
Abstract
Returning to work in critical care after a break in clinical practice can be a daunting process. This article describes development and evolution of the Critical Care, Resuscitation, Airway Skills: Helping you return to work (CRASH) course, including the supporting literature. CRASH is the first bi-national course assisting return to work (RTW) for critical care practitioners. It evolved as a collaborative effort across Australia and New Zealand, involving anaesthetists, emergency physicians and intensivists. The course is based around tailored sessions practising skills and clinical decision-making using simulation and case discussions, incorporating practical tips on returning to work. Participants receive resources to assist RTW including questionnaires and checklists developed by the faculty, which have been used to aid RTW in more than 30 hospitals in Australia and New Zealand. Attendance is open to all critical care practitioners who are registered with the relevant medical board and returning to work, who have taken leave from work for any reason. Since 2014, 197 participants have attended CRASH in-person or virtually, one of the largest RTW groups described in the literature. The aim of this article is to outline the literature around inactivity and RTW, and describe the development and adaptation of the CRASH course.
Introduction
Returning to work after clinical inactivity is a challenging time in a doctor’s career. Extended periods of inactivity may result in attrition of medical practitioners, with long-term workforce implications. 1 Data on inactivity is sparse and may be inaccurate. 2 Helping competent doctors return to work (RTW) successfully has broad economic benefits as well as improving individual practitioner wellbeing. 3
RTW programmes exist overseas which may target anaesthetists 4 or a range of specialties. 5 programmes in the United States are geographically diverse,6–9 time-consuming, 10 resource-intensive 7 and broad enough to cover multiple disciplines. 6 Many of them are expensive, costing upwards of US$6000. 10 The United Kingdom has an anaesthesia-specific course, Giving Anaesthesia Safely Again (GAS Again), developed in 2012 and adapted to virtual in 2021. 11 An anaesthesia-specific course is currently in development in Canada. 12
Prior to 2014, there were no national RTW courses or programmes for doctors in Australia or New Zealand. The faculty, experienced in RTW, recognised a role for developing a course which would provide targeted education, meet continuing professional development requirements and offer practical advice on navigating RTW. We expected the objectives of improving confidence and refreshing skills could be met through a one-day course, based on the GAS Again faculty experience. Our intention was to create a cost-effective, accessible, modifiable curriculum10,13 including planning resources which could be used by individuals and departments to support RTW.
The Critical Care, Resuscitation, Airway Skills: Helping you return to work (CRASH) course targets critical care vocational trainees and specialists who have not practised clinically for at least three months (a period of time which correlates with perceived skill deterioration), 14 and who are registered with either the Medical Board of Australia or the Medical Council of New Zealand. After three years of providing an anaesthetic-focused curriculum, the curriculum was expanded to include content relevant to emergency and intensive care physicians, in response to a lack of specialty-specific return to work courses and overlapping scope of practice. Initially a bi-annual Melbourne course, CRASH expanded over five years to run several times a year in multiple locations across Australia and New Zealand. Transition to a virtual format occurred due to travel and social distancing restrictions related to the coronavirus pandemic. In the eight years since inception, more than 190 doctors who are returning to work have attended CRASH. In line with expert recommendations for RTW programmes,3,13 propagation and development of the course continues through constant course evolution, central oversight and development of local faculty, and provision of RTW resources (see Appendix 1, available online). The resources developed by the faculty have been implemented in more than 30 hospitals in Australia and New Zealand, including departments of anaesthesia, intensive care and emergency medicine. The course was developed using published guidance on RTW programmes, by a national faculty with iterative development of course content based on feedback from participants and faculty, supported by resources in use across Australia and New Zealand. The curriculum focuses on the clinical aspects of RTW but CRASH also aims for participants to benefit from the collective knowledge of the faculty in their RTW experiences. This article aims to describe the rationale and development of the CRASH course, including the evolution of the course over the first eight years and adaptation to a virtual platform in response to travel restrictions.
