
Abstract
Major respiratory catastrophe associated with iatrogenic airway injury during the Sistrunk operation is a rare event. A three-year-old patient underwent thyroglossal duct cyst removal under general anaesthesia. An iatrogenic thyroid cartilage injury occurred in the intraoperative period, and it was repaired primarily. Later, in the post-anaesthesia care unit, the patient developed subcutaneous emphysema in the neck and face, and then pneumomediastinum and bilateral pneumothoraces. The patient was managed with bilateral chest drains and endotracheal intubation, and he required mechanical ventilation for three days. So, even after repair of a recognised iatrogenic airway injury associated with the Sistrunk operation, it may be necessary to continue positive pressure ventilation in the postoperative period to avoid serious respiratory complications.
Introduction
The Sistrunk operation is the standard procedure for the removal of thyroglossal duct cysts. It involves removal of the cyst, tract and part of the hyoid bone, with resection extending superiorly towards the base of the tongue.1,2
Major complications associated with the Sistrunk operation are not common; 3 however, there are reports of critical respiratory events associated with it.4,5 In our case, a paediatric patient developed pneumomediastinum followed by bilateral pneumothoraces due to iatrogenic thyroid cartilage injury during excision of a thyroglossal duct cyst.
The main purpose of this case report is to describe the complications that arose after a Sistrunk procedure, despite immediate surgical repair of a recognised injury. This case demonstrates that even after repair of the airway, an air leak may persist until the suture line has healed. Finally, an air leak test performed at the end of surgery may help in the detection of any breach in the integrity of the airway. Written informed consent was obtained from the patient’s mother for publication.
Case report
A three-year-old boy presented with a non-painful midline swelling on the anterior aspect of the neck. The lump was 3.5 cm by 2 cm in size, and it moved with both deglutition and tongue protrusion. On palpation, crepitus was felt while the laryngeal framework was intact. An ultrasound of the neck showed a well-defined cystic lesion with internal echoes and septations anterior to the isthmus. There was no history of other medical illness and all laboratory parameters were within normal limits. The patient was planned for a Sistrunk operation in a tertiary care hospital by an experienced otorhinolaryngologist.
After induction of general anaesthesia and adequate neuromuscular blockade, the airway was secured with a 4 mm internal diameter cuffed endotracheal tube (ETT). Anaesthesia was maintained with isoflurane and 40% oxygen mixed with air. Thereafter, volume control ventilation (tidal volume 6 ml/kg, rate 20/min, inspiratory to expiratory ratio 1:2) and standard monitoring were continued. The patient received intravenous dexamethasone 2mg, paracetamol 150mg, and ondansetron 1mg.
During the procedure, the thyroid cartilage was injured accidentally. The injury was an approximately 5 mm linear cut and it was repaired primarily. Haemodynamic and airway pressure parameters were stable throughout the surgery. At the end of the surgery, the trachea was extubated, and the patient was shifted to the post-anaesthesia care unit (PACU). He was conscious, and his initial vital signs were stable. Later, his respiratory and heart rate started to rise. The nursing staff noticed subcutaneous emphysema on the neck and face, and called immediately for anaesthetic assistance. The patient was in respiratory distress and his oxygen saturation was declining. The sequence of events and subsequent management is shown in Figure 1. Orotracheal intubation was performed immediately without difficulty, and bilateral chest drains were inserted to treat the bilaterally evolving pneumothoraces. A chest X-ray was performed, confirming bilateral pneumothoraces (Figure 2). After insertion of bilateral chest drains, the lungs expanded (Figure 3). The endotracheal tube was removed on the third day. The patient was transferred out of the intensive care unit on the fifth day. The chest drains on the left and right side were removed on the seventh and 14th day, respectively. On the 16th day, the patient was discharged from the hospital.
