
Abstract
Lingual tonsillar hypertrophy is rarely identified on routine airway assessment but may cause difficulties in airway management. We conducted a narrative review of case reports of lingual tonsillar hypertrophy to examine associated patient factors, success rates of airway management techniques and complications. We searched the literature for anaesthetic management of cases with lingual tonsillar hypertrophy. We found 89 patients in various case reports, from which we derived 92 cases to analyse. 64% of cases were assessed as having a normal airway. Difficult and impossible face mask ventilation occurred in 29.6% and 1.4% of cases, respectively. Difficult intubation and failed intubation occurred in 89.1% and 21.7% of cases, respectively. Multiple attempts (up to six) at intubation were performed, with no successful intubation after the third attempt with direct laryngoscopy. Some 16.5% of patients were woken up and 4.3% required emergency front of neck access. Complications included oesophageal intubation (10.9%), bleeding (9.8%) and severe hypoxia (3.2%). Our findings show that severe cases of lingual hypertrophy may cause an unanticipated difficult airway and serious complications, including hypoxic brain damage and death. A robust airway strategy is required which includes limiting the number of attempts at laryngoscopy, and early priming and performance of emergency front of neck access if required. In patients with known severe lingual tonsillar hypertrophy, awake intubation should be considered.
Introduction
The lingual tonsils are located at the base of the tongue, and ‘although out of sight … should not be out of mind’. 1 They are part of Waldeyer’s ring of lymphoid tissue, and sit at the base of the tongue between the epiglottis posteriorly, the circumvallate papilla anteriorly and tonsillar pillars laterally.1,2 Lingual tonsillar hypertrophy (LTH) occurs in 0.3–3% of surgical patients.3 –5 However, one endoscopic study showed clinically meaningful LTH in 14–15%. 6 In the classification system of Friedman et al., clinically meaningful LTH includes lymphoid tissue classed as grade 3 (covering the entire tongue base with a vertical thickness of 5–10 mm) or grade 4 (covering the entire tongue base with a vertical thickness of approximately 1 cm, rising above the tip of the epiglottis). 7 A flexible nasendoscopic view of LTH is shown in Figure 1. The aetiology of LTH is unclear but it is associated with an elevated body mass index (BMI) and gastro-oesophageal reflux. 8
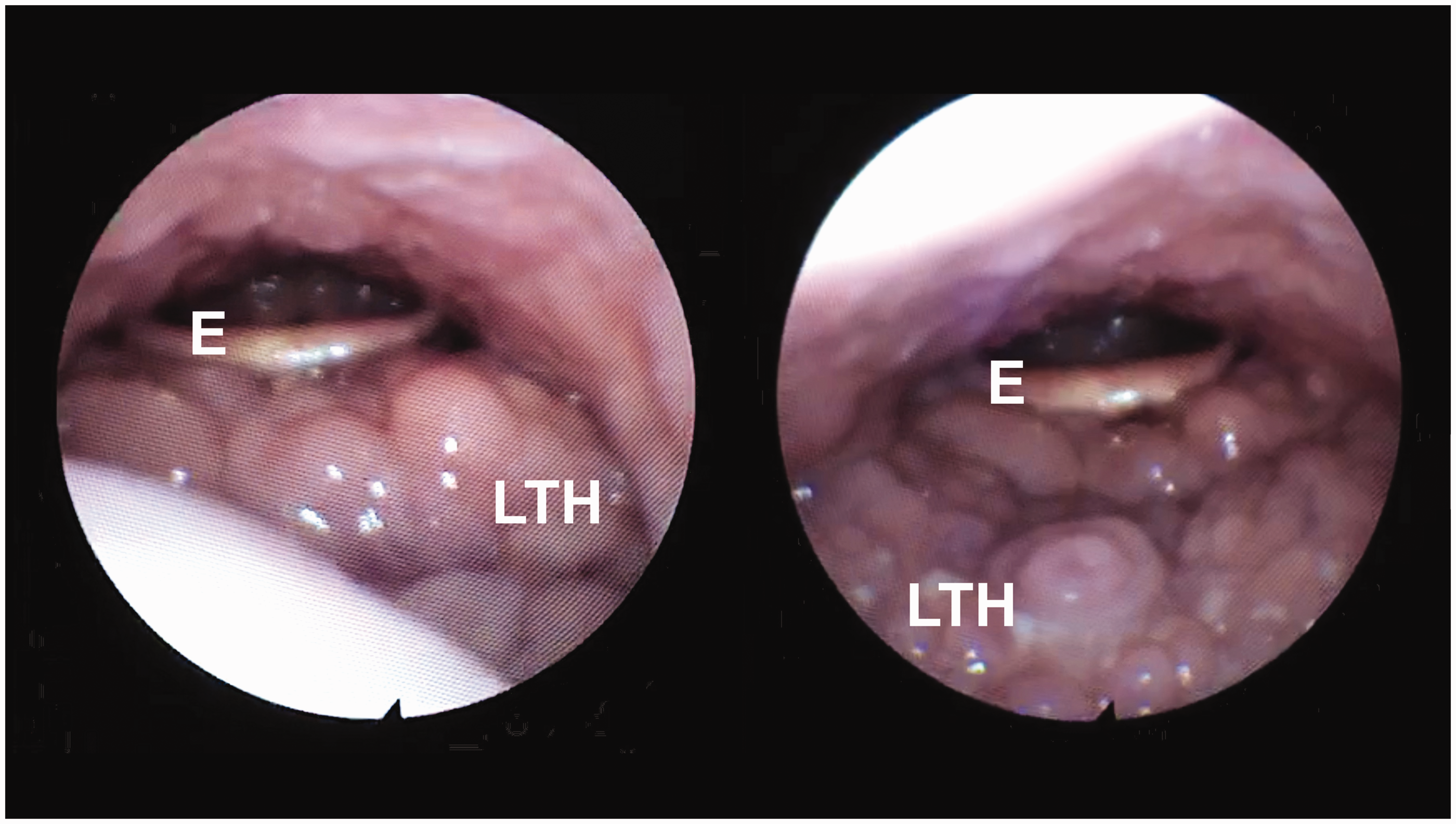
Flexible nasendoscopy of a patient with lingual tonsillar hypertrophy occupying the tongue base. E: epiglottis; LTH: lingual tonsillar hypertrophy.
