
Abstract
Opioid analgesics prescribed for the management of acute pain following orthopaedic surgery may lead to unintended long-term opioid use and associated patient harms. This study aimed to examine the prevalence of opioid use at 90 days after elective orthopaedic surgery across major city, regional and rural locations in New South Wales, Australia. We conducted a prospective, observational cohort study of patients undergoing elective orthopaedic surgery at five hospitals from major city, regional, rural, public and private settings between April 2017 and February 2020. Data were collected by patient questionnaire at the pre-admission clinic 2–6 weeks before surgery and by telephone call after 90 days following surgery. Of the 361 participants recruited, 54% (195/361) were women and the mean age was 67.7 years (standard deviation 10.1 years). Opioid use at 90 or more days after orthopaedic surgery was reported by 15.8% (57/361; 95% confidence interval (CI) 12.2–20%) of all participants and ranged from 3.5% (2/57) at a major city location to 37.8% (14/37) at an inner regional location. Predictors of long-term postoperative opioid use in the multivariable analysis were surgery performed at an inner regional location (adjusted odds ratio 12.26; 95% CI 2.2–68.24) and outer regional location (adjusted odds ratio 5.46; 95% CI 1.09–27.50) after adjusting for known covariates. Long-term opioid use was reported in over 15% of patients following orthopaedic surgery and appears to be more prevalent in regional locations in Australia.
Introduction
Opioid analgesics are routinely used for the management of acute pain following surgery. 1 Of the surgical specialties, patients undergoing orthopaedic surgery are among the three highest users of opioids postoperatively. 2 However, opioids prescribed for acute post-surgical pain may lead to unintended long-term opioid use and associated patient harms. A retrospective cohort study of 23,726 patients undergoing total knee arthroplasty in the United States of America (USA) reported that 41.2% of patients were still taking opioids at 90 days postoperatively, and 30.4% of patients continued opioid use up to one year after surgery. 3 In the Australian context, a systematic review identified that 3.9–10.5% of surgical patients continued opioid use between 2 and 4 months postoperatively. 4 Long-term opioid use (defined as opioid use for 90 days or more) 5 is associated with opioid tolerance, dependence and an increased risk of adverse effects including respiratory depression and falls.6,7 The identification of factors associated with an increased risk of long-term postoperative opioid use may aid clinicians in reducing the prevalence and harms associated with long-term opioid use.
Previous studies have identified variables associated with increased odds of long-term opioid use after orthopaedic surgery. Such factors include anxiety (odds ratio (OR) 2.1; 95% confidence interval (CI) 1.1–4.1), higher self-reported pain score at 90 or more days after surgery (OR 5.8; 95% CI 2.9–11.9), 8 preoperative opioid use (OR 1.72; 95% CI 1.27–2.33), 9 knee surgery compared with hip surgery (OR 1.75; 95% CI 1.59–1.93), 9 tobacco use (OR 1.20; 95% CI 1.07–1.35), 9 benzodiazepine use (OR 1.42; 95% CI 1.27–1.56) 9 and preoperative substance abuse (OR 1.45; 95% CI 1.07–1.98). 10 In addition, a study of 5676 patients who underwent total shoulder arthroplasty in the USA reported significant regional variation in rates of long-term opioid use after surgery, with surgery performed in the western USA (OR 1.8; 95% CI 1.3–2.4) identified as a strong predictor of long-term postoperative opioid use. 11 Geographical differences in patterns of long-term opioid use may be linked with socioeconomic indicators such as employment rates, education status and access to health services. As such, a USA-based study demonstrated that low socioeconomic status was associated with a lower likelihood of opioid discontinuation after total joint arthroplasty (hazard ratio (HR) 0.67, 95% CI 0.56–0.80). 12 However, it is unknown whether these trends from the USA are generalisable to the Australian context. Therefore, the primary objective of this study was to examine the prevalence of any opioid use (defined as the use of opioids to any extent, including daily opioid use as well as when-required opioid use) at 90 days after elective orthopaedic surgery across Australian major city, regional and rural locations. Our secondary objective was to examine the association between hospital location and opioid use at 90 days after elective orthopaedic surgery while adjusting for covariates.
