
Abstract
Among all surgical specialties, vascular surgery has the greatest proportion of patients with unplanned admissions to the intensive care unit postoperatively. Therefore, current clinical pathways for the postoperative management of vascular surgery patients may need to be revised. We aimed to compare the prevalence of postoperative deterioration in the high and standard risk cohorts of patients through several markers: medical emergency team activations and unplanned intensive care unit admissions. This was a single-centre, retrospective cohort study of all vascular surgical patients, emergency and elective, between 1 January and 31 December 2020 at Fiona Stanley Hospital, a tertiary hospital located in Perth, Western Australia. Patients (n = 680) were risk stratified using the surgical outcome risk tool into standard-risk (30-day mortality risk <5%; n = 475, 69.9%) and high-risk (30-day mortality risk ≥5%; n = 205, 30.1%). There were 43 unplanned intensive care unit admissions (6.3%) in total. Furthermore, surgical outcome risk tool 5% or greater risk patients were approximately eight times more likely to experience an unplanned intensive care unit admission compared with their surgical outcome risk tool less than 5% risk counterparts (relative risk 7.65, 95% confidence interval 3.84–15.21). There were 87 medical emergency team calls (12.8%) in total. In addition, surgical outcome risk tool 5% or greater risk patients were approximately five times more likely to experience a medical emergency team activation than their surgical outcome risk tool less than 5% risk counterparts (relative risk 5.15, 95% confidence interval 3.37–7.86). Our findings highlight the need for a revision of the inpatient journey for surgical outcome risk tool 5% or greater risk vascular patients, given their increased rates of unfavourable postoperative outcomes such as unplanned intensive care unit admission and medical emergency team activation. Ideally this can be addressed through appropriate postoperative triage, thus allowing this vulnerable population group early access to higher acuity care.
Introduction
Among non-cardiac surgery, vascular surgery patients have been identified to be at the greatest risk of postoperative cardiac complications. 1 The determinants of any postoperative event can be classified as factors related to either the patient or the procedure. 2 Patients undergoing vascular surgery tend to have risk factors such as hypertension, diabetes and dyslipidaemia, that both contribute to their vascular disease and increase the risk of postoperative complications. 3 In addition, perioperative physiological alterations such as significant blood loss and increased thrombogenicity are observed in vascular surgery.4,5 Among all surgical specialties, vascular surgery has the greatest proportion of patients with unplanned admissions to the intensive care unit (ICU) postoperatively. 6 Therefore, accurate prediction of which patients are likely to deteriorate would be helpful in planning appropriate postoperative disposition.
Unplanned ICU admissions are an unfavourable postoperative marker, 7 given their association with increased morbidity and mortality.8–10 Furthermore, from the organisational perspective, they lead to increased length of stay (LOS) and financial burden on the institution.10,11 Appropriate planning of postoperative disposition is required, such as a planned ICU admission prior to standard ward care. However, ICU beds are a scarce resource, with overwhelming demand from multiple specialties, and limited availability. This presents a challenge as delayed access to a high acuity facility is known to contribute up to 80% of postoperative morbidity.12,13
This study was conducted to assess postoperative deterioration in vascular patients who did not have a planned ICU admission. In particular, we aimed to compare the prevalence of postoperative deterioration in the high- and standard-risk cohorts of patients through several markers: medical emergency team (MET) activations, unplanned ICU admissions and median LOS.
Materials and methods
This is a single-centred, retrospective cohort study of all vascular surgical patients between 1 January and 31 December 2020 at Fiona Stanley Hospital (FSH). FSH is a tertiary hospital located in Perth, Western Australia. Ethics approval was granted by the governance evidence knowledge outcomes FSH – anaesthesia and pain medicine committee (quality improvement activity 40550 – 29/04/21).