LTH may be associated with hypoxia, oropharyngeal trauma, oesophageal intubation, cardiac arrest, and death.2,9 As such, the aims of our review are to obtain a detailed understanding of LTH, the success rates of various airway techniques, and the airway difficulties and complications associated with significant LTH. We also investigate the mechanism of failure of various airway techniques in relation to LTH. These may aid with decision making, choosing the optimal airway strategy, and minimising patient morbidity.
Methods
We performed a search of the literature reporting anaesthetic management of adult patients with LTH, and describe the patient characteristics, airway techniques used, and their outcomes and complications. We searched PubMed, Google Scholar and Google for relevant adult case reports relating to the anaesthetic airway management of LTH. We used the following keywords: ‘lingual tonsil’, ‘lingual tonsillar hypertrophy’, ‘lingual tonsillar hyperplasia’, ‘lingual tonsil hypertrophy’, ‘lingual tonsil hyperplasia’ combined with ‘anaesthesia’, ‘intubation’, or ‘difficult airway’. The search included all articles until December 2021 and was not limited by language.
We retrieved data on airway assessment including: Mallampati score, 10 mouth opening, thyromental distance, 11 head and neck movement, and whether the authors subjectively considered the patient as having a ‘normal airway’ (airway assessment unremarkable or not anticipating a difficult intubation). We collected data on anaesthetic techniques used; if the type of direct laryngoscope was not described, we assumed it was the Macintosh type. Outcome data were collected on airway technique success (e.g. ease of ventilation, laryngoscopic view and intubation success) and complications. Laryngoscopic laryngeal view was graded using the Cormack–Lehane (CL) classification: 12 1, full view of the vocal cords; 2, only part of the vocal cords or arytenoids seen; 3, epiglottis seen; and 4, no epiglottis seen. We applied this to direct laryngoscopy, videolaryngoscopy and flexible bronchoscopy intubation (FBI) views. If ‘no glottis’ was documented then we classified this as CL grade 3. For data analysis, we grouped CL grades 1 and 2 together so as to include those documented as ‘easy view of the glottis’ (or similar). We defined ‘difficult intubation’ as CL grade 3 or greater, or tracheal intubation requiring threeor more attempts, or failed tracheal intubation. 12 ‘Multiple attempts’ was defined as three or more documented attempts, and severe hypoxia as an arterial saturation (SpO2) less than 80%.
Each episode that a patient presented for surgery was termed a ‘case’. If, following induction of anaesthesia and failed airway management, a patient was woken up and required a subsequent awake FBI, we termed this a ‘postoperative awake FBI’. We did not count this as an extra case as the scheduled surgery was not performed and we regarded awake FBI as a continuum of the original airway strategy. 13
