
Abstract
Superior mesenteric artery (SMA) thrombosis is a critical illness and requires prompt intervention to obtain a good clinical outcome. 1 Revascularisation after prolonged ischaemia of a significant amount of intestinal tissue often induces remote organ injury, acute metabolic lactic acidosis and hyperkalaemia which can induce a severe cardiac event (e.g. ventricular fibrillation and asystole), as a so-called ischaemia reperfusion injury (IRI). 2 , 3 We report the case of a patient with a SMA thrombosis that required surgical embolectomy of the SMA, and we describe the efficacy of phlebotomy from the superior mesenteric vein (SMV) just after revascularisation to prevent life-threatening hyperkalaemia during surgery. The patient provided informed consent for the publication of these details.
A 79-year-old Japanese man, height 166 cm and body weight 72 kg, complained of severe upper abdominal pain for ten hours. He had untreated atrial fibrillation (heart rate 120–150 per minute) and diabetes mellitus. Abdominal and pelvic computed tomography revealed thrombus of the SMA, thus an emergency partial resection of the small intestine and embolectomy were planned under general anaesthesia.
Due to the patient’s comorbidities, an invasive arterial line was placed with the patient under local anaesthesia prior to the induction of general anaesthesia. The arterial gas analysis revealed presenting severe acidaemia, respiratory and lactic acidosis and hyperglycaemia (Table 1). Rapid sequence induction and tracheal intubation with fentanyl (100 µg), ketamine (80 mg) and rocuronium (70 mg) was successful without aspiration pneumonia or hypotension. Anaesthesia was maintained with propofol, ketamine and fentanyl. A central venous double-lumen catheter and vascular access were inserted at the right internal jugular vein and the right femoral vein, respectively. Noradrenaline (0.1–0.2 µg/kg/min) and landiolol (2–3 µg/kg/min) were administered to maintain the patient’s haemodynamic condition. Regular short-acting insulin (2–3 U/hour) was also required to control serum glucose and potassium concentrations.
Changes in arterial and superior mesenteric venous blood gas analysis.
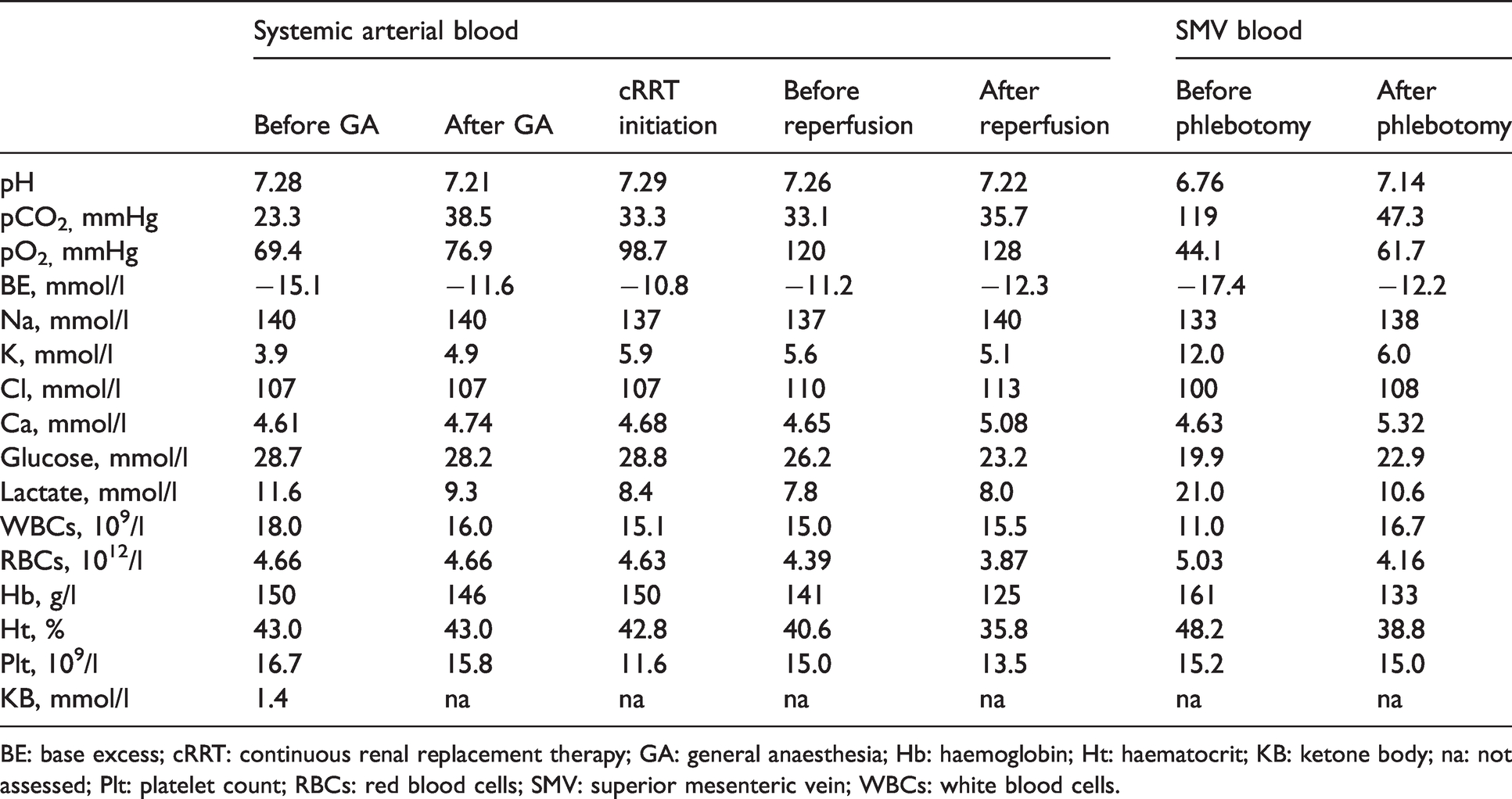
BE: base excess; cRRT: continuous renal replacement therapy; GA: general anaesthesia; Hb: haemoglobin; Ht: haematocrit; KB: ketone body; na: not assessed; Plt: platelet count; RBCs: red blood cells; SMV: superior mesenteric vein; WBCs: white blood cells.