Background
Physician inactivity is variably defined in the literature as from 3–36 months away from clinical practice6,15 to working less than 20 h per week in either clinical or non-clinical work. 16 The number of doctors returning to work after more than three months’ leave is estimated to be 1%–4% annually in the United States (US). 6 The American Medical Association’s Masterfile had a sensitivity of only 9% in detecting inactivity, 2 with the definition of ‘inactive’ including doctors working less than 20 h per week in any role, including non-clinical work. 16 Australian practice differs from US practice, with greater availability of part-time work and longer entitlements to leave (including parental and long service leave). 17 A survey of inactive physicians in the US found that the most common reasons for inactivity were personal health, caring for young children, and administrative burdens. 16 Similar data is not available for critical care practitioners in Australia. Data from the Medical Board of Australia suggests that 2.3% of doctors are non-practising, 18 although doctors on leave for less than 36 months may maintain registration. Australian and New Zealand College of Anaesthetists (ANZCA) trainee data indicates 12%–15% are in interrupted training, 25% of these on parental leave and the remainder not specified (personal communication, Wilson L, Executive Director, Professional Affairs, ANZCA). In New Zealand, 23% of doctors with an anaesthesia scope of practice do not have a current practising certificate; however, many of these are likely retired or overseas (personal communication, Vercoelen H, Team Manager, Practising Certificates, Medical Council of New Zealand).
With increasing numbers of women in the workforce, and increasing graduate prevocational medical training, more clinicians will seek to take extended leave during training or early consultant practice. Forty-five percent of ANZCA trainees are female, but of trainees who take parental leave, 96% are women. 19 Returning to work during career transitions can be challenging, both professionally and personally.20,21 Many of these challenges may be anticipated, such as meeting governance requirements and maintaining competence. Others are not modifiable, including practitioner characteristics such as age or health.6,22