For data analysis, the denominator was the total number of patients or cases with recorded data. We defined the ‘overall technique success rate’ as the number of times a technique was used and was ultimately successful = (number of cases a technique was successful)/(number of cases in which the technique was used). However, a given technique may be used multiple times. Accordingly, the ‘attempt success rate’= number of successful attempts/total number of attempts using that technique. For example, direct laryngoscopy may have been used in 10 cases and was successful in four cases but there was a total of 20 attempts. This gives an overall technique success rate of 40% (four out 10 cases) but an attempt success rate of 20% (four out of 20 attempts).
Statistical analysis
Descriptive data are presented as mean (range) for continuous variables, or number (percentages) for categorical variables. Each preoperative airway assessment method was categorised into two groups based on criteria predicting difficult intubation: that is, Mallampati scores 3 or 4; 10 mouth opening less than 4 cm or less than two finger breadths; thyromental distance (<6 cm or less than three finger breadths); 11 and moderately or severely limited head and neck movement. The predictive power for each airway assessment was described using sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV), with their respective 95% confidence intervals (CIs). Confidence intervals for sensitivity and specificity were estimated using the Clopper–Pearson exact method. 14 We used a Fisher’s exact test to determine if there was a statistically significant relationship between predicted and actual successful tracheal intubations. A P value less than 0.05 was considered statistically significant.
Results
We retrieved 48 articles: 34 in English,2,5,9,15 –45 nine in Japanese,46 –54 two in Spanish,55,56 one in Korean, 57 one in French, 58 and one in Italian. 59 These articles described a total of 89 patients and 92 cases (see Figure 2). One case series by Ovassapian et al. included a total of 33 patients: 27 patients had unanticipated failed direct laryngoscopic intubation followed by successful asleep FBI and six patients had an awake FBI due to their history of unanticipated failed intubation. 2 Another article reported three patients but we only included one patient due to a lack of data for the others. 21
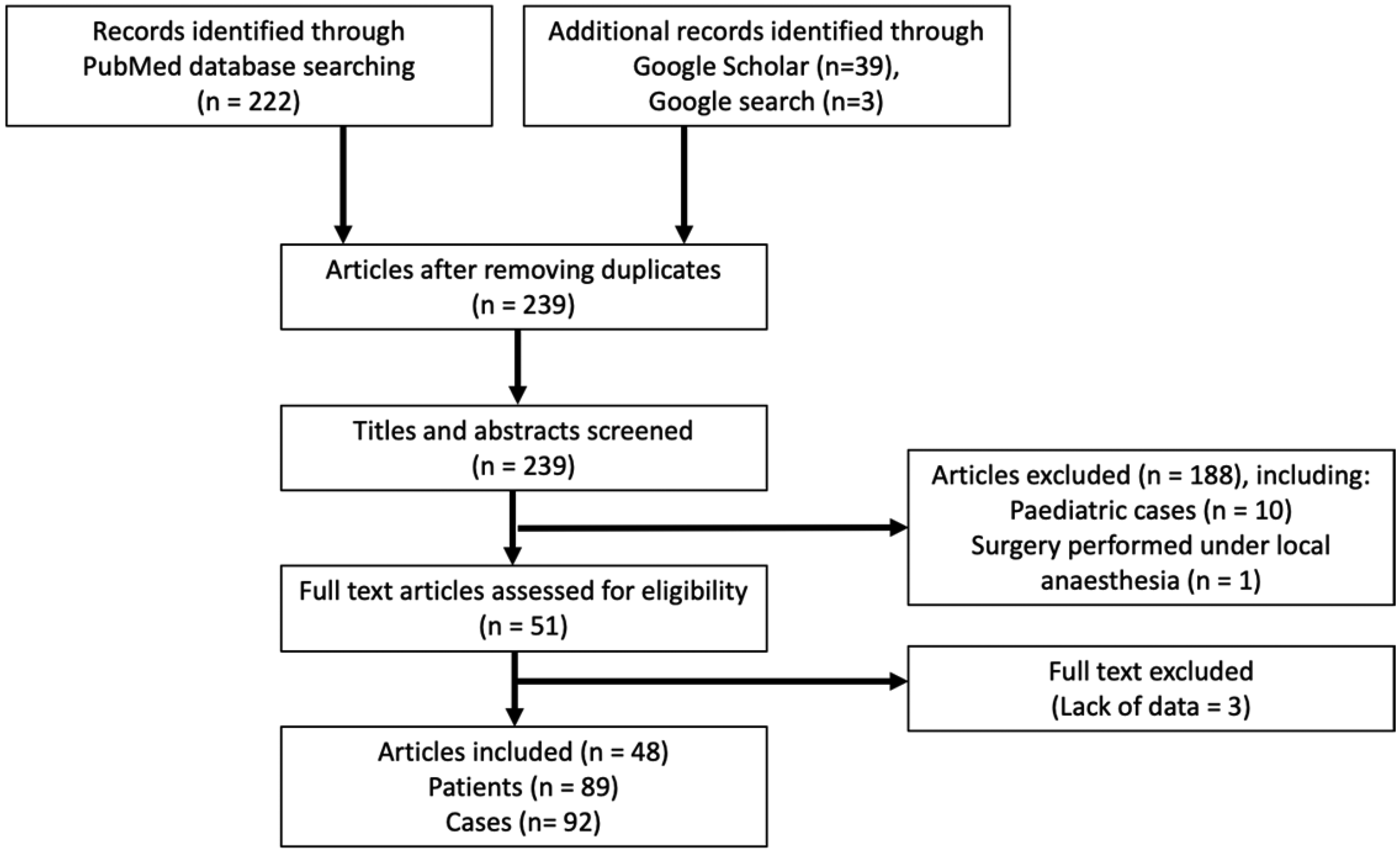
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flow chart.
The patient characteristics are presented in Table 1. The mean age, weight and BMI of our patients were 49.3 years, 89.3 kg and 31.2 kg/m2, respectively. Some 19.7% of cases had a BMI of 40 kg/m2 or greater. In the four cases of severe hypoxia, three had BMI greater than 30 kg/m2.9,28 13.5% of cases had either obstructive sleep apnoea (OSA) or LTH-related symptoms preoperatively: sore throat, dysphagia, globus sensation, speech change, chronic cough, dyspnoea, snoring, choking on food, otalgia and submandibular referred pain;1,8,9,26 64.0% of LTH patients had a ‘normal airway’ (Table 1). In LTH patients, predictive values of routine airway assessments varied (Table 2): sensitivity 6.0–31.3%; specificity 37.5–100%; PPV 70.6–100%; and NPV 6.8–15.1%.
Patient characteristics and routine airway assessments.
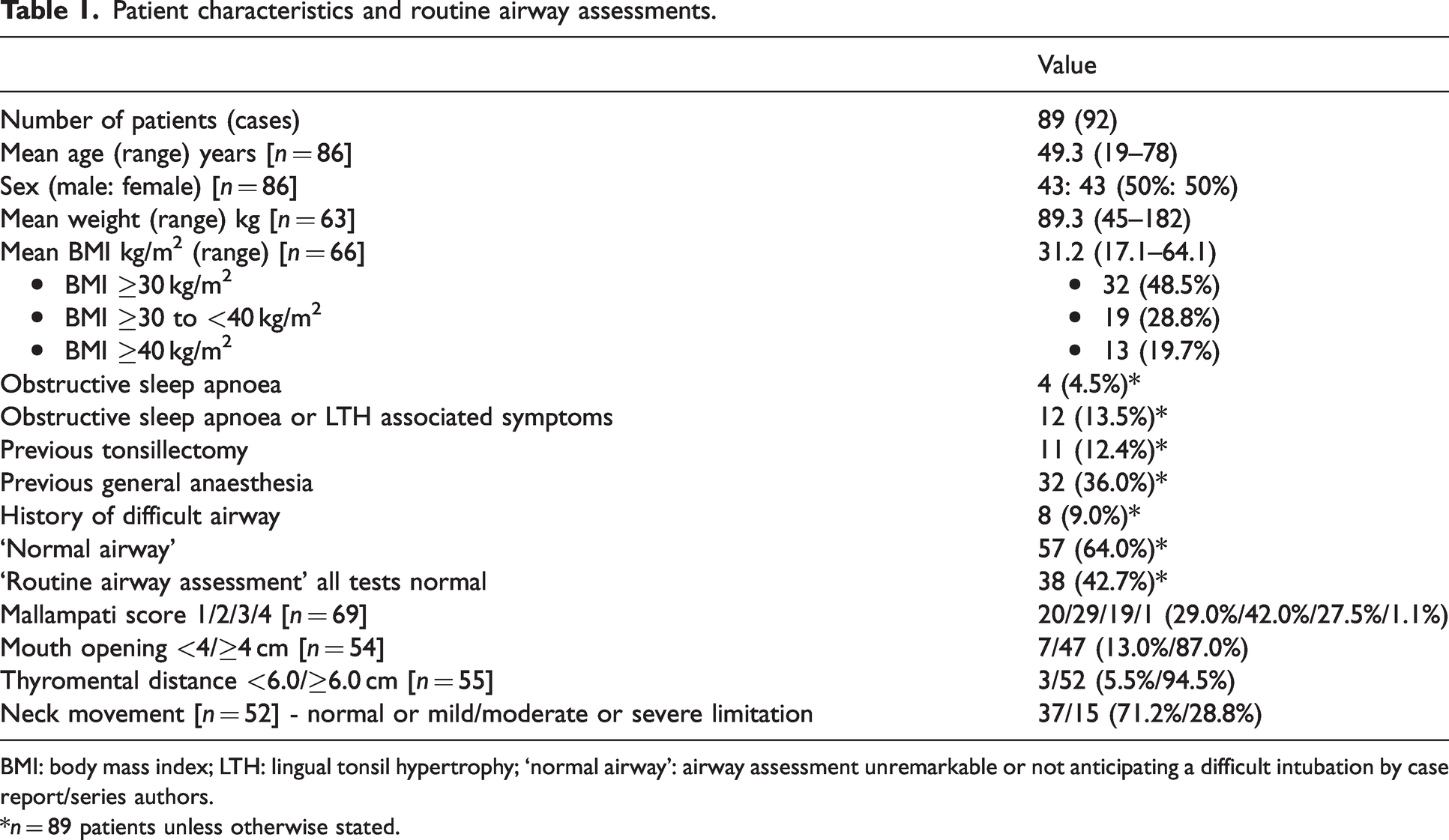
BMI: body mass index; LTH: lingual tonsil hypertrophy; ‘normal airway’: airway assessment unremarkable or not anticipating a difficult intubation by case report/series authors.