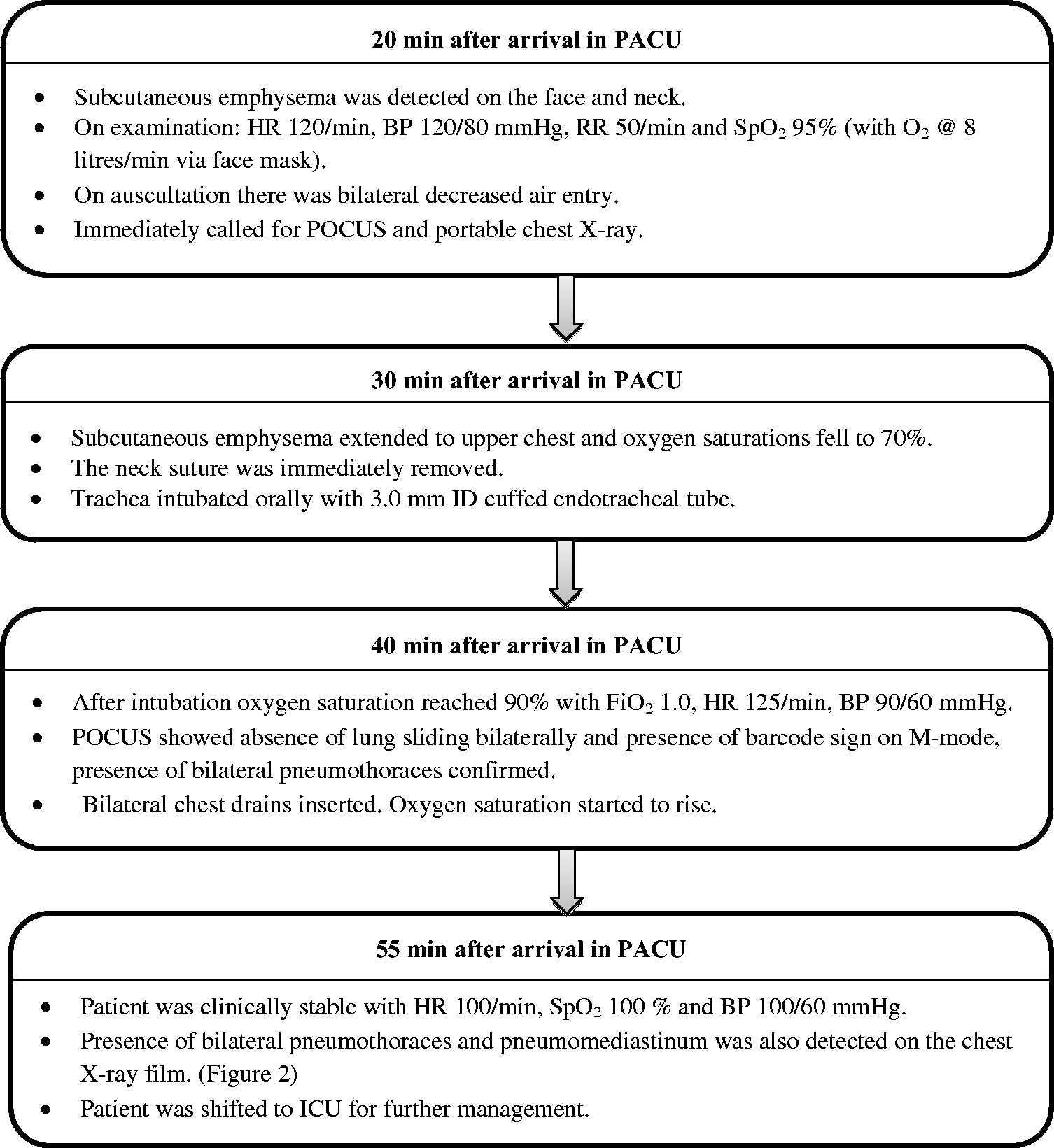
Flowchart of events and the subsequent management. PACU: post-anaesthesia care unit; HR: heart rate; BP: blood pressure; RR: respiratory rate; SpO2: pulse oximetry oxygen saturation; POCUS: point-of-care ultrasound; ID: internal diameter; FiO2: inspired fraction of oxygen; ICU: intensive care unit.
