
Abstract
The cerebrospinal fluid volume affects the block height of spinal anaesthesia. Laminectomy of the lumbar spine may result in increased lumbosacral cerebrospinal fluid volume. This study aimed to test the hypothesis that the lumbosacral cerebrospinal fluid volume of patients with a history of lumbar laminectomy would be larger than that of patients with normal lumbar spine anatomy using magnetic resonance imaging. Lumbosacral spine magnetic resonance images of 147 patients who underwent laminectomy at the L2 vertebrae or below (laminectomy group) and 115 patients without a history of spinal surgery (control group) were retrospectively reviewed. The lumbosacral cerebrospinal fluid volumes between the L1–L2 intervertebral disc level and the end of the dural sac were measured and compared between the two groups. The mean (standard deviation) lumbosacral cerebrospinal fluid volume was 22.3 (7.8) ml and 21.1 (7.4) ml in the laminectomy and control groups, respectively (mean difference 1.2 ml; 95% confidence interval −0.7 to 3.0 ml; P = 0.218). In the prespecified subgroup analysis according to the number of laminectomy levels, patients who underwent more than two levels of laminectomy exhibited slightly larger lumbosacral cerebrospinal fluid volume (n = 17, 30.5 (13.5) ml) compared with those who underwent two (n = 40, 20.7 (5.6) ml; P = 0.014) or one level of laminectomy (n = 90, 21.4 (6.2) ml; P = 0.010) and the control group (21.1 (7.4) ml; P = 0.012). In conclusion, the lumbosacral cerebrospinal fluid volume did not differ between patients who underwent lumbar laminectomy and those without a history of laminectomy. However, patients who underwent laminectomy at more than two levels had a slightly larger volume of lumbosacral cerebrospinal fluid than those who underwent less extensive laminectomy and those without a history of lumbar spine surgery. Further studies are warranted to confirm the subgroup analysis findings and elucidate the clinical implications of such differences in the lumbosacral cerebrospinal fluid volume.
Introduction
Spinal anaesthesia is widely used to provide anaesthesia for lower body surgery. However, spinal anaesthesia failure occurs in 3.2%–3.9% of patients1,2 Various factors associated with local anaesthetics, procedures, and patients affect the block level during spinal anaesthesia. In particular, the lumbosacral cerebrospinal fluid (CSF) volume is a major factor determining the block level of spinal anaesthesia. 3 Although the lumbosacral CSF volume varies among patients according to the body habitus, 4 acquired changes in the lumbosacral CSF volume can also affect the distribution of the local anaesthetic and extent of spinal anaesthesia. 5
Laminectomy of the lumbar spine is the most common procedure performed in spinal and neurological surgeries. Laminectomy can affect the lumbosacral CSF volume by eliminating the posterior portion of the spinal canal that surrounds the dural sac. However, the influence of previous laminectomy on lumbosacral CSF volume has rarely been evaluated. Although recent studies reported that patients who underwent lumbar spine surgery showed an increase in the thecal sac diameter on magnetic resonance imaging (MRI),6,7 these findings did not reflect the postoperative changes in the lumbosacral CSF volume, which is directly related to the distribution of the local anaesthetic during spinal anaesthesia. Moreover, no data exist on the influence of the extent of laminectomy on the CSF volume.
We performed this retrospective observational study to investigate the effect of laminectomy and the number of laminectomy levels on the lumbosacral CSF volume using MRI data. We hypothesised that the lumbosacral CSF volume of patients who underwent lumbar laminectomy would be larger than that of the patients without a history of lumbar spine surgery.
