
Abstract

In 2015, we conducted a six-month prospective single centre study, 1 Rational Clinical Pathology Assessment in Intensive Care Unit (RCPA-ICU), to rationalise routine blood tests ordered more frequently in ICU named as high volume tests (HVTs). These tests contributed to more than 50% of total ICU laboratory expenditure in our ICU at Liverpool Hospital, New South Wales, Australia. We used a multimodal approach: (a) displaying the cost of these HVTs at the bedside, (b) staff education on clinical relevance of laboratory tests in ICU and (c) ICU specialist to exclusively authorise HVTs for next day during the evening ward rounds. This approach was associated with a significant reduction in cost of the overall laboratory expenses and also for the individual groups of tests when compared with 2014 baseline data. There were no adverse events recorded in that study. Dhanani et al. used a similar multimodal approach and observed similar results in their single-centre study with the results of their intervention sustained for one year after the intervention period. 2 However, Mehari and Havill, in their study, 3 concluded that even after three years, written guidelines remained effective to reduce the laboratory tests cost in cardiothoracic ICU by 4% and general ICU by 5.6%.
After receiving ethics approval, we performed a follow-up study in our unit to investigate whether the cost reductions achieved in the 2015 study were sustained from 2016 to 2018, when the above multi-modal strategies to rationalise HVT orders were not strictly enforced. We hypothesised increased overall laboratory costs by 10% over a three-year period. The laboratory costing data was collected retrospectively for a six-month period in each year from 2016 to 2018 and analysed.
When compared with baseline values in 2015, the total average laboratory costs increased by 8.3% over a three-year period, close to our hypothesis of 10%. The cost of routine HVTs consistently accounted for >50% of overall laboratory expenses with an average of 55%. Also there was a gradual increase in cost from years 2016 to 2018. There was no observable difference in the median length of stay and Acute Physiology and Chronic Health Evaluation (APACHE III) scores (Table 1).
Demographics and unadjusted costings in Australian dollars.
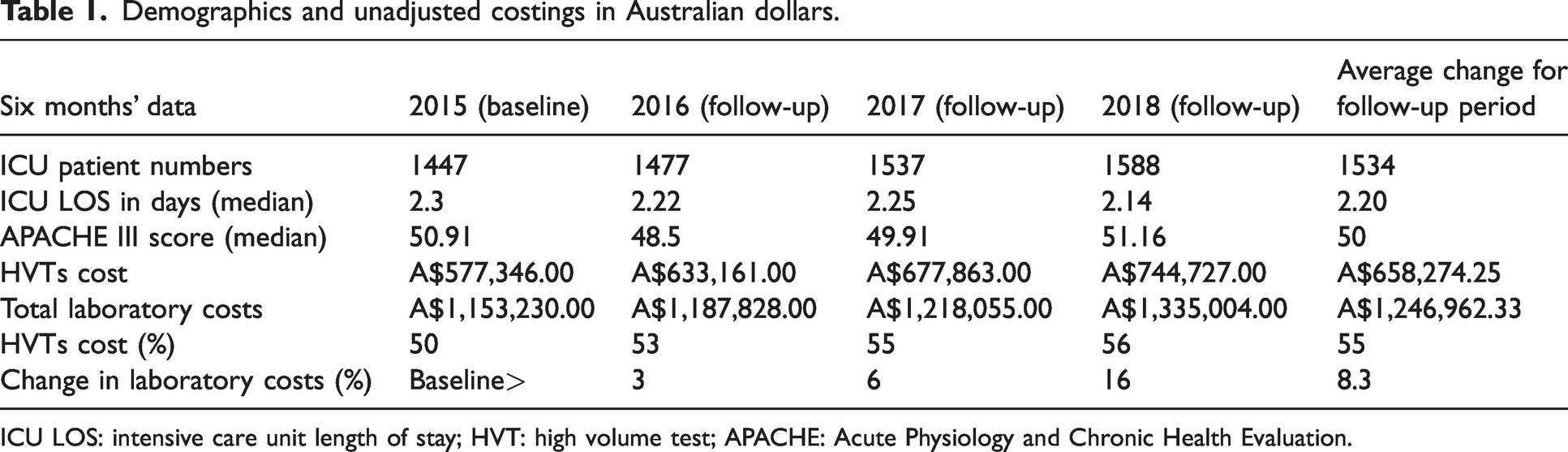
ICU LOS: intensive care unit length of stay; HVT: high volume test; APACHE: Acute Physiology and Chronic Health Evaluation.
