
Abstract
A low tidal volume ventilation (LTVV) strategy improves outcomes in patients with acute respiratory distress syndrome (ARDS). Subsequently, a LTVV strategy has become the standard of care for patients receiving mechanical ventilation. This strategy is poorly adhered to within intensive care units (ICUs). A retrospective analysis was conducted of prescribed tidal volumes in mechanically ventilated patients with hypoxic respiratory failure between April 2013 and March 2017. Data collection included the establishment of a new data-entry box for patient height in March 2016, aimed at assisting the calculation of LTVV. We reviewed 836 ICU admissions, comprising 19,884 hours of ventilation. A total of 92% of admissions lacked patient height recording. When height was recorded, 54% of hours of ventilation were LTVV adherent. Non-LTVV hours for both groups involved higher tidal volumes (38%) rather than lower tidal volumes (8%). Non–LTVV-adherent hours were significantly (P<0.001) more likely to be associated with patient mortality than LTVV-adherent hours were. For all hours of ventilation, mean tidal volume before March 2016 was significantly higher (496 (standard deviation (SD) 101) ml, compared to after March 2016 (451 (SD 107) ml, P<0.001, 95% confidence interval for true difference in means 42 to 48 ml). However, this trend gradually reversed over time. There was a clinician preference for multiples of 50 ml. There was poor adherence to LTVV strategy in patients with hypoxic respiratory failure, which was associated with an increase in patient mortality. An electronic medical record intervention was successful in producing change, but this was not sustainable over time. Clinician ventilation prescribing habits were based on numerical simplicity rather than evidence-based practice.
Keywords
Introduction
Mechanical ventilation to support effective gas exchange is commonly required to manage patients admitted to the intensive care unit (ICU) with respiratory failure. Modern mechanical ventilation strategies have been strongly influenced by the literature around ventilation in patients with acute respiratory distress syndrome (ARDS). 1 ARDS is a pathological state defined as an acute, diffuse, inflammatory lung injury, leading to increased pulmonary vascular permeability, loss of aerated lung tissue, increased venous admixture, increased physiological dead space and decreased lung compliance. 2 The consequences of ARDS—worsening gas exchange and progressive hypoxaemia—have a high burden of morbidity and mortality. 3
A historical shift in mechanical ventilation practices has developed from the accumulation of new evidence regarding ventilation strategies. Older ventilation strategies had been motivated by a perceived need to achieve physiological levels of arterial blood pH and oxygen, and particularly CO2. 1 This typically resulted in ventilation with tidal volumes of 10–15 ml/kg of body weight. However, beginning with a consensus conference of the American College of Chest Physicians in 1993, 4 an alternative view emerged in favour of ventilation with lower tidal volumes. This low tidal volume ventilation (LTVV) strategy was hypothesised to reduce morbidity and mortality by minimising mechanical damage to lung tissue due to overinflation (barotrauma),5–7 which may generate or exacerbate inflammation and contribute to increased respiratory distress as well as multiple organ dysfunction.8–10 Definitive evidence in support of LTVV was provided by the ARDSNet trial, a multicentre randomised controlled trial that found ventilation with an initial tidal volume of 6 ml/kg and the use of height-predicted body weight (PBW) rather than measured body weight reduced mortality among patients with acute lung injury from 39.8% to 31%. 1 The use of height-PBW may prevent over-ventilation in overweight and obese patients, as lung volume varies independently of excess body weight. 11
The ARDSNet study had a clear impact on ventilation practices across the world. A study of intensive care units in 40 countries found that mean administered tidal volumes declined from 8.8 ml/kg of measured body weight to 6.9 ml/kg between 1998 and 2010, with a concomitant decrease in mortality, 12 although it is unclear if these changes were due only to increased LTVV adherence or to other factors. Two more recent studies of single ICUs in the USA have reported LTVV adherence (defined as tidal volume ≤6.5 ml/kg PBW) rates of 27% 13 and, in a paediatric unit, 32%–33%. 14 Despite a recommendation by the College of Intensive Care Medicine of Australia and New Zealand that LTVV adherence be monitored as an ICU quality of care measure, 15 there is little publicly available information on LTVV adherence in Australia. A 2015 retrospective study on mechanical ventilation of patients with acute lung injury in the ICU of St Vincent’s Hospital, Melbourne, found that only 13.4% of ventilation measurements were ≤6.5 ml/kg PBW, 16 while a one-week observational study of seven Victorian ICUs focused on non-ARDS patients found that only 62% of initial ventilation volumes were ≤8.0 ml/kg PBW. 17 While varying measurement methods and definitions of LTVV adherence complicate any comparison between centres and across time, the available evidence suggests that the majority of ARDS patients in Australian ICUs may not be receiving LTVV-adherent mechanical ventilation.
