
Abstract

Carly Wright, Greg R McAnulty, and Paul J Secombe. The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study. Anaesth Intensive Care 2021; 49: 35–43.
The authors of this paper 1 neglected to include in the abstract and methods sections a clear articulation that the dataset used for the study overlaps with several other publications. In order to be consistent with the International Committee of Medical Journal Editors policy on overlapping data, the authors provide this corrigendum.
Our original intent had been a prospective study describing the epidemiology of critical care admissions in the Northern Territory (NT), not having anticipated changes in alcohol harm minimisation policy introduced by the NT government halfway through the study. That study became “Alcohol Misuse and Critical Care Admissions in the Northern Territory” published in the Internal Medicine Journal. 2
The unplanned and unforeseen introduction of the minimum unit price (MUP) for alcohol and the full-time stationing of Police Auxiliary Liquor Inspectors (PALIs) outside non–Darwin-located bottle shops provided an opportunity to further investigate the impact of these interventions. Due to staffing issues within the research unit of the Darwin intensive care unit (ICU), however, only data for Central Australia were available when we undertook an interim analysis. The results appeared to be so striking that we considered it important for this to be promulgated as soon as possible. This became the research letter “The impact of an alcohol floor price on critical care admissions in Central Australia” 3 published in the Medical Journal of Australia well before our originally planned manuscript. 2
Once data were available for the full 12-month period following the introduction of the new harm minimisation policies, we were in a position to undertake an NT-wide analysis of the impact of the MUP and PALI’s. However, we could only access data for the period up to and including six months prior to the introduction of the policies. Therefore, an NT-wide analysis was undertaken acknowledging that seasonal variation was a necessary limitation in our analysis. Nevertheless, the multi-site nature of the data offered a unique insight into the impact of the new harm minimisation policies. This became “Hazardous and harmful alcohol use in the Northern Territory, Australia: the impact of alcohol policy on critical care admissions using an extended sampling period”, published in the journal Addiction. 4 The possibility of expanding the dataset by having a Darwin-based researcher hand search admissions for the six months, October 2017 to April 2018, was explored but was not logistically possible.
In order to include an analysis that included a full 12 months of data preceding introduction of the harm minimisation policies and a full 12 months following, an ICU registrar at Alice Springs Hospital (CW) undertook to manually review all ICU admissions during that period. This became “The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study”, published in Anaesthesia and Intensive Care. 1
Figure 1 describes the sampling time and whether the data are single-centre or multicentre in nature. From both this description, and Figure 1, the authors trust this corrigendum provides transparency around the overlapping data across the several published manuscripts describing the effect of alcohol misuse on critical care admissions in the NT.
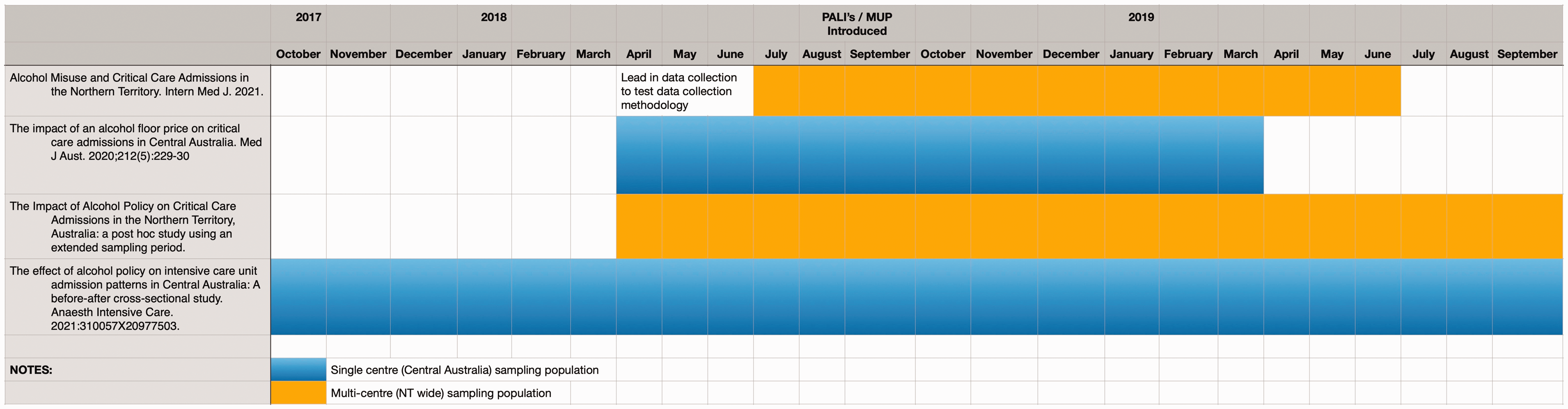
Sampling time of manuscripts describing alcohol misuse in the NT.