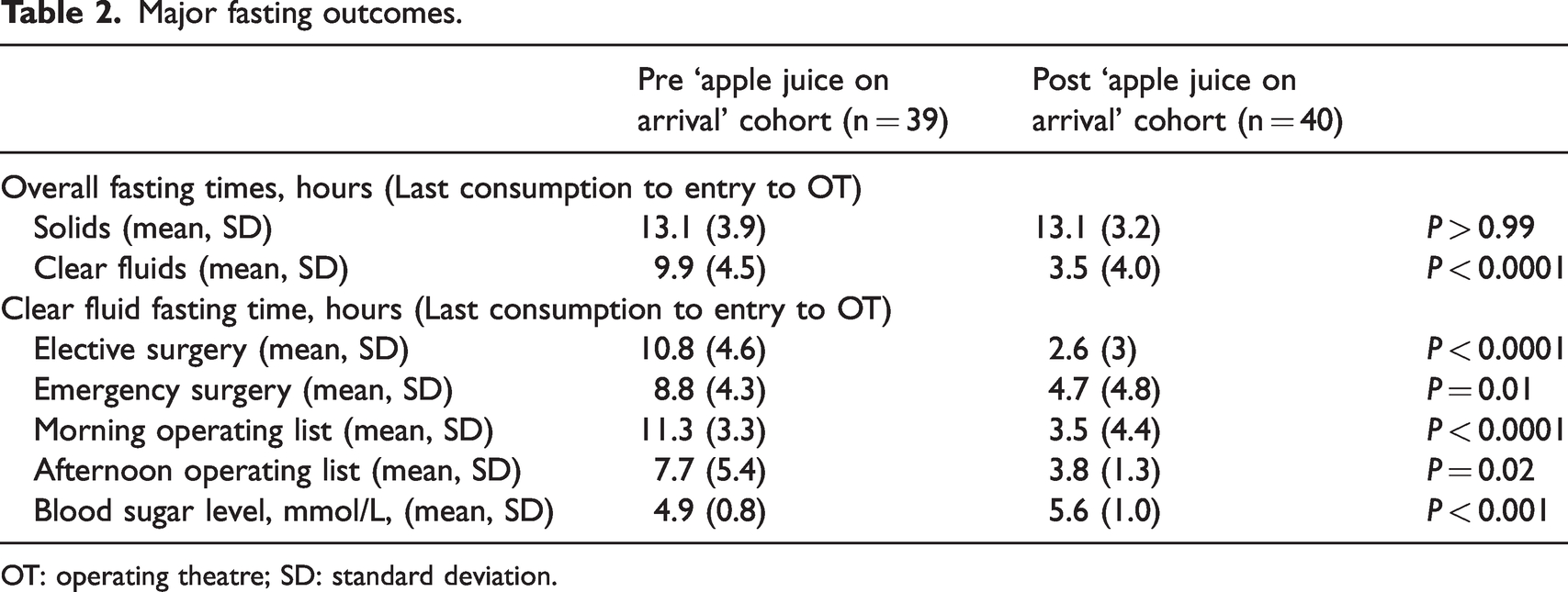
OT: operating theatre; SD: standard deviation.
As expected, fasting times for solids were not changed by the intervention and averaged 13.1 hours during both audit periods (Table 2). In the pre-intervention period, clear fluid fasting times were much greater than recommended guidelines at 9.9 hours (Table 2). Following the implementation of the apple juice on arrival protocol, the mean clear fluid fasting times were 6.4 hours shorter at 3.5 hours (P < 0.0001) (Table 2). Significantly shorter clear fluid fasting occurred in the post-intervention group, regardless of whether surgery was elective/emergency or occurred on a morning or afternoon operating list. Prior to the intervention, clear fluid fasting was significantly longer for morning cases (11.3 hours) than afternoon cases (7.7 hours) (P = 0.01), but such list-time effects ceased to be significant following the intervention (morning 3.5 hours versus afternoon 3.8 hours, P = 0.9) (Table 2). Although elective surgery clear fluid fasting was particularly impacted by the intervention, there were no significant elective/emergency fasting time differences before (elective 10.8 hours versus emergency 8.8 hours, P = 0.17) or after the intervention (elective 2.6 hours versus emergency 4.7 hours, P = 0.1) (Table 2). In the pre-intervention period, there was one case of borderline hypoglycaemia (3.4 mmol/L) and one severe case (1.8 mmol/L), requiring intervention and delay to surgery. The lowest blood sugar in the post-intervention period was 4.4 mmol/L. No cases of aspiration occurred, but one case of delay to surgery occurred post-intervention, with one child arriving in the anaesthesia room having only had 50 minutes of clear fluid fasting.
