
Abstract

It is now recognised that correction of hypofibrinogenaemia is a priority in the management of coagulopathic bleeding, once drug-related causes have been reversed as far as possible.1,2 Correction of low fibrinogen levels has also been shown to improve clot strength in the presence of thrombocytopenia.2,3 For this reason, an additional alert to the likelihood of hypofibrinogenaemia may help clinicians to improve coagulation management, by prompting them to measure the fibrinogen level, and replace fibrinogen in a timely manner if necessary. We reasoned that such an alert could be obtained by considering the preoperative fibrinogen level and the extent of haemodilution pertaining at any particular stage of a procedure. This reasoning is based on the fact that fibrinogen is a large molecule, which under normal circumstances is confined to the intravascular space in the same way as haemoglobin.4,5 Moreover, normal levels are not restored immediately, but instead occur over several hours.6,7 Therefore, any reduction in the haemoglobin level caused by blood loss and its replacement with non-sanguineous fluid should be accompanied by a similar or greater proportional reduction in the fibrinogen level, assuming no blood products have been administered.
We recently published two studies on the diagnostic accuracy of rotational thromboelastometry estimations of fibrinogen levels during cardiac surgery.8,9 Both involved the measurement of fibrinogen levels intraoperatively. This provided an opportunity to assess the relationship between the proportional reductions in haemoglobin and fibrinogen during cardiac surgery using data already collected.
With new institutional ethics approval (RGS0000005391), we identified all patients in our two recently published diagnostic accuracy studies who met the following criteria: (a) they had simultaneous laboratory haemoglobin and fibrinogen measurements preoperatively within one week of their surgical procedure; (b) they had simultaneous laboratory fibrinogen and haemoglobin measurements intraoperatively either on rewarming during cardiopulmonary bypass (CPB) just prior to or immediately following separation from CPB and the administration of protamine; (c) they had received no haemoglobin or fibrinogen supplementation between the preoperative and the intraoperative samples.
The eligibility criteria for the previous studies were previously published.8,9 Likewise, the anaesthetic management of the patients and the method of blood sampling were previously described.8,9 Blood for fibrinogen measurement was collected into a 2.7 ml citrated blood collection tube (Vacutainer; Becton Dickinson & Co., Franklin Lakes, NJ, USA). Blood for haemoglobin measurement (as part of a full blood count) was collected into a 2.2 ml EDTA tube. Both tubes were transported within five min to a pathology laboratory where on being received the fibrinogen was measured using the Clauss method (STAR Max3; Diagnostica Stago, France); the haemoglobin was measured using a Roche Haematology Analyzer (Sysmex XN, Milton Keynes, UK).
For each eligible patient we calculated the proportional reduction in laboratory haemoglobin (i.e. percentage haemodilution), the proportional reduction in laboratory fibrinogen, and the estimated intraoperative fibrinogen value, based on the starting fibrinogen and extent of haemodilution that had occurred (i.e. starting fibrinogen × (1 minus percentage haemodilution)). We calculated the Pearson correlation coefficient between the proportional reduction in haemoglobin and the proportional reduction of fibrinogen, along with its 95% confidence interval (CI) and P value. We calculated the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the ‘estimated’ fibrinogen for the identification of a laboratory fibrinogen of less than 1.5 g/l.
Data on 255 of the 400 patients in the original two studies met the inclusion criteria. Details of the patients and the surgical procedures are included in Table 1. The mean preoperative haemoglobin was 139 (range 77–186) g/l. The mean haemoglobin at the time of intraoperative sampling was 88 (range 52–127) g/l. This represented a median 37% reduction (interquartile range (IQR) 30%–43%). The mean preoperative laboratory fibrinogen was 3.7 (range 2.0–6.7) g/l. The mean laboratory fibrinogen at the time of intraoperative sampling was 2.0 (range 0.9–4.8) g/l. This represented a median reduction of 44% (IQR 37%–53%). The Pearson correlation coefficient between these reductions was 0.72 (95% CI 0.66 to 0.78, P < 0.001) (Figure 1).
Patient and procedure characteristics.
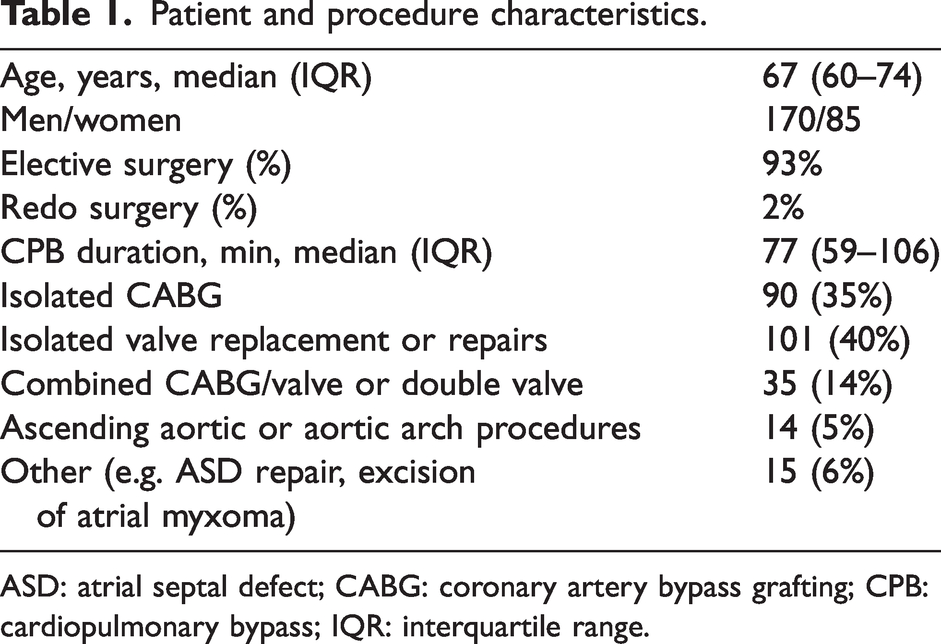
ASD: atrial septal defect; CABG: coronary artery bypass grafting; CPB: cardiopulmonary bypass; IQR: interquartile range.