Several centres have reported successful efforts to improve LTVV adherence with various interventions, including adjusting default ventilator settings, generating automatic alerts for large tidal volumes and clinician education,18,19 although education is not always successful. 12 In March 2016, an ICU in a Sydney metropolitan tertiary hospital introduced an intervention aimed at improving LTVV adherence by encouraging the measurement and recording of ventilated patients’ heights. This intervention involved adding a prominent text field for patient height to the electronic medical record (EMR) software used in the ICU. The text field also provided an optional tool for estimating patient height from their demi-span—half the distance between outstretched fingertips—to reduce the difficulty of estimating and recording the height of an unconscious and bed-bound patient.
This study aimed to measure and report adherence to the LTVV strategy in the management of mechanically ventilated patients in a single-centre, metropolitan Sydney ICU. Secondary aims included evaluating the effect of an intervention intended to improve LTVV adherence, the first prospective study in Australia to do so, and to quantify the relationship between LTVV adherence and patient mortality.
Methods
Study population and data collection
A retrospective cohort of patients was selected according to the following criteria: admitted to the ICU between 1 April 2013 and 31 March 2017 inclusive; intubated and mechanically ventilated; and Acute Physiology and Chronic Health Evaluation (APACHE) II score for oxygenation ≥2. 20 Other than APACHE II score, there were no diagnostic criteria for inclusion. While not strictly meeting the diagnostic criteria for ARDS, this clinical situation still requires a LTVV strategy. For this cohort, the following data were retrieved: date of birth, date of admission, sex, height (if recorded during the admission), mortality in the ICU and hourly mechanical ventilation observations, including mode of ventilation, number of spontaneous breaths and tidal volume. Tidal volume was the measured expired tidal volume. Data for the study were collected from the clinical information system. For patients who were admitted more than once during the study period, each admission was considered separately, as it was associated with a separate set of patient data. For a subset of records that lacked discharge information, medical and nursing notes were reviewed to determine mortality.
For admissions on or after 21 March 2016 (the date of the intervention) without patient height recorded in the EMR, an additional search was performed for information on patient height. For each of these patients, the most recent volume of paper medical records was requested from the hospital records department. The records were then manually reviewed for instances where patient height was recorded. In cases where multiple conflicting heights were recorded, the most recently dated height was used. Heights were excluded if the patient was younger than 18 years of age at the time of recording.
This study was approved by the Nepean Blue Mountains Local Health District Human Research Ethics Committee (LNR/17/NEPEAN/80), and consent was waived. A flow chart showing the total number of patients needing mechanical ventilation during the four-year period and number of patients excluded is shown in Figure 1.
