
Abstract

Lung isolation and one lung ventilation (OLV) represent the cornerstone of anaesthesia for thoracic surgery. In most situations, a double-lumen endotracheal tube (DLT) is the preferred airway device. However, in certain situations where a DLT is not appropriate or otherwise problematic to insert, such as a difficult upper airway or abnormal tracheobronchial anatomy, a bronchial blocker can be used with a single-lumen endotracheal tube (ETT). 1 The bronchial blocker is typically advanced co-axially within the lumen of a standard ETT, and a flexible bronchoscope advanced, also within the lumen, to facilitate positioning of the distal portion of the bronchial blocker within the right or left mainstem bronchus as required under vision.
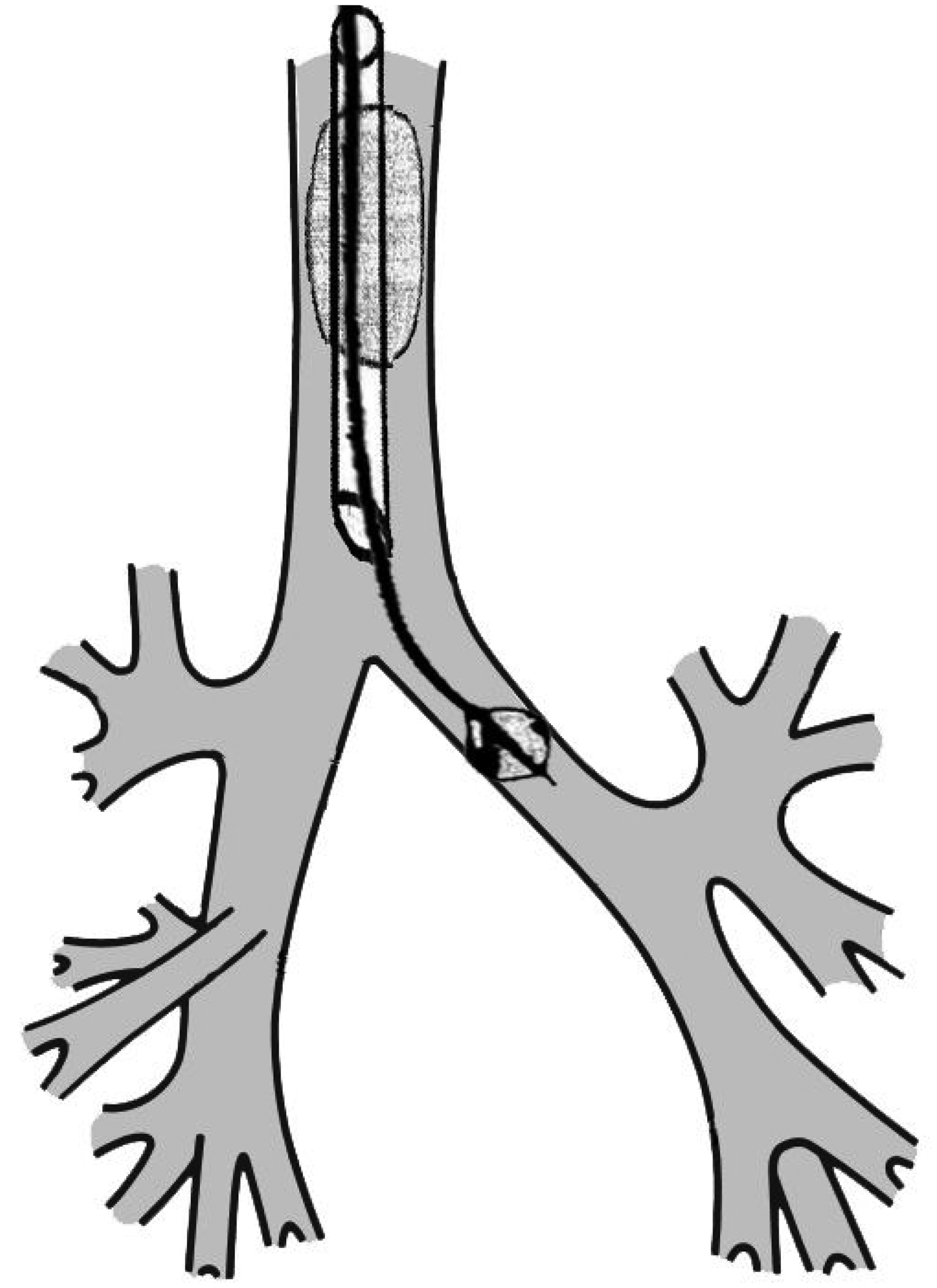
Co-axial position of a bronchial blocker within the lumen of an endotracheal tube.