Both employers and practitioners are concerned about skill attrition in returning to work.23,24 Some studies failed to differentiate between doctors returning after a period of family leave or sick leave, and those who required remedial education or revalidation. 10 Other studies have demonstrated differences in competence between these groups.4,10,23 Previously competent doctors have a good prognosis for RTW, although doctors who ceased work due to disciplinary issues are less likely to demonstrate competence on RTW assessment. 22
In a survey in the US, 85% of inactive doctors believed that the process of RTW would be challenging, regardless of whether RTW had been attempted. 16 Barriers to RTW have been described in medical and population literature, summarised in Figure 1. Poor prognostic factors include individual characteristics,6,23,25 workplace characteristics, including discrimination,16,23,25–27 and the ‘hassle factor’ of returning to work.16,23 These barriers may dissuade physicians from continuing clinical medicine1,3 and result in reduction in working hours 21 or in women being less likely to take on leadership roles after returning from maternity leave.27–30
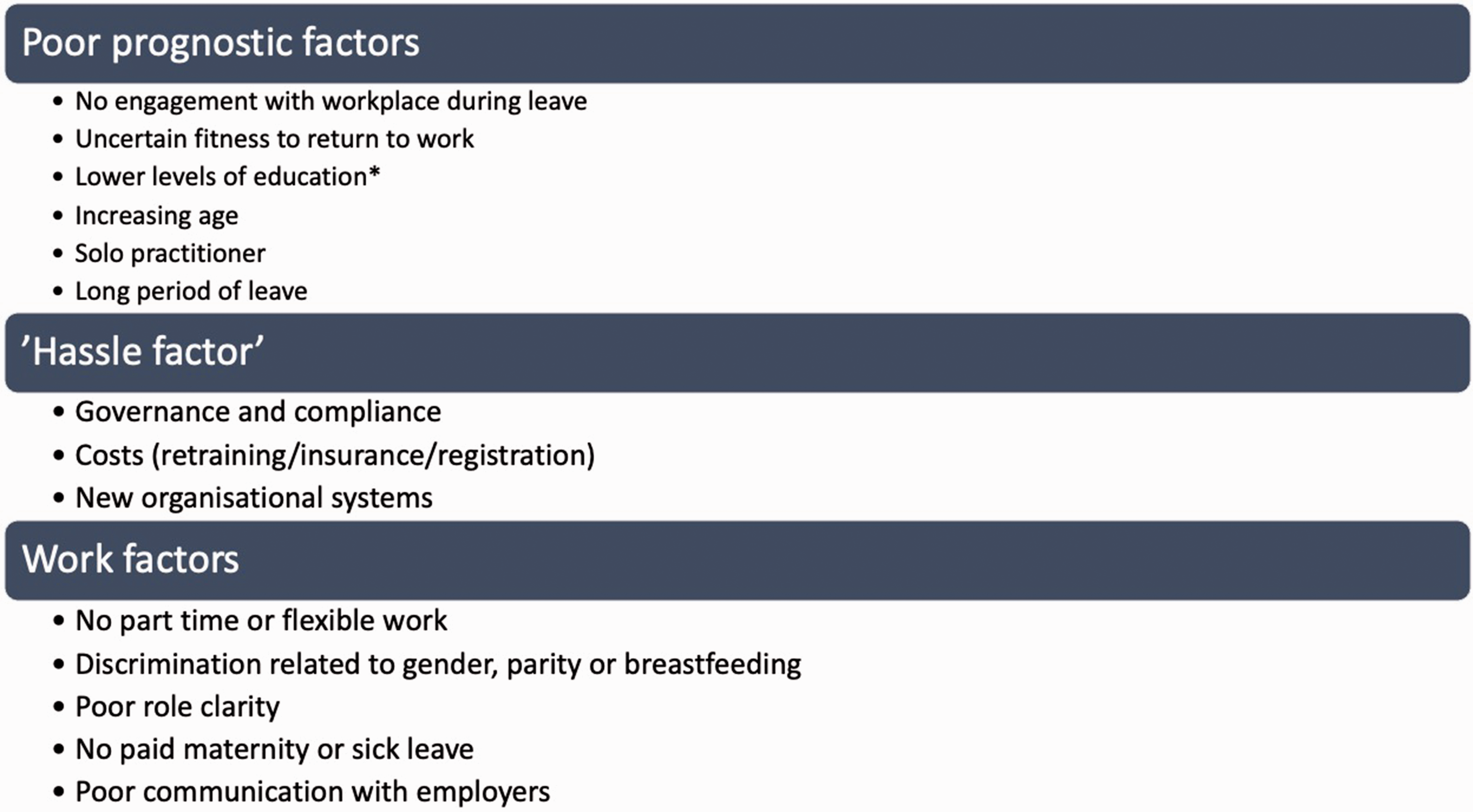
Barriers to returning to work.
Requirements for re-entry to practice in Australia and New Zealand are summarised in Figure 2. These vary based on length of time off and pre-leave experience and are governed by regulations from the Medical Board of Australia, the Australian Health Practitioner Regulation Agency (AHPRA), the Medical Council of New Zealand (MCNZ) and the relevant colleges.
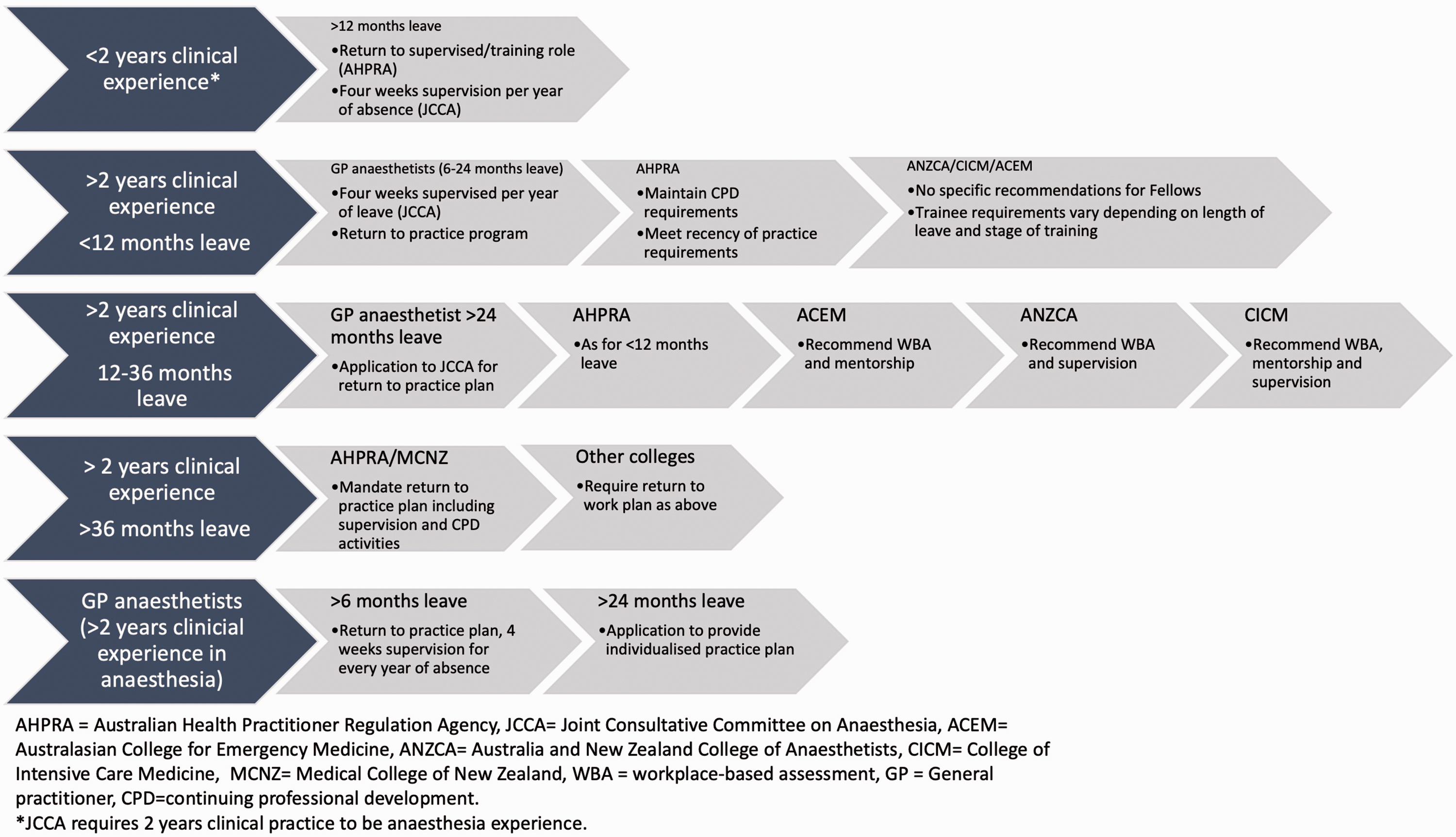
Return to practice requirements.
