
Abstract

Central venous cannulation is a core technical skill in anaesthesia and critical care medicine. It is vital in those patients in whom peripheral venous cannulation cannot be achieved or is unsuitable. The right internal jugular vein (RIJV) is a common site of central venous catheter (CVC) insertion. The use of procedural ultrasound to assist in vessel identification during catheterisation of the RIJV was first systematically described in 1984
1
and is now commonplace, although not universal.2,3 Although use of ultrasound is recommended, knowledge and teaching of the landmark technique remains important. According to the latest National Institute for Health and Care Excellence (NICE) guidance, last updated in 2016, the landmark method would remain important in some circumstances, such as emergency situations, when ultrasound equipment and/or expertise might not be immediately available. Consequently, the Committee thought it important that operators maintain their ability to use the landmark method and that the method continues to be taught alongside the 2-D-ultrasound-guided technique.
4
The study was approved by the University of Nottingham FHMS Research Ethics Committee on 25 May 2022 (reference: FMHS 11-0422). Inclusion criteria were anaesthetic or critical care staff, of any grade and/or experience, expected to be able to perform CVC insertion in the course of their routine clinical duties. If in a postgraduate training post, individuals were required to meet the recommendations of the Royal College of Anaesthetists, UK, 2021 curriculum. Those who did not meet the above criteria were excluded, including medical and non-medical staff in clinical specialities outside anaesthesia or critical care. The study was conducted at Nottingham University Hospitals NHS Trust—a 1700 bed academic health centre providing anaesthesia for all major surgical specialities.
Invitations for voluntary study participation were distributed via routine organisational electronic mailing lists. After eligibility assessment, informed written consent was obtained for study enrolment. Participants completed a questionnaire on their current role within anaesthesia and/or critical care, past experience of CVC insertions and current preferred CVC insertion techniques (Table 1). Participants were then invited to position a healthy volunteer for insertion of a right internal jugular CVC. The volunteer had normal neck vascular sonoanatomy, with the internal jugular vein lying antero-lateral to the carotid artery at the level of the cricoid cartilage. This was confirmed prior to the study by an investigator (DWH). The same volunteer was used for all participants. After choosing how to position the volunteer, participants were asked to identify the point on the volunteer’s skin through which they would insert a phantom needle/cannula, as if they were to perform a landmark-guided guidewire technique RIJV CVC insertion. When satisfied, a high-frequency linear array ultrasound transducer with the mid-point labelled was used by participants to correspond to the desired phantom needle insertion point and trajectory to cannulate the anticipated RIJV. The screen of the ultrasound machine was concealed from both participant and volunteer and frozen by a study investor. Images were exported for later analysis by a blinded investigator.
Experience and current activity of participants in insertion of right internal jugular central venous catheters.
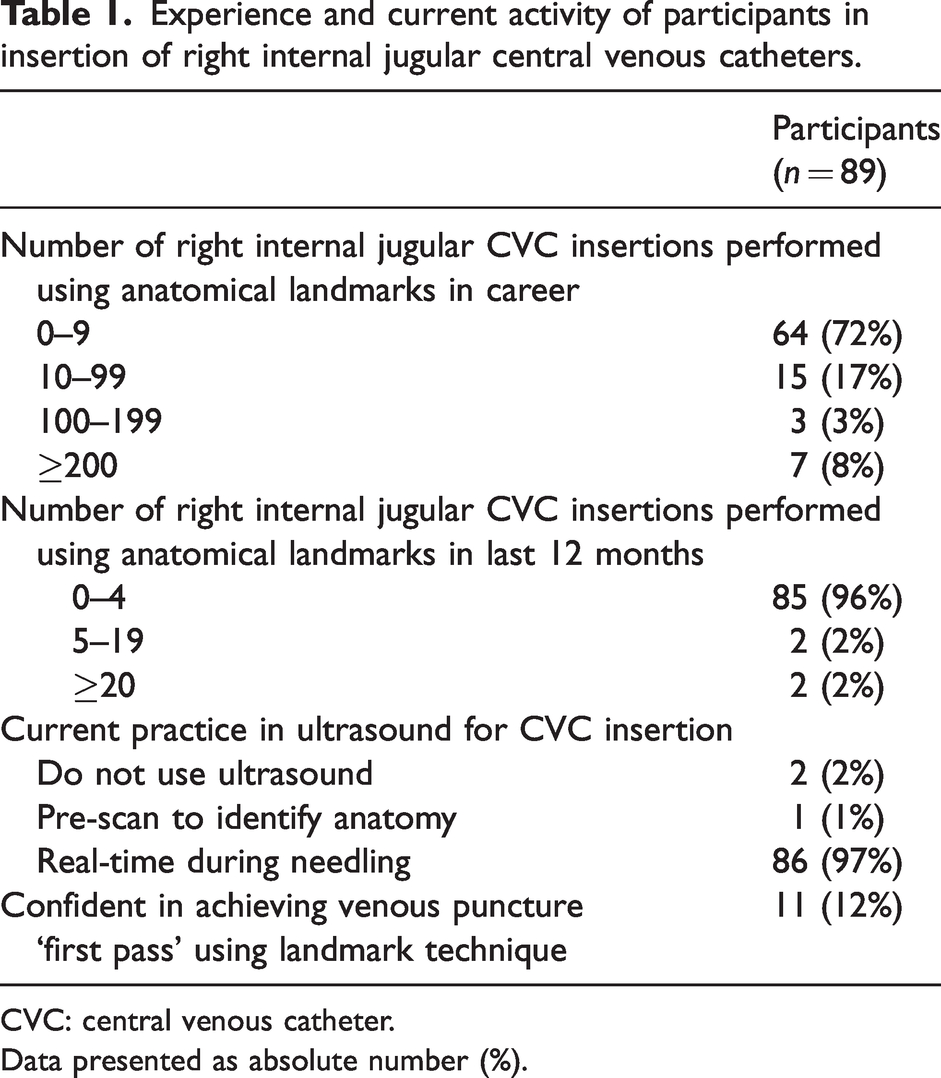
CVC: central venous catheter.
