
Abstract
In recent years there has been a significant investment in education on the management of neuromuscular blockade and increased availability of sugammadex in anaesthetic practice. This survey aimed to examine contemporary practice of Australian and New Zealand anaesthetists in managing neuromuscular blockade and its reversal. A web-based, voluntary survey was distributed to a cohort of 1000 Fellows of the Australian and New Zealand College of Anaesthetists. We received 229 completed responses (survey response rate of 23%). Seventy-one percent (95% confidence interval (CI) 64% to 76%) of the survey respondents thought that 5% or fewer of the patients in their hospital display clinically significant postoperative paralysis. Only 35% (95% CI 18% to 29%) thought that quantitative neuromuscular twitch monitors should be used to monitor neuromuscular block, and the dose and time given for reversal agents was often inconsistent with published recommendations. Sugammadex was the preferred reversal agent for 78% (95% CI 72% to 83%) of survey respondents, but they indicated that cost remains a significant barrier to its widespread uptake. Despite the low response rate, this survey identified that some reported practices in Australia and New Zealand deviate from guidelines and current recommendations in the management of neuromuscular blockade. If the respondents are representative of the broader anaesthetic community, there appears be a greater preference for sugammadex over neostigmine for reversal of neuromuscular blockade.
Introduction
Residual paralysis, as defined by a train-of-four ratio (TOFR) less than 0.9 following the administration of neuromuscular blockers, has been shown to be associated with increased postoperative morbidity.1,2 The reported incidence of residual paralysis varies widely from 4% to 64% when neostigmine is used.3–8 In contrast, in one study the incidence was reduced to 4.3% with the unmonitored use of sugammadex, and 0% with the use of sugammadex and quantitative neuromuscular twitch (NMT) monitoring. 9 Recognition of residual paralysis as a clinically significant problem has led to Australian and New Zealand guidelines recommending the routine use of quantitative NMT monitoring prior to extubation when non-depolarising blocking agents have been administered. 10
Previous surveys in Australia, New Zealand and internationally have identified poor knowledge of guideline recommendations, low utilisation of quantitative NMT and underestimation of the incidence of residual paralysis.11,12 Increasing use and availability of sugammadex has led to a change in anaesthetic practice, with more rapid and reliable reversal of neuromuscular blockade. It is therefore timely to reassess anaesthetists’ attitudes towards neuromuscular monitoring and the use of reversal agents and NMT monitoring to identify if changes in practice have occurred since previous surveys. The aim of this survey was to assess these attitudes by surveying a representative sample of Australian and New Zealand anaesthetists.
Materials and methods
Following ethics approval (NSLHD LNR/17/HAWKE/410), we conducted a survey among anaesthetists registered with the Australian and New Zealand College of Anaesthetists (ANZCA). In August 2018, a randomly selected cohort of 1000 Fellows of ANZCA were sent an email containing a link to complete an online survey of 26 questions (Supplemental Digital Content 1). Informed consent was obtained from an introductory email, with implied consent on clicking through to the formal survey, rather than formal written consent (this method of consent was approved during the ethics review). Completion of the survey was entirely voluntary and no incentives or rewards were given for survey completion. One reminder email was sent one week after the initial email. The survey was open to responses for six weeks from the first email.
The questions in the survey were based on those previously published by Naguib et al., 11 with a number of new questions developed to reflect the more recent availability and use of sugammadex. Some questions originally asked were amalgamated or omitted to reduce the time and complexity of the survey. The questions were refined following a pilot survey sent to anaesthetists at the Royal North Shore Hospital in Sydney, Australia. Our aim was to examine Australian and New Zealand anaesthetists’ attitudes to neuromuscular blockade and its monitoring and reversal in current modern anaesthesia practice. Descriptive statistics were used, presenting the data as frequency tables.
Results
Of 1000 surveys sent, we received 229 completed responses (survey response rate of 23%).
Demographics
Table 1 outlines the demographic data of the respondents along with summary demographic data for all Fellows of ANZCA.
Demographic data of respondents.
