
Abstract
Nitrous oxide is a potent greenhouse gas and ozone-depleting agent with a long atmospheric lifetime. Several previous reports indicate that over half of supplied nitrous oxide is wasted from leaking manifold-pipeline systems infrastructure prior to patient use, and that remediating leaks can have significant environmental benefits. We describe an accurate, simple and cost-effective cylinder weighing method to quantify nitrous oxide leak from the manifold-pipeline network at our tertiary non-obstetric facility. Nitrous oxide cylinder depletion was prospectively compared with clinical usage derived from the electronic medical record over an 18-day period. A total of 1932 l (3.62 kg) of nitrous oxide was used in 35 operating theatre cases during the period. This was only 16.5% of actual cylinder depletion (11,686 l; 21.88 kg), indicating that 83.5% (9754 l; 18.26 kg) of nitrous oxide had leaked to the atmosphere (376 ml/minute; 22.6 l/hour; 542 l/day). The fraction of nitrous oxide wasted was consistent with a retrospective analysis of the previous 2-year period at the site that compared purchasing records with estimated clinical use. If maintained over a year, the leak would be equivalent to 101 tonnes of carbon dioxide per annum.
Keywords
Nitrous oxide (N2O) is a potent greenhouse gas, accounting for 75–90% of the total carbon footprint of inhaled anaesthetic agents.1 –3 Studies from the UK, Ireland, Australia and New Zealand have consistently reported 75–95% N2O wastage from leaking hospital pipeline manifold N2O systems.3 –6 At our own institution, retrospective comparison of N2O cylinder purchasing records with estimated clinical usage derived from the electronic medical record (EMR) over a 2-year period indicated approximately 80% wastage of N2O. Our objective was to quantify N2O leakage accurately at the site. We designed a weighing method so that N2O cylinder depletion could be prospectively compared with EMR-derived clinical usage in the operating suite.
Materials and methods
The Alfred Hospital is a large, tertiary, non-obstetric teaching centre in Melbourne, Australia providing state-wide trauma, burns and cardiothoracic transplant services. Reticulated N2O is supplied at 400 kPa from a 2 × 4 ‘G’ sized cylinder manifold to 48 wall outlets by way of pipelines. Wall outlet valves and seals are serviced every 2 years according to Australian standards 7 but the pipelines themselves are not routinely maintained and no pipeline map exists for the site.
After multidisciplinary consultation (e.g. engineering, external contractors) at an early stage, we designed a cylinder weighing method for the N2O manifold to compare N2O depletion with clinical usage over an 18-day period of reduced clinical activity between December 2022 and January 2023. According to the calculator supplied by the medical gas supplier, 8 the mass of N2O gas at atmospheric pressure (15°C) is 1.8724 kg per 1000 l. Consumption of N2O was measured by converting the manifold to a single live ‘G’ sized cylinder set on 150 kg industrial scales (Correct Weight Scales Pty Ltd.) with a sensitivity of 10 g (Figure 1). The tare (empty) weight of the ‘G’ sized cylinder was 50.5 kg. Pliable spiral copper cylinder connecting leads attaching the cylinder yoke to the manifold were manipulated into a neutral position by a trained technician so that it did not influence the weight of the cylinder by more than 10 g. Using a video camera (Eufy 4G Starlight camera) viewed remotely, the digitally displayed gross weight of the cylinder was recorded every 12 hours.

Single ‘G’ sized nitrous oxide cylinder mounted on an industrial 150 kg scale with continuous display viewable by a wireless 4G camera.
All anaesthesia machine (GE Aisys, GE Healthcare, Chicago, IL, USA) cumulative gas usage meters (kilolitres) were reset to zero. The EMR was interrogated to identify each episode of care when N2O was used in the operating suite including case identifier, date, anaesthesia provider, maintenance fraction of inspired nitrous oxide (FiN2O) and case duration in minutes. Using these data, two of the investigators (SJG, VXC) independently calculated the clinical usage of N2O in litres over the 18-day period. Fresh gas flows (FGFs) are not recorded on our EMR system. Where FGF rates were not available from the anaesthesia provider, we assumed FGFs of 5 l/minute for the first 7.5 minutes and 1 l/minute subsequently. Because we are reporting an investigation of site infrastructure leaks, ethics approval was not required.