*n = 89 patients unless otherwise stated.
Predictive value for difficult intubation for various airway assessment methods (% and 95% confidence interval).
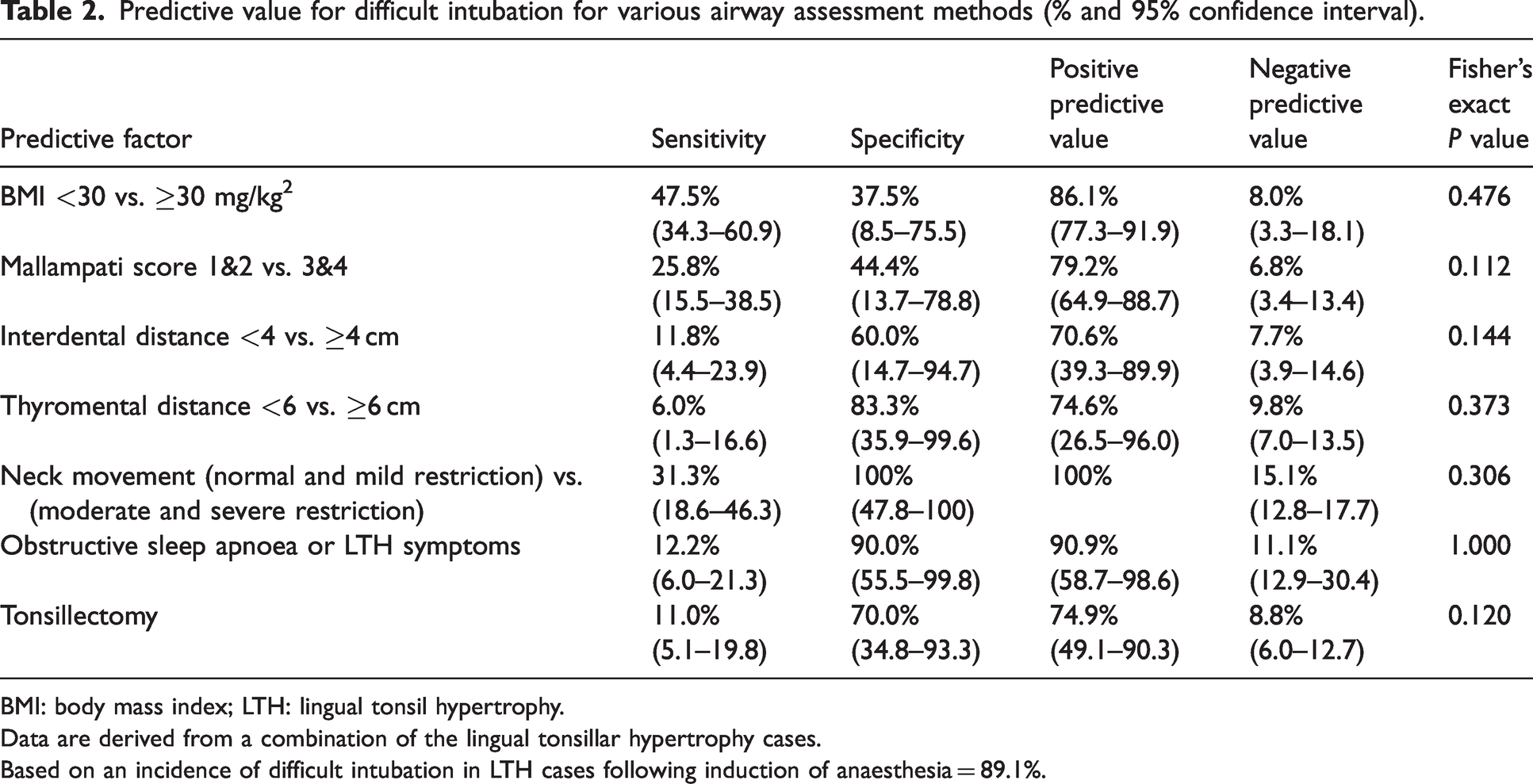
BMI: body mass index; LTH: lingual tonsil hypertrophy.
Data are derived from a combination of the lingual tonsillar hypertrophy cases.
Based on an incidence of difficult intubation in LTH cases following induction of anaesthesia = 89.1%.
Most (92.4%) LTH cases had attempts at securing their airway after induction of anaesthesia. Four cases had known LTH after preoperative assessment and investigations.25,45,52,57 Failed airway management resulted in attempts to wake up the patient in 14 (16.5%) cases. Seven (7.6%) LTH cases were anticipated as having a difficult airway and had awake tracheal intubation.
