
Abstract
The current severe acute respiratory virus coronavirus 2 (COVID-19) pandemic has highlighted the largely untapped versatility of three-dimensional (3D) printing in medicine. As the technology has entered the mainstream, 3D printers have become as accessible as conventional desktop printers and can retail now for as little as a few hundred US dollars. Recently, 3D printing has been leveraged to create and modify personal protective and other equipment 1 in the context of global disruptions to traditional manufacturing supply chains.
Three-dimensional printing also facilitates the cheap and accessible production of anatomical models for medical education. These models can be produced for as little as a few dollars 2 compared to the substantial investment required to purchase commercial simulation trainers. Through recent improvements in available software, clinicians can now 3D print anatomical models from anonymised patient imaging, allowing educators to simulate procedures in both normal anatomy and more complex pathologies.
Developing a model for 3D printing previously required advanced computer modelling and engineering skills to design a 3D virtual computer-aided design (CAD) file and export it for 3D printing. However, with improved software, after some basic training, developing 3D virtual images and models are now within the realm of hobbyist and amateur users of 3D printers. Once a useable 3D file has been created, it can in theory be successfully replicated on any 3D printer utilising the same settings anywhere in the world, similar to how an email attachment can be downloaded and printed on any paper printer worldwide.
In low- and middle-income countries (LMIC), wired or wi-fi internet is not necessarily commonplace, but mobile data (3G/4G/5G) are still readily available. We aimed to ascertain if a healthcare team uninitiated in 3D printing could download, print and re-create a 3D phantom that had been developed by an expert team on the other side of the world with access to only simple instructions, mobile data, email and internet-based mobile messaging.
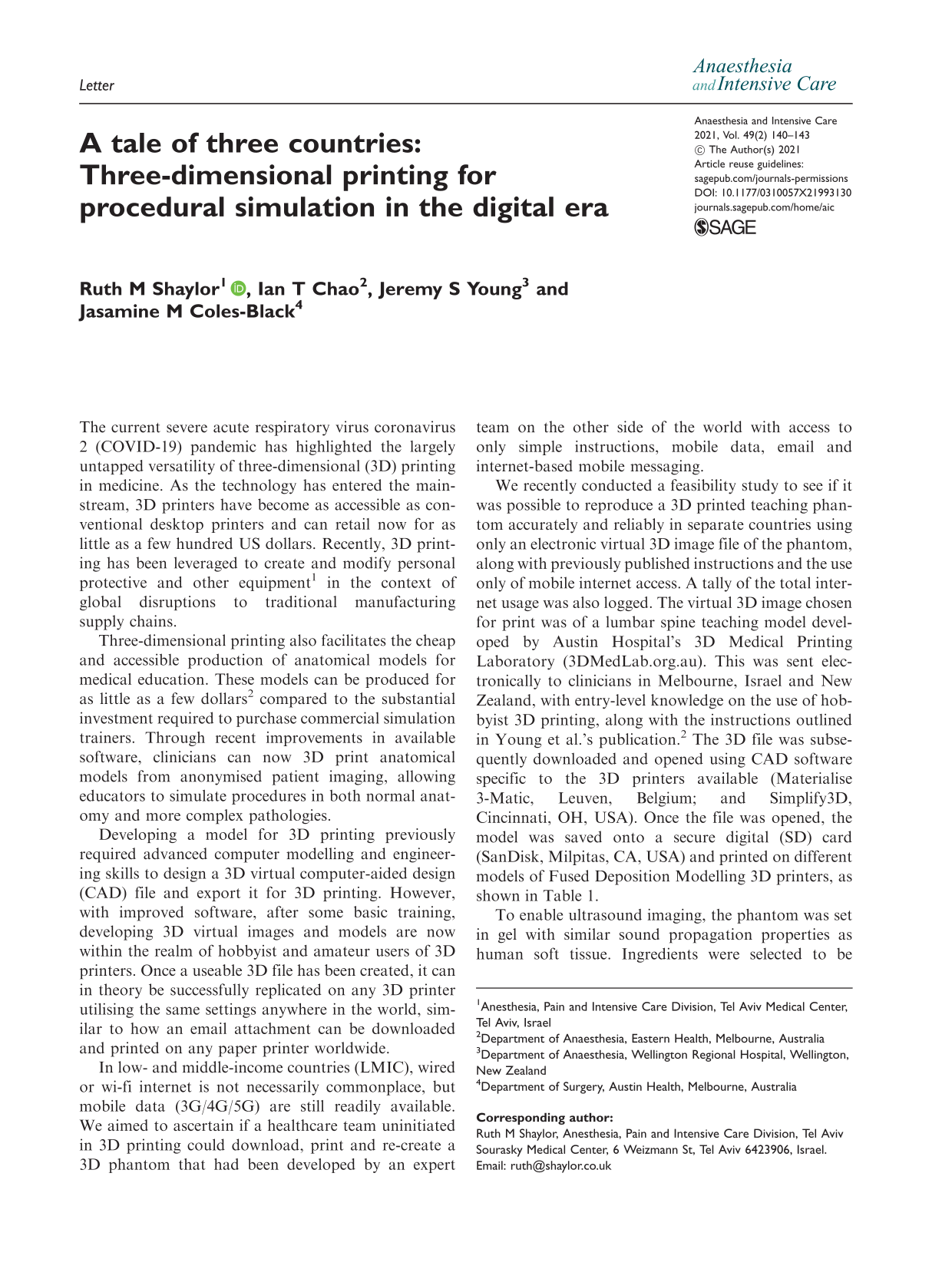