Patients were identified through a list generated by the medical coding team via the electronic theatre management system software. All patients undergoing vascular surgery, both elective and emergency, were included in the study (n = 877). However, patients who had a planned postoperative ICU admission (n = 171) and patients with incomplete medical records (n = 26) were excluded from the study. The remaining patients (n = 680) were risk stratified using the Surgical Outcome Risk Tool (SORT) into standard risk (30-day mortality risk <5%; n = 475, 69.9%) and high risk (30-day mortality risk ≥5%; n = 205, 30.1%). 14 The threshold of 5% or greater was used to identify ‘high-risk’ patients to reflect the recent recommendations by the Royal College of Surgeons of UK in 2018. Furthermore, this threshold has been shown not to lead to overestimation of unplanned ICU admissions among high-risk patients. 15
Data were collected from the hospital’s digital medical records system called ‘Bossnet’. Data included were anaesthetic record notes, discharge summaries and inpatient progress notes. Primary outcomes for this study were the incidence of MET activation (yes versus no), unplanned ICU admission (yes versus no) and hospital LOS (in days).
All statistical analyses were conducted using Microsoft Excel and the Statistical Package for the Social Sciences (SPSS). Categorical variables (MET activations and unplanned ICU admissions) were analysed with the chi-square test with a P value of less than 0.05 to reject null hypotheses.
Results
Among the 680 vascular surgery patients, the average age was 66 years and 68% were men. The majority of our patients were American Society of Anesthesiologists physical status (ASA-PS) 3 (69.0%) or ASA-PS 4 (17.4%). In addition, demographic details for SORT less than 5% risk and SORT 5% or greater risk can be seen in Table 1. There were 87 MET calls (12.8%) in total. The median age for these patients was 67 years and approximately 75% of them were men. As seen in Table 2, the commonest types of surgery involved with postoperative MET activation were amputations (n = 29, 33.3%), arterial embolectomy (n = 15, 17.2%) and wound debridement with washout (n = 14, 16.7%).
Characteristics of patients undergoing vascular surgery according to SORT risk.
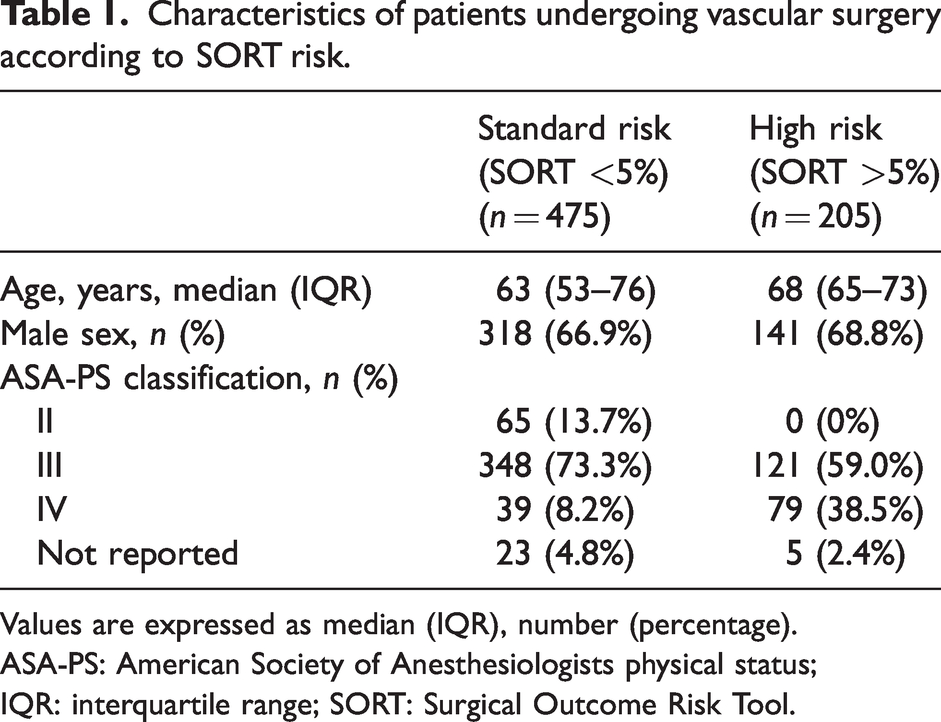
Values are expressed as median (IQR), number (percentage).
ASA-PS: American Society of Anesthesiologists physical status; IQR: interquartile range; SORT: Surgical Outcome Risk Tool.
Procedures and MET activation.
