
Abstract

Awake tracheal intubation (ATI) remains an important skill for the management of complex or threatened airways. However, anaesthetists indicate that we are less confident with this technique than any other airway management skill. 1 These days, it also appears that ATI is less commonly performed. 2 Australian and New Zealand College of Anaesthetists' training currently requires trainees to be present or perform five awake bronchoscopies or intubations. 3 Experts believe more hands-on time is required for proficiency. Marsland et al. described that the development of basic bronchoscopic psychomotor skills on a bench-top trainer required multiple episodes of training, each lasting 20–30 minutes and totalling two to four hours. 4 Moreover, handling of a bronchoscope is only one aspect of awake bronchoscopic intubation. Safe and well-tolerated passage of an endotracheal tube also requires experience with topicalisation, ergonomics, troubleshooting technical issues and sedation (if provided). To our knowledge, there are no data guiding how many awake intubations are required to gain competence across all these skills. While five episodes with ideal conditions are achievable during training years, they are unlikely to convert a novice to a confident practitioner, let alone an expert.
A review of our electronic medical records during a 12-month period (1 September 2021 to 31 August 2022) at Peter MacCallum Cancer Centre, a tertiary referral hospital for head and neck malignancy, revealed that 29 fibreoptic intubations were performed out of 4827 theatre cases. When considering the number of consultant anaesthetists, fellows and senior registrars in the department, this equates to approximately half an awake bronchoscopic intubation per year per anaesthetist. We suspect this situation is not unique to our institution.
If we are to develop or maintain skills in ATI (and bronchoscope handling), creative approaches are required. Born out of recommendations from the 4th National Audit Project (NAP4), the Bath ‘tea trolley teaching’ tool was first introduced in 2015 as a novel tool for teaching and maintaining skills in difficult airway management and fibreoptic intubation. 5 It required two anaesthetists and a training trolley: one anaesthetist would relieve a colleague in theatre who was guided through a training episode by the other anaesthetist (replete with tea refreshments). Virtual-reality simulators have also been shown to improve skill acquisition in fibreoptic intubation (Figure 1).6,7