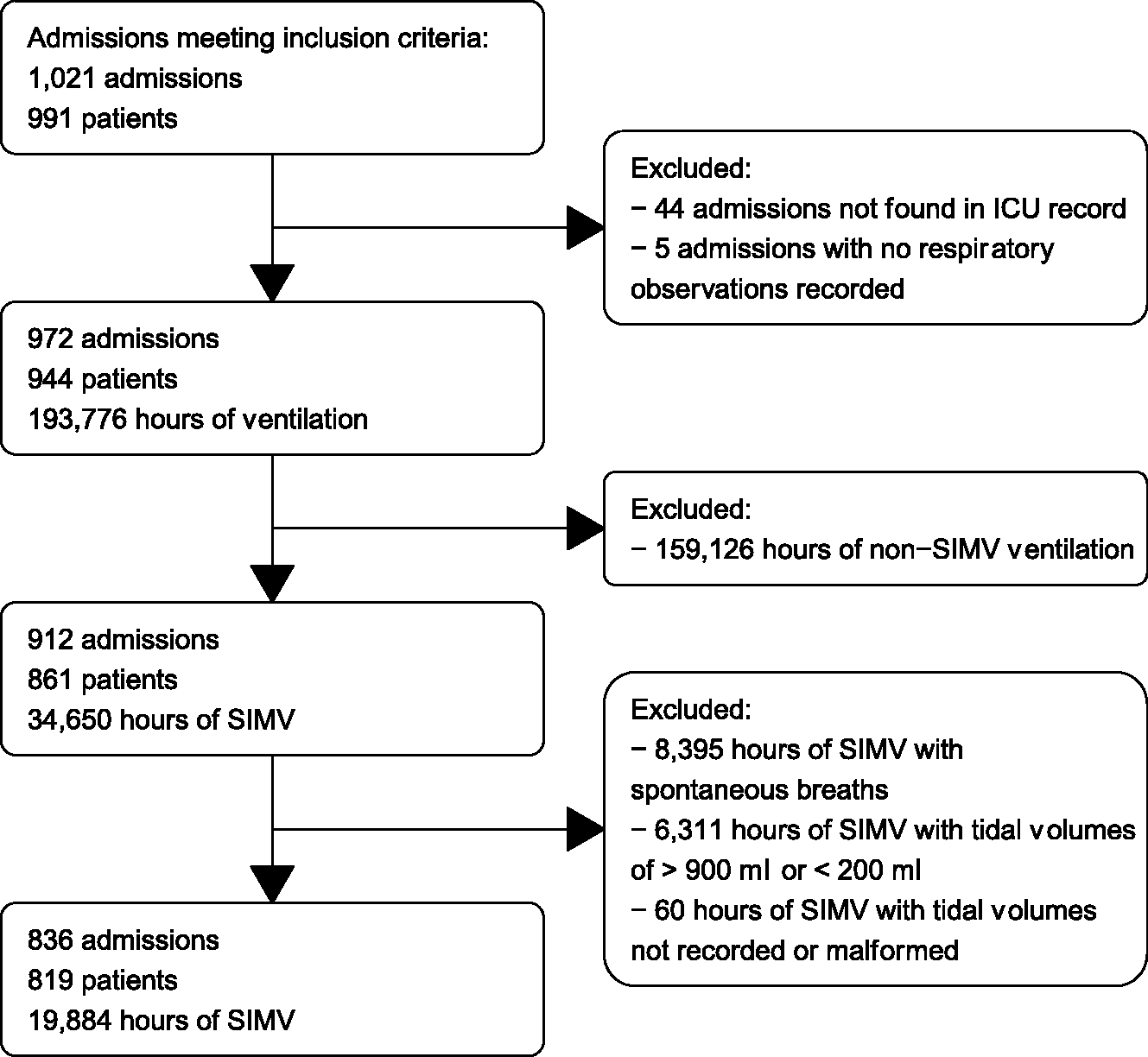
Flow diagram of patients, admissions and hours of ventilation considered for inclusion in this study. ICU: intensive care unit; SIMV: synchronised intermittent mechanical ventilation.
Data analysis
All analyses were performed using R with the tidyverse package (R Foundation for Statistical Computing, Vienna, Austria). 21 Hourly respiratory observations were filtered to select only hours where the ventilation mode was recorded as synchronised intermittent mechanical ventilation (SIMV)—the default volume-controlled mandatory ventilation mode used in the unit. The study excluded ventilation with other modes, including pressure-controlled modes. Because ventilation mode was a manually recorded observation, any case-insensitive variation of SIMV (e.g. ‘simv’, ‘Simv’) was accepted as equivalent. Observations were further filtered to select only hours where no spontaneous patient breaths were recorded, so that only clinician-set volumes were included in the analysis. Volumes >990 ml (the maximum programmable tidal volume for the ventilation machines used in the ICU under study) or <200 ml were removed as probable recording errors. Admissions that did not have any respiratory observations following these quality control steps were removed from further analysis. Demographic data for the patients included in the final analysis are given in Table 1.
Demographics of patients included in the study.