Materials and methods
Study design
We conducted a prospective, observational cohort study at five hospitals in New South Wales, Australia:
480-bed major city private hospital; 796-bed inner regional major tertiary referral public hospital and trauma centre; 292-bed outer regional major referral public hospital (outer regional hospital A); 151-bed outer regional private hospital (outer regional hospital B); 180-bed rural referral public hospital.
Patients were recruited from April 2017 to November 2019, then followed up by telephone call or email from June 2017 to February 2020.
The study was conducted in accordance with the strengthening the reporting of observational studies in epidemiology (STROBE) guidelines. 13 This study was approved by the St Vincent’s Hospital Human Research Ethics Committee (LNR/17/SVH/155). No incentives were offered to participants in the study.
Participants
Patients aged 18 years or older who underwent elective orthopaedic surgery were included in the study. Exclusion criteria included surgical procedures conducted under local anaesthesia, surgery due to malignancy, and inability to complete the study questionnaire due to a medical condition (such as dementia) or a significant language barrier. A sample of potentially eligible patients was selected using simple randomisation during the hospital pre-admission visit held from 2 to 6 weeks before surgery. Written informed consent was obtained on study enrolment.
Data collection
Preoperative data collection
During the pre-admission clinic visit, participants were asked by study investigators to complete a 26-item questionnaire to collect demographic and clinical information, including sex, age, analgesia use, average pain intensity over the past 24 hours, residential location, identification as an Aboriginal or Torres Strait Islander, orthopaedic procedure conducted, education level, employment status and relevant psychological and social background. Orthopaedic procedures classified as ‘other’ included Achilles tendon repair, ankle replacement, removal of clavicle plate, revision of total knee replacement, revision of total hip replacement and unilateral metatarsal replacement.
Residential location by postcode was used to determine indicators of residential remoteness and socioeconomic decile. The Australian statistical geography standard-remoteness area (ASGS-RA) was used to classify participants’ residential remoteness. 14 Values ranged from 1 to 6, where 1 indicated a major city of Australia, 2 indicated inner regional Australia, 3 indicated outer regional Australia, 4 indicated remote Australia, and 5 indicated very remote Australia. We also used the ASGS-RA to classify hospitals located in a major city, inner regional, outer regional or remote area of Australia. 14 the index of relative socioeconomic disadvantage (IRSD) was used to classify socioeconomic decile, where decile 1 indicated the greatest disadvantage and decile 10 indicated the least disadvantage. 15
Psychological and social background data were collected using validated tools. These included the measurement of depressive traits using the two-item patient health questionnaire (PHQ-2) 16 and anxiety traits were collected using the generalised anxiety disorder questionnaire (GAD-2) 17 by taking the mean score on a five-point Likert scale. Individuals at risk of substance use disorder were assessed by taking the mean score of the five-item screener and opioid assessment for patients with pain (SOAPP-R version 1.0-SF). 18
Further details on baseline data collection are available in a previous publication which focused on preoperative opioid use. 19
Postoperative data collection
Participants were followed up by telephone or email by study investigators between 90 and 150 days after surgery and asked to complete a four-item questionnaire to collect information on average pain intensity over the past 24 hours, and opioid use.
Opioid use was defined as the use of buprenorphine, codeine, fentanyl, hydromorphone, methadone, morphine, tapentadol or tramadol. Formulations used for opioid use disorder (liquid methadone and sublingual buprenorphine), antidiarrhoeal and antitussive purposes were excluded. We classified opioid use as ‘daily’ and ‘any’ opioid use. Daily opioid use was defined as the use of opioids every day over the previous 2 weeks or longer. Any opioid use was defined as the use of opioids to any extent, including daily opioid use as well as when-required opioid use over the previous 2 weeks or longer. For ‘daily’ and ‘any’ opioid use, we calculated the daily oral morphine milligram equivalent (MME) dose using equianalgesic factors recommended by the Australian and New Zealand College of Anaesthetists. 20 Doses taken ‘when-required’ were accounted for by calculating the average consumption over one week to determine a daily equivalent quantity.
Average pain intensity over the 24 hours prior to questionnaire administration was collected using an 11-point numerical pain rating scale, 21 in which integers from 0 to 10 were used and a score of 0 indicated no pain and 10 indicated the worst imaginable pain.