After 36 months of leave, the process of return to work is overseen by the relevant college as mandated by AHPRA or the MCNZ. Practitioners are required to undertake a return to work plan including continuing professional development and which may include periods of supervised practice. Guidance is provided by the individual colleges, including incorporating mentorship, 31 workplace-based assessment31–33 and supervision.31–33 Each college has a committee or assessor who oversees the process.
Although there are no requirements for return to practice for periods of leave under 12 months, many clinicians may experience decreased confidence in clinical decision-making, procedural skills, and management of emergencies. This can impair the RTW process. 34 Building confidence with explicit strategies in combination with didactic instruction has been effective in returning doctors to work in other programmes.34,35 Our aim was to develop a one-day course offering an opportunity to refresh skills, underpinned by practical guidance in managing RTW, with strategies to build confidence embedded in the instruction.4,36
Course development
A group of clinicians (led by JW and KA) with medical education and clinical content expertise met to establish faculty characteristics, curriculum development and evaluation strategy for the course. Faculty recruitment occurred through professional networks Australia-wide, commencing in 2013. The ideal faculty member was defined as having a minimum of seven years’ clinical experience, educational qualifications and personal experience of RTW after more than three months’ leave. An initial meeting of a core group of faculty designed an outline for the course (see Figure 3) and development of the evaluation instruments. Faculty development occurred through pre-course meetings and online resources. A faculty handbook outlines the learning objectives, teaching plans and common discussion points for each module. Prior to travel restrictions, faculty members from each location taught on courses in other locations, providing consistency and adaptation of delivery for participants from all regions. Emphasis was placed on the supportive functions of the course, including embedding simulation through all sections of the course with debriefing strategies designed to help participants manage cognitive load.