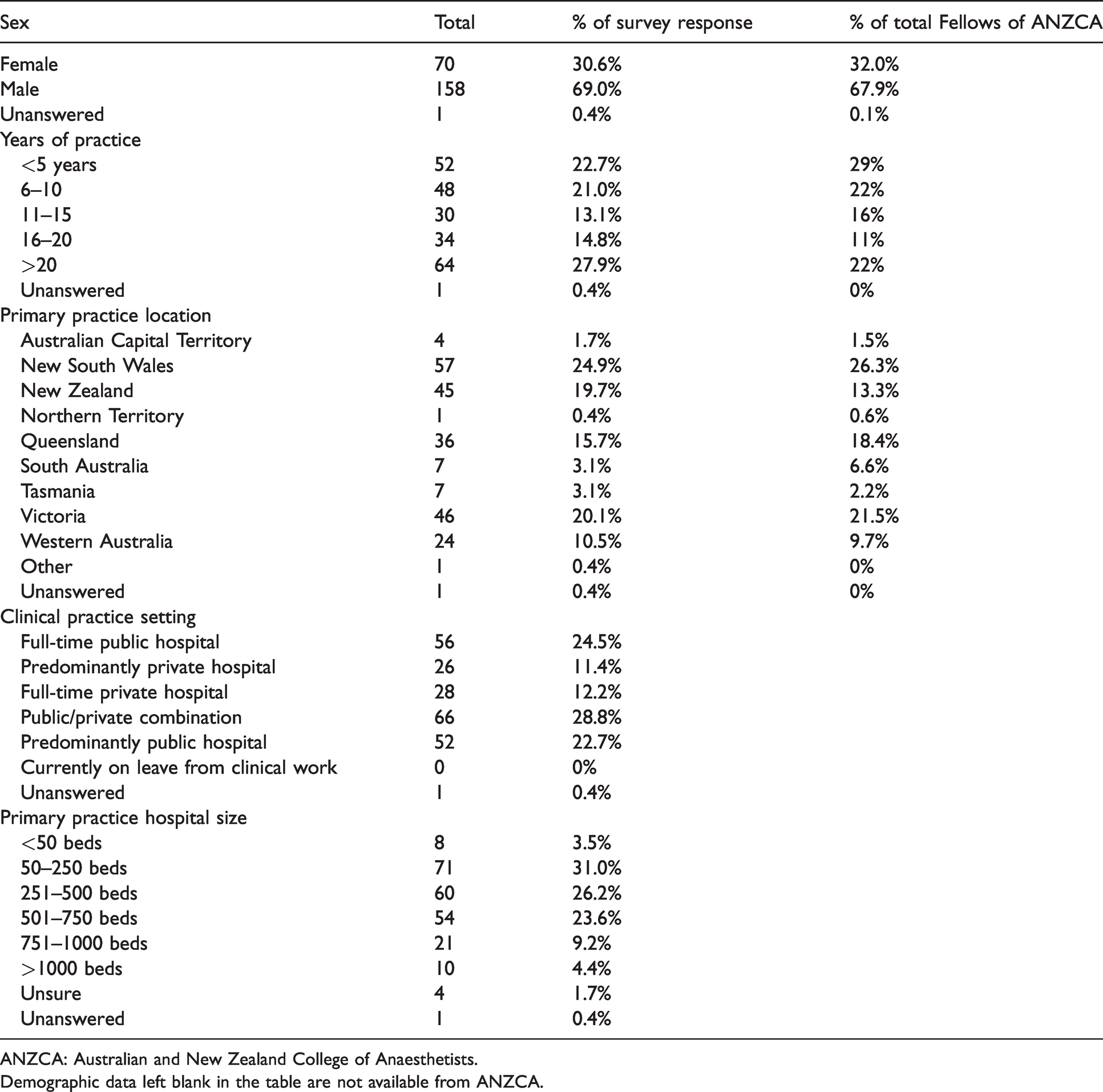
ANZCA: Australian and New Zealand College of Anaesthetists.
Demographic data left blank in the table are not available from ANZCA.
In terms of experience, practice location and size of hospital, there was a broad range of anaesthetists responding to the survey. Forty-five of 229 respondents (20%) were practising in New Zealand, while 182/229 (80%) were practising in Australia. Most demographic data from the survey respondents were comparable to demographic data available for all Fellows of ANZCA.