Sample size
A sample size calculation was conducted to identify a representative sample of patients attending the five study hospitals using methodology described by Krejcie and Morgan. 22 We assumed a margin of error of 5%, a confidence level of 95%, and the proportion of the population with the expected outcome of 50%. The required sample size to be representative of approximately 3000 patients undergoing elective orthopaedic surgery at the five study hospitals during the study period 23 was 341 patients. Accounting for a 5% rate of patients lost to follow-up based on previous literature, 8 we aimed to recruit 359 participants.
Data analysis
Descriptive statistics were reported for patient demographics and opioid use at 90 days postoperatively. Differences between participants who did or did not use opioids at 90 or more days after surgery were examined using univariate analysis. Categorical variables were compared using the chi-squared test. If any cells contained an expected frequency of less than five, the Fisher’s exact test was used to compare categorical variables. Continuous variables were not normally distributed, thus were analysed using the Mann–Whitney U test. Prespecified subgroup analyses were performed to identify rates of postoperative opioid use among patients who were opioid naïve before elective orthopaedic surgery.
Multivariable logistic regression was conducted to examine the association between hospital location and postoperative opioid use at 90 days following orthopaedic surgery while accounting for known covariates. Based on existing literature, covariates included age, 24 baseline anxiety, 8 tobacco use,5,9 preoperative opioid use,5,9 preoperative use of drugs of addiction 10 and higher postoperative pain scores. 8 Collinearity between variables in the model was evaluated using a tolerance value set at greater than 0.1. A sensitivity analysis was conducted to examine whether statistically significant clustering existed by hospital site.