Data presented as absolute number (%).
The statistical analysis was performed according to a prespecified analysis plan. Continuous data were presented as mean and 95% confidence interval (CI), or median and interquartile range (IQR) if not normally distributed. Binary data were presented as absolute number and frequency (%). All analyses were performed using SPSS version 26 (IBM Corp., NY, USA).
The study was performed between 29 June 2022 and 20 February 2023. There were 89 participants, (26 consultants, two speciality or specialist grade doctors with at least 4 years of postgraduate training, 60 trainees, and one anaesthesia associate). Only two participants used a landmark technique on a routine basis (i.e. ≥20 insertions per year) (Table 1).
The proportion of clinicians whose phantom needle insertion point and trajectory intersected the RIJV was 50/89 (56%). However, the proportion of phantom needle trajectories that would have resulted in a carotid puncture was 16/89 (18%) (Table 2).
Ability of participants to identify needle insertion point and trajectory to intersect the right internal jugular vein.
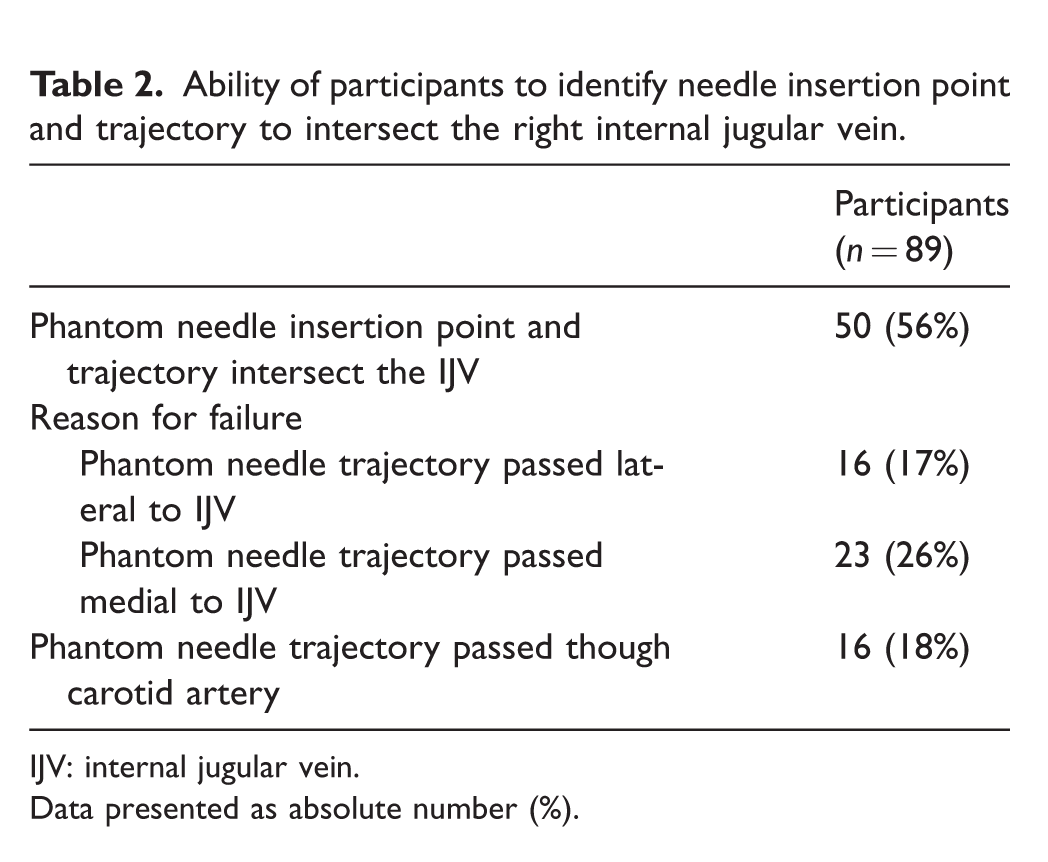
IJV: internal jugular vein.
Data presented as absolute number (%).
In comparison to a similar study in 2009, 6 the confidence and routine practice of clinicians using a landmark technique for CVCs was lower. The number of phantom needle carotid artery punctures was higher (16/89 (18%) vs 6/85 (7%); P = 0.039), but the proportion of clinicians able to intersect the RIJV with a phantom needle between the current and the previous study was broadly similar (50/89 (56%) vs 42/85 (49%); P = 0.448).
Given the low correct phantom needle insertion point and trajectory for RIJV cannulation in this study (56%) and the wide availability of ultrasound equipment in anaesthetic practice in the UK, 7 the findings of this study do not support the use of a landmark technique, particularly by inexperienced clinicians. Indeed, the increased incidence of potential carotid puncture from our study was notable and cautions against the use of the landmark technique, even in emergency situations. In the case of an emergency without access to ultrasound equipment, it may be preferable for other supportive measures and patient transfer to a facility where ultrasound equipment is available rather than attempting a landmark technique for RIJV CVC insertion.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.