
Abstract
Summary
A vascular introducer sheath is often used for rapid volume replacement. However, common manipulations such as the addition of needleless connectors to infusion ports and the insertion of catheters or other devices through the introducer sheath may impede flow. In this study we utilised a rapid infuser to deliver room-temperature normal saline through two introducer sheath configurations with and without the addition of needleless connectors and the placement of catheters through the introducer sheaths. The maximal flow rate delivered by the rapid infuser was 1000 mL/min, which was observed with both introducer sheath sizes tested without additional resistive elements. However, with the addition of a needleless connector, flow rates through the introducer sheaths were substantially lower (64 (standard deviation (SD) 6) mL/min and 61 (SD 7) mL/min for the 8.5 Fr and 9 Fr introducers, respectively). Flow rates were also reduced when catheters were placed within the sheaths (298 (SD 9) mL/min with the 7 Fr catheter and 74 (SD 9) mL/min with the 8 Fr catheter placed in an 8.5 Fr sheath; 649 (SD 6) mL/min with the 7 Fr catheter and 356 (SD 14) mL/min with the 8 Fr catheter placed in the 9 Fr sheath). These findings indicated that both needleless connectors and the placement of catheters through vascular introducer sheaths substantially reduced potential flow rates. Even ‘large’ vascular introducer sheaths capable of delivering high flow rates could be rendered minimally effective for rapid fluid administration when used in this way. Clinicians should consider these impediments to flow when rapid fluid administration is required, and obtain alternative vascular access if necessary.
Keywords
Introduction
Vascular introducer sheaths are used to provide access for the insertion of other catheters (e.g. pulmonary artery catheters) or other vascular devices. Due to their large lumen they can also be used for rapid fluid administration. However, there are many variables that can influence flow rates through introducer sheaths1,2 including the use of needleless connectors, and utilising the sheaths for the insertion of other catheters which reduces their free lumen size.3 –5
Unfortunately, it is not possible to make theoretical predictions about flow rates in intravenous (IV) systems due to the complexity of the tubing, connectors, and distal pressures. Moreover, experimental measurements of flow rates through vascular access devices and IV systems are found to deviate from those predicted using the Hagen–Poiseuille equation or Reynolds number.6 –9 In particular, experimental data flow rates from vascular access devices do not vary with the fourth power of the radius,6,7 and it is unlikely that clinical IV systems would have properties such as uniform laminar flow. Although previous studies have compared the flow rates of different types of venous access devices,2,4,10 –14 the effect of needleless connectors and inserted catheters on flow through vascular introducer sheaths has not been previously investigated. Therefore, we undertook an equipment study to measure flow rates in a similar manner to previous investigations, but focused on the influence of needleless connectors and catheter insertion through vascular introducer sheaths. Our hypothesis was that these interventions would both significantly reduce flow rates; a finding that would inform flow rate expectations and facilitate appropriate choices regarding vascular access components when using vascular introducer sheaths.
Materials and methods
A Belmont® Rapid Infuser (Belmont Medical Technologies, Billerica, MA, USA) was used to generate up to 300 mmHg of driving pressure to deliver room-temperature normal saline through different vascular introducer sheath configurations. The investigation was an equipment study with fluid delivery to an open container; no humans or animals were included in the experiments. Consistent with the manufacturer’s design, the maximal flow rate produced by the rapid infuser without any other devices attached was 1000 mL/min. In this study, flow rates reported below 1000 mL/min reflect flow that is pressure-limited at approximately 300 mmHg.
A systematic assessment of flow rates was undertaken with an Arrow® 8.5 Fr introducer sheath (Teleflex Incorporated, Wayne, PA, USA) and an Arrow 9 Fr multi-lumen access catheter (MAC) with or without additional elements. These are the two vascular introducer sheaths used at our institution. The term ‘side arm’ is used to describe the channel of these devices emptying directly into the introducer sheath. Whereas the introducer port can be indirectly used for volume delivery via catheters inserted into the main lumen, fluids cannot be directly administered through the introducer port. This is in contrast to the side arms, which are intended for fluid delivery only. The additional elements were the One-Link Needle-Free IV Connector (Baxter, Deerfield, IL, USA), an Arrow 7 Fr triple lumen central venous catheter and an 8 Fr continuous cardiac output pulmonary artery catheter (PAC) (Edwards Lifesciences; Irvine, CA, USA). The experiments are summarised in Table 1.