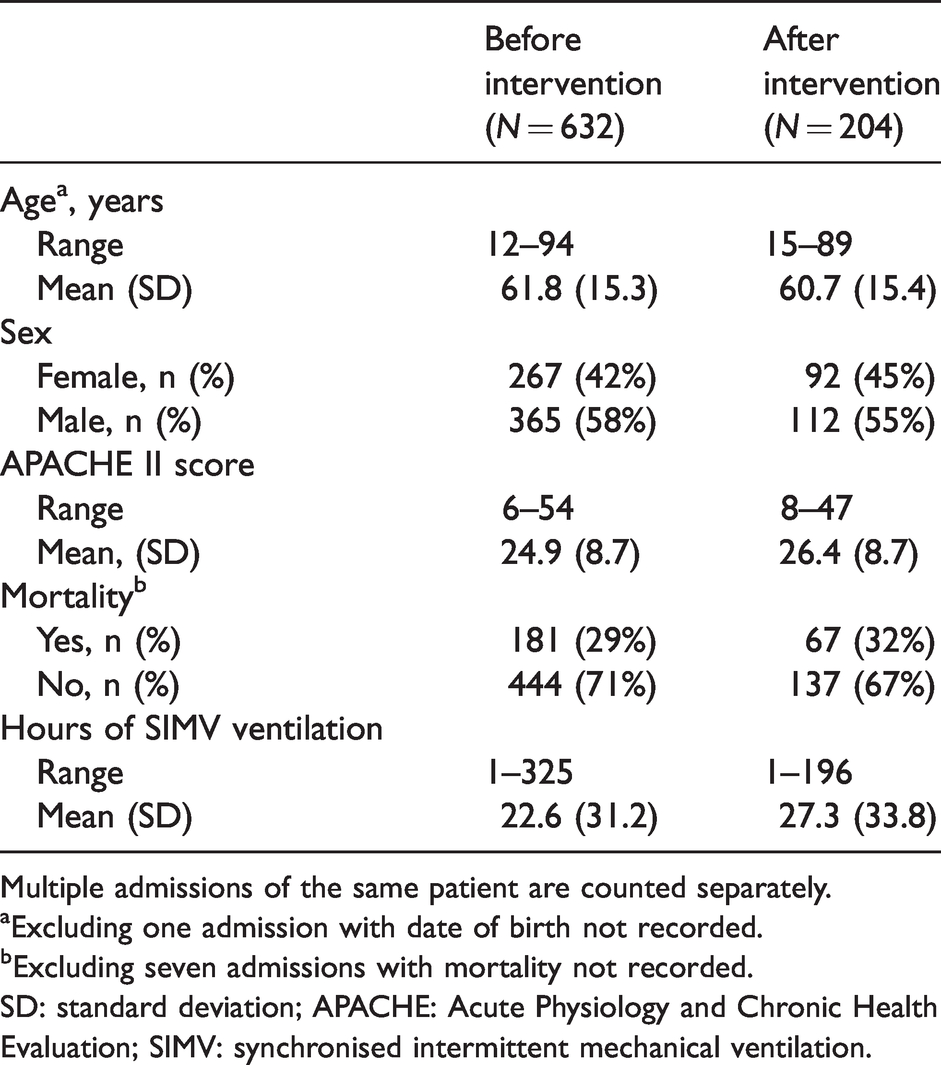
Multiple admissions of the same patient are counted separately.
aExcluding one admission with date of birth not recorded.
bExcluding seven admissions with mortality not recorded.
SD: standard deviation; APACHE: Acute Physiology and Chronic Health Evaluation; SIMV: synchronised intermittent mechanical ventilation.
PBW for patients with a recorded height was calculated according to the following formulae 1 : for female patients, PBW = 45.5+(0.91×(centimeters of height–152.4)); for male patients, PBW = 50+(0.91×(centimeters of height–152.4)). LTVV adherence was defined as a tidal volume between 5 and 7 ml/kg PBW.