Materials and methods
Ethical approval for this retrospective imaging study was obtained from the Institutional Review Board of Seoul National University Hospital, Seoul, Korea (ref. 2011-153-1176) on 27 November 2020. Written informed consent was waived by the Institutional Review Board of Seoul National University Hospital because of the retrospective nature of the study. This study was conducted in adherence with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
We reviewed the electronic medical records of adult patients (age ≥19 years) who underwent lumbar spine MRI scans at the Seoul National University Hospital between January 2009 and December 2018. The history of laminectomy was determined based on the official MRI and surgical records. The exclusion criteria were as follows: presence of anatomical anomalies, absence of data on resected lamina levels, insufficient MRI coverage (MRI performed using protocols that focused on the intervertebral area or not containing the end of the dural sac), and irrelevant surgeries (thoracic laminectomies or L1 laminectomies). Cases with unknown height or weight of the patient at the time of scanning, and those with poor image quality were also excluded. Thereafter, MRI scans from healthy participants of the same number as patients with a history of lumbar laminectomy were randomly extracted for a 1:1 comparison.
Surgical records were reviewed to confirm the number of laminectomy levels. Data on the patient age, height, weight, type and site of surgery, date of surgery, and date of the MRI images were also obtained from the electronic medical records.
Measurements
The lumbosacral CSF volume was calculated from the MRI data obtained with the patient in the supine position. The cross-sectional area of the CSF component was calculated by subtracting the conus medullaris area from the dural sac area in each transverse T2-weighted MRI section using the Picture Archiving and Communication System (INFINITT Healthcare Co. Ltd., Seoul, Korea) (Figure 1). To calculate the segmental CSF volume between two transverse sections, the average of the two CSF areas was multiplied by the height (the sum of the layer thickness and the distance between the layers). 8 The total lumbosacral CSF volume was obtained by adding the segmental CSF volumes between the L1–L2 intervertebral disc levels and the end of the dural sac. The number of laminectomy levels was defined as the sum of all the laminectomy levels. The maximum number of laminectomy levels was four as L1 laminectomy was excluded because of the lumbosacral spine MRI protocol in our institution not covering the interspace between the L1 and L2 vertebrae. All the measurements were conducted by one investigator (YH) to minimise inter-observer variation.