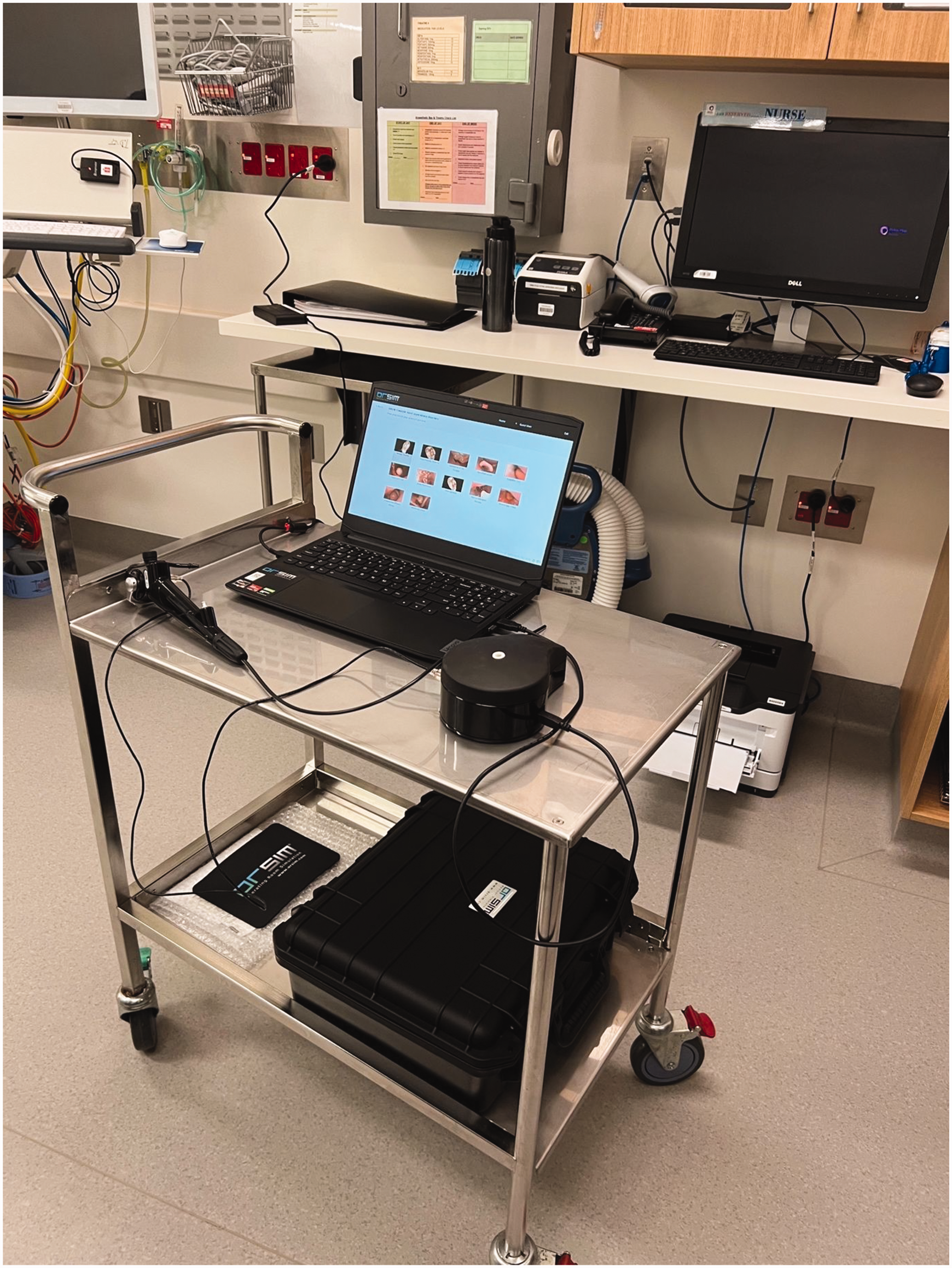
‘Tea trolley’ set-up with the ORSIM® simulator.
The ORSIM® bronchoscopic simulator (ORSIM, Auckland, New Zealand) is a flexible bronchoscope simulator with a library of difficult airways. Use of the simulator has been associated with increased speed, improved performance and faster upskilling than traditional training devices.6,7 A ‘virtual warm-up’ improved time to completion of successful fibreoptic intubation in consultant anaesthetists. 8 Importantly, it is a small, ergonomic and portable device well suited to rapid set-up and use in a busy operating theatre environment.
As a ‘proof-of-concept’ project, we provided one-to-one bedside training sessions using the Bath ‘tea trolley’ training method at our institution. Sessions were opportunistic, took approximately 15–20 minutes, were performed in the anaesthetic bay during routine in-hours theatre sessions and were supervised by a consultant anaesthetist with an interest in airway management. Participants first completed the ‘normal’ airway simulation to become acquainted with the simulator prior to navigating two or three of the difficult airway scenarios.
Over the course of one week, 21 anaesthesia registrars and consultants were given the opportunity to use the ORSIM. All participants felt that the simulator provided a high-quality experience with regards to practicing bronchoscopic dexterity and was more useful than traditional bench dexterity trainers. Furthermore, all agreed that there are currently limited opportunities to maintain, learn and practise skills in bronchoscopic intubation and would use the ORSIM for independent practice for skills maintenance if it were available in our department.
Despite providing an excellent opportunity to practise the motor skills, use of virtual-reality simulators does not provide practice for the other crucial components required for successful ATI such as topicalisation, ergonomics, peri-intubation oxygenation, communication, teamwork and sedation. These skills need to be addressed separately with other forms of education, case-based discussion or workshops.
We propose that virtual-reality simulators, such as the ORSIM, are a transferable and reproducible training tool that could be used in other theatre suites. Use of such a training device could significantly support training opportunities and skills maintenance for relatively uncommon airway techniques that nonetheless remain a core competence for anaesthetists (Figure 2).