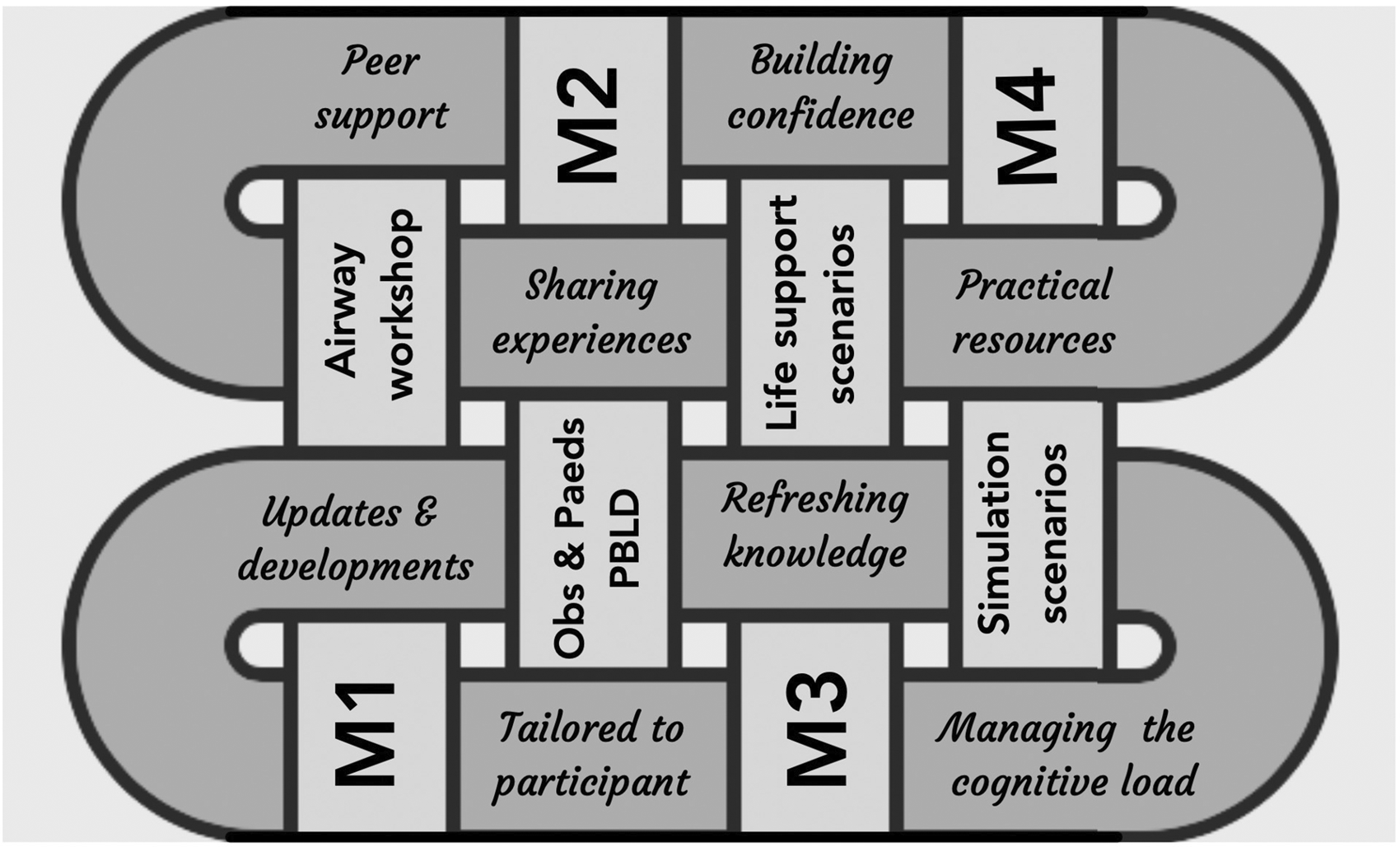
Four modules (M) of the course linked with themes of course including integrated support tailored to participant group.
CRASH was designed initially as a refresher course for anaesthetists returning to work. Using the expert guidance of principles for physician re-entry programmes,3,10,13 the initial modules of CRASH (see Figure 3) were assigned to clinical leads, and developed by subgroups of faculty, with cross-checking by others. Ongoing iterative development of the initial curriculum framework by course faculty occurred at every course based on participant feedback. Lead facilitators (including SB, BV and EL) for each section of the course were overseen across regions by the course convenors (KA and JW).
The CRASH course was not designed with an assessment component for several reasons, including feasibility, applicability and acceptance by participants. Assessment of one participant is resource-intensive for faculty and requires training and robust assessment tools. While much of the literature has grouped all returning practitioners together, some studies have highlighted significant differences in the requirements of practitioners who have had disciplinary or regulatory issues and those whose competence and performance were not in question prior to leave.6,10,23 Assessment of competence is not applicable for most of the participants of the course. Most participants lack confidence, but there is no compelling evidence that competence is significantly affected by clinical inactivity. 14 A lack of confidence can reduce work rate and decrease practitioner wellbeing14,37,38 but is not directly correlated with competence, particularly in the RTW setting. Formal assessment of competence was judged to be an unnecessary burden on both faculty and participants and was therefore not incorporated into the design of the course. Ethics approval has been gained for research involving CRASH course participants but was not required for reporting course development.