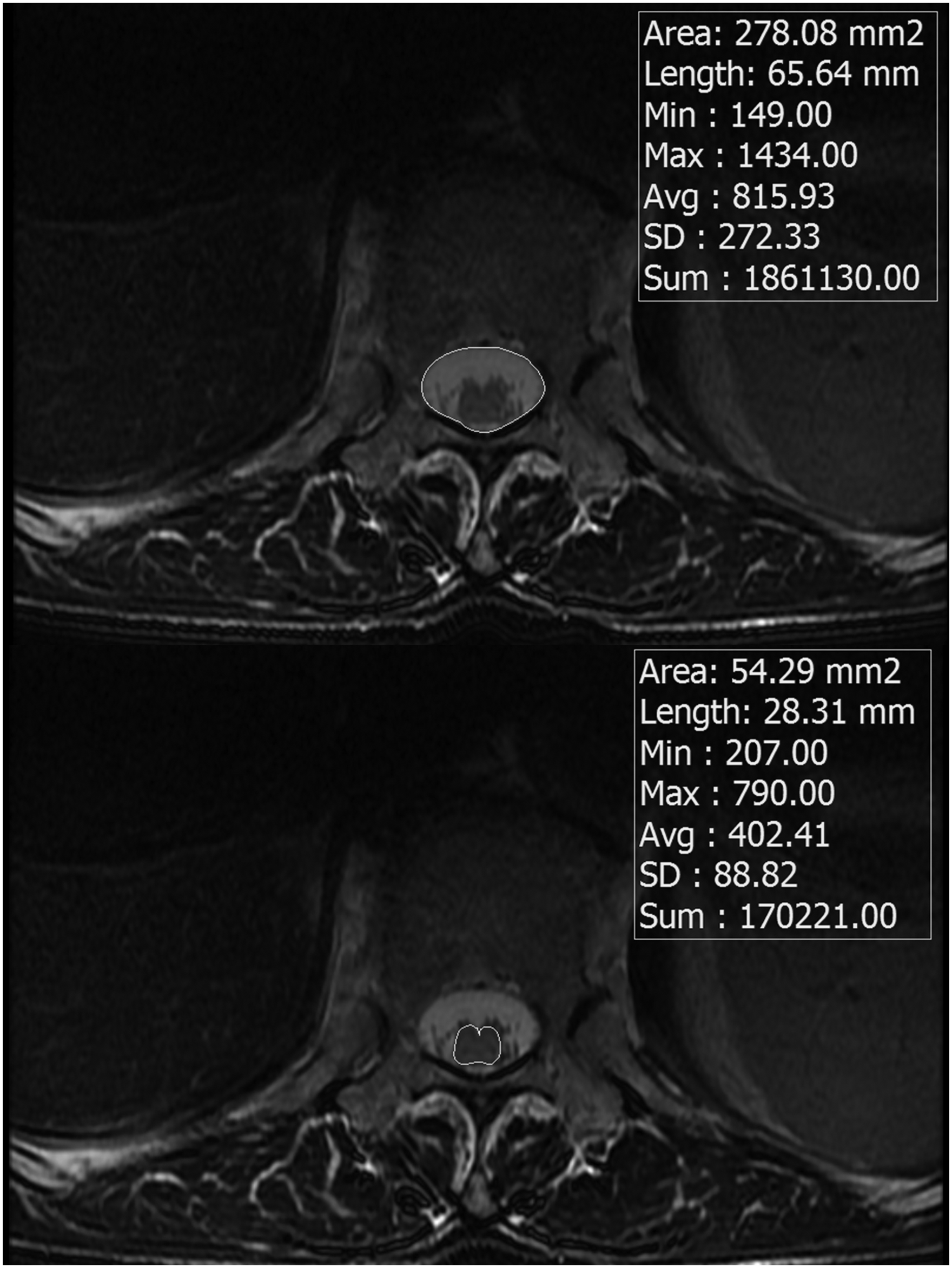
Examples of T2-weighted transverse images (L1–L2 intervertebral disc level). The conus medullaris area (below) was subtracted from the dural sac area (above) to determine the cerebrospinal fluid (CSF) area.
Statistical analysis
The sample size was determined based on the available data from the patients during the study period without a prior power calculation. Continuous variables are presented as mean (standard deviation) or median (interquartile range, IQR) and compared using an independent-samples t-test or Mann–Whitney U test following normality assessment using the normal quantile-quantile plot. Categorical variables are presented as numbers (percentages) and were compared using Pearson’s chi-square test.
To evaluate the impact of the surgical extent on the lumbosacral CSF volume, the laminectomy group was divided according to the number of laminectomy levels, and subgroup analyses were performed between these groups and the control group. One-way analysis of variance or the Kruskal–Wallis test was used for the subgroup analyses, and post hoc analyses were performed using an independent-samples t-test or Mann–Whitney U test with Bonferroni correction.
All analyses were performed using R software version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria); statistical significance was set at P <0.05.
Results
A total of 432 MRI scans from patients with a history of laminectomy were acquired. Among them, 285 scans were excluded because of insufficient MRI scan coverage (n = 200), a history of laminectomy of other parts of the spine (thoracic laminectomy, sacral laminectomy, or L1 laminectomy; n = 29), missing height or weight at the time of scanning (n = 27), presence of anatomical anomalies (n = 15), unclear MRI images (n = 10), and insufficient surgical records (n = 4). The remaining 147 scans from the patients who underwent lumbar spine surgery were included, as were 115 out of 147 scans from normal participants (Figure 2). Patient characteristics are presented in Table 1; no statistically significant differences were observed in the variables with the exception of the number of resected laminae. The median time interval between lumbar spine surgery and MRI scans was 24 (IQR 4–60) months.