Difficult and impossible face mask ventilation (as defined by the case report authors) in LTH cases occurred in 29.6% and 1.4% of cases, respectively (Table 3). Supraglottic airways provided easy/adequate and difficult ventilation in 72.0% and 20.0% of LTH cases, respectively. Difficult and failed intubation rates occurred in 89.1% and 21.7% of LTH cases, respectively. The overall technique success rates for Macintosh, straight blade and videolaryngoscopy were 15.4%, 20.0% and 50.0%, respectively. However, attempt success rates were lower for the Macintosh and straight blade laryngoscopy: 2.0% and 12.5%, respectively. Macintosh laryngoscopy grades were reported in 65 cases, and CL grades 1 and 2 (combined), grade 3 and grade 4 were obtained in five (7.7%), 35 (53.8%) and 25 (38.5%) cases, respectively. These were associated with decreasing intubation success rates: 80%, 20% and 4%, respectively.
Anaesthetic airway management of lingual tonsillar hypertrophy cases and outcomes of each airway technique.
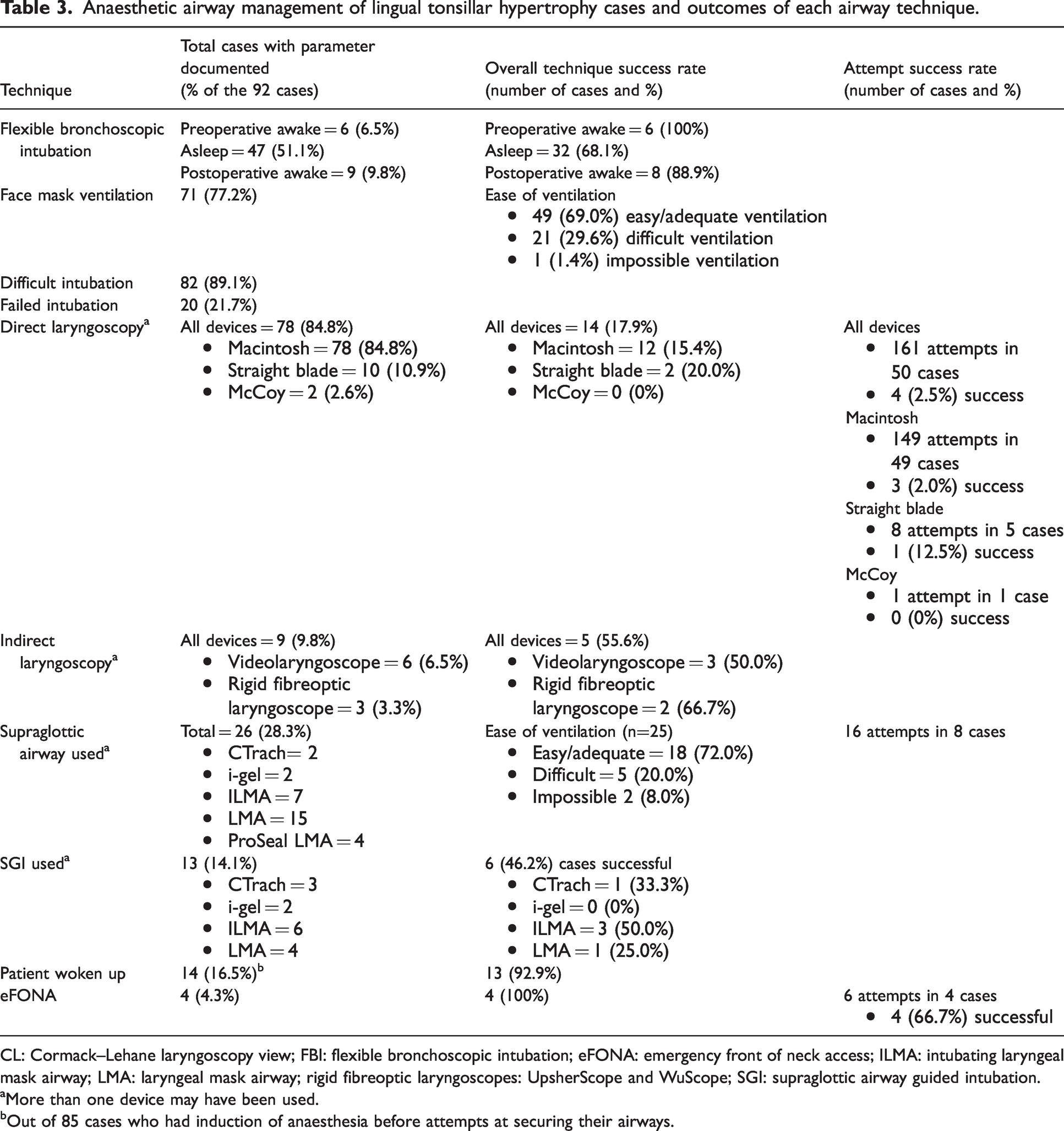
CL: Cormack–Lehane laryngoscopy view; FBI: flexible bronchoscopic intubation; eFONA: emergency front of neck access; ILMA: intubating laryngeal mask airway; LMA: laryngeal mask airway; rigid fibreoptic laryngoscopes: UpsherScope and WuScope; SGI: supraglottic airway guided intubation.
More than one device may have been used.
Out of 85 cases who had induction of anaesthesia before attempts at securing their airways.
Direct laryngoscopy was associated with multiple attempts: one to six attempts were made in four (5.1%), nine (12.8%), 15 (19.2%), 17 (21.8%), four (5.1%) and one (1.3%) cases, respectively. Intubation success rates for one, two and three attempts were 25.0%, 22.2% and 6.7%, respectively. No successful intubations occurred after a third attempt.
FBI under anaesthesia was the technique most often used in LTH cases after failed intubation (51.5%), and had an overall technique success rate of 68.1% (Table 4). Impingement and failure to railroad the tracheal tube occurred in 11 (23.4%) and two (4.3%) cases, respectively. FBI was also performed by way of a supraglottic airway (supraglottic airway guided intubation, SGI) 60 in 13 (14.1%) cases and had an overall technique success rate of 46.2%.
Success rates of airway techniques in the lingual tonsillar hypertrophy cases compared with those from other difficult airway studies (% and 95% confidence interval).