Significance of postoperative residual neuromuscular paralysis
Twenty-six percent (95% confidence interval (CI) 20% to 32%) of respondents (59/229) reported that they thought that clinically significant residual paralysis occurs in fewer than 1% of patients in their primary hospital post-anaesthesia care unit (PACU). Seventy-one percent (95% CI 64% to 76%) of respondents (162/229) felt that fewer than 5% of patients in their hospital displayed clinically significant postoperative paralysis, while 45% (95% CI 38% to 52%) of respondents felt that residual paralysis was not a significant public health problem.
Table 2 summarises opinions on the use of neuromuscular monitors. Eleven percent of respondents thought the use of conventional nerve stimulators to monitor the depth of neuromuscular blockade was unnecessary and 11% reported that they felt quantitative train-of-four monitors were unnecessary.
Opinions regarding the use of neuromuscular transmission monitors among respondents (N=229).
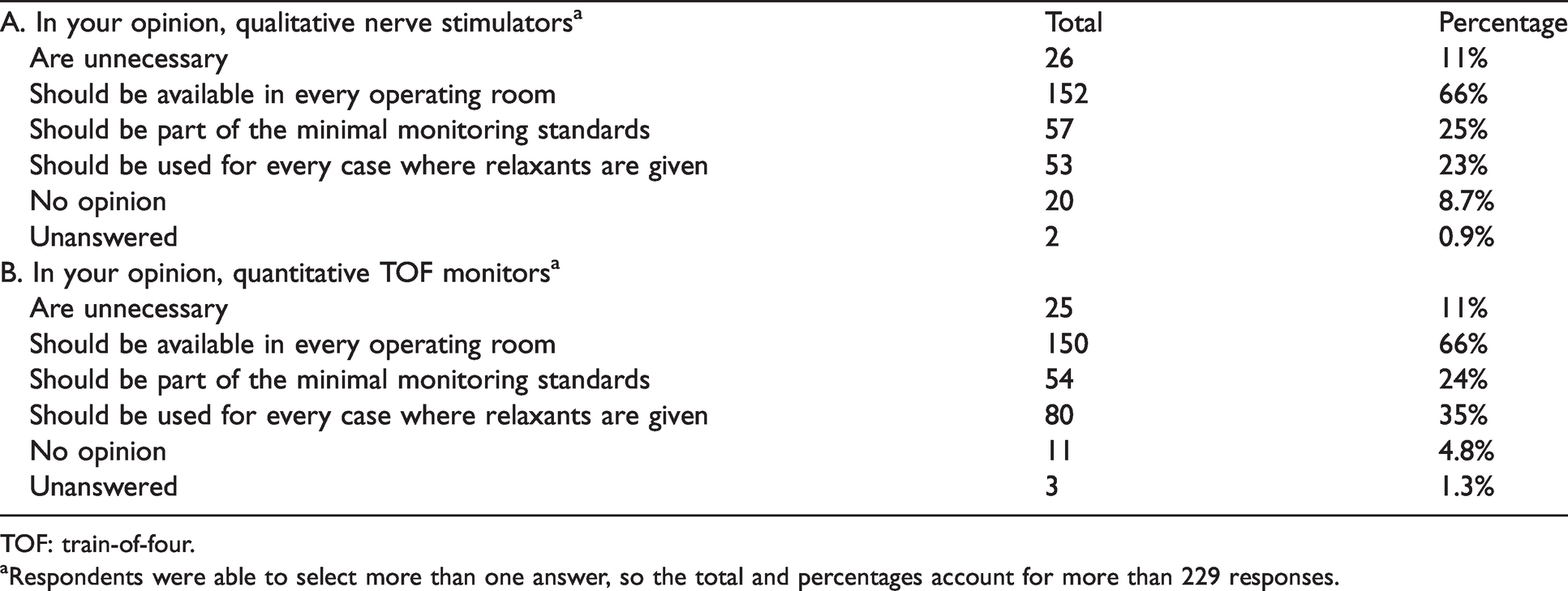
TOF: train-of-four.
aRespondents were able to select more than one answer, so the total and percentages account for more than 229 responses.