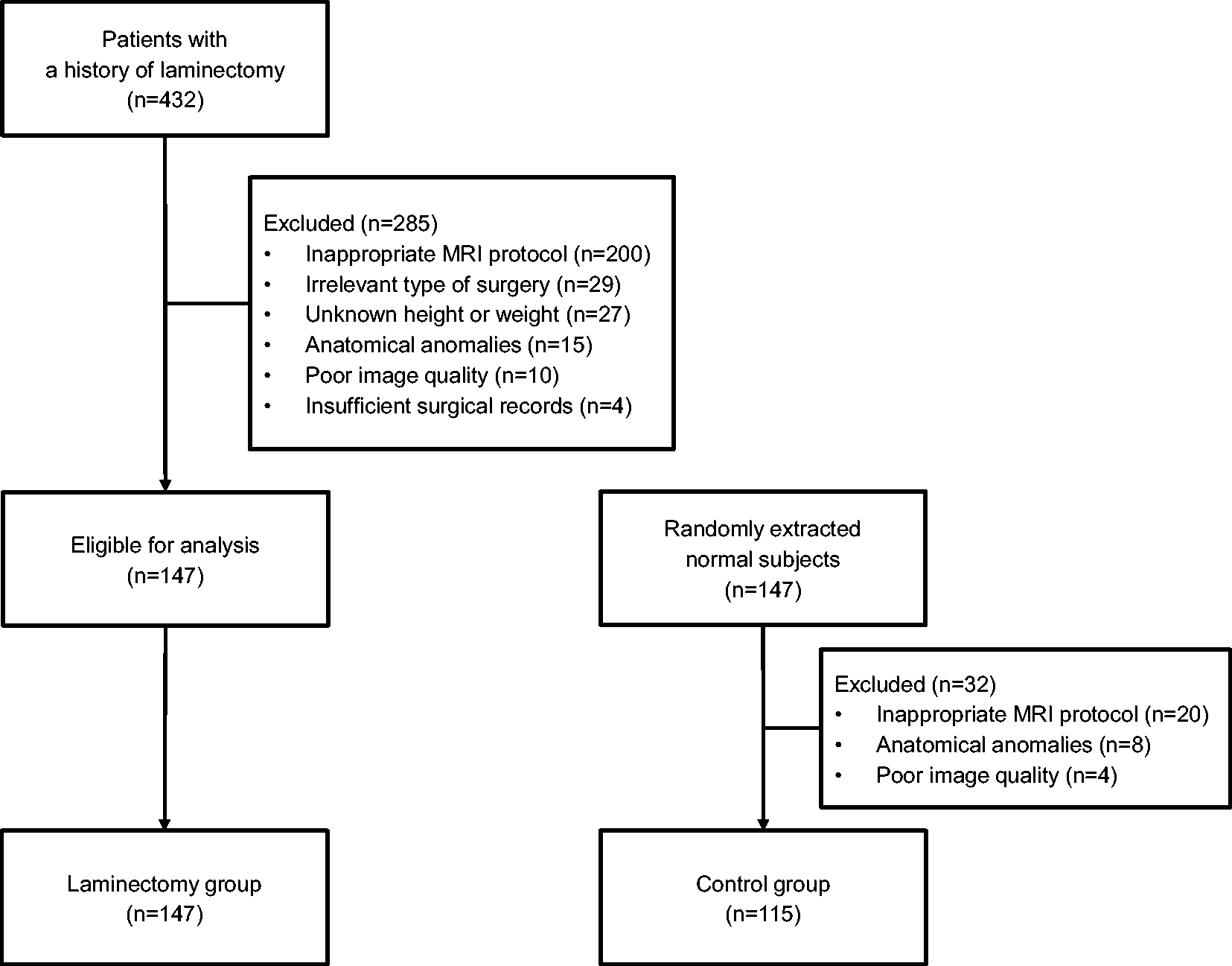
Study flowchart.
Patient characteristics.
