
Abstract
We describe a case of bilateral parotid swelling developing shortly after laryngeal mask airway insertion. Spontaneous resolution occurred within 12 h postoperatively This unusual phenomenon has been termed ‘anaesthesia mumps’ or ‘acute sialadenosis’. Its exact relationship to anaesthesia remains unknown. It arises in a variety of patients and surgeries, making its pathogenesis difficult to determine. Its presentation can be confused with acute angioedema, but, unlike the latter, it is benign and not normally associated with airway compromise. Diagnosis is a process of exclusion, but careful airway assessment is an important component of this. Strategies to aid diagnosis and management are described.
Introduction
‘Acute sialadenosis’ refers to a benign, non-inflammatory swelling of the salivary glands which may occur in the perioperative period. This phenomenon has also been termed ‘anaesthesia mumps’ in the literature. Although this condition is generally benign, it is important to exclude other causes of facial swelling which can lead to airway compromise. We present a case of acute parotid swelling immediately following laryngeal mask airway (LMA) insertion. This report also describes differential diagnoses, investigations and perioperative management strategies for such a case.
This report and images were published with consent from our patient.
Case history
A 72 kg, 40-year-old gentleman presented for elective haemorrhoid banding under general anaesthesia. He had no known drug allergies and no significant medical comorbidities apart from mildly elevated liver enzymes (gamma-glutamyl transferase 273 IU/l, alanine aminotransferase 60 IU/l, aspartate aminotransferase 57 IU/l) in the context of moderate alcohol consumption. He had undergone three previous uneventful general anaesthetics for proctoscopy procedures, where a size 4 LMA had been used. He was appropriately fasted with no history of reflux.
In theatre, the patient received midazolam 1 mg, fentanyl 75 µg, and propofol 180 mg for induction. The patient was easy to bag-mask ventilate with low inflation pressures of less than 10 cmH2O and a size 4 LMA was easily inserted on first attempt with no manipulation or repositioning required. Immediately following LMA insertion, substantial, clearly visible bilateral parotid swellings developed (Figure 1). These swellings steadily increased over 3–5 min and were firm on palpation. There were no changes to the patient’s vital signs, airway pressures or ventilation. In order to exclude swelling extending into the airway, the larynx was visualised with a flexible endoscope (single use Ambu® aScope™ 5.5 mm Flexible Endoscope (Ambu Australia Pty Ltd, Warriewood, NSW)) that was passed through the LMA, and which demonstrated no evidence of mucosal or laryngeal oedema. Because of uncertainty regarding the potential for further extension of these swellings, the LMA was removed, intravenous suxamethonium 100 mg was administered and the patient was intubated with direct laryngoscopy as a precaution. The endotracheal tube was secured with a tie, placed inferiorly to the parotid swellings. Despite the appearance of Figure 1B, the tie was sufficiently loose that two fingers could be easily inserted between it and the patient’s skin. Anaesthesia was maintained with sevoflurane. An urgent intraoperative otorhinolaryngology (ORL) consult and ultrasound scan (USS) were obtained, which confirmed diffusely enlarged bilateral parotid glands, with no calculi, free gas, haemorrhage or duct dilation.
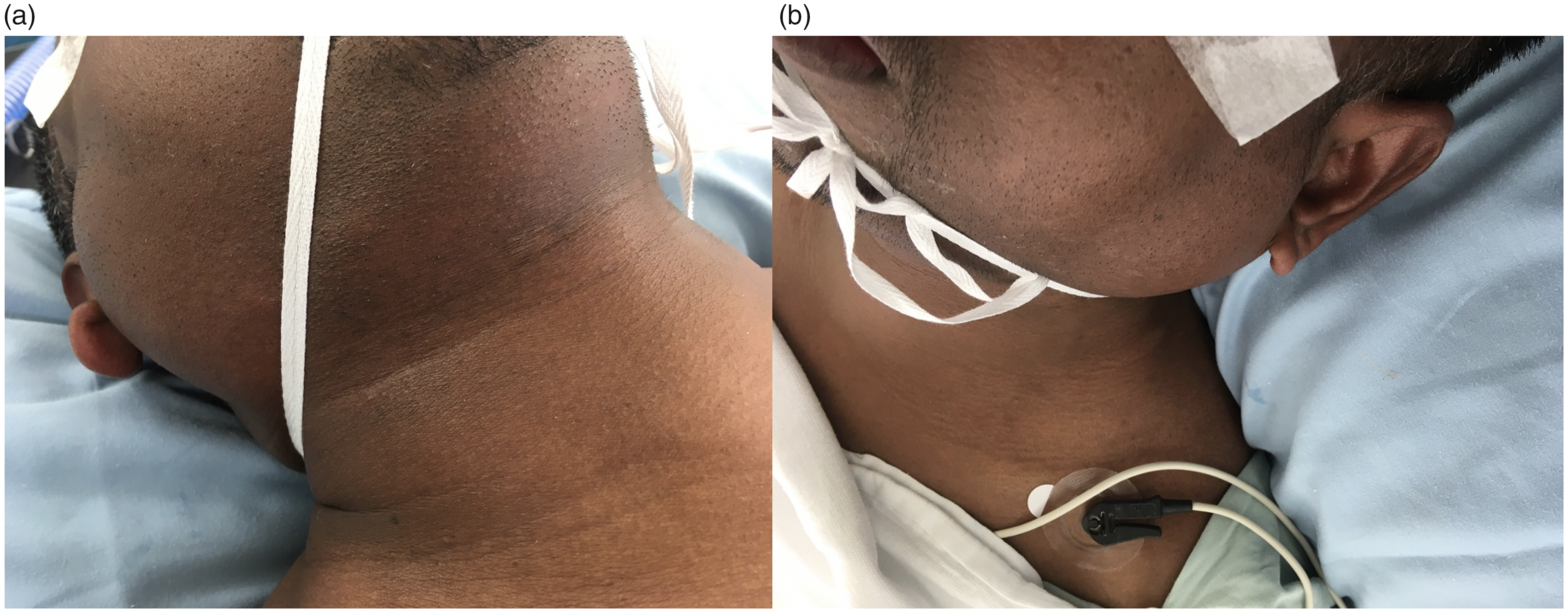
Acute right (a) and left (b) parotid swellings. Images were taken after patient was intubated and the endotracheal tube secured.