Neuromuscular monitor availability
Forty-five percent (95% CI 39% to 52%) of respondents had a quantitative NMT monitor available in every operating room at their primary practice location. Thirty-seven percent (95% CI 31% to 43%) had quantitative monitors available, but not in every operating room. Eighty-two percent (95% CI 76% to 87%) of respondents had access to quantitative monitors at their primary place of practice. Table 3 shows the remainder of responses regarding the availability of neuromuscular junction monitors.
Availability of neuromuscular transmission monitor in respondents’ primary practice locations.
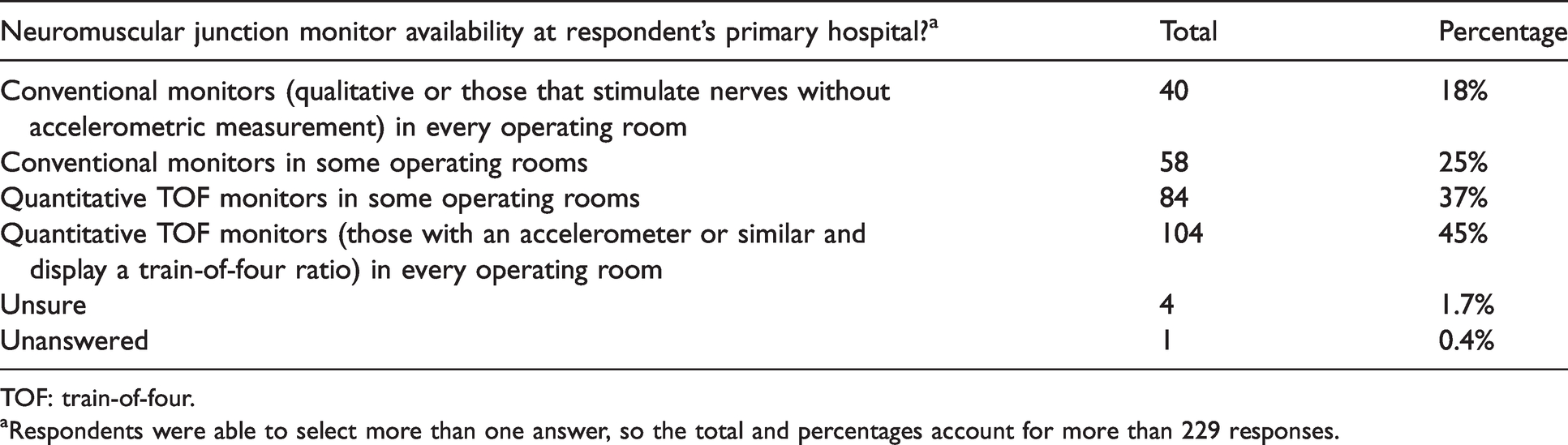
TOF: train-of-four.
aRespondents were able to select more than one answer, so the total and percentages account for more than 229 responses.
Pattern of use of neuromuscular blockers
There was a clear preference among respondents to use rocuronium for both intubation and maintenance of paralysis, with 40% (95% CI 34% to 47%) of respondents using rocuronium for 76% or more of all anaesthetics requiring intubation. Vecuronium was the second most popular neuromuscular blocker for tracheal intubation and surgical relaxation, while atracurium was the third most common for both uses. Figure 1 summarises the use of neuromuscular blockers among respondents in Australia and New Zealand.