Parents had significant gaps in knowledge regarding fasting, both before and after the intervention, with 72% believing it was the same for solids as clear fluids during both periods. Before the intervention, 15% were aware that there were different fasting times for clear fluids compared with solids, rising to 18% after the intervention, with the rest unsure. Parental recall of how they received the fasting instructions varied little between the pre and post-intervention periods (Figure 1). Staff on the paediatric ward most frequently communicated instructions, followed by emergency department staff and surgeons. Anaesthetists did not directly communicate instructions to families.
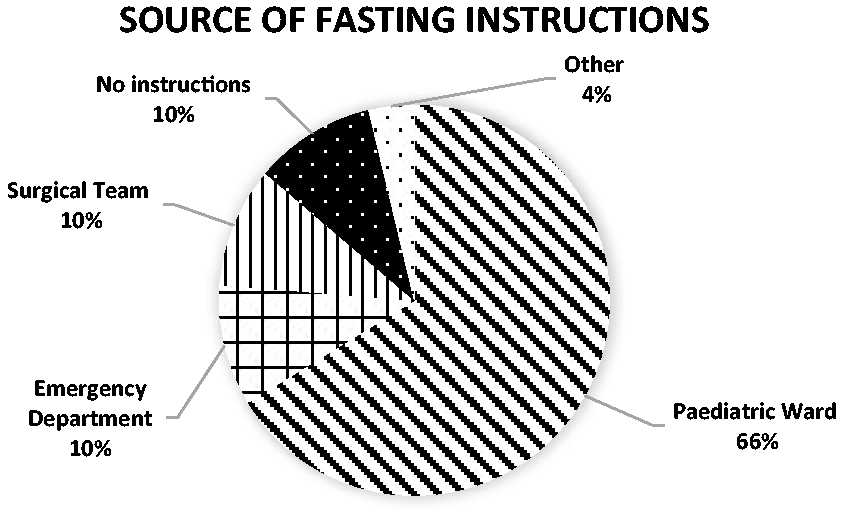
The source of fasting instructions provided to children and their families.
Discussion
This study showed that our existing preoperative fasting practices resulted in excessive paediatric fasting times and increased the risk of hypoglycaemia. Even though our local guideline was for 2 hours of clear fluid fasting, the initial audit found average fasting times almost five times longer. There were significant gaps in patient/carer understanding of fasting times, and communication about this important anaesthetic issue had largely been delegated to paediatric ward nurses. The implementation of an apple juice on arrival protocol to the paediatric ward rapidly improved our clear fluid fasting times without implementation of any significant educational campaigns for patients/carers, or health-service staff outside the paediatric ward. In the post-intervention period, the previously described variability in clear fluid fasting between morning and afternoon lists decreased significantly, and improvements occurred regardless of surgery being elective or non-elective. A unique aspect of our study is that because blood glucose levels are routinely performed on children before surgery, we were able to demonstrate that the intervention improved blood sugar levels, and there were no post-intervention hypoglycaemic events. There were no aspirations or other significant morbidity in this small sample. Apple juice was easily obtained by nursing staff in a timely manner, was easy to administer and acceptable to the majority of children.
Traditional 6-4-2 fasting guidelines were in place when conducting the initial audit on the pre-intervention cohort. Our reported mean clear fluid fasting time of 9.9 hours was similar to previously published studies of 6-4-2 fasting regimens.13 –15 The most recent ANZCA guidelines recommended paediatric patients fast for clear fluids for one hour preoperatively. 12 We have shown that offering all children apple juice on arrival to the paediatric ward is an effective method for quickly achieving clear fluid fasting closer to ANZCA recommendations. Others have achieved transitioning from 6-4-2 fasting rules to more liberal regimens in other ways, such as using quality improvement (QI) methodologies (plan-do-study-act cycles). For example, Newton et al. demonstrated that altering their protocol to allow children to consume fluid on arrival and up to one hour prior to surgery achieved a reduction in clear fluid fasting times from a mean of 6.3 hours to 3.1 hours. 15 However, this QI project took 2.5 years to complete and a significant investment in educational resources.