We recently conducted a feasibility study to see if it was possible to reproduce a 3D printed teaching phantom accurately and reliably in separate countries using only an electronic virtual 3D image file of the phantom, along with previously published instructions and the use only of mobile internet access. A tally of the total internet usage was also logged. The virtual 3D image chosen for print was of a lumbar spine teaching model developed by Austin Hospital’s 3D Medical Printing Laboratory (3DMedLab.org.au). This was sent electronically to clinicians in Melbourne, Israel and New Zealand, with entry-level knowledge on the use of hobbyist 3D printing, along with the instructions outlined in Young et al.’s publication. 2 The 3D file was subsequently downloaded and opened using CAD software specific to the 3D printers available (Materialise 3-Matic, Leuven, Belgium; and Simplify3D, Cincinnati, OH, USA). Once the file was opened, the model was saved onto a secure digital (SD) card (SanDisk, Milpitas, CA, USA) and printed on different models of Fused Deposition Modelling 3D printers, as shown in Table 1.
Three-dimensional printers and materials used in each participating centre.
All costs are in US$. Where there has been a conversion from local currencies, this was based on the exchange rate on 9 September 2020.
ABS: acrylonitrile butadiene styrene; PLA: polylactic acid.
To enable ultrasound imaging, the phantom was set in gel with similar sound propagation properties as human soft tissue. Ingredients were selected to be accessible in a low-resource setting. For the Israeli team, fish gelatine was used. Bovine gelatine was used in Melbourne and New Zealand. The gel was prepared according to the recipe previously published by Young et al. 2
To gauge further the achievability of this exercise where internet access may be limited, we tallied the total mobile data used. Any clarification regarding the standardised instructions was addressed via mobile messaging, and due to international time differences, a response was awaited before proceeding. All internet access was measured via phone hotspot tethering and precise recording of actual data usage for both file transfers and email or messaging for support.
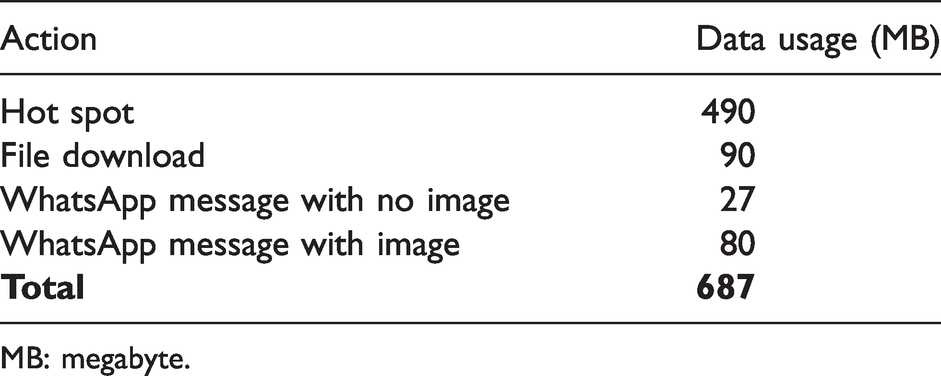
Within three days, each of the three centres successfully 3D printed the assigned neuraxial phantoms on the first attempt (Figure 1). Each model was an identical copy of the original, and accurately represented the anatomy seen on ultrasound in vivo, despite the use of different printers and materials. When assessed by an expert in neuraxial ultrasound, the images acquired were said to concur with the images obtained in clinical practice. The clinical educators at each centre agreed the 3D printed anatomical models were suitable for simulation training.