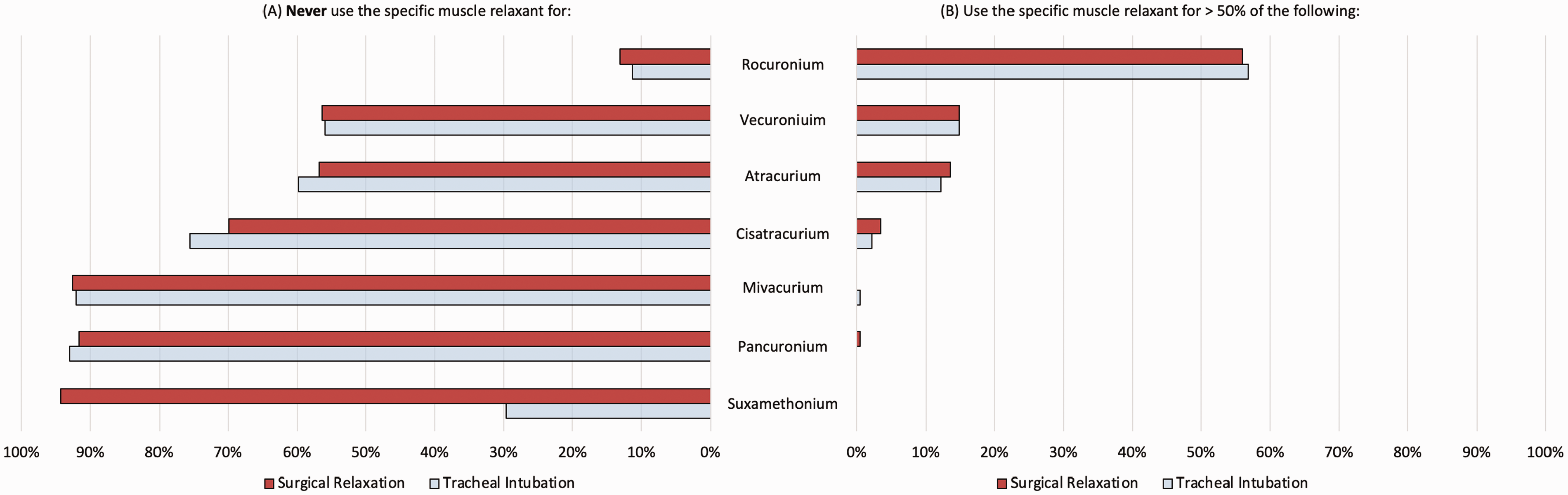
Patterns of neuromuscular blocker use among respondents.
Reversal considerations
While only 25% (95% CI 20% to 32%) of respondents always gave a reversal agent, 49% (95% CI 43% to 56%) administered reversal in 76% or more cases when a muscle relaxant was used. Thirteen percent (95% CI 9% to 18%) of respondents used a reversal agent in less than half of their cases when a neuromuscular blocker was administered. Sixty percent (95% CI 53% to 66%) and 38% (95% CI 32% to 45%) of respondents considered the timing of the last dose of relaxant and the total dose of relaxant important in assessing the need for reversal. Only 45% (95% CI 38% to 51%) considered the measurement of TOFR an important consideration in the need to administer a reversal agent. Forty-four percent (95% CI 37% to 50%) of respondents felt that clinical signs were adequate to show neuromuscular reversal, while 83% (95% CI 77% to 87%) reported that they felt that a TOFR greater than 0.9 indicated adequate reversal.
While almost two-thirds of respondents felt that neuromuscular TOFR monitors should be available in every operating theatre, only 35% (95% CI 29% to 42%) felt they should be used in every case when a non-depolarising relaxant was used. Furthermore, approximately 25% (95% CI 20% to 31%) felt that TOFR monitors should be part of minimal monitoring standards.
Seventy-eight percent (95% CI 72% to 83%) of respondents administered neostigmine less than ten minutes prior to extubation, compared with 88% (95% CI 83% to 92%) for sugammadex. Seven percent (95% CI 4.5% to 11.8%) stated that they would allow less than two minutes between neostigmine administration and extubation. For sugammadex, 83% (95% CI 77% to 87%) of respondents reported that they would allow less than five minutes prior to extubation. These considerations are summarised in Table 4.
Reversal considerations among respondents.
