
Abstract
The regional and rural intensivist workforce is vital to delivering high standards of healthcare to all Australians. Currently, there is an impending workforce disaster, with higher senior medical officer vacancy rates among regional and rural intensive care units, with these units being staffed by junior doctors who are in earlier stages of their training, which in turn increases supervisory burden. There is a lack of comprehensive literature on the barriers and enablers of training, recruiting and retaining regional and rural intensivists. To address this gap, a qualitative study was conducted, involving 13 in-depth, structured interviews with full-time and part-time intensivists from eight Australian regional and rural hospitals. Content analysis of the interview data resulted in the identification of four major categories: unique practice context, need for a broad generalist skill set, perks and challenges of working in a regional/rural area and workforce implications. The study findings revealed that regional and rural intensive care practice offers positive aspects, including work satisfaction, supportive local teams and an appealing lifestyle. However, these benefits are counterbalanced by challenges such as a heavier burden of on-call work, a higher proportion of junior staff which increase supervisory burden and limited access to subspecialist services. The implications of these findings are noteworthy and can be utilised to inform government policies, hospitals, the College of Intensive Care Medicine and the Australian and New Zealand College of Anaesthetists in developing strategies to enhance the provision of intensive care services and improve workforce planning in regional and rural areas.
Introduction
Almost a third of the Australian population resides in regional, rural and remote areas, away from major metropolitan areas. 1 The rural and remote health report published by the Australian Institute of Health and Welfare in 2023 found regional, rural and remote Australians have poorer health outcomes than metropolitan Australians, and have less access to medical services. 2 A retrospective database review in 2020 found nearly 20% of intensive care unit (ICU) admissions in Australia were to ICUs located in regional and rural hospitals. 3 The provision of these regional and rural intensive care services is important to delivering equitable and high standards of healthcare to all Australians. Despite this importance, the most recent iteration of the Australian and New Zealand Intensive Care Society’s (ANZICS) critical care resources survey demonstrated higher senior medical officer vacancy rates among regional and rural ICUs, with these units being staffed by junior doctors who were in earlier stages of their training, which in turn increases the supervisory burden when compared with both public metropolitan and tertiary ICUs. 4
Understanding the lived experiences and perspectives of regional and rural intensivists can provide insights into barriers and enablers to an intensivist’s career and equitable regional and rural intensive care services. This can inform the educational requirements for training future intensivists in these settings, improve senior medical officer vacancy rates and shape training strategies for attracting more experienced junior doctors. 5 Furthermore, this can influence workforce planning and training strategies for government policymakers, hospitals, the College of Intensive Care Medicine (CICM), and the Australian and New Zealand College of Anaesthetists (ANZCA). This qualitative study explored important but inadequately addressed knowledge gaps on the experiences of regional and rural intensivists, and their perspectives on specific skills, workforce implications, and training, recruiting and retaining intensivists for regional and rural areas.
Materials and methods
Ethics
This study was approved by the St Vincent’s Human Research Ethics Committee (SVHAC HREC number: HREC 21/14; 29 November 2021).
Research design
This study employed a qualitative design utilising individual, in-depth, structured interviews.
Participants, sample and recruitment
Two rounds of participant recruitment occurred. In round one, all full-time, part-time and locum intensivists holding a fellowship with CICM and working in Toowoomba at the time of the study were invited to participate. Toowoomba is located 125 km west of Brisbane, with a population of over 115,000 and is classed as an MMM2 centre. This study adopted the modified Monash model (MMM), a geographical classification used by CICM, and defined regional and rural ICUs as those in MMM categories 2–7, excluding metropolitan centres.6,7 It is an inner regional city with one public and two private level 2 ICUs. 8 A convenience sampling strategy was used to facilitate recruitment. A target sample size of 10 participants was chosen based on recommendations for usability testing and credibility of qualitative data collection, analysis and pragmatic considerations for data adequacy.9 –12 A second round of targeted recruitment was necessitated to include representation from female intensivists. Information about the study was sent by email to members of the rural committee in CICM, shared on the CICM research promotion webpage and with established professional networks. Potential participants were provided with information about the study, recruitment details and a consent form.