Flow rates through vascular introducer sheaths measured with different resistive variables.
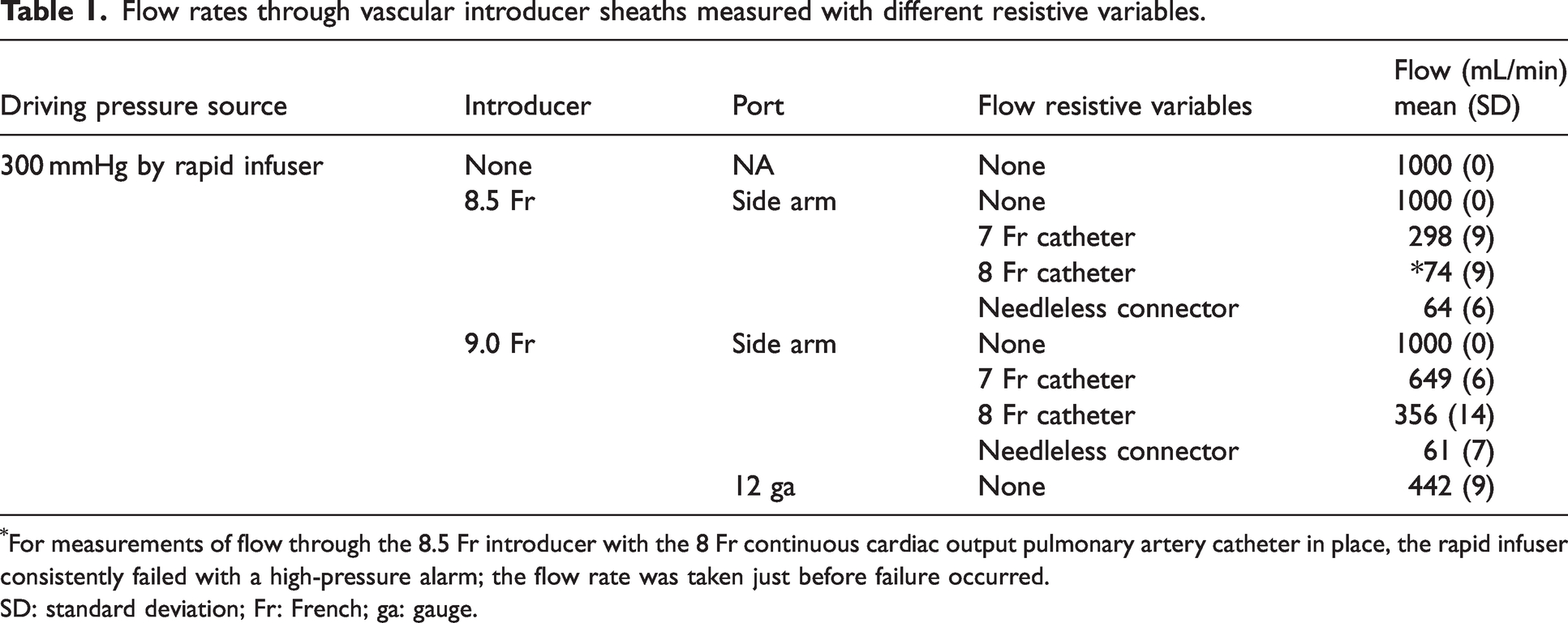
For measurements of flow through the 8.5 Fr introducer with the 8 Fr continuous cardiac output pulmonary artery catheter in place, the rapid infuser consistently failed with a high-pressure alarm; the flow rate was taken just before failure occurred.
SD: standard deviation; Fr: French; ga: gauge.
The primary outcomes were the comparison of 1) the flow rates through the side arms of the introducer sheaths without and with a needleless connector and 2) the flow rates through the side arm of the introducer sheaths without and with a device inserted via the introducer port. The flow rate and driving pressure were measured 10 times with the addition of each device, and the mean (standard deviation (SD)) was collected to indicate measurement error and not biological variation. Driving pressure was monitored to ensure a constant 300 mmHg was being generated to avoid false low measurements.