Results
Prior to undertaking the cylinder weighing analysis we reviewed purchasing records and clinical usage of N2O for the previous 2-year period. From October 2020 to September 2022, 58 ‘G’ sized cylinders were purchased with a usable volume of 980,200 l N2O (29 cylinders or 490,100 l per annum). Comparison with EMR-derived data indicated approximately 80% wastage of nitrous oxide from infrastructure leaks. Interestingly, the proportion of anaesthesia cases utilising N2O decreased from 18% to 4% between 2015 and 2021.
Prospective cylinder weighing analysis
The starting weight of the ‘G’ sized cylinder was 82.38 kg indicating contents of 31.88 kg N2O (17,026 l) and the final weight of the cylinder was 60.50 kg (5340 l N2O remaining). Cylinder depletion was 21.88 kg (11,686 l) of N2O over 18 days. N2O was utilised in 35 theatre cases during this period for a total of 2127 minutes (mean 60.7 minutes/case). There was no reported usage in the emergency department. Mean clinical usage of N2O calculated by the investigators was 1932 l (range 1736–2127 l). This was 16.5% of the actual N2O cylinder depletion indicating that 83.5% of N2O (9754 l; 18.26 kg) was leaked to the atmosphere over 18 days (376 ml/minute; 22.6 l/hour; 542 l/day). We observed a stable decrement in N2O cylinder weight of 0.96 kg per 24 hours during periods with no N2O usage (Figure 2). At the end of the 18-day period, a zero-kilolitre reading was displayed on all GE Aisys anaesthesia machine N2O gas meters.
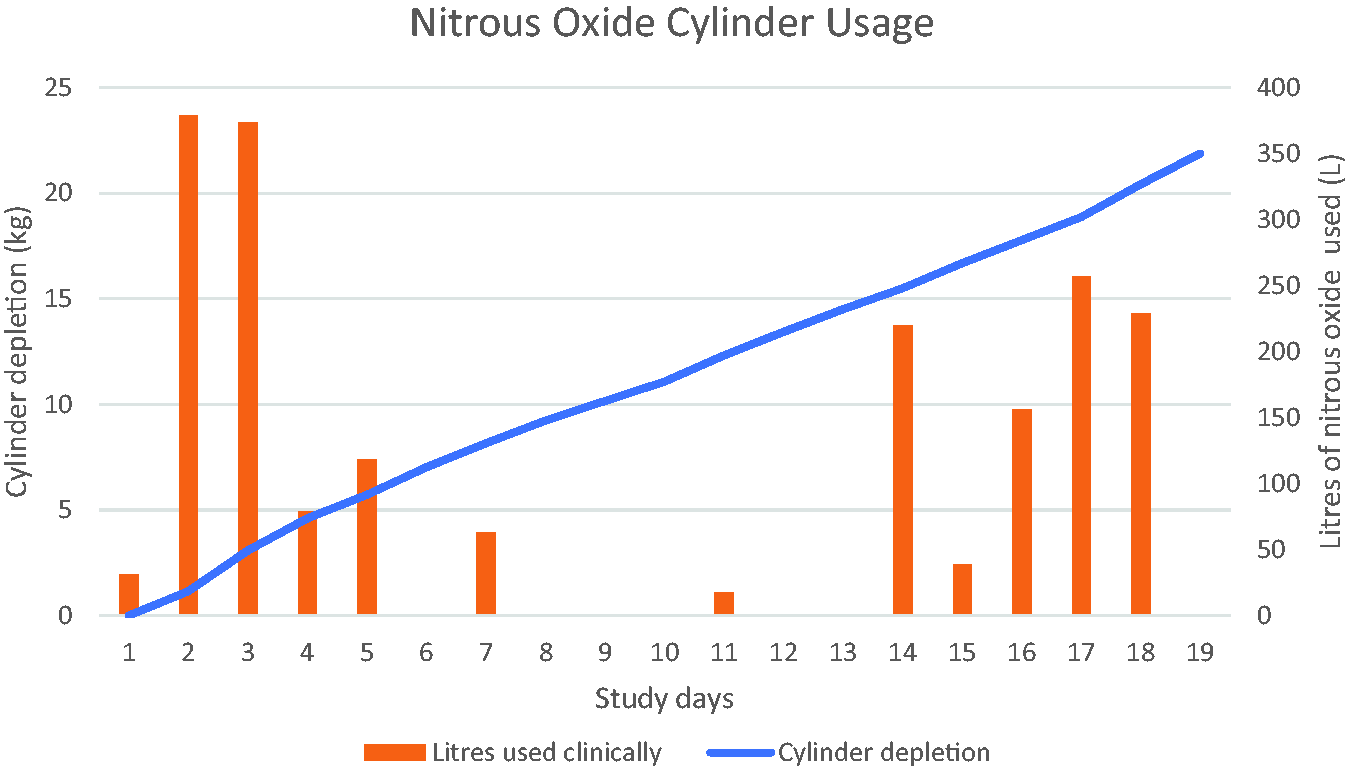
Comparison of actual cylinder depletion (kilograms) versus clinical usage (litres) during the 18-day study period.