Surgery proceeded as planned and the patient remained stable throughout. Surgery and extubation were uneventful, with no further enlargement of the parotid swellings. The patient was admitted overnight for observation and discharged the following morning with complete resolution of this phenomenon. A nasopharyngeal swab (full respiratory viral panel), complement screen (C3 and C4), full blood count (FBC), electrolytes, amylase, C-reactive protein (CRP) and venous blood gas were obtained half an hour following intubation. Bloods for tryptase levels were taken at one, four and 12 h after swelling onset. All laboratory investigations produced results within the normal range.
Discussion
There are a limited number of reports describing acute swelling of the parotid glands (‘acute sialadenosis’) in association with general anaesthesia. This phenomenon has also been termed ‘anaesthesia mumps’, although its exact correlation to anaesthesia remains unknown. It was first described in 1968 and since then there have been a small number of case reports outlining its occurrence as a benign, self-limiting condition in both adult and paediatric populations undergoing a wide variety of surgical procedures under general anaesthesia. It can present as a unilateral or bilateral swelling of the parotid gland with or without oedema or pain and can occur at any time intraoperatively or postoperatively. 1
Differential diagnoses of acute facial swelling in this context include:
Acute parotitis due to infective causes (bacterial or viral) or non-infective causes (allergic, traumatic or autoimmune, such as human immunodeficiency virus or Sjogren’s syndrome); Acute parotid duct obstruction due to ductal stone, tumour or hyposecretion (secondary to anticholinergic drugs) resulting in increased salivary viscosity; Pneumoparotid due to retrograde flow into salivary duct associated with high inflation pressures; Venous pooling from prolonged head-down position; Acute angioedema due to anaphylaxis, drug-induced causes (angiotensin-converting enzyme inhibitors or non-steroidal anti-inflammatory drugs), or hereditary causes (C1-INH deficiency). Early exclusion of angioedema is important as this may worsen swelling of tissues and cause acute airway obstruction.2,3
We recommend that diagnosis and management should commence with a systematic approach; prioritising visualisation and protection of the airway with endotracheal intubation if swelling is present, a review of drugs administered to the patient, followed by investigations including nasopharyngeal swab, FBC, electrolytes, amylase, serial tryptase, complement screen, CRP and USS imaging. Further imaging (computed tomography, magnetic resonance imaging or sialography) may be indicated at a later stage upon follow-up with ORL services.
Our case occurred during a repeat elective proctoscopy procedure. Development of bilateral parotid swellings occurred following administration of drugs that our patient had been given for previous general anaesthetics and following an uncomplicated LMA insertion. The induction was performed supine with the head in a neutral position. Both parotid glands steadily enlarged following LMA insertion but remained stable during the operation and subsided 12 h postoperatively. The patient did not experience pain, airway compromise, dysphagia or dysphonia. Obstructive, traumatic, infective, drug-induced and autoimmune differential causes were excluded following negative USS and blood results. Our clinical diagnosis was made based on descriptions outlined in similar case reports and on the basis that, like these similar case reports, spontaneous resolution was achieved without pharmacological intervention or subsequent complications.