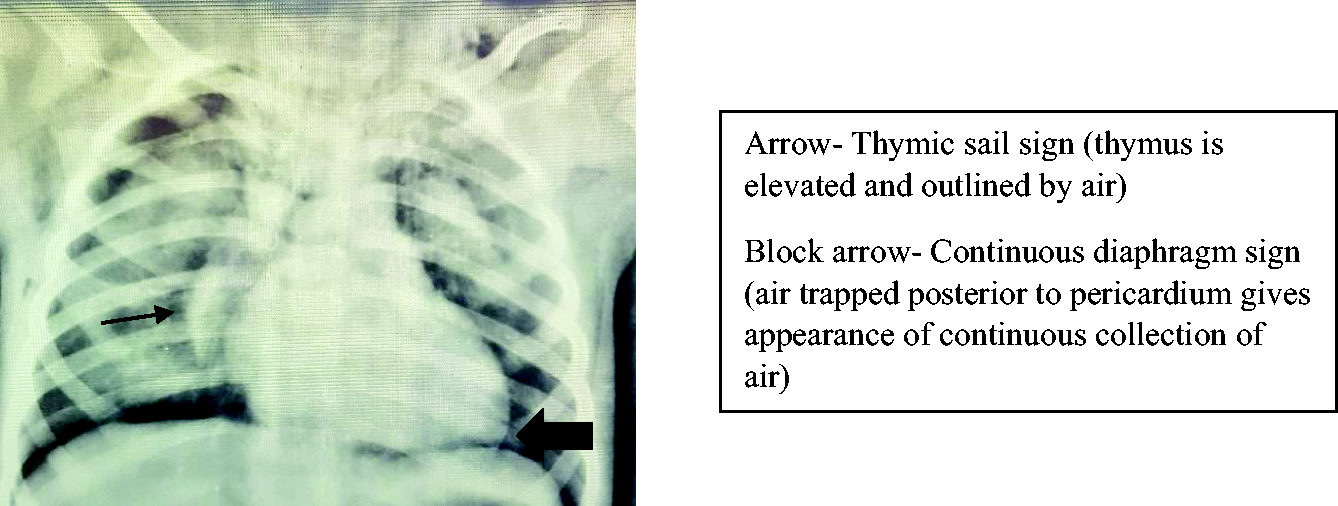
Pneumomediastinum with bilateral pneumothorax.
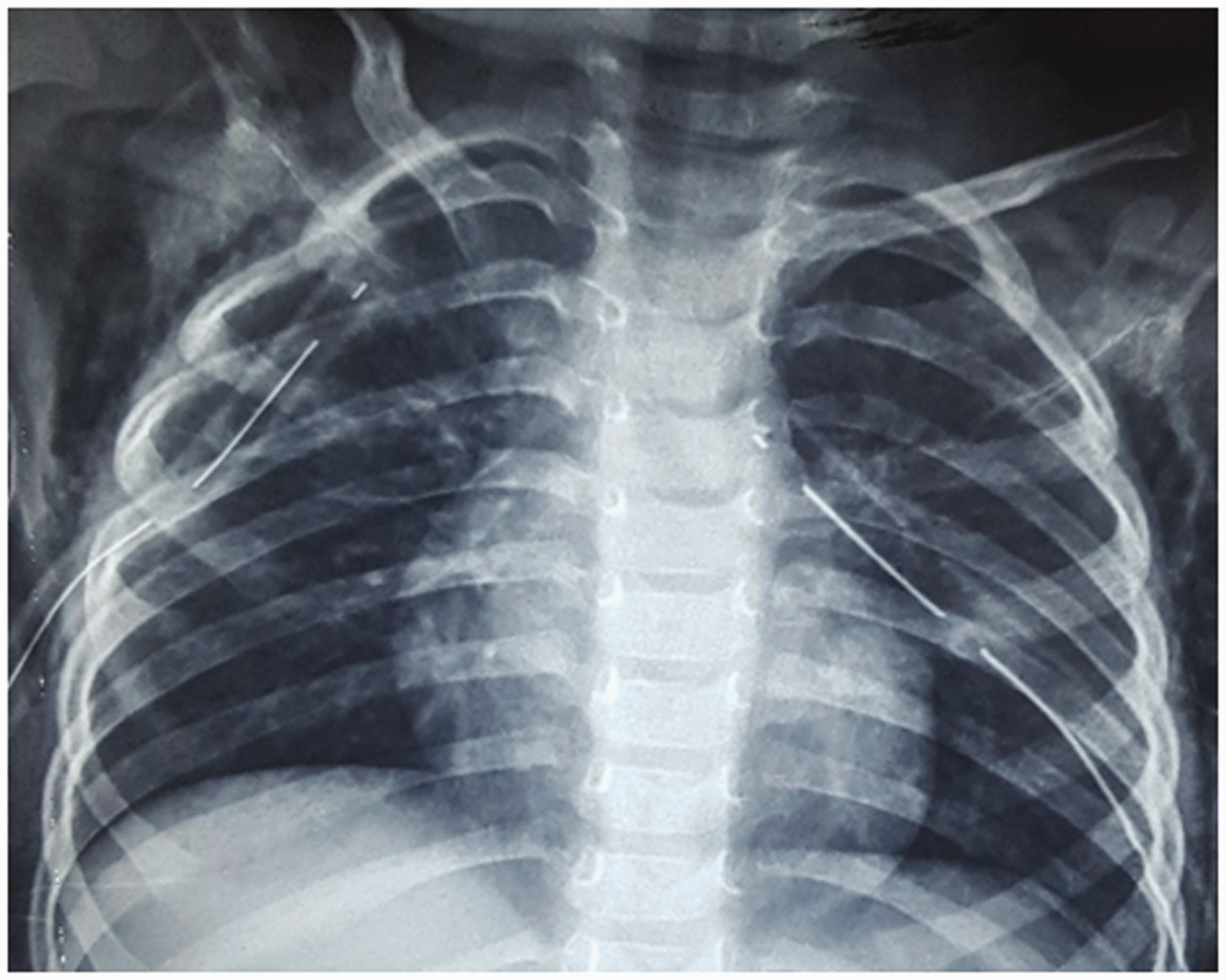
Lung expansion after bilateral chest drain insertion.
Discussion
Airway injury leading to respiratory catastrophes is a rare complication of the Sistrunk operation. In our report, despite primary repair of the iatrogenic thyroid cartilage injury, the patient developed pneumomediastinum followed by bilateral pneumothoraces in the PACU.
Several mechanisms describe the development of pneumomediastinum. 6 The possible explanation in our case is that as soon as the patient started to breathe spontaneously, atmospheric air entrained through the injured thyroid cartilage. This led to the accumulation of air in the pre-visceral and visceral spaces of the neck. With each respiratory effort, the amount of air in those spaces increased, resulting in subcutaneous emphysema in the upper chest, neck and face. Further, the air from the visceral space of the neck may have tracked into the mediastinum leading to pneumomediastinum. This increase in air pressure in the mediastinum led to the rupture of the mediastinal pleura causing bilateral pneumothoraces, as described in previous reports.7,8 A schematic diagram of the pathway taken by air is shown in Figure 4.
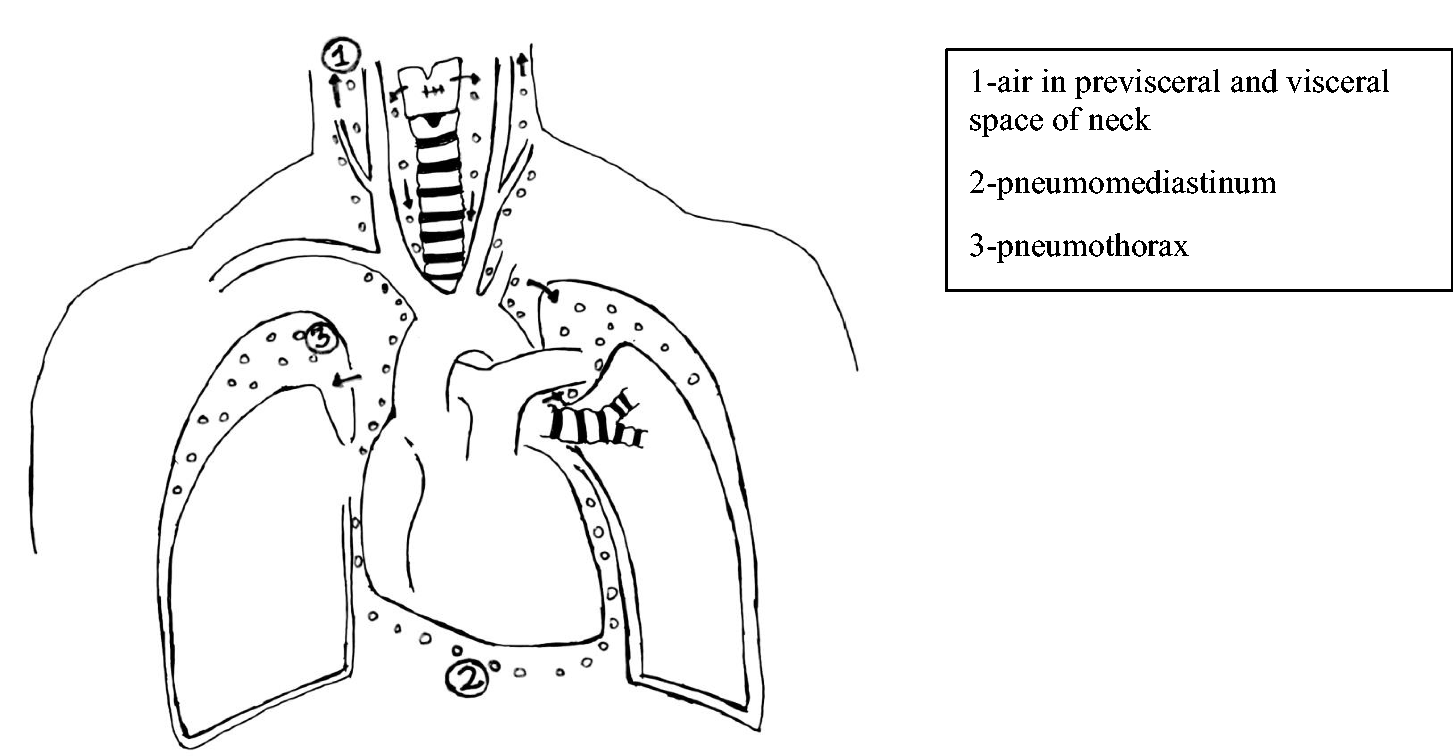
The schematic diagram of the pathway taken by air.
As per standard guidelines, laryngeal trauma is managed primarily by securing the airway, followed by either conservative or surgical treatment depending on the extent of the injury. 