Data collection
Participants who provided written consent completed an interview with one of the researchers (JGA or AJG) by Zoom, phone, or in-person between July 2022 and August 2023. Both researchers collecting data were novice researchers and were mentored by the first author (BKC; content expert) and the last author (PM; qualitative research expert). All researchers are experienced with working in clinical roles in healthcare settings. While all researchers have worked in rural and remote healthcare settings, the first and last authors (BKC and PM) are embedded in rural healthcare settings, having worked most of their careers in non-metropolitan areas. Interview recordings were reviewed periodically by the research team, and the interview guide was refined during the data collection process. Interviews were audio-recorded and subsequently transcribed by the second author (JGA) with participant consent. An interview guide (see supplementary online file) was used to facilitate the interviews. To minimise potential bias, power dynamics and assumptions, the interviewers (JGA and AJG) did not have direct relationships with the participants, unlike the first author (BKC). Data collection occurred until data sufficiency was reached, and in line with pragmatic resources considerations. 13 Data sufficiency depends both on the rigour of the analytical process (i.e. analytical sufficiency) and the richness of data it generates. This was demonstrated in this research through iteratively revising the interview guide, sampling new participants, and engaging in multiple rounds of data generation and analysis. 13
Data analysis
Transcribed and de-identified data were analysed through a conventional inductive content analysis approach facilitating category development 14 by two researchers (PM and JGA) and validated by a third researcher (BKC). This inductive approach required researchers to become familiar with the dataset and code data manually to generate categories, through multiple rounds. Regular discussions between the three researchers involved in the analysis process provided an opportunity to generate categories collectively and enabled researcher triangulation. Content analysis was chosen as it can be used on any type of written text and provides a range of approaches for researchers to use within this method, such as an inductive or deductive approach. 15
Trustworthiness
The researchers employed several strategies to ensure trustworthiness of this research through demonstration of credibility, dependability, transferability and confirmability. 15 Credibility was ensured by the provision of adequate descriptions of the data collection and analysis processes and by including all data in the analysis. The first author (BKC) obtained expert input and guidance from several experts in the field throughout the study. Three researchers engaged in the analysis process to undertake peer checking throughout the analysis process to ensure conformability. Dependability was ensured through keeping track of coding decisions, and engaging in regular discussions throughout the data collection and analysis process. While the transferability of the findings may be limited given the small sample size, participants represent several practice contexts and included both genders, thereby maximising the transferability of findings to other settings. Confirmability was ensured by the researchers being objective throughout the study process, declaring and discussing biases, and by taking a neutral stance to ensure that the participant voice is reflected in the findings. For this reason, the first author (BKC), who was known to some research participants, did not engage in data collection. The researchers acknowledged and worked through their different areas of expertise, subjective biases, methodological preferences and world views throughout the study, demonstrating reflexivity. 16
Results
We contacted 15 intensivists, of whom 13 provided consent and participated in an interview. Interviewees were from regional and rural centres in Queensland and the Northern Territory, with some also having locum experiences in regional and rural Tasmania and New South Wales. All but one interviewee lived in the regional/rural work location. Interview length ranged from 45 to 120 minutes and yielded over 14 hours of audio-recorded data. Ten participants were men, and three participants were women. Three intensivists worked 0.5 full-time equivalent (FTE) anaesthesia and 0.5 FTE intensive care medicine, while the other 10 were 1.0 FTE intensivists. Participants represented regional and rural ICUs from five Queensland, one Tasmanian, one New South Wales, and one Northern Territory centre(s). ICUs represented in this study were mostly in MMM2 sites, while one each was from an MMM3 and MMM6 site. 17 Participants varied in country of primary medical degree, years since fellowship with CICM, previous experience in a regional/rural area and amount of time in the current role. Further participant demographics are presented in Table 1.
Characteristics of study participants (n = 13).