We identified 15 case reports describing a total of 18 patients who developed bilateral parotid swellings in the context of general anaesthesia. Dates of these case reports ranged from 1968 to present day.1,4 The majority of these reports occurred in adults with well-controlled comorbidities (epilepsy, hypertension, reflux and chronic hepatitis B).5–9 Ages ranged from three to 73 years. All surgery was elective and included craniotomy,5,6 carotid endarterectomy, 7 thyroidectomy, 8 lumbar spine fixation,4,9 hysterectomy,10–12 caesarean section,13,14 laparotomy,14,15 upper limb orthopaedic surgery 16 and urological surgery. 17 Two cases documented co-induction with midazolam, more than half received fentanyl and all cases used either propofol or thiopentone for induction.
All cases were intubated orally using either suxamethonium or rocuronium, with neostigmine/glycopyrrolate or sugammadex for reversal. Less than half were bilateral. Unilateral swellings did not appear to have a correlation with intraoperative head position.4–6,9 Swelling was first noticed postoperatively in all cases except one. Kiran and colleagues reported bilateral parotid swellings whilst bag-mask ventilating a patient following two failed intubation attempts. 8 Due to concern regarding airway obstruction an emergency tracheostomy was performed. The parotid swellings subsided, and the patient was successfully extubated with no further complications. In all cases complete resolution was achieved in less than two weeks with conservative management. Complications were reported in only two cases, who developed self-limiting vocal cord palsies.5,6
Several authors have postulated the underlying aetiology of this phenomenon. However, a definitive underlying cause is yet to be proven. Among these theories is the potential vasodilation of parotid vasculature associated with vagal nerve stimulation upon intubation or mechanical laryngeal trauma. 6 Head position has also been identified as a possible cause where venous pooling and perioral congestion associated with prone, lateral or Trendelenburg positions may also contribute towards the development of swelling.6,10,17 Head extension or lateral positions have been thought to cause glandular ischaemia through arterial and venous compression. 6 Retrograde flow through Stensen’s duct due to straining and coughing 17 or retention of secretions in salivary glands due to dehydration or anticholinergics were also proposed.13,15,17 High airway pressures generated during bag-mask ventilation can cause air to enter the parotid orifice and obstruct excretory ducts, creating a pneumoparotid. 4 Excretory duct obstruction due to calculi or thickened secretions can precipitate bacterial infection, causing purulent sialadenitis. 18 Although few case reports documented morphine use, a possible adverse drug reaction to morphine has been considered by Kenningham. 19 It was proposed that the ability for morphine to reduce amylase secretion from isolated parotid acini may have precipitated this occurrence. 19
The genesis of this event in our patient has not been definitively explained by the aforementioned hypotheses. Mechanical trauma is unlikely given the ease upon insertion of a well-fitted LMA. Our patient remained supine or in lithotomy position with neutral head alignment throughout the procedure, thus perioral congestion and venous pooling were unlikely. Excretory duct obstruction was excluded based on intraoperative USS findings. Pneumoparotid was unlikely due to low inflation pressures and lack of free gas on intraoperative USS. Infective causes were excluded due to negative swab cultures, normal white cell count and low inflammatory markers. Anaphylaxis or adverse drug reactions were deemed unlikely due to normal serial tryptase, lack of eosinophilia and the fact that none of the aforementioned drugs associated with drug-induced parotid swelling had been administered. Although acute facial swelling in this context is a benign, self-limiting condition it is important to exclude other causes which may be life-threatening or require definitive treatment.
In summary, acute parotid swelling (‘anaesthesia mumps’ or ‘acute sialadenosis’) is a rare and benign condition that has been associated with general anaesthesia. This case report reiterates its self-limiting nature and that its occurrence can occur following LMA insertion. This phenomenon appears to arise in a wide range of patients and surgeries, making it difficult to predict the likelihood or time course of developing this condition. If perioperative parotid swelling occurs in the absence of anaphylactic, autoimmune, infective, obstructive or traumatic causes, clinicians should be reassured of its benign presentation and that this condition will resolve spontaneously without treatment. We recommend that acute airway management algorithms should still be followed for patients who develop this condition. If no further changes or progression occur, surgery can continue as planned.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to acknowledge Dr Edward Hughes, specialist anaesthetist, and Gary Boxall, anaesthetic technician, for support during the acute intraoperative management of this case.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.