Statistical tests
To determine whether the 21 March 2016 intervention resulted in a significant reduction in absolute tidal volumes administered to patients, a two-tailed t-test was performed comparing all hourly tidal volumes administered to patients admitted before 21 March 2016 to all hourly tidal volumes administered to patients admitted on or after 21 March 2016. To determine whether LTVV adherence significantly correlated with patient mortality within the cohort of patients who had their height measured and recorded in the EMR, a chi-square test was performed comparing mortality between LTVV-adherent and non-adherent hours of mechanical ventilation. An hour of ventilation was considered associated with mortality if it occurred during an admission associated with mortality.
Results
Following quality control of patient and respiratory observation data (185 admissions removed), 19,884 hourly SIMV ventilation observations drawn from 836 admissions of 819 patients were included in the analysis. Sixty-six (7.9%) admissions had their height recorded in the EMR, with all but one of these having an admission date on or after 21 March 2016. Heights for an additional 54 (6%) patients were found after reviewing the paper medical records for all patients admitted after 21 March 2016 whose heights were not recorded in the EMR.
Considering only admissions with a height recorded in the EMR, 54% of hourly tidal volumes were within the LTVV-adherent range of 5–7 ml/kg PBW (mean (standard deviation, SD) 6.8 (1.6) ml/kg PBW), with the majority of values outside this range representing over-ventilation (38% of all hours) rather than under-ventilation (8.1%). This is shown in Figure 2(a). Among the 54 patients whose heights were not recorded in the EMR but which were found through an additional review of hospital records, 26% of hourly tidal volumes were within the LTVV range (mean (SD) 8.1 (2.4) ml/kg PBW). This is shown in Figure 2(b).