A multivariable linear regression analysis was performed on the HVT costs and estimates were given in Australian dollars (A$) for the same six-month periods (March to August) from 2016 to 2018. The year was taken as the main variable of interest, adjusting for month of the year, monthly median ICU length of stay, median APACHE III score and patient numbers (Table 2). The following results were in comparison with the baseline data in 2015. There were no significant cost differences of all HVTs in 2016 (P = 0.086) and 2017 (P = 0.846) but a significant increase in 2018 (estimate = A$8927, P = 0.005). General chemistry costs were decreased in 2016 (estimate =−A$3632, P < 0.001) and 2017 (estimate = −A$2303, P = 0.003). Full blood count costs were significantly lower in 2016 (estimate = −A$3784, P < 0.001), 2017 (estimate = –A$3271, P < 0.001) and also in 2018 (estimate = −A$1824, P < 0.001). Coagulation costs were increased in 2018 (estimate = A$4869, P = 0.001). Arterial blood gas analysis test costs increased in 2017 (estimate = A$3788, P = 0.026) and 2018 (estimate = A$4986, P = 0.005).
Multivariable linear regression analysis of high volume tests costs.
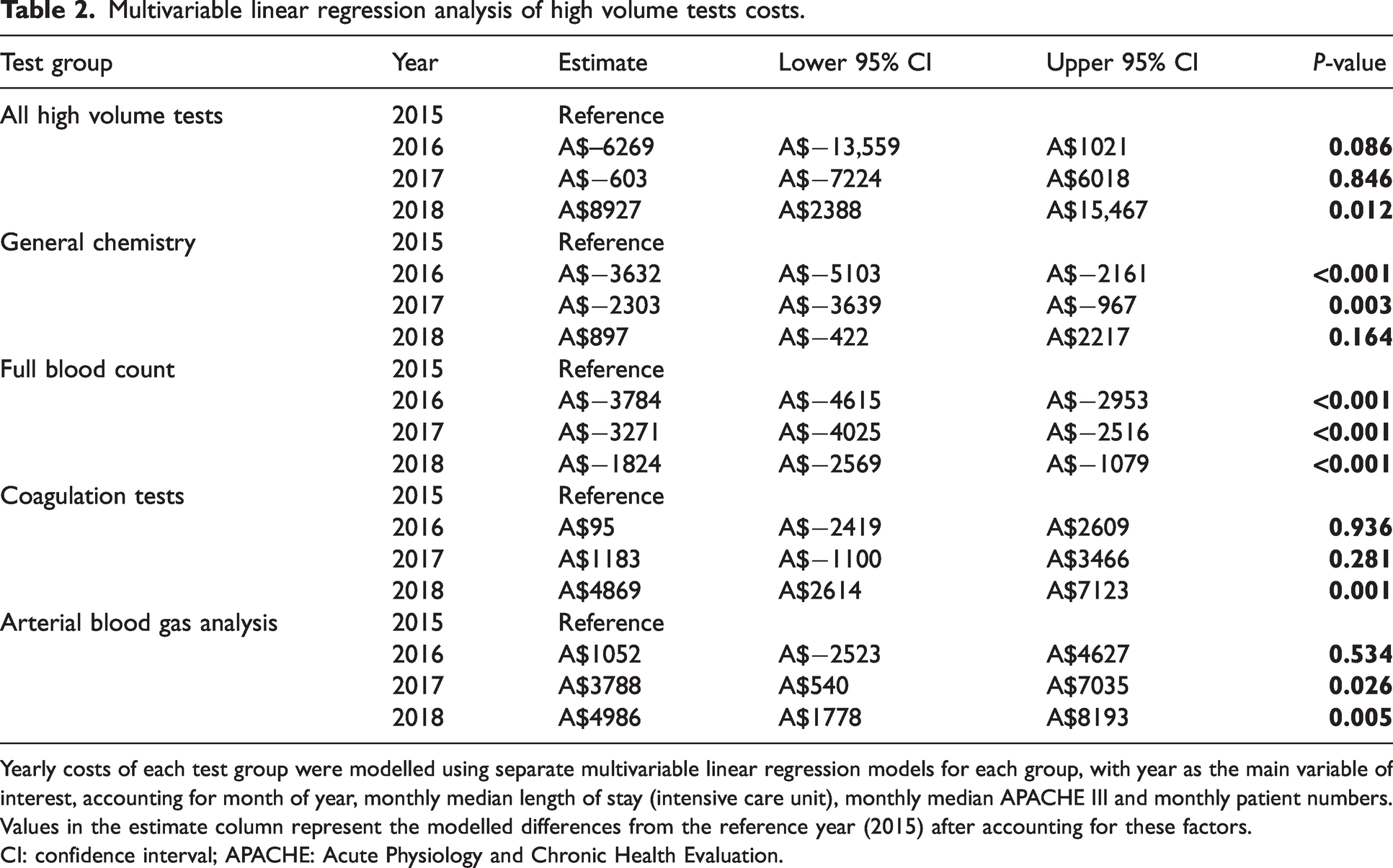
Yearly costs of each test group were modelled using separate multivariable linear regression models for each group, with year as the main variable of interest, accounting for month of year, monthly median length of stay (intensive care unit), monthly median APACHE III and monthly patient numbers. Values in the estimate column represent the modelled differences from the reference year (2015) after accounting for these factors.
CI: confidence interval; APACHE: Acute Physiology and Chronic Health Evaluation.
We believe that certain factors might have potentially contributed to the non-uniformity of costings results in this follow-up study, such as: (a) decreased involvement of senior medical staff in direct authorisation of test orders as done in our 2015 study, (b) ongoing use of a predefined ICU profile by ICU trainee specialists, (c) absence of flagging arrangements to deter repetitive testing in a short space of