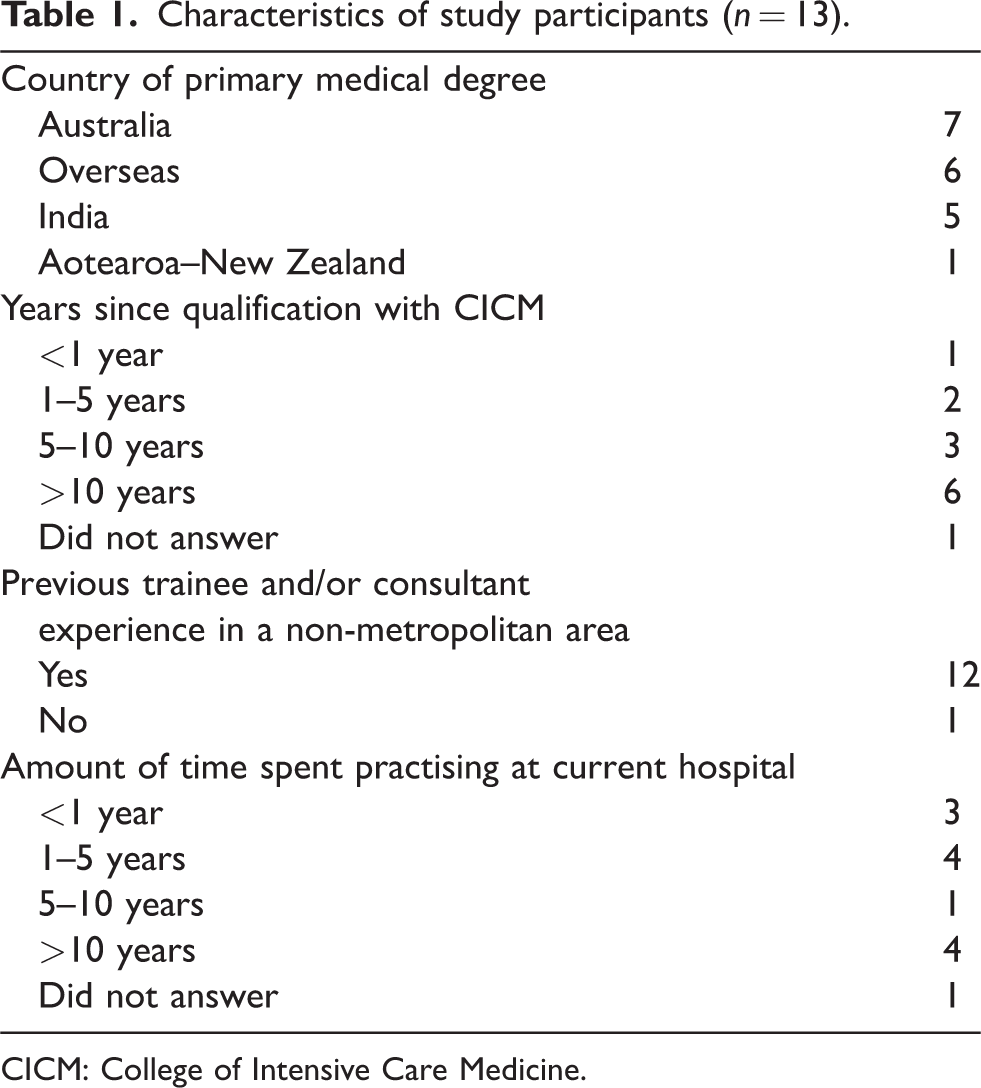
CICM: College of Intensive Care Medicine.
The content analysis of the interview data resulted in the development of the following categories: unique practice context, need for a generalist skill set, perks and challenges of working in a regional/rural area and workforce implications.
Unique practice context
Participants noted that working in regional and rural ICUs provided them with a unique practice context where they must work with the available resources and problem solve challenges to provide the best care. While they noted that immediate subspecialist teams in regional and rural areas are generally supportive, they highlighted perceived misperceptions of their metropolitan non-intensivist subspecialists about intensivists’ roles and contexts in regional and rural areas.