Results
The flow rates in all configurations are shown in Figure 1 and Table 1. Flow through both the 8.5 Fr and 9 Fr introducer sheaths alone consistently reached the maximal possible flow rate of 1000 mL/min. Lower flow rates through the side arms were observed with the 8 Fr catheter compared to the 7 Fr catheter inserted into the 8.5 Fr introducer sheath port (74 (SD 9) mL/min and 298 (SD 9) mL/min, respectively) and the 9 Fr introducer sheath port (356 (SD 14) mL/min and 649 (SD 6) mL/min, respectively). The 12 ga side arm of the 9 Fr MAC introducer sheath, which is separate from the main channel, flowed better than the 9 Fr side arm when an 8 Fr catheter was inserted (442 (SD 9) mL/min and 356 (SD 14) mL/min, respectively). Notably, the rapid infuser consistently failed while displaying a high-pressure alarm shortly after flow through the 8.5 Fr introducer with the 8 Fr PAC inserted was attempted; the reported measurements were taken prior to failure.
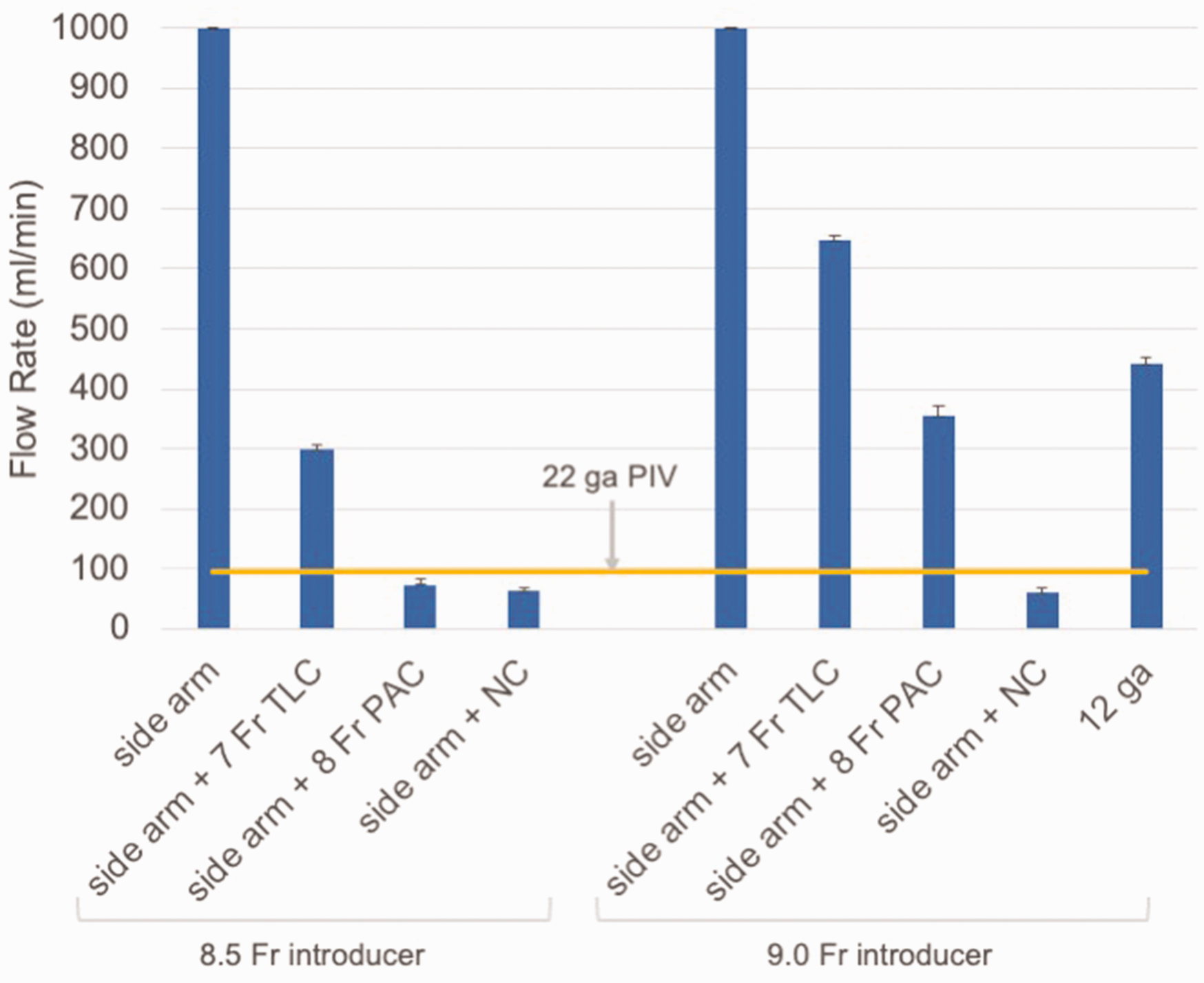
Flow rates through vascular introducer sheaths. Bars denote mean flow rate in mL/min (SD). For comparison, the flow rate of a 22 ga peripheral intravenous catheter is shown, measured using the same method as with the introducers without needleless connectors or additional catheters (unpublished observation).