time without indication, and (d) nursing staff having the permission to order the ICU routine tests, especially arterial blood gases, unlike in the 2015 study. It is time to develop a consensus for pathology tests in Australasian ICUs, whereby patient discomfort and anaemia, which have been observed especially in long-stay ICU patients, may be potentially minimised by avoiding unnecessary tests and potentially save valuable health dollars.
Although it was a retrospective analysis of the laboratory costing data, our study has several merits in its design. We compared data from the same time periods of six months from 1 March to 31 August for all the three years, replicating the same seasonal data from 2015. There was a Medicare Benefits Schedule (MBS) freeze during these years from 2015 to 2018 and our study was not affected by any change in MBS funding. All data was obtained from the NSW Health Pathology billing system and hence is likely to be accurate. We performed multivariable analysis adjusting for monthly median values of number of patients, APACHE III scores and ICU length of stay from 2016 to 2018 to accurately present any changes. We therefore think this data may be applicable to any large tertiary ICU in Australia.
This study was a single-centre large tertiary ICU study, and the cost savings may not be applicable to other smaller and private units in NSW and health services in other states with different pathology billing arrangements. Routine HVTs contribute to greater than 50% of the total laboratory costs of ICU. Achieving sustained reduction in the cost of HVTs in ICUs is not possible without ongoing attention to the multimodal approach we used in our 2015 study or application of similar guidelines.
Footnotes
Author Contribution(s)
Acknowledgements
We are grateful to John Tran from NSW Health Pathology working in liaison with Dr Michael Maley to provide all laboratory data required for the study; Suzanne Whiteman, ICU Data Manager, for providing data from ANZICS adult database; and NSW Health Pathology Clinical Governance for supporting the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.