Analyses were conducted using IBM SPSS Statistics version 27 software (IBM, Armonk, NY, USA). A P value of less than 0.05 was considered statistically significant.
Results
Of the 561 patients assessed for eligibility preoperatively, 506 patients were eligible (Figure 1). There were 76 patients who declined participation and 430 participants enrolled in the study. There were 11 participants who had their surgery cancelled and 58 participants were lost to follow-up, resulting in 361 participants included in the analysis. The mean age was 67.7 years (standard deviation (SD) 10.1 years) and 195 (54%) were women. Approximately 63% (228/361) of participants attended a public hospital and 37% (133/361) attended a private hospital. The most common orthopaedic procedures were unilateral total knee replacement (56.8%, 205/361) and unilateral total hip replacement (28.5%, 103/361). The rates of orthopaedic procedures conducted at each hospital site are reported in Supplementary Table 1. Most participants resided in a remoteness classification 2 area (57.9%, 209/361) or classification 1 area (30.7%, 111/361). The majority of participants resided in areas of socioeconomic decile 1 (28%, 101/361), decile 2 (20.2%, 73/361) or decile 3 (12.5%, 45/361). A history of chronic pain was reported in 269 participants (74.5%) and the mean preoperative pain score was 5 (SD 2.7, Table 1).
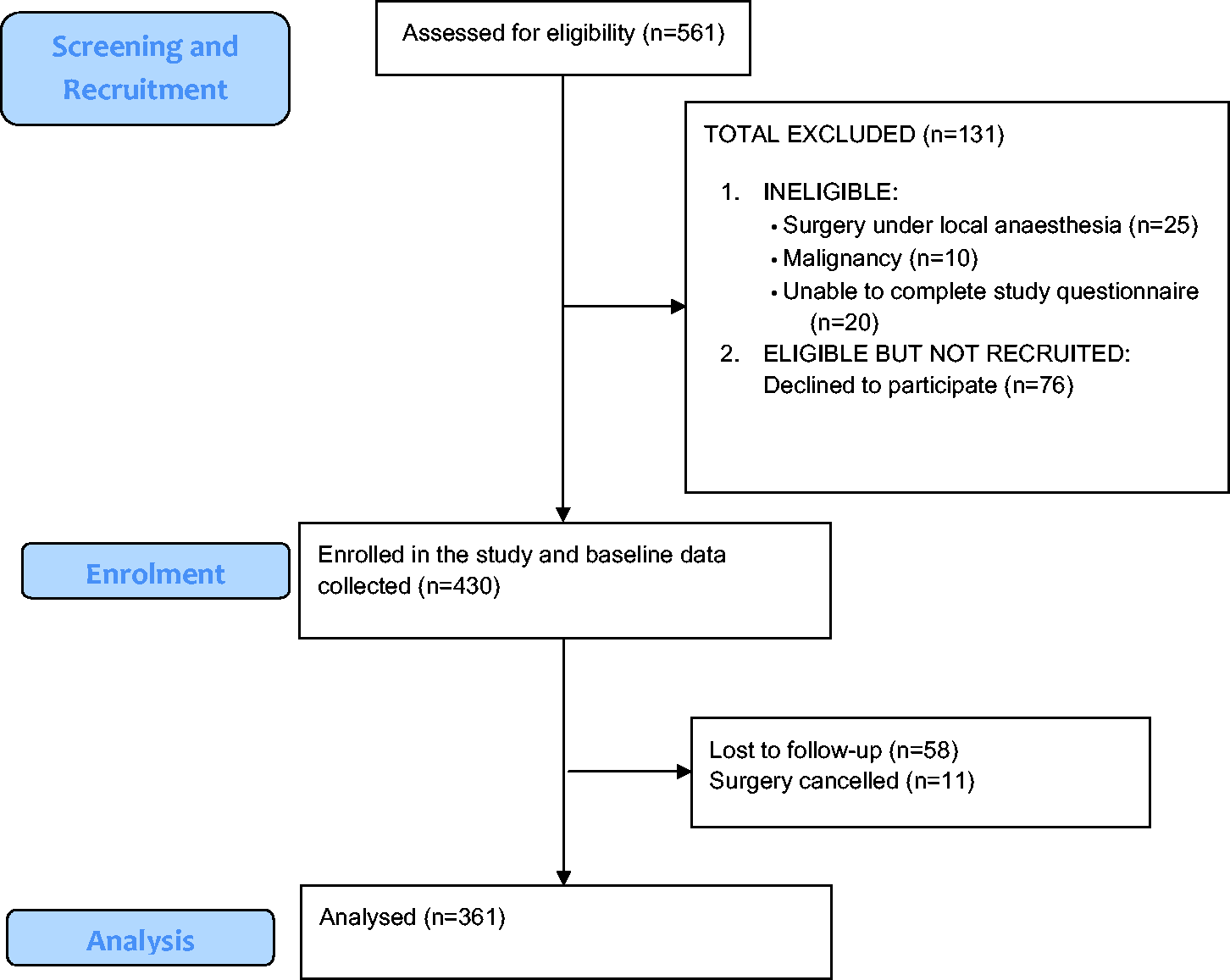
Study flow diagram.
Characteristics and univariate analysis to compare patients who did or did not report postoperative opioid use 90 days or more after elective orthopaedic surgery.