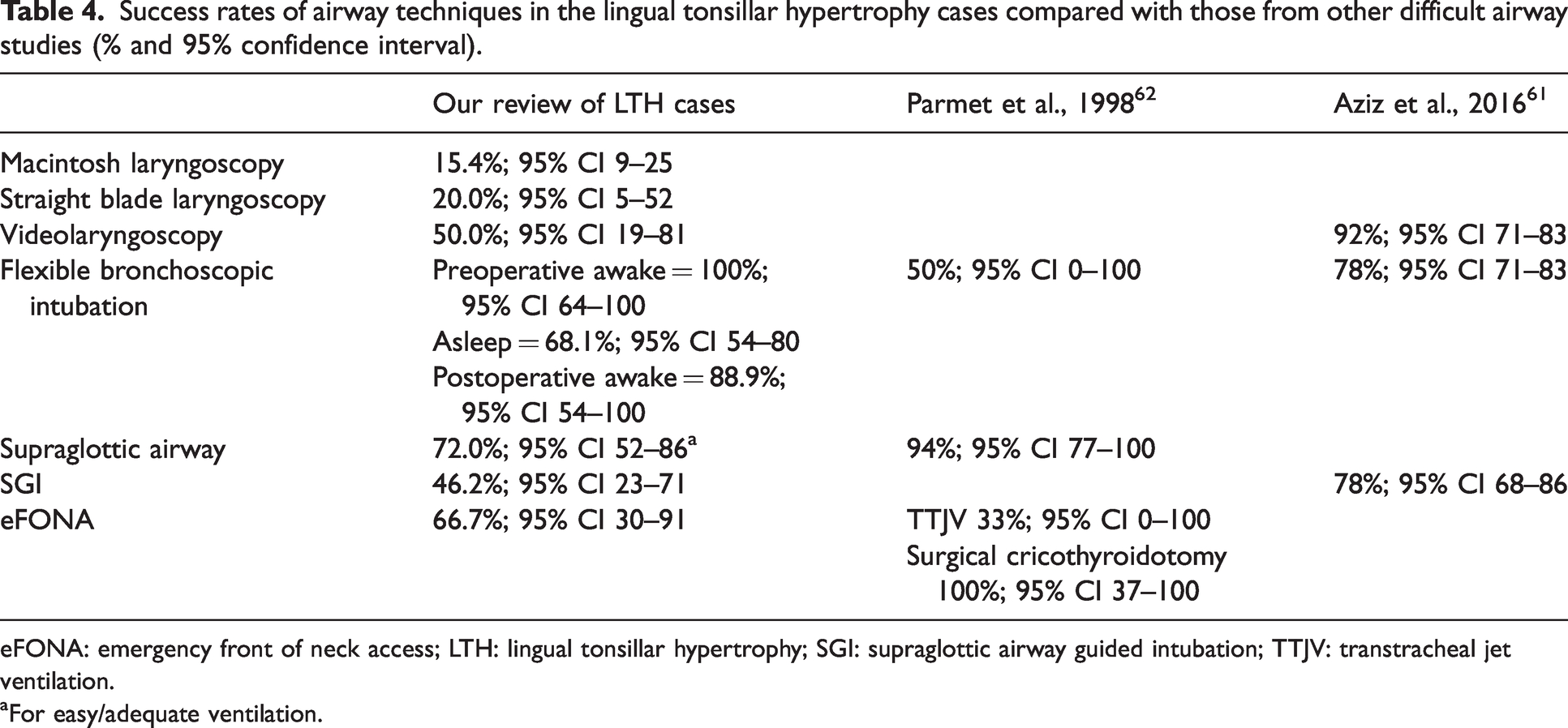
eFONA: emergency front of neck access; LTH: lingual tonsillar hypertrophy; SGI: supraglottic airway guided intubation; TTJV: transtracheal jet ventilation.
For easy/adequate ventilation.
‘Non-standard airway techniques’ were those other than the conventional use of the above airway techniques (supraglottic airway, direct and videolaryngoscopy, FBI and SGI), and were mainly performed after more conventional techniques had failed. They included bougie guided Pro-Seal LMA insertion, 22 light wand guided intubation,24,48 FBI by a stylet guided double lumen tube, 39 direct or videolaryngoscopy facilitating FBI, 57 rigid bronchoscopy, 23 retrograde wire guided intubation,18,43,47 surgical laryngoscopy, 26 and laryngeal tube. 37 Further description of these are beyond the scope of this review.
The LTH cases had a 4.3% incidence of emergency front of neck access (eFONA), which had an overall technique and attempt success rates of 100% and 66.7%, respectively. Two cases of failed eFONA were rescued by an alternative eFONA approach.26,28 Most eFONA cases were associated with serious complications; for example, cyanosis, 26 severe hypoxia (SpO2 30%), 28 hypoxic brain damage, cardiac arrest and death. 9
Oesophageal intubation occurred in 10 (10.9%) LTH cases.2,9,20,23,51 Other complications included oropharyngeal bleeding in nine (9.8%) cases, severe hypoxia in three (3.3%) cases,9,28,53 and one case (1.1%) each of an oesophageal tear, 2 epistaxis 51 and death. 9
Discussion
In our review of the literature reporting anaesthetic management of patients with LTH we found that LTH was usually not identified on clinical airway assessment, techniques to secure the airway had lower rates of success compared with other studies of difficult airways,61,62 and failure to secure the airway often led to serious complications.
Routine airway assessment did not pick up lingual tonsillar hypertrophy
Most LTH cases had a ‘normal airway’ on assessment and only 13.5% of cases had OSA or LTH associated symptoms. This suggests that routine airway assessment rarely identifies LTH due to its tongue-base location, although in one case it was seen on oral examination. 25 The high PPV for difficult intubation in LTH cases reflects the high prevalence of difficult intubation. 63 Of concern, the low NPV values in LTH patients may lead clinicians erroneously to assume an easy intubation. In the case series of unanticipated failed intubation by Ovassapian et al., preoperative airway assessment by an experienced anaesthetist failed to suggest a difficult airway in almost half of the patients, when LTH was the only finding that could have contributed to failure of intubation. 2
Most LTH cases were unanticipated difficult airways, for which the Difficult Airway Society (DAS) recommend a plan A, B, C, D strategy: plan A, face mask ventilation and laryngoscopy; B, supraglottic airway insertion and ventilation; C, final attempt at face mask ventilation; and D, emergency front of neck access (eFONA). 13 Optimization manoeuvres are carried out while early priming of eFONA allows its implementation as soon as a ‘cannot intubate, cannot oxygenate’ (CICO) is declared. 64 In addition, the Vortex is a recently introduced tool that facilitates efficient implementation of best efforts at upper airway lifelines (facemask ventilation, supraglottic airway ventilation and laryngoscopy) with early and parallel preparation, priming and implementation of eFONA.