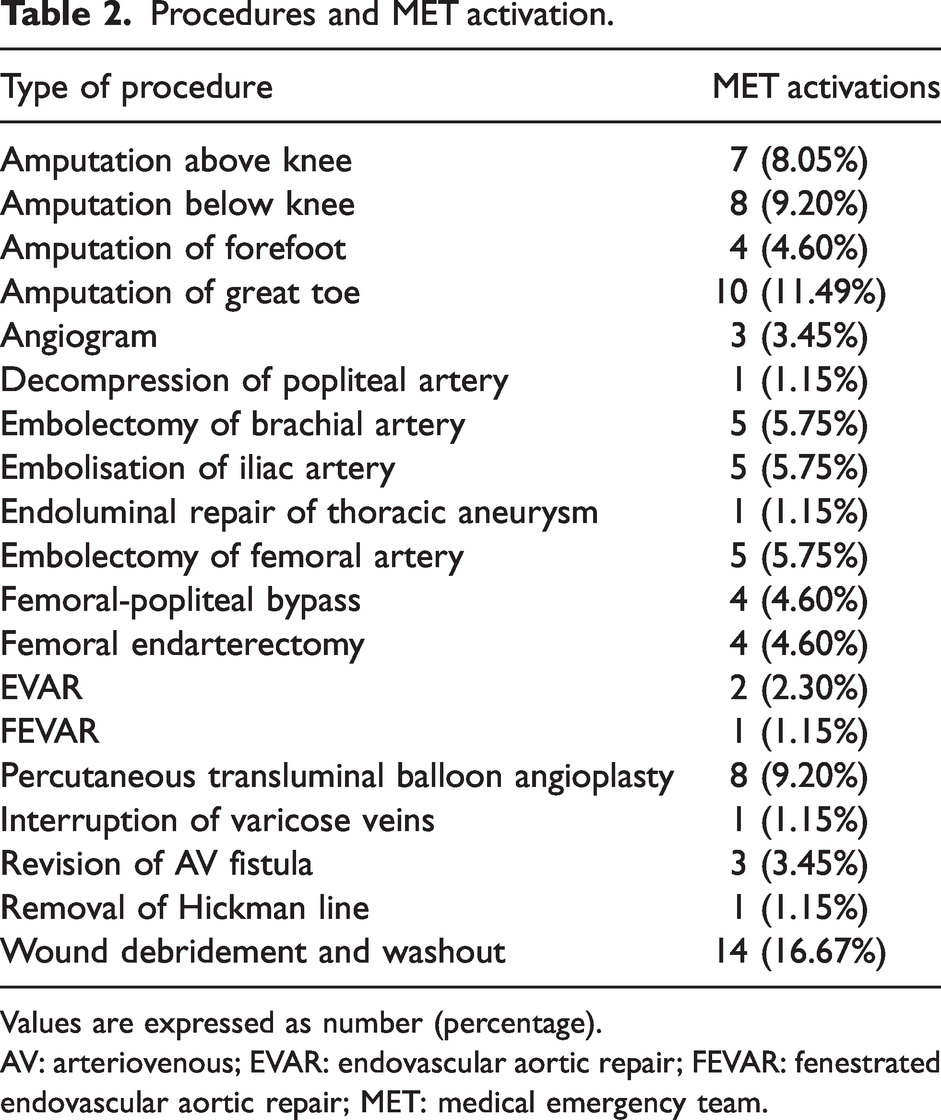
Values are expressed as number (percentage).
AV: arteriovenous; EVAR: endovascular aortic repair; FEVAR: fenestrated endovascular aortic repair; MET: medical emergency team.
SORT 5% or greater risk patients were more likely to experience MET activation than SORT less than 5% risk patients (χ2 = 71.39, 1 degree of freedom (df), P < 0.01). Among SORT 5% or greater risk patients, 29% (n = 60) experienced a MET activation during their hospital stay compared with 6% (n = 27) of SORT less than 5% risk patients. Furthermore, as seen in Table 3, SORT 5% or greater risk patients were approximately five times more likely to experience a MET activation than their SORT less than 5% risk counterparts (relative risk (RR) 5.15, 95% confidence intervals (CI) 3.37 to 7.86).