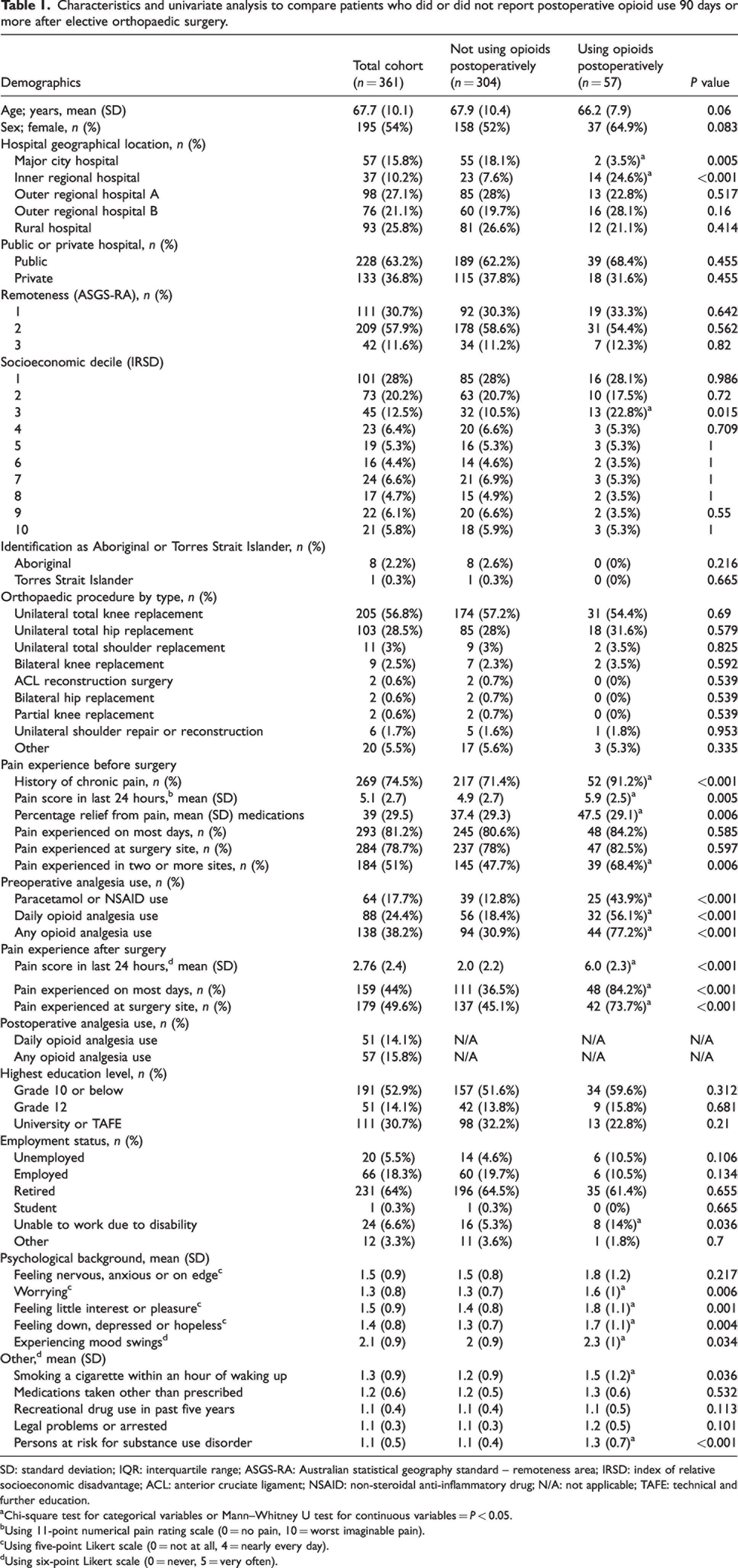
SD: standard deviation; IQR: interquartile range; ASGS-RA: Australian statistical geography standard – remoteness area; IRSD: index of relative socioeconomic disadvantage; ACL: anterior cruciate ligament; NSAID: non-steroidal anti-inflammatory drug; N/A: not applicable; TAFE: technical and further education.
Chi-square test for categorical variables or Mann–Whitney U test for continuous variables = P < 0.05.
Using 11-point numerical pain rating scale (0 = no pain, 10 = worst imaginable pain).
Using five-point Likert scale (0 = not at all, 4 = nearly every day).
Using six-point Likert scale (0 = never, 5 = very often).
The primary outcome, postoperative opioid use, was reported in 57 participants (15.8%; 95% CI 12.2–20%) and of these, 51 participants (14.1%; 95% CI 10.7–18.2%) reported daily opioid use at 90 days or more following orthopaedic surgery (Table 1). The rates of postoperative opioid use among participants 90 days or more after surgery were 3.5% (2/57) at the major city hospital, 37.8% (14/37) at the inner regional hospital, 13.3% (13/98) at outer regional hospital A, 21.1% (16/76) at outer regional hospital B and 12.9% (12/93) at the rural hospital (Supplementary Table 2). There were 223 opioid naïve patients prior to orthopaedic surgery, of whom 5.8% (13/223) reported opioid use to some degree and 3.6% (8/223) reported daily opioid use at 90 days or more postoperatively (Supplementary Table 3). The most frequently used opioids postoperatively were codeine (57.9%, 33/57), oxycodone (29.8%, 17/57) and tramadol (14%, 8/57). The median postoperative opioid consumption in oral MME per day was 15.6 (IQR 23.4, range 3.33–300, Supplementary Table 4).