Awake tracheal intubation may be the best option for known severe lingual tonsillar hypertrophy patients
For LTH patients with an anticipated difficult airway, reports indicated preoperative airway assessment with flexible nasendoscopy and radiological investigations may be helpful.1,6 A flexible nasendoscopy gives a ‘birds eye view’ of the oropharynx. A ‘negative’ flexible nasendoscopy view (i.e. glottis not visualised) may be due to abnormal anatomy (e.g reduced neck mobility) or the presence of an airway lesion (e.g. obstructing, vascular, friable or a rapidly changing one), and thus predict a difficult airway. However, photographs from Ovassapian et al. also show falsely reassuring ‘positive’ awake flexible nasendoscopy views (i.e. glottis seen), yet all were from patients who had failed intubation. 2 This may be partly explained by the flexible nasendoscopy being performed in the awake patient. However, after induction of anaesthesia, there is an abrupt decrease in upper airway muscle activity and increase in upper airway collapsibility. 65 This, with the added presence of LTH causing obstruction, may lead to difficult facemask ventilation and difficult intubation.
In the anticipated difficult airway, awake intubation techniques may be indicated.66,67 In the LTH cases, awake preoperative and postoperative FBI had high success rates, that is, 100% and 88.9%, respectively, which may be explained as follows. Airway patency, airway protective reflexes and spontaneous ventilation are maintained. A sitting patient has added advantages—gravity helps open up the airway and secretions are pooled away and functional residual capacity is increased. 68 The absence of induction agents helps maintain cardiovascular stability. In the LTH cases, awake FBI views were improved when the LTH mass was displaced by changing a patient from supine to a sitting position, 37 or when the patient was asked to phonate ‘E’. 31 However, awake FBI has been associated with airway obstruction or loss of airway control due to sedation and local anaesthetic topicalization.60,66
The incidence of difficult and impossible facemask ventilation was higher in the LTH cases than that reported in the general population (29.6 vs. 1.4% and 1.4% vs. 0.16%, respectively). 69 Facemask ventilation may be more difficult as the LTH may distort the supraglottis,2,19,23,25,26,36,38,39 or overhang the borders of the epiglottis and cause airway obstruction. 2 Posterior displacement of the tongue may limit airflow from both nasal and oral routes, and an increased thickness of the tongue base is a predictor of difficult face mask ventilation. 70
Direct laryngoscopy commonly failed in lingual tonsillar hypertrophy cases
Difficult and failed intubation rates in the LTH cases compared unfavourably with those from the unselected population: 89.1% versus 0.3–13.3% 12 and 21.7% versus 0.4%, 61 respectively. Direct laryngoscopy in our LTH cases had an overall technique success rate of 15.4%, which contrasts with 90.6% from a Cochrane review of adult patients (with or without predicted/known difficult airways) requiring tracheal intubation. 71 There are various reasons to explain this. All our cases likely had clinically significant LTH whereas the incidence of LTH across surgical patients is low (0.3–3%).3 –5 Direct laryngoscopy requires a ‘line of sight’ to the larynx, 72 which is obtained by inserting the laryngoscope blade lateral to the tongue, moving the latter to the left, and then advancing the blade in the midline into the vallecula to visualise the glottis. 72 However, this may not be possible if the LTH lesion occupies the entire vallecula,1,7 or causes the epiglottis to be downfolded, retroflexed, immobile or buried.2,19,23,25,26,36,38,39 In addition, if the tongue is not displaced to the left, the base of the tongue may be compressed distally producing posterior displacement of the epiglottis. 72
Straight blade laryngoscopy has theoretical advantages over Macintosh laryngoscopy for LTH cases: reduced lifting, compression and displacement of the tongue and epiglottis; an improved line of sight (no intrusion as seen with the curved Macintosh blade); and with the retromolar approach, reduction of the intrusion of maxillary structures into the line of sight. 73 However, straight blade laryngoscopy in LTH cases still had a low success rate and this may be due to it being not commonly used or taught, the aryepiglottic fold may obscure the glottis with the paraglossal approach, and control of the epiglottis may be poorer. 73
Most LTH cases pre-dated the introduction of videolaryngoscopy in the early 2000s. However, there are various benefits of videolaryngoscopy over direct laryngoscopy:71,74 improved glottic view, less airway trauma, reduced number of failed intubations, shorter learning curves, and a shared ‘video’ view of the airway. However, videolaryngoscopy in LTH cases resulted in a lower overall technique success rate (50%) than those seen in other studies (Tables 3 and 4).61,75 Several factors may account for this. Our review only contained six cases. Correct videolaryngoscope placement may be impaired by the LTH or decreased oropharyngeal space as seen in obese and OSA patients.76,77 Compression of the tongue, distortion of the epiglottis and bleeding during videolaryngoscopy were reported in several cases.16,20,23,39,44,58,59 LTH may also obstruct the videolaryngoscope light, creating a shadow and preventing glottic visualization. 15 There may also be a ‘blind spot’ during videolaryngoscopy, that is, after the tracheal tube enters the oropharynx but before it comes into view on the device’s monitor, leading to airway trauma. 45
Multiple attempts at intubation were associated with an increased incidence of serious morbidity, 78 and the number of attempts should be limited.66,78 Furthermore, in cases with a documented number of attempts, no successful intubations occurred after a third attempt using direct laryngoscopy. This is important as it suggests that further attempts may be futile or harmful, countering the DAS recommended maximum ‘3 + 1’ attempts, where the ‘+1’ refers to a ‘fourth attempt by a more experienced colleague’. 13
Rescue supraglottic ventilation succeeded in only three-quarters of lingual tonsillar hypertrophy cases
After failed intubation, an attempt to rescue ventilation by a supraglottic airway is recommended13,64,66 as it has a success rate of 65.1–94% in the literature.62,79 In LTH cases, it provided easy/adequate and difficult ventilation in 72.0% and 20.0% of cases, respectively. However, in some LTH cases, insertion of a supraglottic airway failed or caused bleeding.17,28 If supraglottic airway ventilation is successful, four options are available: 13 proceed with surgery with the supraglottic airway in situ, perform SGI, wake up the patient, or perform eFONA. The first option is a high-risk strategy in LTH cases as a CICO scenario may result from airway oedema, bleeding, laryngospasm, and supraglottic airway displacement.13,66 This option was chosen in one LTH case for urgent surgery, 64 but we would recommend that eFONA be primed and ready to implement.