Bronchial blockers were not always co-axial devices. The modern practice of bronchial blockade dates to 1981, when Ginsberg described the off-label use of the Fogarty embolectomy catheter (Baxter Healthcare Corporation, Santa Ana, CA, USA) as an alternative to the DLT for lung isolation. 2 Placement involved initial intubation through the vocal cords with the embolectomy catheter followed by parallel or ‘side-by-side’ intubation with a single lumen ETT. A bronchoscope was then passed down the lumen of the ETT and the embolectomy catheter positioned under vision into the appropriate main bronchus.
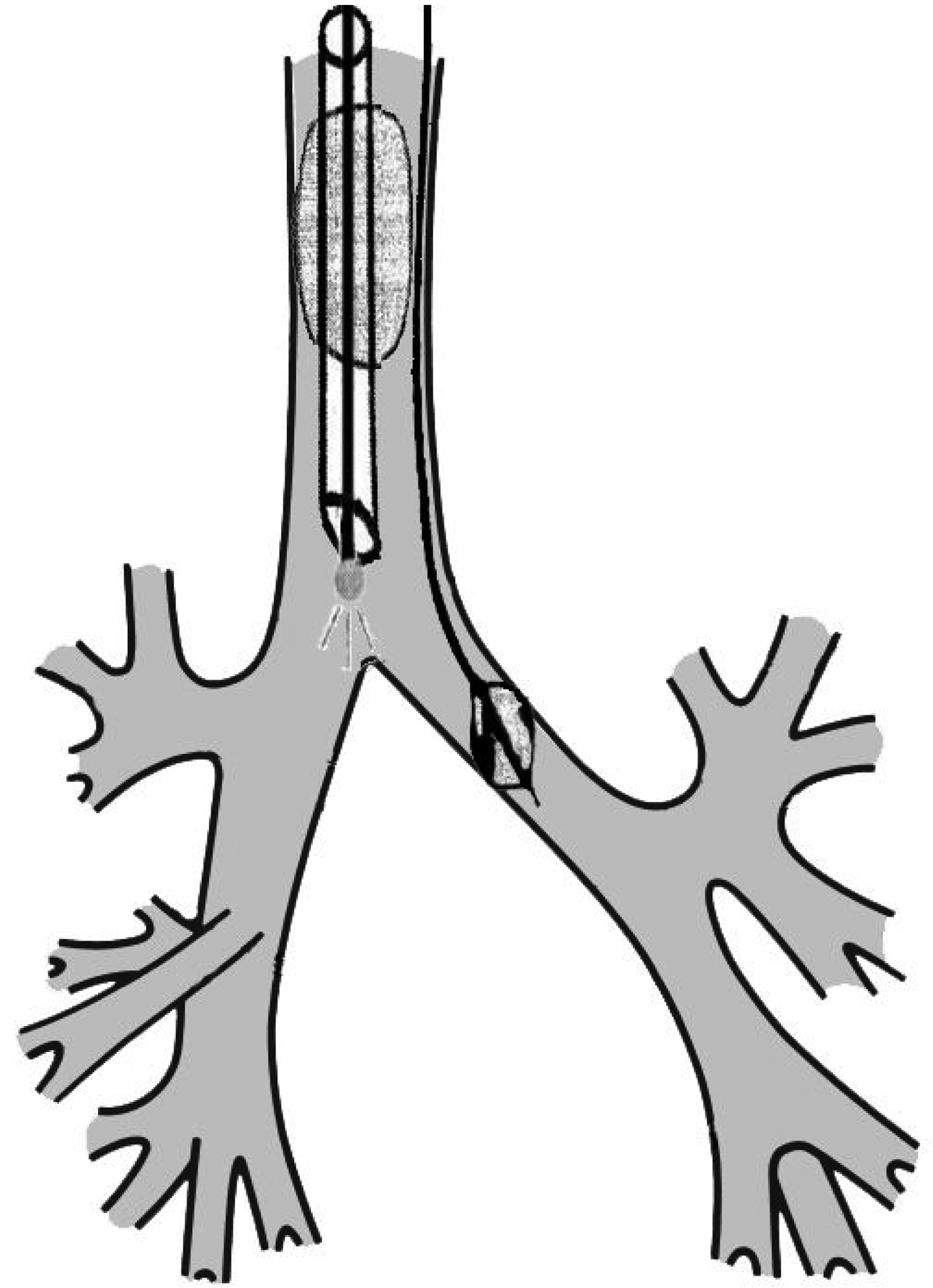
‘Side-by-side’ position of bronchial blocker with bronchoscope in the lumen of an endotracheal tube.
In 1999, the Arndt endobronchial blocker (Cook Medical Inc., Bloomington, IN, USA) became available. 3 This device was specifically designed for airway use, and featured a blocker balloon with favourable pressure-volume characteristics and a multi-orifice connector for attaching a single lumen ETT to the breathing circuit that facilitated the passage of the endobronchial blocker and the bronchoscope within the lumen of the ETT. Several other blockers have since been introduced, all of which feature a similar multi-orifice airway connector designed for co-axial placement of the blocker via the ETT.