Flow rates were also greatly reduced whenever a needleless connector was added to the infusion port (64 (SD 6) mL/min and 61 (SD 7) mL/min for the 8.5 Fr and 9 Fr introducers, respectively). To further illustrate the extent to which flow was impacted, the resultant flow with the trial using a needleless connector and the 8.5 Fr introducer with an 8 Fr PAC inserted was less than that of a 22 ga peripheral IV catheter, measured at 94 (SD 4) mL/min (unpublished observation).
Discussion
This study demonstrated that the addition of a needleless connector or placement of a central venous catheter or PAC into a vascular introducer sheath dramatically decreased flow rates and thus utility for rapid fluid administration. It is intuitive that placement of a separate device such as a PAC through the lumen of an introducer will decrease flow, but perhaps what is surprising is the magnitude of the effect. With either the addition of a needleless connector or placement of the 8 Fr continuous cardiac output PAC into the 8.5 Fr introducer, flow rates were below that of a 22 ga peripheral IV catheter.
This study’s findings are consistent with previous investigations.2,4,10 –14 Per the manufacturer specifications for the 9 Fr MAC introducer sheath, flow rates achieved using gravity at 100 cm of bag height were 29,920 mL/h with no inserted catheters, 19,810 mL/h with a 7 Fr catheter inserted, and 12,180 mL/h with an 8 Fr catheter inserted. Thus, the decrement in flow with the insertion of 7 Fr and 8 Fr catheters, relative to unobstructed flow, observed in our study using a rapid infuser was comparably similar to that reported by the manufacturer with gravity (35% versus 34% and 65% versus 59%, respectively).
The findings of this report and others2 –4,11,13,14 support the temporary removal of needleless connectors as a simple and highly effective manoeuvre to increase the capacity for rapid fluid administration. Temporarily removing needleless connectors from vascular introducers can dramatically increase the flow rates during pivotal moments of fluid resuscitation and massive transfusion. A sterile technique should be used whenever needleless connectors are temporarily removed or replaced.
This study has several limitations. It is a bench study with flow rate measurements obtained under idealised conditions, most notably in the absence of a patient. As such, the reported results are unlikely to be achieved in clinical practice. However, the presented findings can be considered as an upper bound with these manipulations of the IV system, as clinical flow rates will not be higher. Given that only crystalloid was used, the flow rates do not apply to fluids with a higher viscosity, particularly red blood cell transfusions. Lehn et al. previously demonstrated that the magnitude of flow decrease can be greater than 50% when red blood cells are infused compared to crystalloid, with even more profound fractional decreases in flow observed when needleless connectors were used. 11 Pressurised administration of fluids with a rapid infuser is performed in only the minority of clinical cases. However, this configuration has the experimental advantage of a constant stimulus for measurements and is the configuration often used when rapid fluid resuscitation and massive transfusion is necessary. Although the study was an investigation of the equipment available in our health system, there are other manufacturers, introducer sheath models, and numerous other needleless connectors available.2,3,11 While the presented results apply only to the equipment tested, they are likely to be representative of similar sheaths and devices. The authors recommend that clinicians consider the impact of these impediments to flow in their own practice and if necessary, undertake measurements of flow rates through their own systems.
This study demonstrated that both needleless connectors and catheters inserted into introducer sheaths significantly restricted flow. Even ‘large’ vascular introducer sheaths capable of delivering the maximal flow rate with a rapid infuser could be rendered minimally effective when used in this way. Clinicians should consider these impediments to flow when rapid fluid administration is required and obtain alternative vascular access if necessary.