Relative risk of unplanned admission to intensive care unit and medical emergency team activation for Surgical Outcome Risk Tool risk 5% or greater compared with risk less than 5%.
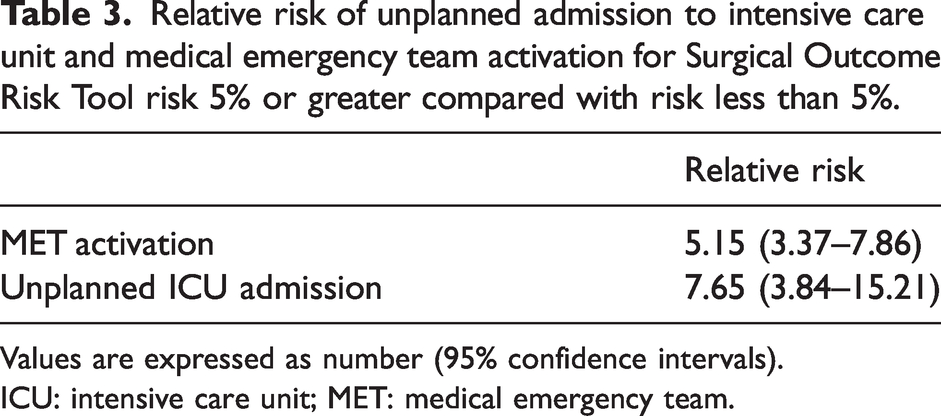
Values are expressed as number (95% confidence intervals).
ICU: intensive care unit; MET: medical emergency team.
There were 43 unplanned ICU admissions (6.3%) in total. The median age of these patients was 70 years and approximately 70% were men. SORT 5% or greater risk patients were more likely to require an unplanned ICU admission than SORT less than 5% risk patients (χ2 = 47.32, 1 df, P < 0.01). Among SORT 5% or greater risk patients, 16% (n = 33) required unplanned ICU admissions compared with 2% (n = 10) of SORT less than 5% risk patients. Furthermore, as seen in Table 3, SORT 5% or greater risk patients were approximately eight times more likely to experience an unplanned ICU admission compared with their SORT less than 5% risk counterparts (RR 7.65, 95% CI 3.84 to 15.21). SORT 5% or greater risk patients also experienced greater median lengths of stay compared with SORT less than 5% risk patients, 13 days and six days, respectively.
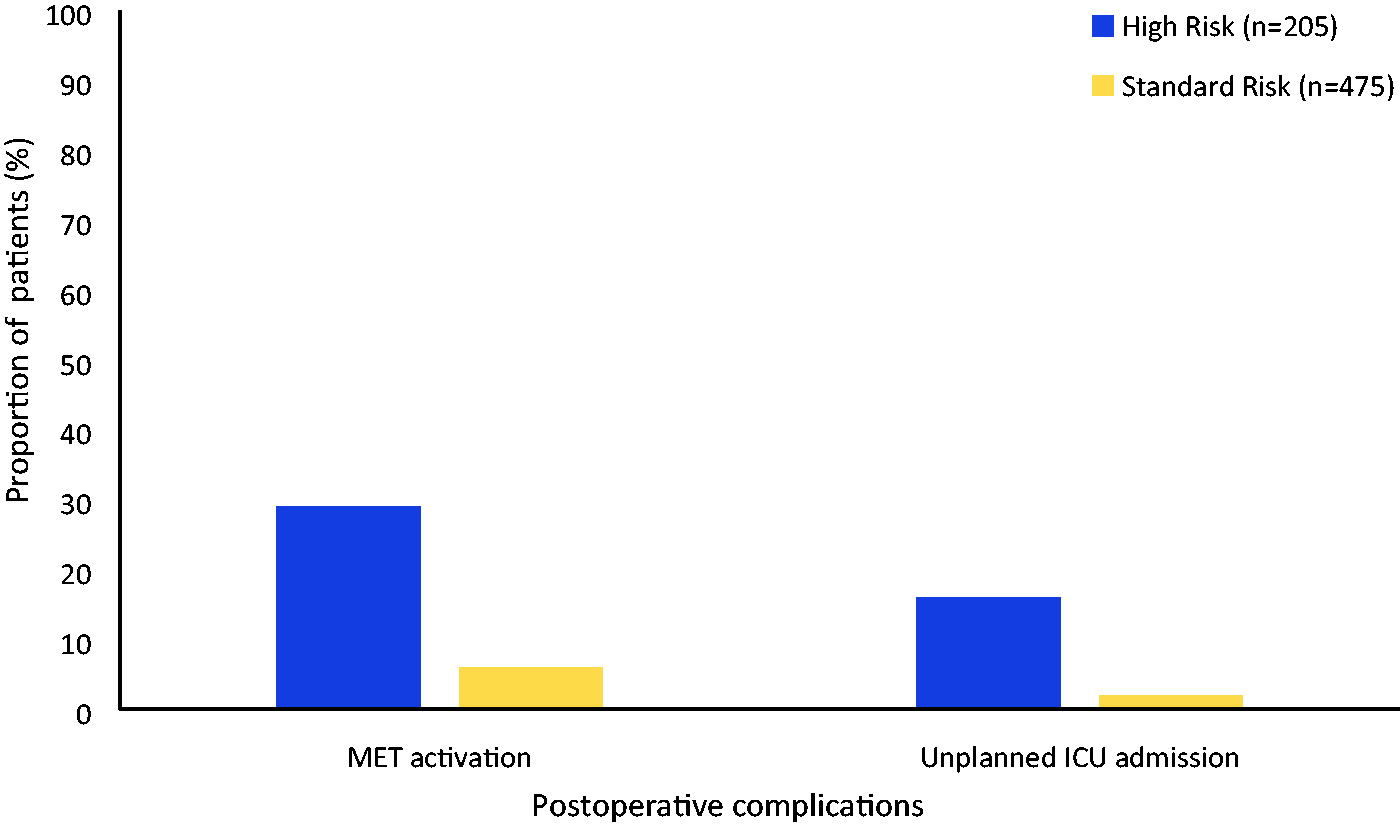
Comparison of postoperative deterioration. High risk: Surgical Outcome Risk Tool (SORT) risk 5% or greater; standard risk: SORT risk less than 5%.
Discussion
The principal findings in our study are that SORT 5% or greater risk patients are more likely to experience unplanned ICU admission and MET activation by eightfold and fivefold, respectively, compared with their SORT less than 5% risk counterparts. Furthermore, SORT 5% or greater risk patients tend to stay twice as long in hospital compared with SORT less than 5% risk patients. Therefore, our findings suggest that postoperative management for SORT 5% or greater risk vascular patients could be improved, such as appropriate disposition planning to a high acuity unit, as opposed to a standard ward, which may consequently place this vulnerable group at a greater risk of deterioration.