Resource constraints
Participants described significant resource limitations when working in regional and rural areas, particularly with respect to availability and access to subspecialist services and radiology. The available subspecialist support tends to be more junior and generalised in these regions. Some participants noted that resource limitations meant that they cannot provide the type of service they would like to: If a patient comes with a STEMI, and needs an urgent intervention, which might not be available in a regional hospital—what do you do? Do you ship the patient out? By the time the patient reaches the centre to get a PCI, they might not survive. (Interview 10) If there’s a patient that’s got a destination-defining injury, then I try and discuss it earlier with them (nearest metropolitan centre). And then also an extra bit of being uncomfortable sometimes and having to just bite the bullet and see what happens. (Interview 4)
Supportive work teams
Among their local subspecialist colleagues, participants noted a high degree of camaraderie, explaining that their surgical and medical colleagues were often willing to come in and provide support after hours: I’ve just had good experiences with being quite collegial and easy to get help from and everyone seems to get along because it’s a smaller pool of people. (Interview 4)
Perceived misperceptions of metropolitan colleagues
However, participants noted that their metropolitan colleagues did not truly understand medical practice in regional and rural hospitals and the role of intensivists in that context. While participants felt that metropolitan intensivists were usually understanding of the distinct capabilities of regional and rural ICUs, they felt that other metropolitan subspecialists were less aware: I think that basically, a lot of them, that is subspecialists, have not had enough rural experience or regional experience. They don’t really understand the challenge of what the regional centres are facing. Some of them are very supportive, but some of them are not particularly supportive. (Interview 9) The only thing that’s annoying is interacting with tertiary hospitals who just refuse to accept patients when they’re being asked to. Like okay, we can’t look after this patient here and we want you to take them because the patient needs to come. And they’re like, ‘oh no, we think you can cope with this‘. Like I’m ringing you and telling you that we can’t cope … (Interview 5)