Course evolution
The first course was piloted in Melbourne in January 2014. Initial advertisement was by word of mouth, and by January 2015 participants were attending from most states in Australia and from New Zealand. Interstate faculty successfully piloted CRASH Perth (in conjunction with the ANZCA Annual Scientific Meeting (ASM)) and CRASH Brisbane, both in 2017. A further course was piloted in Auckland in 2018 at the request of the organising committee of the New Zealand ASM. Expressions of interest were received from intensive care and emergency faculty about expanding the course, which resulted in development of specific modules for these groups. Several key strategies were utilised in the expansion of the course, including identification of senior faculty in each location, cross-pollination of faculty, and faculty development.
The timeline of the course is outlined in Figure 4. A needs analysis is performed six weeks prior to course delivery to guide selection of curriculum components of each module. Participants self-assess confidence across specialty-specific domains, including complex procedures and management of emergencies. This determines the specific components and scenarios of the core modules that will be run for each course, based on specialty mix and career stages of participants. For example, a heterogeneous participant group including intensive care, emergency medicine and anaesthetists will require an interprofessional curriculum designed around clinical scenarios common to any practice (e.g. emergency intubation, haemorrhage, myocardial ischaemia). Post-course evaluation by participants is performed as an anonymous survey on the day of the course, and at six weeks post-attendance. Faculty evaluation occurs post-course with detailed feedback to the convenors.
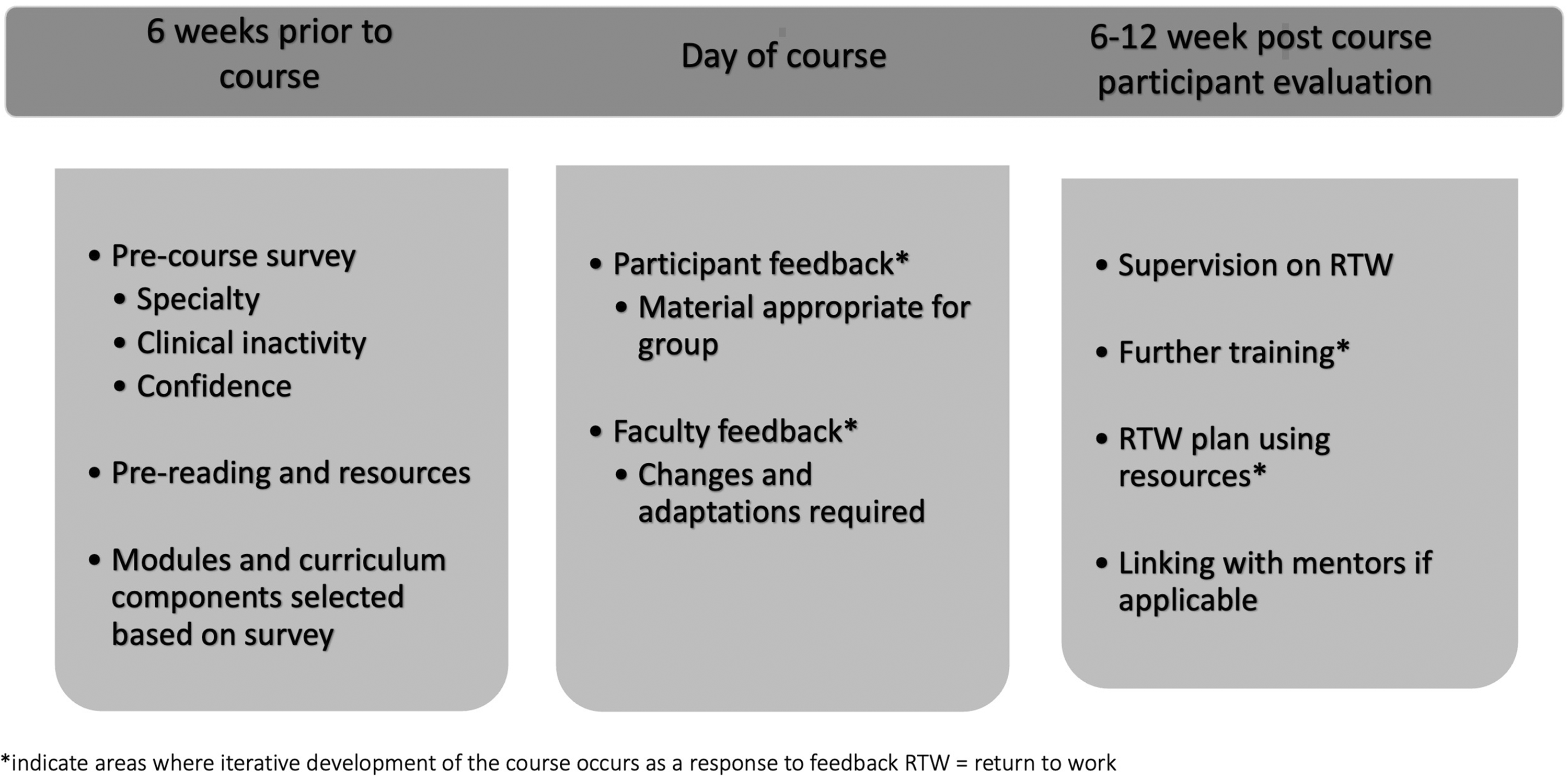
Timeline of Critical care, Resuscitation, Airway Skills: Helping you return to work (CRASH) course.