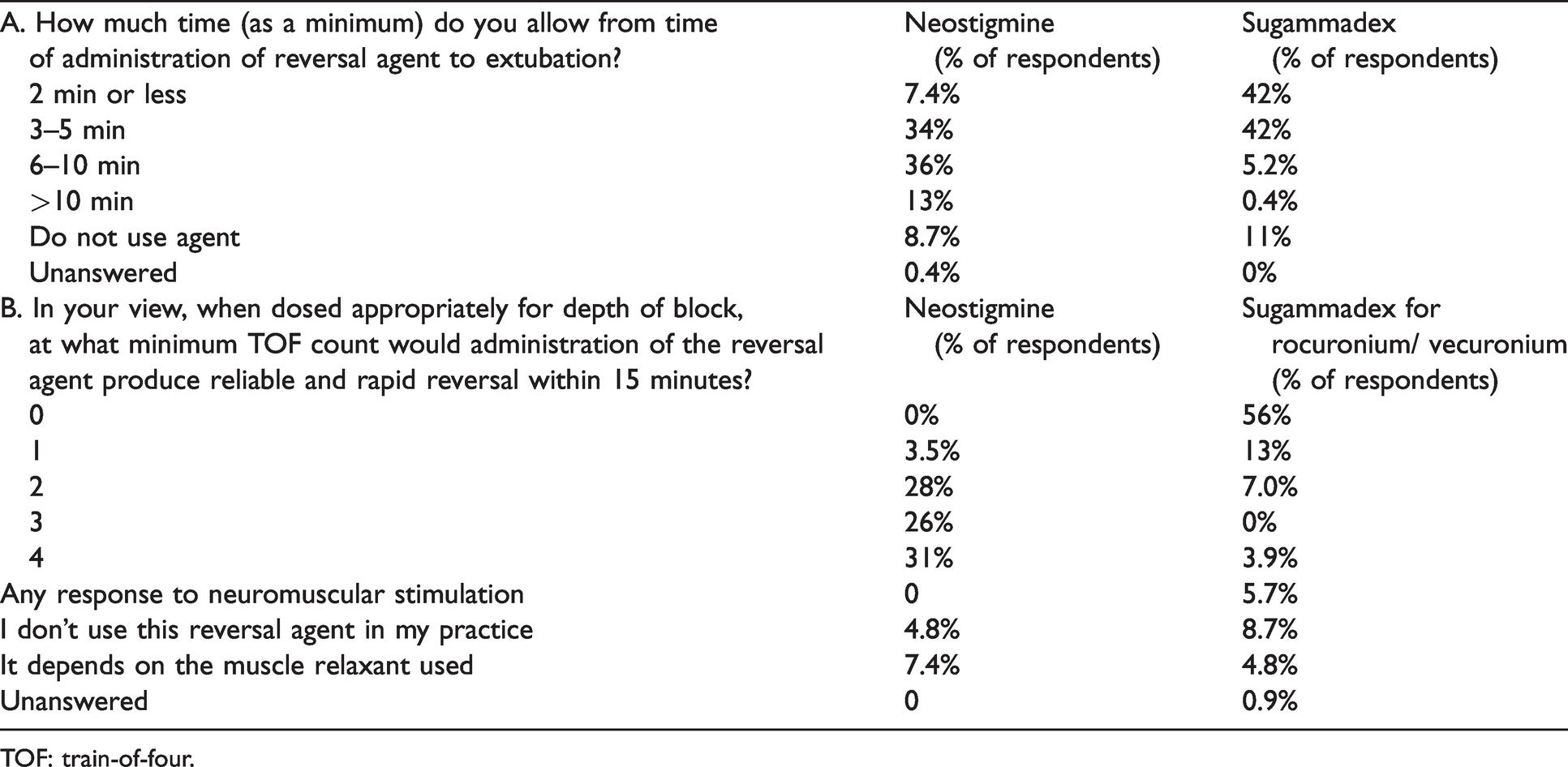
TOF: train-of-four.
Over half of the respondents administered a standard dose (2.5 mg neostigmine or 200 mg sugammadex, which is equivalent to one ampoule in Australia and New Zealand) rather than a weight-based dose of neostigmine (69% of respondents (95% CI 62% to 75%)) or sugammadex (61% of respondents (95% CI 54% to 67%)).
The majority of respondents had concerns with neostigmine regarding haemodynamic effects, inadequacy of reversal, and postoperative nausea and vomiting; while for sugammadex, concerns shared by the majority were limited to cost alone, with the allergic potential of sugammadex being a concern for almost 50% of respondents. These concerns are summarised in Figure 2.