9 In a previous case report by Patel et al., 10 cricoid cartilage injury was unrecognised during excision of a thyroglossal duct cyst. Later, in the recovery room, the patient developed serious respiratory complications and required immediate endotracheal intubation. Surgical repair of the defect with a graft was performed. The patient required mechanical ventilation for a few days postoperatively. Similarly, in the case series by Wootten et al., 5 all patients with an airway injury sustained during a Sistrunk procedure eventually required laryngotracheoplasty and tracheostomy.
In contrast, in our case, the injury was minimal, and it was identified immediately and repaired. As we had used a cuffed ETT, and the injury site was above the ETT cuff, the haemodynamic and airway pressure parameters were stable after the repair of the injury. This led to a false sense of reassurance and the decision to extubate the patient. Unfortunately, during spontaneous ventilation in the PACU, the pressure difference between the atmosphere and the trachea (being negative to the environment) was sufficient to create leakage of air, causing serious respiratory complications. In fact, these complications may have occurred earlier in the operating theatre if an uncuffed ETT had been used, as air leakage around the ETT during positive pressure ventilation would have disrupted the laryngeal repair.
The most common reason for airway injury during the Sistrunk operation is mistaking airway structures for the hyoid bone.5,10–12 Moreover, in all these reported cases the iatrogenic injury was missed initially. As a preventive measure, an intraoperative air leak test might help in the assessment of the integrity of the airway after surgical repair. This is performed by irrigating the wound with normal saline, then deflating the ETT cuff and ventilating the patient to a pressure of 20–40 cm of water with occlusion of the nose and mouth. In the presence of leakage, there will be bubbling of air. Although this technique is well described during the repair of trachea–oesophageal fistula and tracheal surgeries,13,14 it has not been reported with the Sistrunk operation. If we had performed this test, perhaps the leakage could have been recognised earlier and management would have been different. However, an intraoperative negative air leak test may not be completely reliable in predicting whether postoperative air leakage will occur or not. Therefore, the decision to continue positive pressure ventilation after completion of surgery has to be individualised based on the size of the injury, site of the injury (supraglottic versus sub-glottic), the experience of the operator, along with the presence or absence of an air leak.
In conclusion, pneumomediastinum followed by bilateral pneumothoraces due to iatrogenic injury of the airway during excision of a thyroglossal duct cyst is a rare complication. Therefore, early detection is crucial for proper management. Moreover, it may be necessary to continue mechanical ventilation with an endotracheal tube in situ as a preventive measure postoperatively, even after the repair of the primary injury.
Footnotes
Acknowledgement
The author(s) would like to acknowledge Prof. KA Kelly McQueen for assistance with editing of the manuscript.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.