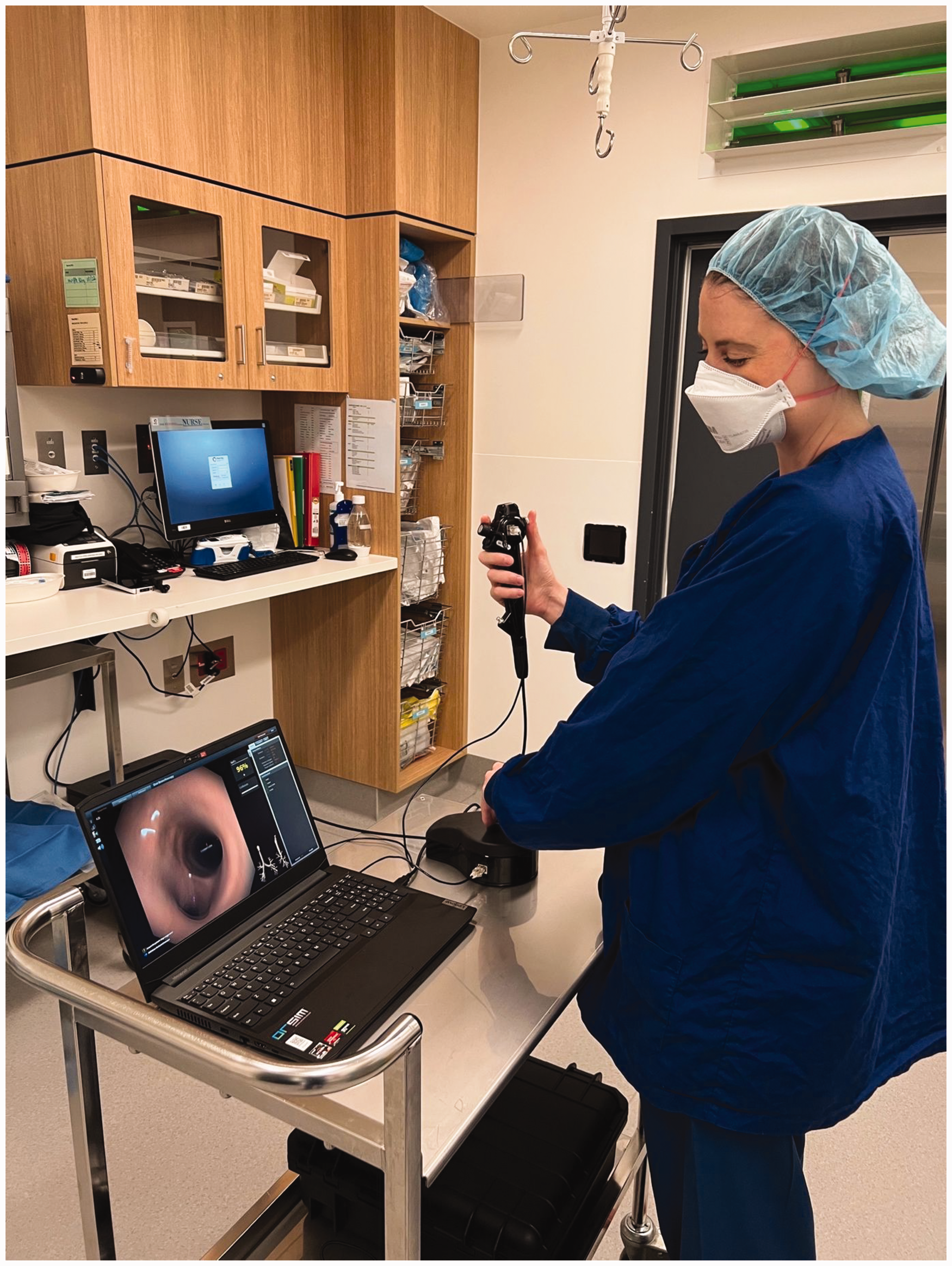
Trainee anaesthetist performing ‘tea trolley teaching’ using the ORSIM simulator.
Footnotes
Author Contribution
Declaration of conflicting interests
The authors declare no conflict of interest with respect to the research, authorship and/or publication.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.