Multivariable logistic regression showed that participants who underwent surgery in an inner regional hospital (adjusted odds ratio (aOR) 12.26; 95% CI 2.2–68.24) and an outer regional location (aOR 5.46; 95% CI 1.09–27.50) were more likely to use opioids more than 90 days after orthopaedic surgery compared with participants who attended a major city hospital, after adjusting for known covariates including baseline anxiety, preoperative opioid use and postoperative pain score. The Hosmer–emeshow test indicated a good fit of the data to the logistic regression model (P > 0.05, Table 2). 25 A sensitivity analysis to examine potential clustering by hospital site showed no significant clustering by hospital site (P > 0.05).
Multivariable logistic regression analyses for predictors and covariates of postoperative opioid use 90 days or more after elective orthopaedic surgery.
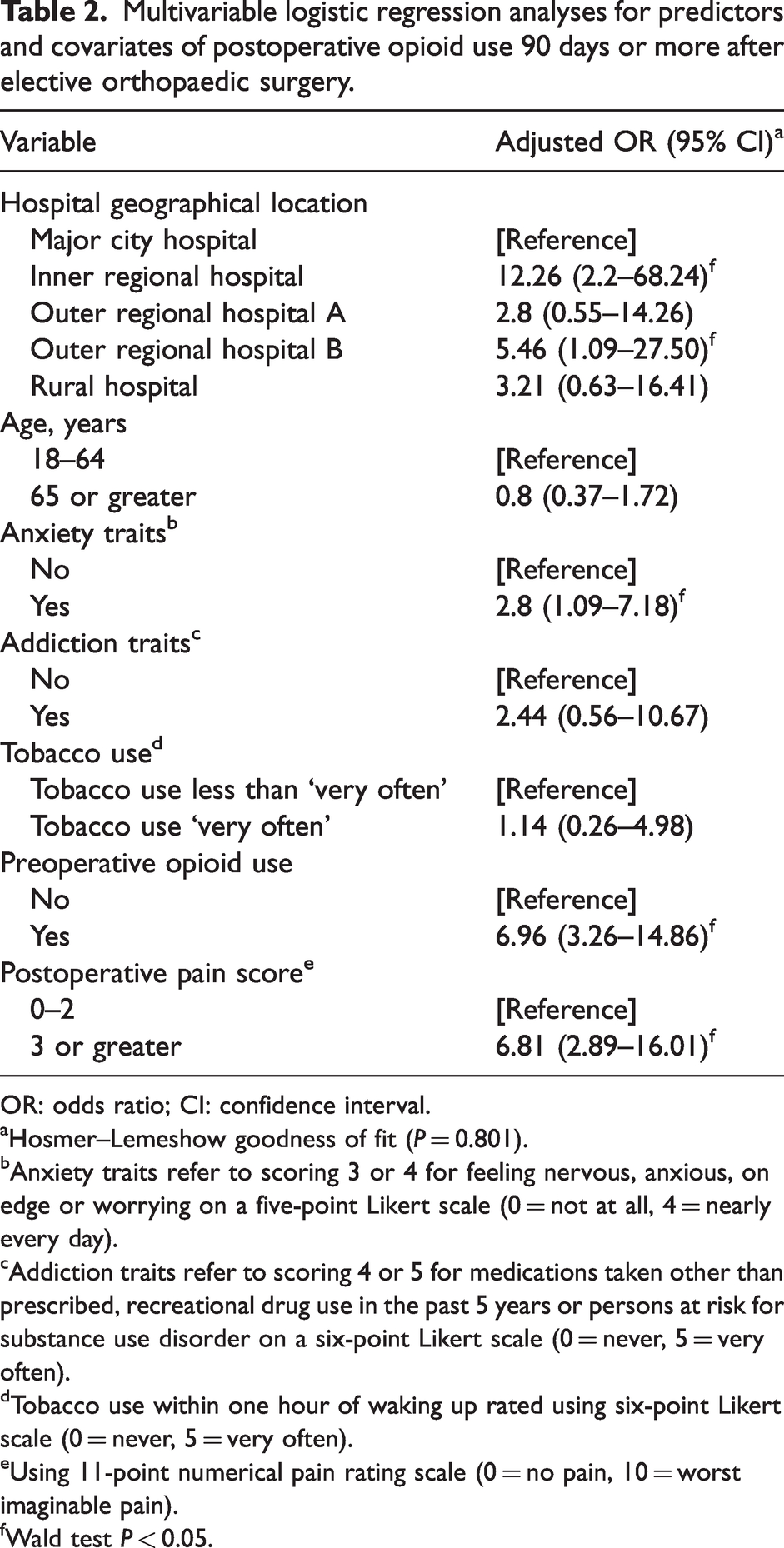
OR: odds ratio; CI: confidence interval.