Need for a generalist skill set
Participants unanimously noted that a regional and rural intensivist needs to be a jack of all trades to compensate for the smaller workforce and lack of subspecialists in these regions. Examples were provided where a regional and rural intensivist had to work at a broader scope of practice to manage patients in areas such as including advanced airway issues, paediatrics, obstetrics, retrieval medicine, telemedicine, echocardiography, temporary transvenous pacing, pericardiocentesis and outreach (Table 2). Being a generalist is deemed necessary for regional and rural intensivists:
Participant quotes to support ‘Category 2: Need for a generalist skill set’.
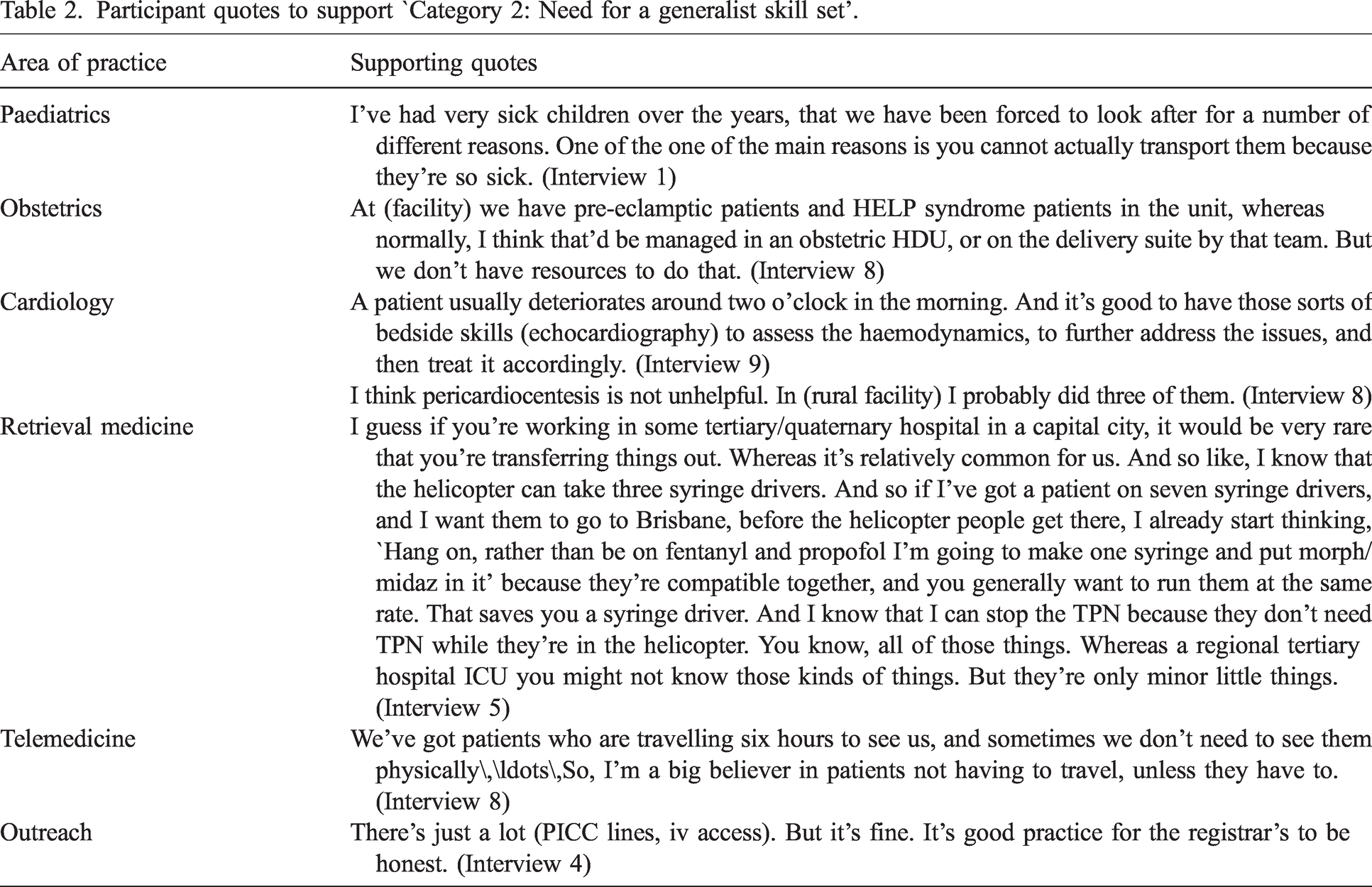
Regional practice is very challenging and as a regional intensivist, you need to be a bit of a generalist because whatever comes through the door, you can’t say that ‘I’m not qualified enough to handle this’. Whatever comes through the door, you just have to (handle). It can be a paediatric patient or an adult patient. It can be trauma. It can be anything. You just can’t say, ‘oh, we don’t have those specialties here. So, we can’t do neuro. We can’t do trauma.’ You just have to manage whatever we can with whatever limited resources you have. (Interview 10)
As a regional ICU specialist, you need a very broad experience. You need to know a little bit of everything, and you need to be pretty decent with your medicine and your anaesthetic skills. (Interview 9)
In addition, participants reported the need to possess sound problem-solving skills and adaptability to rise to challenges as an important non-technical skill, as this was seen as imperative to thriving in resource-constrained regional and rural areas.
Perks and challenges of working in a regional/rural area
Being based in a regional and rural hospital was said to come with its perks and challenges both for one’s career and personal life circumstances. Participants noted that the greatest perks included spending less time commuting to work and back, more time with family, housing affordability, options for primary and secondary education for their children, work satisfaction, and being embedded in a close-knit community.