Our rate of unplanned ICU admission (6.3%) was greater than the findings seen in other studies that ranged between 0.5% and 0.8%.8,16 However, the difference in the rate of unplanned ICU admission is likely to be multifactorial and this can be attributed to disparities in patient characteristics, procedure-related factors and hospital policies. For instance, the average age of the aforementioned studies ranged between 54 and 59 years.8,16 Meanwhile, the average age in our study was 66 years. Furthermore, previous studies considered a variety of surgical specialties. Meanwhile, we only considered vascular surgery, which has previously been identified as one of the leading surgical specialties for unplanned ICU admission postoperatively. 6
The rate of unplanned ICU admission was greater in SORT 5% or greater risk (16%) than SORT less than 5% risk (2%) patients. The burden of postoperative morbidity in SORT 5% or greater risk patients can be reduced by appropriate triage, as timely access to acute care will reduce postoperative morbidity and mortality.12,13 For instance, earlier identification of SORT 5% or greater risk patients preoperatively will allow the anaesthetist to liaise with the ICU earlier for a planned admission postoperatively. Another strategy would be a tailored assessment of SORT 5% or greater patients postoperatively in the anaesthesia recovery unit to minimise unnecessary admissions to the ICU. This is limited by the lack of a standardised ICU triage tool that is universally accepted by physicians and also incorporates intraoperative data. 16 However, the underlying issue is the limited supply of ICU beds relative to its high demand. Therefore, the extended recovery unit (ERU) could be a solution. This will allow for extended monitoring of patients postoperatively who are not unwell enough to warrant an ICU admission but are at high risk of deterioration with standard ward care. Furthermore, the ERU will alleviate the shortage of high acuity care beds and is likely to have greater turnover than the ICU due to the nature of patients that are admitted to the unit.