Discussion
We describe a novel and cost-effective weighing method to assess N2O wastage at a non-obstetric surgical site with EMR capability. Widely available digital scales can be used to measure accurately the depletion of N2O cylinders and enable the detection of relatively small infrastructure leaks. Although we used the EMR to determine operating suite usage, measurement of clinical N2O consumption in a birthing suite (i.e. without anaesthetic machines) has been reported using a flowmeter. 9
Because of the constant pressure maintained by the regulator distal to the manifold, linear depletion of compressed gas and reduction in cylinder weight occurs in the presence of a leak. Hence the weighing technique can be used over shorter timeframes during any period of clinical inactivity (i.e. periods when N2O is not being used) using live camera recording or data cable feed.
The fraction of leaked N2O (83.5%) is consistent with other reports3 –6 as well as analysis of the previous 2-year period at our own institution. Extrapolating the 18-day result indicates annual wastage of 197,789 l N2O at our hospital site. This is equivalent to 101 tonnes CO2e per annum or driving a medium-sized sports utility vehicle 1571 km per day. 1 The financial impost of the leak is approximately $AUD4000 per annum. Residual N2O vented to the atmosphere when a cylinder is returned to the supplier also contributes to the emissions profile of a manifold-pipeline system. According to Boyle’s law, this residual volume is 400 l (0.75 kg) per cylinder at our institution. There are several potential limitations in our analysis. In the prospective analysis, FGF of N2O was assumed because it is not captured by the EMR. However, we regard the estimated FGF as generous because it was higher than that reported by all clinicians over the trial period. Second, if the prospective weighing analysis was performed during a period of higher clinical activity then the fraction of N2O wasted may have been lower assuming a constant rate of leak. It is possible that the spiral cylinder connecting leads influenced the displayed cylinder weight, although we took measures to minimise this. None of these errors are likely to be significant. Indoor and outdoor summer temperatures at our hospital site are often warmer than 15°C so the average density of N2O gas is likely to be lower than assumed in the calculation. According to the ideal gas law, this adjustment would increase the volume of N2O gas but not the number of N2O molecules (i.e. mass) depleted from the cylinder or wasted.
Australian standard AS 2896:2021 7 requires: (a) the manifold to be tested for leaks and malfunction every 12 months; (b) terminal wall outlet valve/seal assemblies to be tested at least every 2 years and replaced every 4 years; and (c) flexible hoses from wall outlets to the anaesthetic machine to be inspected and pressure tested annually (this includes concealed gas supplies such as theatre pendants and other articulated service modules, although in practice these sections are difficult to test effectively). There is no Australian standard requirement for maintenance or testing of the rigid gas pipelines connecting the manifold to terminal wall assemblies. At our site, a contractor engaged to investigate the discrepancy between cylinder depletion and clinical usage of N2O found a defective blind end in a N2O pipeline causing an audible leak. Significant pipeline leaks have been described elsewhere in Australia. 6
Unfortunately, standard testing and maintenance do not appear to prevent N2O infrastructure leaks adequately. The cylinder weighing technique can be used either to confirm and quantify, or rule out, suspected N2O leakage. Frequency of manifold N2O cylinder changes should also be routinely monitored because a sudden increase in turnover is strongly suggestive of a new leak. Decommissioning of hospital N2O manifold-pipeline networks in favour of cylinders at the point of care may be considered to avoid environmental harm and ongoing costly remedial work.
Footnotes
Author Contribution(s)
Acknowledgements
The authors wish to thank Dr David John, Staff Specialist Anaesthesiologist, Alfred Health; Ahmed Mostafa, Deputy Director, Engineering and Facility Services, Alfred Health; and Adam Deathridge, Director, H.H.M.G Australia for their support and assistance.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.