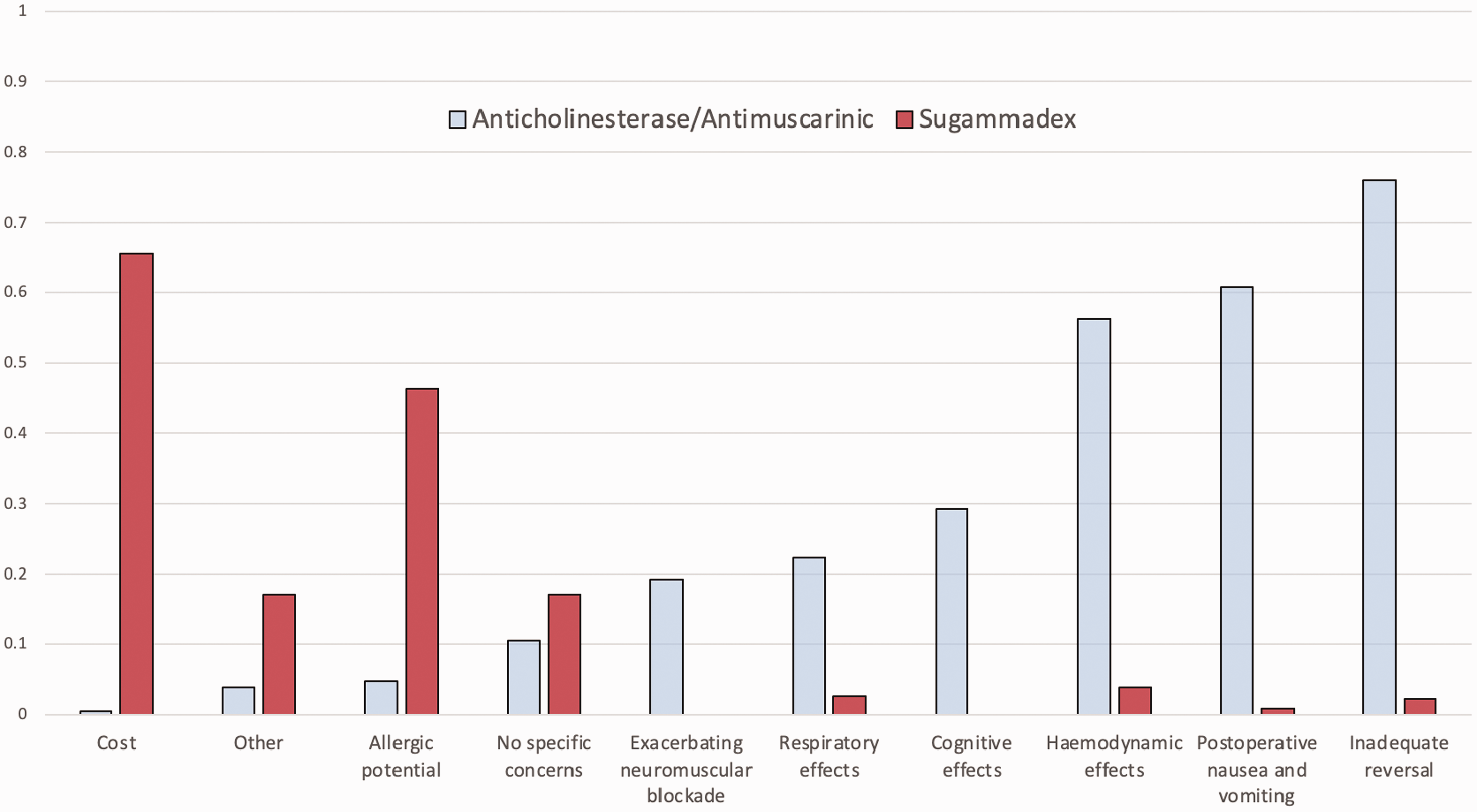
Concerns associated with the administration of anticholinesterase/antimuscarinic medication and sugammadex among respondents.
Availability of sugammadex
Among respondents, sugammadex use was unrestricted in 45% (95% CI 39% to 52%) of anaesthesia locations, while in 41% (95% CI 35% to 48%) of locations it was partially restricted by being stored in a locked cupboard or outside of the operating theatre. In addition, 14% (95% CI 10% to 19%) of respondents’ hospitals had ‘restricted availability’ whereby the use of sugammadex triggered a report. Approximately one-third (95% CI 29% to 42%) of respondents preferred to use neostigmine as a reversal agent, with a similar percentage (95% CI 30% to 43%) preferring sugammadex. The remaining one-third based their preferred agent for reversal on other factors. If cost was not an issue, 78% (95% CI 73% to 84%) of respondents reported that they would prefer to use sugammadex.