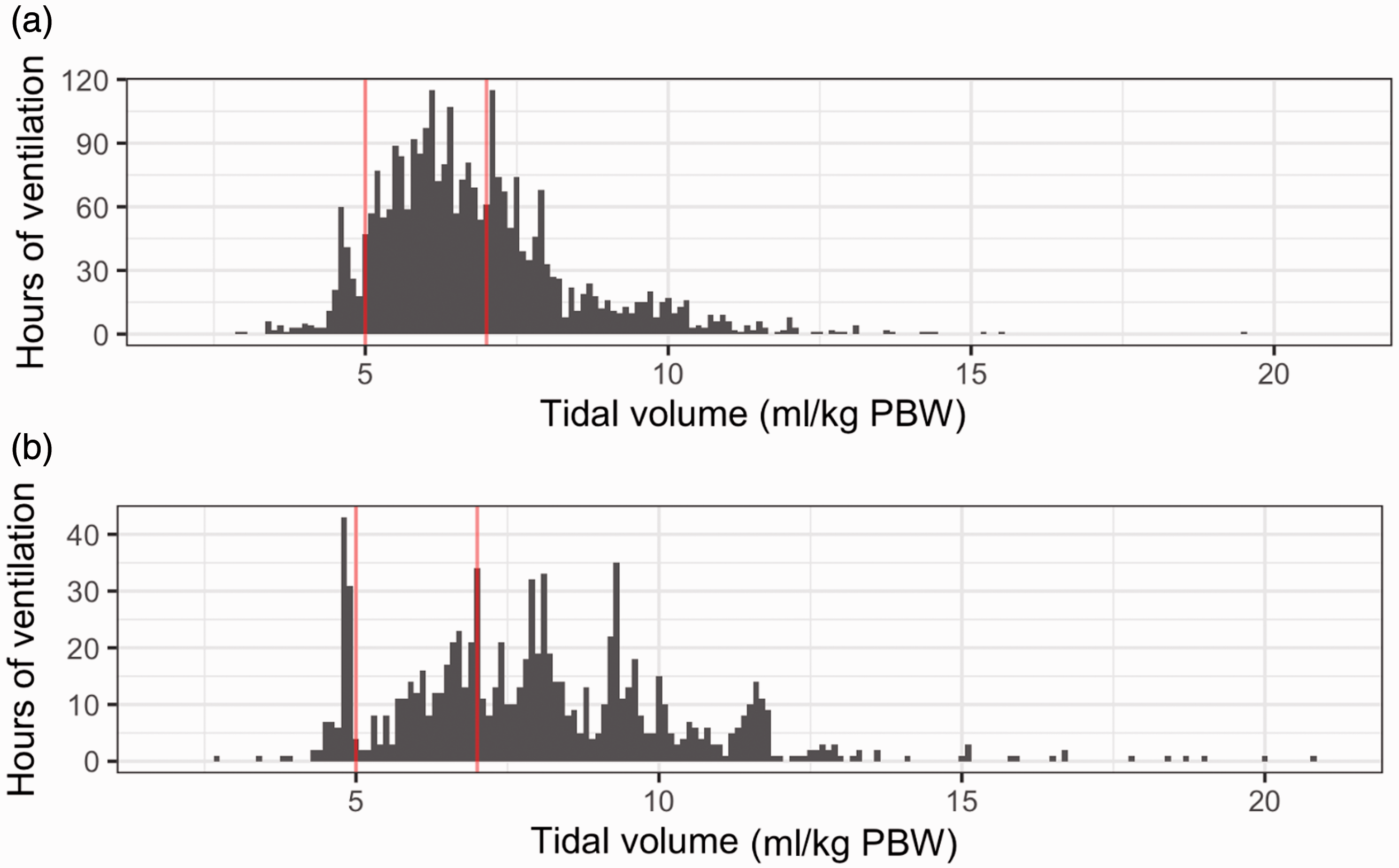
Hours of ventilation by tidal volume administered to (a) patients with heights recorded in electronic medical records (EMR; 2831 total hours) and (b) patients with heights not recorded in EMR but found in a search of paper records (932 total hours). Red vertical lines indicate the criteria used for low tidal volume ventilation adherence in this study (5 to 7 ml/kg PBW (predicted body weight)). PBW: predicted body weight.
There was a significant (χ2 P<0.001) interaction between LTVV adherence and mortality among patients with heights recorded in the EMR, with 33% of LTVV-adherent hours of ventilation associated with patient mortality compared to 47% of non-adherent hours.
Considering all patients and admissions, the absolute tidal volume administered to patients admitted before the 21 March 2016 intervention was on average higher (mean (SD) 496 (101) ml) than that administered to patients admitted on or after this date (mean (SD) 451 (107) ml), which constituted a significant difference (P < 0.001). This is shown in Figure 3.
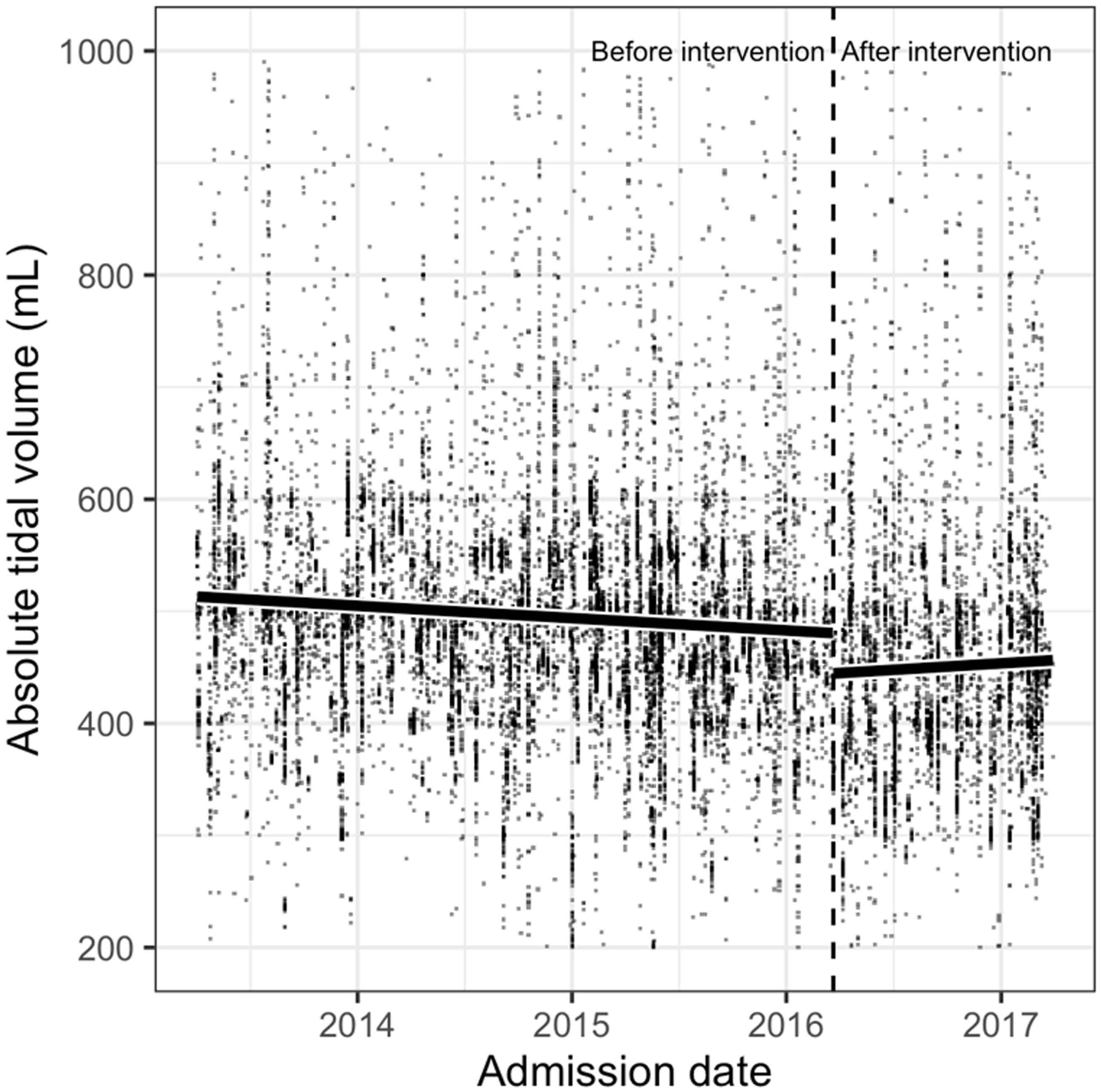
Absolute tidal volumes administered to all patients before and after the 21 March 2016 intervention, indicated by the vertical dashed line. Black solid lines represent linear models fit to observations in each time period. Before the intervention slope = –0.030 ml/day; after the intervention slope = 0.032 ml/day.
Of the 19,884 hourly respiratory observations included in the analysis, 2842 (14%) recorded an absolute tidal volume that was an integer multiple of 10 ml, while 1141 (5.7%) were multiples of 50 ml. The most selected volumes were 500 ml (n = 282), followed by 450 ml (n = 276) and 501 ml (n = 241).
Discussion