As the small intestine was not completely necrotic, the surgeon performed a SMA embolectomy with a 4-Fr Fogarty catheter. Due to the patient’s hyperkalaemia (5.9 mmol/l) and acidaemia (pH 7.29) and to prevent IRI as well as the risk of hyperkalaemic cardiac arrest after revascularisation of the SMA (Table 1), continuous renal replacement therapy (cRRT) via the right femoral vein was started 25 minutes after the initiation of the surgical procedure. The blood flow rate and the dialysate flow rate of the cRRT were 100–120 ml/minute and 2000 ml/hour, respectively.
Despite the initiation of cRRT, the patient’s hyperkalaemia remained unchanged at the end of the embolectomy (Table 1) and, before reperfusion, a phlebotomy from the SMV via an 18-G catheter (catheter length 48 mm) was conducted to prevent life-threatening hyperkalaemia. The blood gas analysis of the initial reperfusion blood taken from the SMV revealed severe acidaemia and hyperkalaemia (12.0 mmol/l) (Table 1). After 500 ml of blood was removed via the phlebotomy, the potassium concentration of the SMV blood decreased to 6 mmol/l (Table 1) and thenceforth the venous blood flow was returned to systemic circulation. No peaked T-wave changes were observed on electrocardiogram, and the lactic acidosis and hyperkalaemia gradually improved during the surgery (Table 1). The surgery’s duration was one hour 23 minutes, and overall blood loss including the blood extracted from the SMV was 680 ml. After the surgery, the patient was admitted to the intensive care unit and heparin was continuously administered at 400 U/hour.
A second-look laparotomy and an embolectomy of the bilateral deep femoral arteries were conducted 12 hours after the initial surgery. As some extent of the small intestine was necrotic, a partial resection of the small intestine and an ileostomy were conducted. On postoperative days one and six, additional resection of the small intestine and an amputation of the right thigh were required, respectively.
We have described the case of a SMA thrombosis which required surgical embolectomy of the SMA; a simultaneous phlebotomy from the SMV prevented life-threatening hyperkalaemia and acidosis. This case provides a new therapeutic option to prevent an acute IRI after revascularisation of the SMA.
Phlebotomy from the SMV could be a therapeutic option to prevent hyperkalaemia and acidosis after revascularisation of the SMA in addition to cRRT during surgery. However, the efficacy of phlebotomy for preventing an IRI after revascularisation of the SMA has not been well evaluated. This report may be the first to show that an intraoperative blood gas analysis revealed the changes in potassium concentration in the SMV blood before and after phlebotomy. After we confirmed that the patient’s potassium concentration had decreased, the SMV blood flow was thence returned to the systemic circulation. These steps were essential to ensure the patient’s safety, because hyperkalaemia could induce cardiac arrhythmias when a vast amount of the small intestine was reperfused after several hours of ischaemia. In an experimental rat model, the post-reperfusion serum potassium concentration after the occlusion of the SMA for 60 minutes was increased to a mean (standard deviation) of 6.0 (0.8) mmol/l even though the potassium concentration before reperfusion was 4.4 (0.2) mmol/l. 4 This result suggests that in our patient’s case, the potassium concentration after reperfusion could have reached a life-threatening level after reperfusion.
Our patient’s case suggests that phlebotomy from the SMV after revascularisation of the SMA can be a therapeutic option to prevent life-threatening hyperkalaemia and acidosis. A blood gas analysis of SMV blood may be a good indicator for determining the timing of reperfusion.