Discussion
Many respondents to this survey felt that residual paralysis was uncommon in their place of practice, and almost half stated that residual paralysis was not an important clinical problem. This was similar to the responses to these two issues in previous surveys published almost a decade ago.11,12 Since then, guidelines and educational efforts have highlighted the importance of residual paralysis. The increased availability of sugammadex in the past decade has likely reduced the incidence of residual paralysis. Internationally, studies in which sugammadex was unrestricted have shown low rates of residual paralysis (4.3%) when quantitative NMT monitoring was not used and as low as 0% with the use of a NMT monitor.9,13 However, this does not likely reflect contemporary practice in Australia and New Zealand as not all hospitals have unrestricted use of sugammadex. In addition, an Australian audit of hospitals with unrestricted use of sugammadex has shown that the incidence of residual paralysis is much higher than 0%–4%. 14 This suggests that the importance of residual paralysis remains underappreciated.
Respondents to our survey reported limited access to quantitative NMT monitoring, with only 45% stating they had quantitative train-of-four monitors available in every operating room in their primary place of practice. This is despite the majority of respondents primarily working in larger hospitals which are presumed to be better resourced, and ANZCA monitoring guidelines advising that quantitative NMT monitoring should be utilised for any patient in whom neuromuscular blockade is induced and extubation is anticipated. 10
There did not appear to be a clear difference in attitudes towards monitoring or reversal of neuromuscular blockade between respondents from Australia versus New Zealand in this survey. There were some concerning responses regarding the knowledge and practice of reversal of neuromuscular blockade from respondents in both countries. Clinical signs were reported as safe methods to determine if a patient can be extubated by 44% of respondents; 7.4% of respondents felt that less than two minutes was an adequate minimum time to allow for neostigmine-based reversal. Similarly, dosing of neostigmine and sugammadex was most commonly one ampoule of either drug, rather than tailored dosing depending on neuromuscular twitch monitoring. While it is beyond the scope of this survey to describe best practice in neuromuscular block reversal, it appears that many of the practices reported by respondents do not comply with current ANZCA recommendations. 10
This study also illustrates some issues with sugammadex since its introduction in Australia and New Zealand. Although respondents felt that sugammadex has fewer adverse effects and faster onset, its use in many locations remains restricted, with cost being the greatest concern, followed by allergic potential.
The main limitation of this study is the low response rate to the survey (22.9%), so the responses reflect only the practices of respondents and may not be transferable to all Australian and New Zealand anaesthetists. Despite this, the demographic range of the respondents was consistent with the demographic range of all Fellows of ANZCA and, as such, the findings suggest there may be deviation from evidence and ANZCA guidelines in relation to neuromuscular block reversal among all Australian and New Zealand anaesthetists.
This study highlights potential areas for improvement with regard to the reversal of neuromuscular blockade in Australia and New Zealand. There is still a significant proportion of anaesthetists who do not consider residual paralysis to be an important issue. Furthermore, qualitative methods to determine adequate reversal are still being used despite multiple studies demonstrating their inadequacy. In addition, this survey highlights that a common limitation to the greater use of sugammadex in Australia and New Zealand is perceived cost.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X21995498 - Supplemental material for A survey of current management of neuromuscular block and reversal in Australia and New Zealand
Supplemental material, sj-pdf-1-aic-10.1177_0310057X21995498 for A survey of current management of neuromuscular block and reversal in Australia and New Zealand by Benjamin L Olesnicky Andrew Lindberg Kerrie Ren
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X21995498 - Supplemental material for A survey of current management of neuromuscular block and reversal in Australia and New Zealand
Supplemental material, sj-pdf-2-aic-10.1177_0310057X21995498 for A survey of current management of neuromuscular block and reversal in Australia and New Zealand by Benjamin L Olesnicky Andrew Lindberg Kerrie Ren in Anaesthesia and Intensive Care
Footnotes
Acknowledgements
The authors would like to thank the ANZCA Clinical Trials Group for assistance in the review and distribution of the survey to ANZCA members.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.