This study found that the LTVV strategy was poorly adhered to when treating mechanically ventilated patients admitted with hypoxic respiratory failure. A total of 92% of admissions did not have a patient height recorded in the EMR, and as patient height is necessary to calculate the PBW-adjusted ideal LTVV volume, LTVV adherence could not be determined for most admissions. However, the low adherence rate (26%) among admissions where patient height was able to be determined from other sources is likely close to the true rate for the majority of admissions and is in keeping with previous reports.13,14,16
The definition of LTVV adherence used in this study (tidal volume ≥5 ml and ≤7 ml/kg PBW) is different from that used in some previous reports (e.g. ≤6.5 ml/kg)13,16 and from the definition used in the ARDSNet study (initial volume of 6 ml/kg PBW within the first four hours of ventilation followed by stepwise reductions at 1 ml increments). 1 This definition was selected for two reasons: (a) to allow for rounding and measurement error in clinician calculation of PBW and LTVV volumes, and (b) to allow for the fact that episodes of mechanical ventilation were often discontinuous within admissions and involved transitions between different modes of ventilation, making it difficult to distinguish reliably between a low initial tidal volume and downwards titration. Given that this definition captured the peak of volumes administered when height was measured and recorded (Figure 2(a)) and thus when it is most likely that the LTVV strategy was intentionally followed, and that the large majority of non-adherent volumes represented over- rather than under-ventilation (Figure 2), it is likely that the LTVV definition used in this study was representative of true LTVV adherence, and does not exclude a significant number of episodes in which the volume was later titrated downwards.