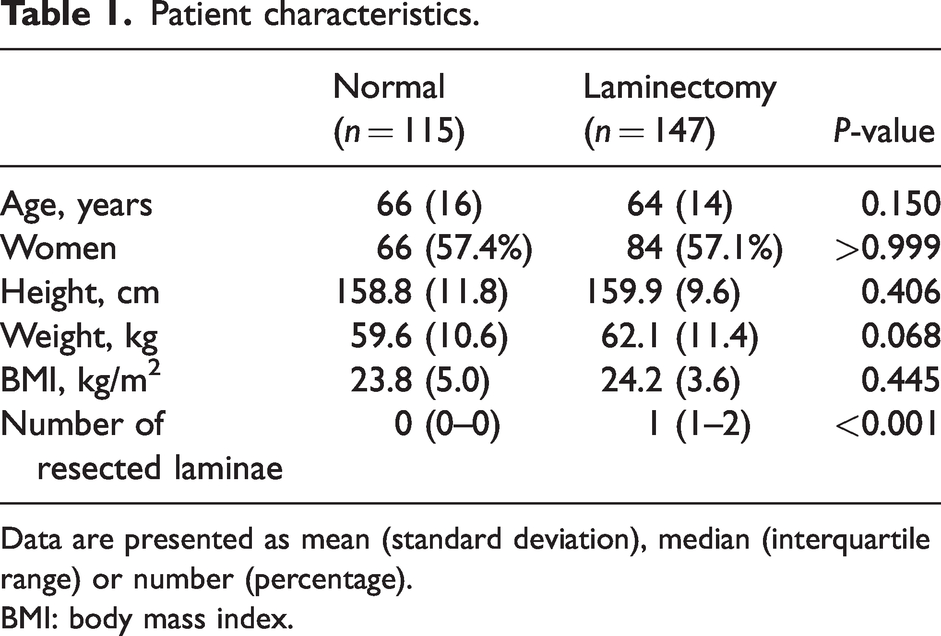
Data are presented as mean (standard deviation), median (interquartile range) or number (percentage).
BMI: body mass index.
In the laminectomy group, the median number of resected laminae was 1 (IQR 1–2) (Table 1). The mean lumbosacral CSF volumes were 22.3 (7.8) ml and 21.1 (7.4) ml in the laminectomy and control groups, respectively (mean difference 1.2 ml; 95% confidence interval −0.7 to 3.0 ml; P = 0.218). The volume of the lumbosacral CSF divided by the height or weight also did not significantly differ between the laminectomy (0.14 (0.04) ml/cm) and control (0.13 (0.04) ml/cm; P = 0.254) groups. There was no statistically significant difference in the lumbosacral CSF volume divided by the weight between the laminectomy (0.37 (0.13) ml/kg) and control (0.36 (0.15) ml/kg; P = 0.900) groups.
The results from the subgroup analyses are presented in Table 2. The most frequent site of laminectomy was the L4 vertebra (Table 2). The subgroup analysis revealed that the lumbosacral CSF volume was significantly larger in patients who had undergone more than two levels of laminectomy (30.5 (13.5) ml) than in those who had undergone two levels (20.7 (5.6) ml; P = 0.014) or one level of laminectomy (21.4 (6.2) ml; P = 0.010) and the control group (P = 0.012) (Table 2). The volume of the lumbosacral CSF divided by height or weight was also significantly larger in patients with a history of more than two levels of laminectomy compared with other subgroups (Table 2). There was no statistically significant difference in the lumbosacral CSF volumes between the other subgroups and the control group.
The results of subgroup analysis according to the number of resected laminae.