A pre-reading and resource package is emailed to participants in advance. This includes emergency algorithms, recent updates or significant changes to practice and resources for planning a successful return to work (see Appendix 1). Material is revised by the curriculum leads to update participants on recent changes in practice or recommendations by specialist colleges. This resource package is in use in many anaesthetic departments in Australia and New Zealand.
Tailoring and planning each course is centralised to the convenors, who are based in Melbourne and regularly instructed on courses in all locations, prior to the pandemic. The course content is scrutinised pre- and post-course and amended based on feedback from faculty and participants.
Adaptation in COVID-19 pandemic
Both travel and in-person education were curtailed due to the coronavirus pandemic in 2020. Returning to work in a rapidly changing environment is challenging, and demand for CRASH has continued, with inclusion of practice changes relevant to the pandemic. The faculty met to develop a virtual course, supplemented by in-person workshops with infection control protections. The curriculum was divided into three components present in each module: didactic content, group discussions and scenario delivery (virtual and face-to-face). Didactic content is delivered by online lectures prior to the course. Group discussions, including virtual scenario delivery, are facilitated by national faculty via a live virtual meeting hosted on a video conferencing platform. Where possible, participants attend a half-day workshop for further scenarios. This curriculum has been delivered five times to 77 participants across Australia and New Zealand. The increase in accessibility is offset by several challenges. These include no opportunity to practise skills, fatigue due to the virtual platform, and a lack of networking and peer support that a face-to-face course provides. The faculty, however, are committed to meeting the needs of critical care practitioners returning to work at this challenging time and continue to modify the course to optimise delivery and ensure sustainability.
Course participants
Demographic data is available for 174 of the 197 participants of the course, collected via anonymous pre-course survey. Most respondents were women (155/174, 89%), and were returning from parental or sick leave (145/174, 83%).
Most participants were senior anaesthetic trainees and consultants (see Table 1). This may reflect the increased responsibility for senior trainees, who may not be supervised when returning to work, particularly during out-of-hours work, as well as a congruency between starting a family and completing training. Lower numbers of participants from other critical care specialties may reflect the later addition of specific content to the course, and the anaesthetic centric nature of the virtual course.