Hosmer–Lemeshow goodness of fit (P = 0.801).
Anxiety traits refer to scoring 3 or 4 for feeling nervous, anxious, on edge or worrying on a five-point Likert scale (0 = not at all, 4 = nearly every day).
Addiction traits refer to scoring 4 or 5 for medications taken other than prescribed, recreational drug use in the past 5 years or persons at risk for substance use disorder on a six-point Likert scale (0 = never, 5 = very often).
Tobacco use within one hour of waking up rated using six-point Likert scale (0 = never, 5 = very often).
Using 11-point numerical pain rating scale (0 = no pain, 10 = worst imaginable pain).
Wald test P < 0.05.
Discussion
This prospective, observational cohort study examined the prevalence of long-term opioid use after elective orthopaedic surgery across Australian major city, regional and rural locations. We identified that 15% (57/361) of patients continued to use opioids after 90 days following elective orthopaedic surgery, with significant variation between major city and regional or rural locations in Australia. Our findings are consistent with rates of long-term postoperative opioid use following orthopaedic surgery reported in other studies. A systematic review and meta-analysis of 15 studies including 416,321 patients reported a pooled rate of opioid use at 90 or more days following total joint arthroplasty of 12% (95% CI 10–14%). 5 This reinforces the external validity of our findings. However, there is notable variation in rates of long-term postoperative opioid use following orthopaedic surgery in the literature, with reported prevalence ranging from 5.2% (787/15,020) 26 to 41.2% (9993/23,726). 3 These differences may be explained in part by the study methods used, such as analysis of insurance claims data, which may not accurately reflect actual opioid consumption. 3 However, there are numerous patient and context-specific predictors for long-term postoperative opioid use which may further explain this variability. 5 A better understanding of these predictors may facilitate the improved management of postoperative pain and minimise unintended progression into long-term opioid use, as well as the associated harms of long-term opioid use.
One such context-specific predictor for long-term opioid use after orthopaedic surgery identified in this study was geographical location. Our findings support data from the 2015 Australian Atlas of Healthcare Variation, which reported over a 10-fold difference between areas with the highest and lowest numbers of opioid prescriptions dispensed under the pharmaceutical benefits scheme. Furthermore, opioid dispensing rates were found to be higher in inner and outer regional areas compared with major city or remote areas. Our study suggests that the regional variation observed in total opioid dispensing patterns appears to extend to rates of long-term postoperative opioid use. Compared with a major city setting, the inner regional location was associated with 12 times higher odds and the outer regional location was associated with five times higher odds of long-term postoperative opioid use. Geographical differences in long-term opioid use following orthopaedic surgery have also been identified in a study conducted in the USA. Best and colleagues analysed 5676 patients who underwent elective primary total shoulder arthroplasty and reported that undergoing surgery in the western USA was associated with 1.8 times higher odds of long-term postoperative opioid use (95% CI 1.3–2.4). 11 Our study adds to the existing literature by demonstrating that regional location also appears to be a predictor of long-term postoperative opioid use in the Australian context. The association between regional location and long-term postoperative opioid use may be explained by limited access to health services, socioeconomic disadvantage and a greater prevalence of known covariates of long-term opioid use including preoperative opioid use and baseline anxiety compared with major city locations. However, regional location remained a predictor of long-term postoperative opioid use even after controlling for these covariates in our study, which suggests other factors such as local prescribing practices and attitudes towards opioid use may also be contributors. Further studies to address the identified variation in postoperative pain management, particularly in regional and rural Australian locations, are warranted.