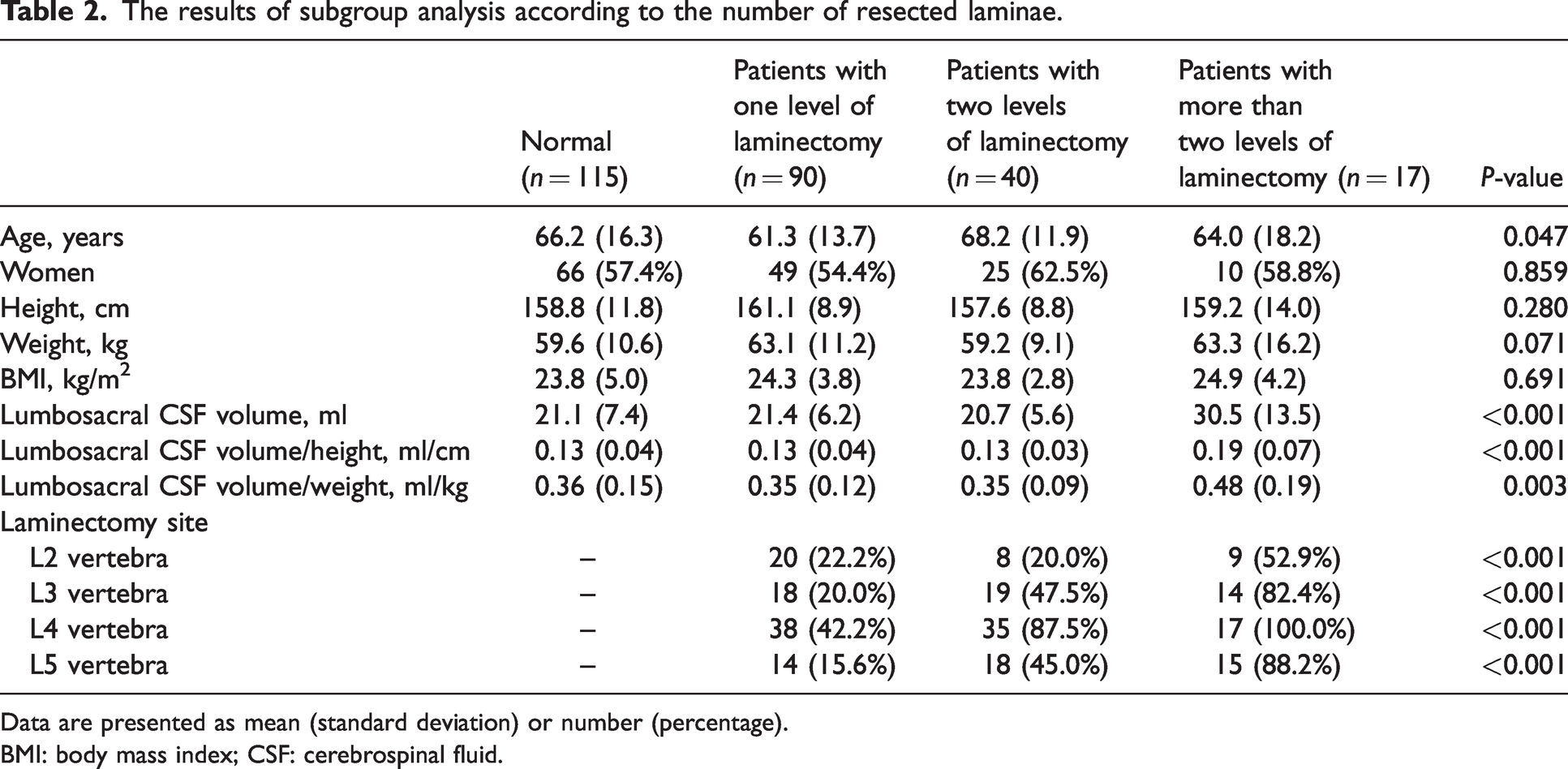
Data are presented as mean (standard deviation) or number (percentage).
BMI: body mass index; CSF: cerebrospinal fluid.
Discussion
We evaluated the influence of laminectomy and its extent on the lumbosacral CSF volume. Taken together, the lumbosacral CSF volume did not differ between the patients who underwent lumbar laminectomy and those without a history of laminectomy regardless of the level of laminectomy. However, the images of the patients who had undergone more than two levels of lumbar laminectomy exhibited a slightly larger lumbosacral CSF volume compared with those with a less extensive laminectomy and those without a history of laminectomy.