FBI under anaesthesia had a lower success rate than for awake FBI (Table 4) and may be due to several reasons. All the advantages of an awake intubation are lost (see above). Many cases were obese and some developed severe hypoxia leading to stress and time pressure on the anaesthetist. Impingement during railroading of the tracheal tube over the bronchoscope may be caused by LTH mass, distorted laryngeal structures, and decreased airway patency secondary to anaesthesia, OSA and obesity. SGI overall technique success rate was 46.2% (Table 4) which is lower than from other studies, that is, 54–94%,61,66 and may be due to the LTH impairing the bronchoscope reaching, or visualising, the glottis.
When a CICO scenario is anticipated, early transition, priming and implementation of eFONA is warranted to avoid hypoxic brain injury and death.9,13,64,66,80 The LTH cases had a 4.3% incidence of eFONA which is one to two orders of magnitude higher than in adults presenting for surgery (0.01%) or ear, nose and throat procedures (0.2%). 81 The overall technique and attempt success rates were 100% and 66.7%, respectively. Two cases of failed eFONA were rescued by an alternative eFONA approach.26,28 Most eFONA cases were associated with serious complications,9,26,28 and may suggest the need for improved training in, and early priming and implementation of, the technique.64,80
Waking up the patient was attempted in 16.5% of cases, which compares with 0.8% of patients in a study of failed laryngoscopy. 61 However, it may not be possible or safe to wake up a patient due to airway oedema or bleeding, cardiac or respiratory instability, urgency of surgery, or inability to reverse the effects of anaesthetic or neuromuscular blocking agents in a timely manner. In one case, after waking up the patient following multiple failed airway techniques, the patient struggled to breathe, became cyanotic and required eFONA. 26
There were many airway-related complications described in the LTH cases, with hypoxic brain damage and death being the most serious. 9 To minimise future complications, Ovassapian et al. recommended fibreoptic nasendoscopy in all patients with unanticipated failed intubation to rule out LTH. 2 Identifiable risk factors for airway complications in the LTH cases included poor management, 66 obesity, 80 emergency out-of-hours surgery, multiple attempts at tracheal intubation,78,80 and performing eFONA. A fifth of cases had a BMI of 40 kg/m2 or greater (‘morbid obesity’) and airway management is more difficult in such patients due to the shorter safe apnoea time and higher incidence of difficult airways.66,82 Oesophageal intubation in LTH cases was not uncommon, and its incidence is higher than in other studies (10.9% vs. 1–2%, respectively). 80 Other non-LTH factors may also have contributed to difficulties in airway management: acromegaly,20,37 temporomandibular joint ankylosis, 35 LTH bleeding precluding the use of FBI, 23 epistaxis,51,59 patient refusal for awake tracheal intubation, 29 and the nasal route not being available for FBI due to the site of surgery. 20
The airway management of some of the LTH cases may be open to criticism, for example, multiple attempts at airway techniques, blind attempts at intubation (in one case causing bleeding), 15 and not performing awake tracheal intubation despite seeing ‘enormous’ LTH on oral examination. 25 Four cases had known LTH but awake tracheal intubation was not performed.25,45,52,57 At the risk of hindsight bias, this raises the question whether awake FBI would have avoided subsequent airway complications such as palatal perforation 45 or the need for tracheostomy. 25
This review is limited by being drawn from mainly case reports and a major case series, constituting a lower level of evidence. In a previous small case series, the authors found no association between LTH and difficult airways. 5 However, it consisted of six cases screened from patients scheduled for elective surgery, and there was no grading of the severity of the LTH. In the current review, data were combined for statistical analysis so caution should be used when interpreting the results. Our comments and recommendations apply only to cases with clinically significant LTH as most of the cases were likely to be grade 4. None of the cases were formally graded as the Friedmann classification is a recent addition. 7 Also, success of airway techniques cannot be accurately calculated as the cases are heterogeneous. Further, data were lacking in many cases, for example, BMI, OSA, previous tonsillectomy, detailed airway assessment, number of attempts of each airway intervention, and the frequency and severity of complications. Although CL grade 3 is included in the definition of ‘difficult intubation’, intubation may still be straightforward with the aid of intubating adjuncts such as a bougie. Reporting and publication bias also favour severe cases and cases when novel airway techniques are used. Despite these limitations, this review provides a detailed database for LTH management.
It should be noted that a third of the reports in this review were published over 20 years ago and so would not have benefitted from recent advances in anaesthetic airway management. These include videolaryngoscopy and second generation supraglottic airways, 80 sugammadex for rapid reversal of neuromuscular blockade, difficult airway algorithms,13,64,67 lessons learnt from large national airway audits (e.g. NAP4), 66 high flow nasal oxygen to prolong safe apnoea time, and availability of difficult airway databases to identify at-risk patients. 80
Conclusions
The findings of this review indicate that LTH is rarely identified on routine airway assessment. Severe cases may lead to unanticipated difficult airways and associated morbidity and even mortality. Rescue techniques after failed intubation may fail due to their exacerbation of the space occupying effect of LTH. A robust airway strategy for managing patients with severe LTH includes consideration of awake tracheal intubation, which has a high success rate. The efficient use of upper airway resources is required including limiting the number of laryngoscopic attempts (more than three attempts at direct laryngoscopy may be futile and harmful), considering the use of straight blade laryngoscopy if experienced, and being mindful that rescue supraglottic airway ventilation may be difficult or fail in up to 30% of severe LTH cases. Finally, plan for success but ‘prepare for failure’ which may require early priming and implementation of eFONA.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.