The reasons why our clear fluid fasting periods in children far exceed recommendations may be multifactorial. Children who sleep through the night may have insufficient time to drink before early morning surgery. It may be difficult or impossible for parents/carers or staff to predict accurately exactly when induction of anaesthesia will occur on a list of several children, particularly once any delays add up. 16 Educational factors were identified in our study, with most parents believing the fasting time for solids was the same as for clear fluids. There can be anxiety about possible delays, cancellation, or morbidity due to inadequate fasting, so fasting longer than required may appear a prudent approach. A major benefit of the implementation of apple juice on arrival within our institution is that regardless of these factors, there is an opportunity to provide clear fluids within guidelines and minimise the impact of these logistical challenges.
Besides thirst, discomfort and irritability, a major risk associated with prolonged fasting is hypoglycaemia. Children are more susceptible to hypoglycaemia than adults due to their comparatively smaller glycogen stores. 16 Fasting of toddlers for at least 6 hours resulted in a 28% incidence of hypoglycaemia in one study. 1 Our study demonstrated that offering apple juice on arrival to the paediatric ward resulted in a significant increase in preoperative blood sugar levels. While not measured in the current study, it has previously been demonstrated that prolonged preoperative fasting can result in ketoacidosis with normal to low blood glucose, particularly in children under 36 months of age.17,18 In addition to the metabolic advantages of reduced fasting times, there are also significant psychological impacts associated with prolonged fasting, including thirst, hunger, anxiety, discomfort, and poor behaviour. 19 Following our study, we have maintained the apple juice on arrival protocol in the paediatric ward, with the nurse unit manager reporting that (previously frequent) parental fasting complaints have been completely eliminated (personal communication, Helen Hutchins).
The mean time between the theatre staff calling for the patient to be brought from the ward to entering the operating room was almost one hour. Of itself, this usually provided enough time for the apple juice to have been given within guidelines, although a nursing staff educational focus on administering the juice as soon as the child arrived on the ward further increased the time safety margin. ‘Sip till send’ is another fasting strategy, allowing patients to consume clear fluids up until the time they transfer from the ward to theatre. 20 When supported by written/illustrated educational material and improved communication between staff and patients, ‘sip till send’ has been shown significantly to reduce clear fluid fasting time to 2.1 hours. 20 Because of the possibility that some children may be called to theatre shortly after arriving in the paediatric ward, we emphasised the importance to theatre staff of rigorously checking fasting times since our apple juice intervention, and we suggest it should be the case with ‘sip till send’. The major risk for patients who are not fasted appropriately is perioperative pulmonary aspiration, and this has been the greatest argument against reducing fasting times. Perioperative pulmonary aspiration is rare, and most patients will recover quickly without long lasting effects. 21 This is supported by studies investigating gastric emptying time in children. A small study of 14 school-aged children investigating gastric emptying time following ingestion of 3 ml/kg of sugared liquid showed that gastric volume returned to baseline within 60 minutes post-ingestion, with a half-life of 20 minutes. 22
Within Frankston Hospital, paediatric patients most often receive fasting instructions by a phone call from a paediatric nurse the day before their scheduled procedure. Most other patients receive their fasting instructions by emergency department doctors or a phone call from a surgical doctor. In this instance, strict fast from midnight instructions are often given to all patients irrespective of age. The results presented here indicate that most of our patients are receiving the same information regarding fasting from solids and clear fluids, which may be contributing to the prolonged fasting times experienced by some children. This highlights the need for continuing education of medical and nursing staff on current fasting guidelines, as better instructions given to patients may assist in avoiding prolonged fasting.
Strengths and limitations
Due to the presence of dedicated data collectors in the preoperative holding bay, complete, quality data were collected for all paediatric patients during the audit period. Blood sugar data and patient/carer knowledge of fasting added further value. However, this was a small, single-centre study. We did not measure patient and parent satisfaction with the implementation of the apple juice on arrival protocol, or determine if thirst, anxiety, or negative behaviour was reduced. There was no formal process for recording aspiration or other adverse outcomes beyond the usual departmental morbidity/mortality reporting system, so although it is unlikely that a significant event was missed, it remains possible.
Conclusion
This study shows that implementation of an apple juice on arrival protocol was feasible and effective at reducing paediatric preoperative clear fluid fasting times and increasing preoperative blood sugar levels. Given the significant metabolic and psychological sequalae of prolonged fasting in children, providing apple juice on arrival with the aim of reducing fasting time is likely to be safe and appropriate. Further education for medical and nursing staff providing fasting instructions to patients and their parents is required within our institution, and it is possible that this is also likely required in other similar institutions.
Footnotes
Acknowledgements
The author(s) wish to thank Ms Helen Hutchins, Nurse Unit Manager, Paediatrics, Peninsula Health for assistance with implementation of this study.
Author Contribution(s)
Data sharing statement
Original, de-identified data are available on any reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.