At present, the technique of ‘side-by-side’ blocker placement has generally become almost obsolete in adult anaesthesia, although it may still have a role in very small children. We wish to report the case of an adult patient with tracheomalacia and sub-glottic stenosis, in whom a 5.5 mm single lumen ETT and bronchial blocker were used ‘side-by-side’ because co-axial insertion was not possible. Satisfactory operating conditions were obtained and there was a successful surgical outcome. Patient consent was obtained for the preparation and publication of this case report.
A 64-year-old woman with biopsy confirmed left lower lobe adenocarcinoma presented for a video-assisted thoracoscopic left lower lobectomy and lymph node dissection. The patient had been involved in a motor vehicle accident in the 1980 s, which resulted in a lengthy intensive care unit (ICU) admission and a temporary tracheostomy. She had subsequently had a nephrectomy in the early 2010 s during which bag-mask ventilation was documented as straightforward, and a Cormack–Lehane grade 1 airway was obtained with direct laryngoscopy. Intubation, however, had been difficult. Both size 7.0 mm (internal diameter) and size 6.0 mm ETTs could not be advanced into the trachea. A size 5.5 mm ETT was eventually introduced and reported to be ‘tight’. The case proceeded uneventfully and the patient was extubated successfully at the end of the procedure.
On preoperative assessment, the patient reported mild dyspnoea on exertion but no stridor. Her dyspnoea was longstanding and was felt to be related to her long smoking history. Her cardiovascular and respiratory examinations were unremarkable and routine spirometry was normal. Her airway was assessed as Mallampati grade 2. A narrowing of the subglottic trachea to 7.4 mm in diameter was confirmed on her most recent computed tomography scan.
The outer diameter of a 5.5 ETT is 7.5 mm. The smallest DLT commonly used at our institution (35 French Shiley Endobronchial Tube, Covidien, Mansfield, MA, USA) has an outer diameter of 11.7 mm and the less commonly used 32 French size has an outer diameter of 10.6 mm—still much larger than a size 9.0 ETT. With this in mind, the use of a DLT was considered not possible and lung isolation/OLV with a standard ETT and bronchial blocker was provisionally planned. However, this was made difficult by the requirement for a small (5.5 mm) ETT. Our smallest bronchial blocker (7 French/2.3 mm outer diameter; Hangzhou Tappa, Hangzhou, China) would not fit within the lumen of a 5.5 mm (internal diameter) ETT alongside our smallest bronchoscope (Ambu aScope Slim 3.8 mm outer diameter; Ambu A/S, Ballerup, Denmark). For this reason we planned for side-by-side positioning of the ETT and bronchial blocker.
General anaesthesia was induced with a propofol bolus and maintained with sevoflurane in oxygen and a remifentanil infusion, following which bag-mask ventilation was confirmed to be possible. In discussion with our surgeon, we then placed a laryngeal mask (LM, iGel size 4; Intersurgical Ltd., Berkshire, UK), through which a bronchoscope could be introduced to visualise the glottic opening and proximal trachea. Ventilation was managed with intermittent manual positive pressure ventilation until the return of spontaneous ventilation, which was maintained during bronchoscopy. The bronchoscopy revealed evidence of tracheomalacia and confirmed the presence of subglottic stenosis. The LM was then removed, bag-mask ventilation recommenced, and neuromuscular blockade was established with rocuronium. A grade 1 laryngoscopic view was obtained using a videolaryngoscope. A size 7 French bronchial blocker (see above) was then inserted into the glottis under direct laryngoscopic vision and advanced into the trachea. While maintaining the laryngoscopic view, a size 5.5 ETT was introduced—albeit tightly—alongside the bronchial blocker into the trachea. The ETT cuff was then inflated, and satisfactory ventilation was confirmed both clinically and by capnography. The bronchoscope was then introduced through the lumen of the ETT. The cuff of the ETT was temporarily deflated while the bronchial blocker was manipulated into a satisfactory position within the left main bronchus. The ETT cuff was then reinflated and lung isolation/OLV was possible. The surgeon reported good operating conditions and the left lower lobe was resected uneventfully. At the conclusion of the case the bronchial blocker cuff was deflated and the left lung reinflated. The patient was extubated without incident and her recovery was uncomplicated.
Using a bronchial blocker ‘side-by-side’ with an ETT is not a new technique, but it is one with which the occasional thoracic anaesthetist may be less familiar. The utility of this technique in paediatric patients, in which the requirement for smaller ETTs is more widespread, is well documented.4 –6 One previous study comparing ‘extraluminal’ versus intraluminal bronchial blockers also suggested that positioning a bronchial blocker ‘extraluminally’ may also make achieving OLV easier in some adult patients compared with conventional intraluminal use. 7 While we are not recommending routine side-by-side placement of bronchial blockers, we suggest that in a scenario which mandates a smaller ETT, this is a worthwhile technique to consider.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.