Currently, there is conflicting evidence regarding the benefits of planned postoperative admission to the ICU. For instance, the STARSurg collaborative revealed no benefit in mortality with planned ICU admission postoperatively. 17 However, that study only considered liver and gastrointestinal surgery and only measured 30-day mortality. Meanwhile, the study by Gillies et al. 10 demonstrated increased morbidity and mortality with unplanned postoperative ICU admissions. That study had a larger scope as it included all surgical specialties in Scotland for 2005–2007, involving approximately 600,000 patients, and had a longer follow-up of one year and four years. The difference in findings is likely to be multifactorial such as disparities in the surgical cases included and its associated risks, patient characteristics and ICU admission criteria. Therefore, our study is unique, given that it is one of the first studies that has solely followed up vascular surgery patients for postoperative deterioration (unplanned ICU admission and MET activations) in the setting of an Australian hospital.
Our rates of postoperative MET activation (13%) were lower than previous findings (25%). This is likely due to the inclusion criteria of Moore et al., 11 as they only selected patients who were unwell enough to warrant an ICU review postoperatively in the recovery unit but were not offered an acute care admission. However, comparable rates were seen with our SORT 5% or greater patients (29%). Alternatively, they may benefit from a prolonged stay in a monitored setting, such as an ERU, given that the majority of MET calls in the study of Moore et al. occurred within the first 12 hours postoperatively. 11
The rates of MET activation greatly varied depending on the vascular surgery procedure (Table 3). As seen in Table 3, almost a third of MET activations occurred following an amputation. Therefore, post-amputation patients represent a high-risk population, and they should be triaged with great consideration for high acuity care, such as an ERU or ICU.
Another potential area to address is the prolonged LOS observed in SORT 5% or greater patients, approximately twofold greater than SORT less than 5% risk counterparts. A previous study identified that there was an eightfold higher rate of postoperative inpatient complication in extended LOS patients compared with those with normal LOS. 18 Furthermore, the study of Gillies et al. found that LOS was greater in patients with unplanned ICU admission compared with those with a planned ICU admission. 10
One of the strengths of our study was the study design, as it included all vascular patients (elective and emergency) over a 12-month period without a planned ICU admission. Furthermore, patients were measured with objective and clinically relevant outcomes, therefore optimising internal validity. The limitations of our study included the use of a single site, thus differing baseline patient characteristics and hospital practices (criteria for ICU admission and MET activation) may have limited the generalisability of our study’s findings. Furthermore, the retrospective nature of our study and reliance on digital medical records is another limitation as some details regarding the patient’s stay may be omitted.
There is a paucity of studies that have retrospectively followed the postoperative journey of vascular surgery patients, particularly comparing deterioration outcomes between SORT less than 5% risk and SORT 5% or greater risk patients in the setting of an Australian hospital. Although we have attempted to address this lack of information in this retrospective observational study, further studies are required in different settings. For instance, findings may differ depending on individual hospital practices and patient mix. Furthermore, it would be useful if in future more studies utilised the SORT tool to risk stratify their patients. This would help raise awareness regarding the reliability of the SORT tool. It might then be implemented more frequently in daily clinical practice, ultimately allowing for earlier identification of patients at higher risk of postoperative deterioration.
Conclusion
Our findings highlight the need for a revision of the inpatient journey for SORT risk 5% or greater vascular patients in Australia, given their increased rates of unfavourable postoperative outcomes such as unplanned ICU admission and MET activation. Ideally, this can be addressed through improved postoperative triage, using validated tools such as the SORT tool, thus facilitating early access to higher acuity care in this vulnerable group.
Footnotes
Acknowledgements
The authors would like to thank the Department of Vascular Surgery at Fiona Stanley Hospital.
Author Contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.