One participant, while commenting on what works well for them in a regional hospital, said: (Managing a patient) over the phone is good, but I don’t do it. I live six minutes away from the hospital. I prefer to come in have a look—see what it really is. I satisfy myself and go back to bed and sleep a lot easier … (Interview 1) We love living in a town where you just get to know people. You meet them in the mall. You sort of live your life with them. (Interview 8) When we started, we were only three full time consultants. So, as you can imagine, the on calls were very frequent. So, you’re doing one in three weekends. (Interview 7) My work-life balance is terrible because I’m always on call. I’m on call a lot. So, I’m on call about 200 nights a year. (Interview 5) … people are obviously concerned about the amount of on-call when they are coming back from maternity leave with young kids. The fact that you might be called into a hospital quite a bit means that you do have to have a partner that will be able to cover those days. There is more buffer, I think, in a tertiary place. (Interview 13)
Workforce implications
Many participants noted that they had to work with a predominantly junior workforce which meant more support and mentoring needs: Junior cover is pretty inadequate, depending upon the case mix and the complexities. Often, what we’re getting is very junior staff who are not exposed to the severe illnesses. So, the understanding of their pathophysiology is limited. Often you have to support them to a very high extent. (Interview 6) … (accessing CPD) probably comes down to (the) ability to get leave or go away and because we have a smaller pool of intensivists, that can be trickier for lots of people to go at the same time. (Interview 8) … that’s why we’re only accredited for six months, because they have to go elsewhere to get the case mix. It’s reasonable. We’ve got sick complex patients obviously, but you simply couldn’t do five years of ICU training in (regional centre). There’s enough stuff that we don’t see and there’s not enough of it either. (Interview 5) The best thing is to finish off training in a tertiary centre where they are exposed to cardiothoracic and neurosurgical exposure before they sit the exam. But prior to that, getting used to all the less tertiary case mix and getting enough hands-on experience would be good in a regional centre. (Interview 7) … (recruiters) are more selective because … they are not necessarily wanting some complete outsider to get into their circle. (Interview 9)
Discussion
Our findings provide timely and relevant insight into experiences and perspectives of intensivists working in Australian regional and rural ICUs. Their perceptions on the unique practice context, need for a generalist skillset, perks and challenges of working in a regional/rural area, and workforce implications can inform government policies, hospitals, CICM, and ANZCA on strategies to improve intensive care service provision and training in regional and rural areas.
Regional and rural Australian healthcare settings were noted to be unique given the workforce and resource constraints. The resource constraints, including infrastructure such as radiology and human resource issues including the availability of subspecialists, were noted to be challenging. The current study also identified that workforce shortages negatively impacted teaching and research activities. This limitation could have an implication for the expansion of local medical school and postgraduate training opportunities in regional and rural areas. 18 In terms of workplace culture, this study found that immediate work teams, local subspecialists and metropolitan intensivist colleagues were largely supportive. However, metropolitan subspecialists were perceived to have inadequate understanding of the unique regional and rural ICU practice context. This in turn contributed to participants’ workplace stress, which can facilitate burnout among intensivists. 19 Previously ANZCA educators have advocated for a shared mindset between different subspecialists and a multidisciplinary focus during anaesthetic non-technical skills training. 20 Early involvement of supportive metropolitan intensivists during engagement with other metropolitan subspecialists, and opportunities for metropolitan subspecialists to experience non-metropolitan ICU practice, could help mitigate this issue. Metropolitan intensivists undertaking locum work in regional and rural areas can support intensive care medicine training in regional and rural areas, as well as meeting a service need in these communities.
This study validated the common perception that an extended scope of practice with a broad clinical and non-technical skill set is required for work in regional and rural ICUs. This finding highlights the importance of intensivists to self-identify potential learning gaps and proactively develop competencies during intensive care medicine training or upskilling as a consultant. For example, several options are available for intensivists to acquire advanced airway skills. 21 Findings can inform the design of a new combined ANZCA and CICM training curriculum and subsequent intensivists’ continuing professional development activities. Findings highlight the relevance of non-technical ICU skills such as adaptability and ability to rise to challenges, problem solving, teamwork, collaboration and communication. Such a multi-dimensional skill set is particularly essential for healthcare workers while working in regional and rural areas, as it allows them to think outside the box, rise to manage challenging clinical situations with resources at hand, and draw on the needed expertise among colleagues to enact service delivery.