Classification of participants in the Critical Care, Resuscitation, Airway Skills: Helping you return to work (CRASH) courses.
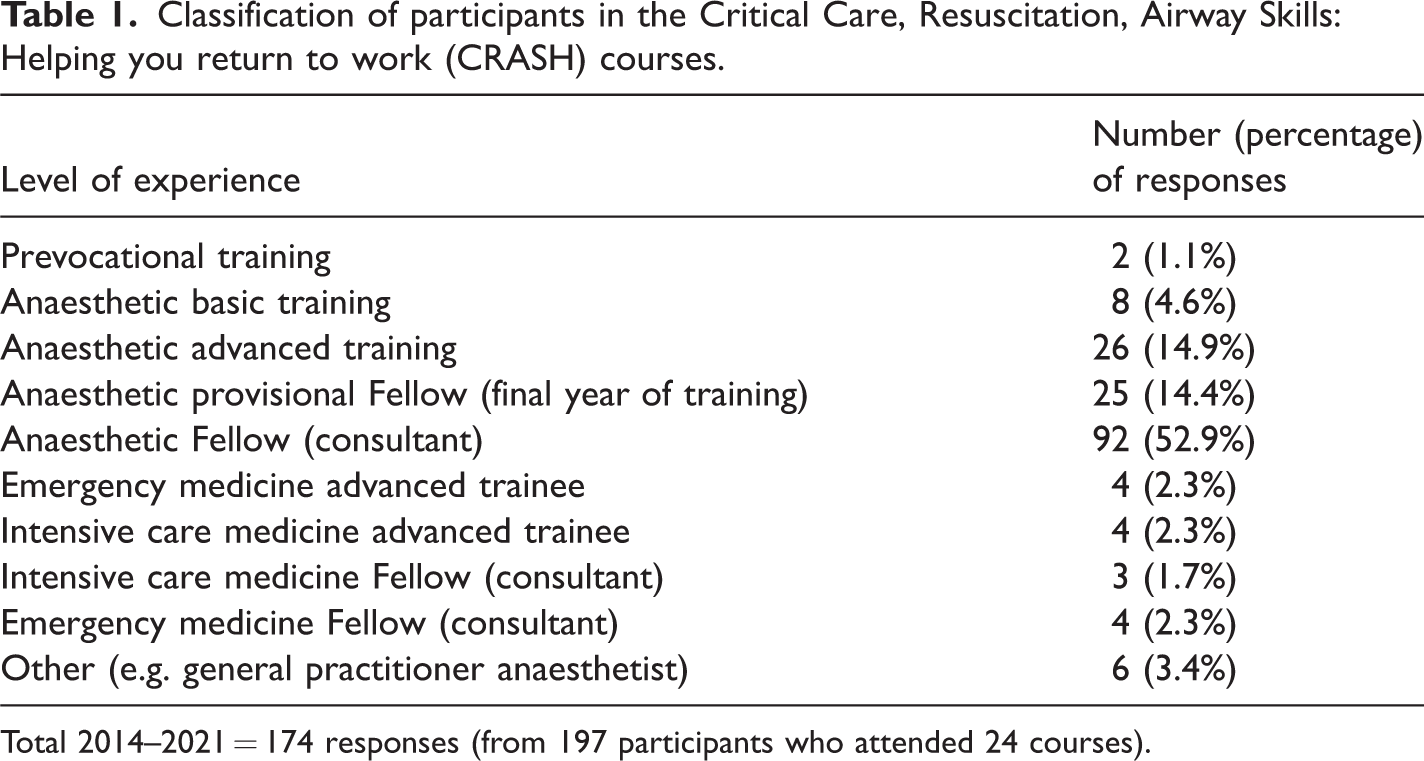
Total 2014–2021 = 174 responses (from 197 participants who attended 24 courses).
Future plans
Limitations of the course include balancing the needs of multiple craft groups, optimising timing for participants to coincide with RTW and virtual faculty development. We believe that the commitment of the faculty providing the course and offering guidance to individuals within departments who are returning to work is a critical component of the sustainability of CRASH. Outcomes in RTW are important and influenced by multiple factors, some of which are summarised in Figure 1. Future directions include investigation of these factors for doctors returning to work. Our goal is for CRASH to remain accessible, possibly in a hybrid format with a combination of virtual and face-to-face modalities, offered at regular intervals in multiple locations, including at anaesthetic meetings. We also hope to create a network of doctors with RTW experience who can proactively support others through the process, with resources and mentoring, outside the confines of the course, so that every department in Australia and New Zealand can help doctors safely and confidently return to work.
For further information and to register for the next CRASH course, please see https://www.thermh.org.au/health-professionals/continuing-education/anaesthesia-and-pain-management-courses/crash-course
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X221094048 - Supplemental material for Eight years of CRASH: A bi-national initiative helping critical care doctors return to work
Supplemental material, sj-pdf-1-aic-10.1177_0310057X221094048 for Eight years of CRASH: A bi-national initiative helping critical care doctors return to work by Kara J Allen, Janette C Wright, Emelyn M Lee, Brooke J Vickerman and Sheila G Barnett in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X221094048 - Supplemental material for Eight years of CRASH: A bi-national initiative helping critical care doctors return to work
Supplemental material, sj-pdf-2-aic-10.1177_0310057X221094048 for Eight years of CRASH: A bi-national initiative helping critical care doctors return to work by Kara J Allen, Janette C Wright, Emelyn M Lee, Brooke J Vickerman and Sheila G Barnett in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The CRASH faculty are indebted to the GAS Again faculty, who kindly shared their knowledge of the challenges of a RTW course. Additionally, we wish to thank Elizabeth Leslie, Barbara Heath, Lara Tickell, Allanah Scott, Megan Allen, Juliana Kok, Annick Depuydt, Tim Byrne, Matt Durie, Mya Cubitt, Alexandra Donaldson, Belinda Lowe, Jade Radnor and Patricia Newell, who have contributed to the development and expansion of the course.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.