As the volume of lumbosacral CSF is a major factor determining the extent of block following spinal anaesthesia,3,9 the administration of a relatively small dose of local anaesthetic compared with the lumbosacral CSF volume could result in an inadequate sensory block following spinal anaesthesia. If patients with a history of extensive lumbar laminectomy had a larger volume of lumbosacral CSF, anaesthetic dose adjustment may be required. However, further clinical studies with a large sample size are warranted to confirm this finding and clarify the clinical implications of such a difference in the lumbosacral CSF volume.
Lumbar surgeries, such as laminectomy, could affect the lumbosacral CSF volume, which is the diluent for the local anaesthetic during spinal anaesthesia as the lamina surrounding the dural sac posteriorly could be resected during surgery. Recent studies have reported that the cross-sectional area of the dural sac expanded significantly following lumbar surgery.6,7 Our findings that multilevel lumbar laminectomy increases the volume of lumbosacral CSF is consistent with previous results and may have clinical implications, such as the possibility of anaesthetic dose modification when performing spinal anaesthesia in these patients; however, further clinical investigations are warranted.
One possible explanation for this finding is the gradual expansion of the dural sac at the lumbosacral area posteriorly through the resected laminae. In a previous study, lumbar laminectomy reportedly resulted in the posterior shift of the dural sac because of a loose connection between the posterior longitudinal ligament and anterior dura mater. 10 Although we did not measure the distance between the vertebral body and dural sac, similar mechanisms could contribute to the increase in the CSF volume in the lumbosacral region, which is most affected by gravity in the standing position. Considering that a significant increase in the lumbosacral CSF volume was only found in patients with a history of more than two levels of lumbar laminectomy, the relationship between the number of laminectomy levels and the lumbosacral CSF volume could be non-linear. Further studies with a larger sample size are warranted to confirm the relationship between the extent of lumbar surgeries and the lumbosacral CSF volume.
Changes in the lumbosacral CSF volume can alter the response to spinal anaesthesia. CSF aspiration reportedly results in a higher level of sensory block during spinal anaesthesia. 5 Considering the inverse correlation between the lumbosacral CSF volume and peak sensory block level, 11 our results suggest that higher doses of local anaesthetic may be required in patients who undergo lumbar laminectomy at more than two levels to achieve an adequate level of blockade equivalent to that in the normal group. Further studies are warranted to determine the optimal dose of local anaesthetic for spinal anaesthesia in this population.
This study had several limitations. First, although this study demonstrated the influence of a large extent of lumbar laminectomy on the lumbosacral CSF volume, this finding was only explorative considering its retrospective nature and the absence of a power calculation. In addition, the influence of laminectomy on the spinal block extent was not evaluated in a clinical setting. Second, although we found a significant increase in the lumbosacral CSF volume in patients with a history of more than two levels of laminectomy, only 17 patients with a history of more than two levels of laminectomy were included, thereby increasing the probability of a random finding. Third, when calculating the lumbosacral CSF volume, the cross-sectional area of the cauda equina was not considered. Fourth, as we did not include patients who had undergone L1 laminectomy, our study findings are not generalisable to this patient subset. Finally, as the MRI data were acquired using various MRI machines with different magnetic field strengths, variations in the measured values could exist.
In conclusion, this MRI study found no statistically significant difference in the lumbosacral CSF volume between patients who underwent laminectomy and those without a history of lumbar spine surgery. However, the magnetic resonance images of the patients with more than two levels of laminectomy showed a slightly larger lumbosacral CSF volume than that noted in those with less extensive laminectomy or the control group. Further investigations are warranted to confirm the subgroup analysis findings and elucidate the clinical implications of such differences in the lumbosacral CSF volume.
Footnotes
Author Contributions
Data sharing statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.