Lifestyle considerations were highlighted as an important influence in deciding to live and work in a regional or rural centre. 22 A previous Queensland study of 32 early career doctors emphasised the importance of children’s education and partners’ career needs as some of the major non-professional needs influencing their decision to live and work outside metropolitan settings. 23 Another Australian study of junior doctors reinforced the importance of family considerations while deciding to pursue regional and rural practice. 24 Health services, employers, and communities all have a role to play in enabling work opportunities for partners, and schooling options for children, to address intensivist shortages in regional and rural areas. The increased on-call burden was noted as another deterrent to work in regional hospitals. This, if unattended, could further exacerbate burnout issues in this group, which can in turn be detrimental to workforce recruitment and retention. 25 Our study also highlighted perceived gender-based differences among intensivists, noting that the increased on-call burden does not cater to intensivists with parenting or caring responsibilities and those choosing part-time return to work following parental leave. While the proportion of female intensivists in this study was comparable to data reported by the critical care resources survey (i.e. 26.6%), 4 further research could specifically explore the role of gender in career choices for intensivists.
This study highlighted the importance of training time in a regional and rural hospital in gaining employment post-training in that location, highlighting the importance of the pipeline factors, which are rural background, and rural undergraduate and postgraduate training.26 –28 A recent tracking study of Australian medical graduates has illuminated the importance of postgraduate regional and rural hospital training time in attracting the workforce back to these regions. 29 Therefore, it is important to continue investment in making training opportunities available in regional and rural areas for those training to be intensivists. A combination of metropolitan, regional and rural training time could be beneficial for intensivist trainees.
Working with a predominantly junior workforce in regional and rural areas was noted as a significant barrier as it meant increased support and mentoring provision to this workforce. This challenge is reflective of the overall workforce challenges experienced outside larger metropolitan centres. 30 CICM, ANZCA and hospitals may need to attract more senior trainees, especially those with previous regional and rural working experience. In addition, a recent Australian survey of trainees and unit directors reported that the CICM’s training and credentialling programme may not always equip the newly trained intensivists with the comprehensive skill set required for safe, independent consultant practice. 31 The recent recommendation by the ANZCA Council in 2021 to develop a dual anaesthesia and intensive care training pathway in collaboration with the CICM can help to address the unmet needs of regional and rural communities. CICM also extended the mandatory regional and rural exposure time from 3 to 6 months in 2023; a step forward to address regional and rural intensivist shortages and training issues.6,32 The Western Australian Intensive Care Training Program (WAICTP) is an alternative networked training pathway commencing in 2024 to facilitate the placement of trainees in regional and rural training positions. The WAICTP initially received seed funding through a successful Commonwealth flexible approach to training in expanded settings (FATES) grant application from the West Australian State Committee and CICM, and now has ongoing funding through partnership with the West Australian Country Health Service, which facilitates training rotation allocation to gain a wide range of experiences in different hospital settings. 33
By capturing experiences of full-time, part-time, and locum intensivists across eight Australian regional and rural hospitals, and through in-depth interviews, the data collected were comprehensive and sufficient to enable the development of meaningful findings. Future research could expand this qualitative study in Aotearoa–New Zealand, as well as survey regional and rural intensivists in both Australia and Aotearoa–New Zealand to strengthen the evidence base in this area. Future research can further explore gender-based differences in intensive medicine and its role in workforce supply in regional and rural areas.
Conclusion
Regional and rural hospital intensivists described their unique practice context, need for a generalist skill set, perks and challenges of working in regional/rural centres, and workforce implications. The main finding was that while practising in regional and rural areas has its challenges, there are also numerous benefits and lifestyle rewards. To ensure the delivery of high-quality intensive care medicine services and maintain a sustainable workforce outside metropolitan areas, careful planning and collaboration are essential among governments, hospitals, CICM, and ANZCA. The findings of this study can inform such efforts.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) thank all the participants. They also thank Jacqueline Tunnecliff, Amelia Martin, Shalia Chavan, Associate Professor Bruce Lister and Dr Wallace Grimmett for their feedback on the final draft of the manuscript. They would also like to thank Ms Kaye Cumming for librarian support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.