Percentage fall in haemoglobin versus percentage fall in fibrinogen during cardiac surgery with cardiopulmonary bypass (no blood products administered) compared with starting values, n = 255.
The mean ‘estimated’ intraoperative fibrinogen based on the starting laboratory fibrinogen and the proportional reduction in haemoglobin at the time of sampling was 2.3 (range 0.95–5.4) g/l. This was a median of 0.28 g/l higher (IQR 0.11–0.43 g/l) than the laboratory fibrinogen. Of the 255 patients, 228 (89.4%) had a laboratory fibrinogen equal to or less than the estimated fibrinogen based on the starting laboratory fibrinogen and the proportional reduction in haemoglobin (see Figure 1).
The prevalence of a laboratory fibrinogen of less than 1.5 g/l was 10.2% (26 of the 255 patients). Only ten of these 26 patients had an estimated fibrinogen of less than 1.5 g/l; that is, the sensitivity of the estimated fibrinogen of less than 1.5 g/l for the identification of a laboratory fibrinogen of less than 1.5 g/l equals 38% (10/26, 95% CI 20% to 59%). However, none of the 229 patients with a laboratory fibrinogen of 1.5 g/l or greater had an estimated fibrinogen of less than 1.5 g/l. This provided a PPV of an estimated fibrinogen of less than 1.5 g/l for a laboratory fibrinogen of less than 1.5 g/l equals 100% (10/10, 95% CI 69% to 100%). The specificity was 100% (229/229, 95% CI 98% to 100%), with a NPV of 93% (229/245, 95% CI 90% to 96%).
These findings indicate that the proportional fall in fibrinogen during cardiac surgery with CPB is similar to or greater than the proportional fall in haemoglobin in the majority of patients, assuming no blood products have been administered. While the correlation coefficient was only 0.72, more than 89% of patients had a laboratory fibrinogen equal to or less than the estimate based on the starting fibrinogen and the proportional reduction in haemoglobin.
The haemoglobin level is typically monitored closely during cardiac surgery and can be checked at the bedside using a point-of-care haemoglobinometer if required. 10 As a result, the proportional fall in haemoglobin can be calculated at any time during surgery, with reference to the pertaining haemoglobin and the starting haemoglobin. It is then a simple matter to apply this proportional fall to the starting fibrinogen, although there would be several important caveats. First, the estimate would not apply if additional red blood cells or fibrinogen had been administered. The estimate would also not apply if there was another cause for a fall in haemoglobin unrelated to haemodilution, such as haemolysis. Another caveat would be ensuring an accurate method of haemoglobin measurement.
An additional observation in this study was that the proportional reduction in fibrinogen was greater than the proportional reduction in haemoglobin in the majority of patients (see Figure 1). The median fall in fibrinogen was 44%, while the median fall in haemoglobin was only 36%. This difference could be explained by the consumption of fibrinogen, such as might occur in the clotting process, by the generation of non-haemostatic fibrin in the CPB circuit, or by the destruction of fibrinogen that might accompany fibrinolysis. However, investigation of the cause was outside the scope of the study. Suffice it to say that because of this difference, the estimated fibrinogen could not be used to ‘rule out’ the likelihood of hypofibrinogenaemia, only to ‘rule it in’. In fact, the sensitivity of the fibrinogen estimate of less than 1.5 g/l to identify a laboratory fibrinogen of less than 1.5 g/l was only 38%. In contrast, the specificity was 100%, indicating that the estimate had high reliability to ‘rule in’ hypofibrinogenaemia. An implication of this difference is that any calculated estimate close to the fibrinogen replacement trigger should be cause for concern, particularly in the presence of abnormal bleeding, and should prompt fibrinogen measurement.
Our findings relate to a retrospective analysis from a single institution. While our patients and practice would be typical of many cardiac surgical units (see Table 1), our findings would require confirmation in prospective cohort studies and in different settings and perhaps with different CPB strategies.
The measurement of fibrinogen is also undertaken routinely during cardiac surgery. However, this is often less frequent than haemoglobin measurement, due to the additional time, disposables, or equipment required. Therefore, an estimate of the fibrinogen level based on the starting fibrinogen and the extent of haemodilution would provide interim information on the likelihood of hypofibrinogenaemia between routine fibrinogen measurements. This might be particularly helpful if the extent of haemodilution was large or the starting fibrinogen was low. The calculation requires no appreciable extra time or expense, and could serve as additional prompt to check or recheck the fibrinogen, using either a point-of-care technique or a laboratory method, depending on the clinical scenario and the rate of bleeding.
Footnotes
Acknowledgements
This paper was presented in part at the Australian and New Zealand College of Anaesthetists Annual Scientific Meeting, Perth, 2022.
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.