Interventions to manage patient-specific factors linked with long-term postoperative opioid use may reduce the risk of long-term opioid use and associated harms. Previous studies have reported that preoperative opioid use is the strongest predictor of long-term opioid use following total joint arthroplasty.5,27 Similarly, our findings also show that the greatest patient-specific risk factor for long-term opioid use after orthopaedic surgery is preoperative opioid use (aOR 6.96; 95% CI 3.26–14.86). Although the mechanism underlying this link is unclear, patients already taking opioids prior to surgery may experience a greater degree of opioid tolerance, dependence or opioid-induced hyperalgesia during the postoperative period, subsequently increasing the risk of long-term postoperative opioid use. 28 In addition, preoperative opioid use is also associated with higher postoperative opioid requirements (46 mg vs. 366 mg mean MME, P < 0.001), 29 worse surgical outcomes (OR 6.15; 95% CI 1.46–25.95), 29 longer length of hospital stay (2.5 days vs. 2.8 days, P < 0.001), 30 increased 30-day hospital readmission rate (3.1% vs. 3.7%, P < 0.001) 30 and higher healthcare costs at 90-days postoperatively (US$12,036.60 vs. US$3863.40, P < 0.001). 30 A retrospective study reported that patients who reduced the quantity of opioids used by at least 50% had greater improvements in disease-specific and generic health outcomes compared with patients who remained on the same opioid dose prior to orthopaedic surgery. 31 However, prospective literature describing interventions to reduce opioid use prior to surgery are limited. 32 Therefore, high-quality studies examining the efficacy of interventions on the reduction of opioid use prior to surgery and outcomes following surgery are required.
The strengths of our study include the prospective, longitudinal design which facilitated follow-up of the same cohort after surgery. This study was conducted across major city, regional and rural geographical locations in Australia, which enhanced the generalisability of our findings. The collection of data by telephone allowed confirmation of opioid use and dosage, which may more accurately reflect patterns of opioid use compared with the audit of insurance claims or dispensing records. However, this study had several limitations. The use of patient self-reported data is subject to response bias and recall bias. We were unable to capture the prevalence of opioid tolerance and dependence, as well as other comorbid conditions besides chronic pain at baseline. The major city hospital location was represented by a major city private hospital and the regional and rural hospitals were predominantly public hospitals which may affect the study findings. The use of a more robust and validated scale to capture tobacco use, such as the Diagnostic and Statistical Manual of Mental Disorders, 5th edition, 33 may improve the accuracy of the data. We did not collect the indication for opioid use before or after surgery, which may lead to the over-representation of the reported rates of opioid use among the cohort. We collected data over a few years during which prescribing practices may have fluctuated due to the introduction of policy and regulation changes over this period. There may have been unmeasured factors contributing towards long-term postoperative opioid use, such as local prescribing practices and local perceptions or attitudes towards opioid use. Finally, these data originated from hospital locations within New South Wales, Australia, thus the generalisability of our findings to other settings is unknown.
In summary, long-term opioid use was reported in 15% of patients who underwent orthopaedic surgery. These rates varied significantly between major city, regional and rural locations in Australia. The regional location was identified as a key predictor of long-term opioid use following orthopaedic surgery. Understanding the local context when addressing predictors for long-term postoperative opioid use may facilitate the improved management of pain among patients undergoing orthopaedic surgery.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X231172790 - Supplemental material for Prevalence and predictors of long-term opioid use following orthopaedic surgery in an Australian setting: A multicentre, prospective cohort study
Supplemental material, sj-pdf-1-aic-10.1177_0310057X231172790 for Prevalence and predictors of long-term opioid use following orthopaedic surgery in an Australian setting: A multicentre, prospective cohort study by Shania Liu, Jennifer A Stevens, Ashleigh E Collins, Jed Duff, Joanna R Sutherland, Morgan D Oddie, Justine M Naylor, Asad E Patanwala, Benita M Suckling and Jonathan Penm in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The authors acknowledge the assistance provided by Laura Hunter, nurse unit manager, for her contribution to the study, as well as the statistical consulting service provided by Alex Shaw from the Sydney Informatics Hub, a core research facility of the University of Sydney.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the St Vincent’s Hospital Human Research Ethics Committee (LNR/17/SVH/155).
Funding
The authors (SL, JAS, JMN, AEP and JP) are partly supported by an AVANT research foundation grant. Shania Liu is supported by a NHMRC postgraduate scholarship and Prince of Wales foundation grant. These funding sources had no role in the design of the study, data collection and analysis or preparation of the manuscript. The remaining authors declare no funding sources.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.