Many previous reports have linked over-ventilation of ARDS patients with increased morbidity and mortality.1,22,23 While this study was not designed to investigate a causal relationship between non-LTVV ventilation and mortality, and the data were likely affected by confounding factors, including time on ventilation and severity of disease, the positive and statistically significant interaction between non-adherent ventilation and mortality suggests that improvements in LTVV adherence have the potential to improve patient outcomes in the ICU.
The 21 March 2016 intervention, in which a modification was made to the display of patient height in the EMR, was intended to increase LTVV adherence by increasing clinician awareness of patient height and reducing the number of steps required to measure and record it. There was a significant reduction in mean absolute tidal volumes administered after this intervention, suggesting the intervention occurred during a period in which mechanical ventilation practice shifted to favour lower tidal volumes, consistent with the linear trend prior to March 2016. However, the linear trends in administered tidal volumes before and after the intervention (Figure 3) do not support the intervention as the cause of this difference, as a general trend of decreasing volumes prior to the intervention was replaced with an increasing trend after it. While these data do not support drawing a causal conclusion for this shift, the trend after March 2016 suggests that the reduction in administered volumes was likely not sustained over the long term.
Qualitative research into clinician awareness of LTVV and the decision-making process when selecting mechanical ventilation volumes is needed to understand this observation fully. Some hypotheses for clinician decision-making strategies are suggested by the distribution of absolute tidal volumes (Supplemental Figure S1), in which multiples of 10 ml were favoured and 50 ml strongly favoured above the rates that would be predicted by chance. Eyington et al. 17 reported a similar preference in ventilation of non-ARDS patients in seven Victorian ICUs, finding 500 ml was set as the initial tidal volume in 33% of cases and was the most commonly set volume, as it was in this study. This pattern suggests that clinicians may be calculating LTVV-adherent volumes which are then rounded to the nearest 10 or 50 ml, estimating round-number volumes based on patients’ measured weight or build, selecting from a set of preferred round-number values or some mixture of these strategies. The further preference for volumes close to these round-number values, for example 501 ml, may reflect situations where round-number values were set but the delivered volume was perturbed by transient effects such as movement of equipment or changes in atmospheric pressure.
Further to this, one potential limitation of the data collected is the use of a tidal volume generated by the expiratory limb of the ventilation circuit. Regarding tidal volumes, due to numerous reasons such as humification levels, sputum and circuit leaks, what is prescribed can be different what the patient receives, and the measurement does depend on where in the ventilator or patient circuit the variable is measured. However, although the initial prescribed tidal volume may differ from what the patient receives, expected clinical practice is to adjust the tidal volume to achieve 6 ml/kg on the measured expiratory tidal volume, taking into account that any huge discrepancy would lead to immediate investigation as to why this was occurring. Therefore, in this study, the use of expired tidal volume did not significantly impact the data collection, interpretation or results.
This study suggests two avenues for improvement of LTVV adherence in ICUs and therefore potentially of patient outcomes. First, as recommended by the College of Intensive Care Medicine of Australia and New Zealand, 15 LTVV adherence should be monitored as a quality of care measure. Second, additional interventions are required to improve LTVV adherence, potentially involving education of clinicians and nurses, improvements to information technology and record keeping, modifications to ventilation machines such as over-ventilation warnings and changes in unit responsibility and reporting practices. Further qualitative investigation into clinical decision-making and behaviour processes involved in selecting and implementing ventilation settings will help to target any future interventions effectively.
Conclusions
This study found poor adherence to the evidence-based LTVV strategy for mechanical ventilation of patients in an Australian metropolitan ICU. Patient height, which is necessary to calculate LTVV-adherent tidal volumes, was not recorded for the large majority (92%) of admissions, and among a subset of those admissions for which patient height could be found in other records, LTVV adherence was low (26%). Non-adherence to LTVV was positively associated with patient mortality. In the first Australian prospective study of an intervention intended to improve LTVV adherence by modifying the display of patients’ EMRs, we found that while the intervention was associated with a decrease in delivered tidal volumes, it was not clearly the cause of this shift, and the trend was not sustained. Further work is needed to understand clinician decision-making better regarding which ventilator parameters are selected for patients with hypoxic respiratory failure.
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this work.
Supplemental material
Supplemental material for this article is available online.