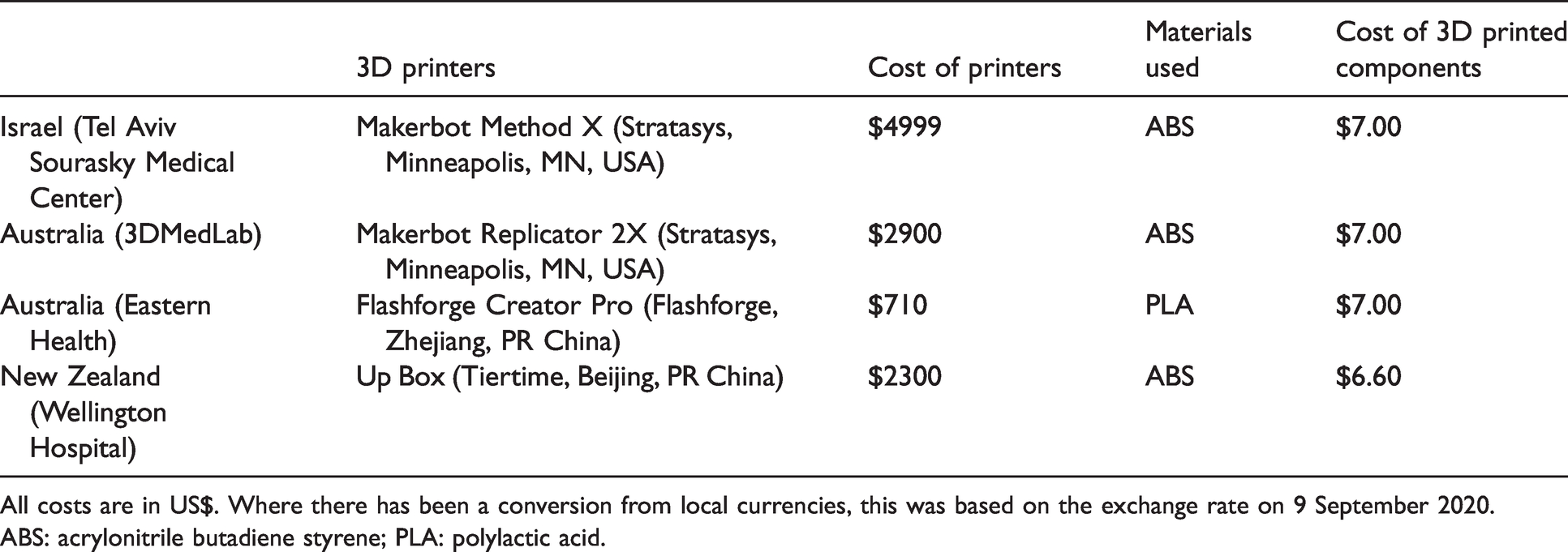
In total, three emails and 17 mobile messages were sent discussing the production of the lumbar spine phantom. This amounted to a total of 687MB of mobile data, as shown in Table 2.
A breakdown of data usage.
MB: megabyte.
We have demonstrated that high-fidelity teaching models using 3D printing can be produced using entry-level 3D printers and mobile data. Along with providing tertiary teaching institutions with affordable access to anatomical trainers, we believe this approach could have a significant impact on how procedural simulation and training is approached in low-resource settings.
Since Interplast pioneered the approach in 1969, it has become commonplace for medical teams to travel to LMICs to perform intense concentrated periods of treatment or surgeries serving the local population, such as cleft lip repairs. However, there has been a change in the approach towards medical aid in LMICs over the last two decades, with a gradual shift towards teaching and supporting local doctors to be able to undertake procedures themselves, thus creating a more sustainable approach. 3
With the travel restrictions due to the COVID-19 pandemic, it is challenging for medical teams to travel to low-resource settings to provide treatment or training. In order to adapt, it seems increasingly likely that teams will have to utilise the ubiquitous nature of mobile internet access as a means for ongoing education, be it by delivering seminars over videoconferencing or, as demonstrated, by exchanging ideas which culminate into tangible outcomes such as 3D files of educational resources. An inexpensive 3D printer could empower low-resource centres to be self-sufficient with much-needed equipment and supplies as well as for procedural skills training.
With the increased availability of 3D printers, there have been several projects investigating their utility in low-resource settings, for example printing parts for water systems, improving logistics and prostheses. 4,5 Thus far, 3D printers have been based in major centres or academic institutions, and we acknowledge that this feasibility study has thus far been conducted in developed countries. The next phase will be to transport 3D printers and supplies to a remote location and apply this technology in the field. However, we do not foresee any further constraints to achieving the above, so long as the materials, printer and basic internet connectivity are present, regardless of geographical locale.
In conclusion, our group has proven that it is feasible to recreate a high-fidelity, low-cost 3D printed lumbar spine phantom with limited prior experience, limited internet access, an inexpensive 3D printer and commercially available materials. This is the first step towards the inevitable adoption of 3D printing in remote and low-resource health settings to provide much-needed equipment during the COVID-19 pandemic and beyond.
A comparison of the different lumbar spine models. A1: The original lumbar spine model. A2: Ultrasound imaging of the original model. B1: The Melbourne lumbar spine model. B2: Ultrasound imaging of the Melbourne model. C1: The Israeli lumbar spine model. C2: Ultrasound imaging of the Israeli model. D1: The Wellington lumbar spine model. D2: Ultrasound imaging of the Wellington model. SP: spinous process; TP: transverse process; N: needle.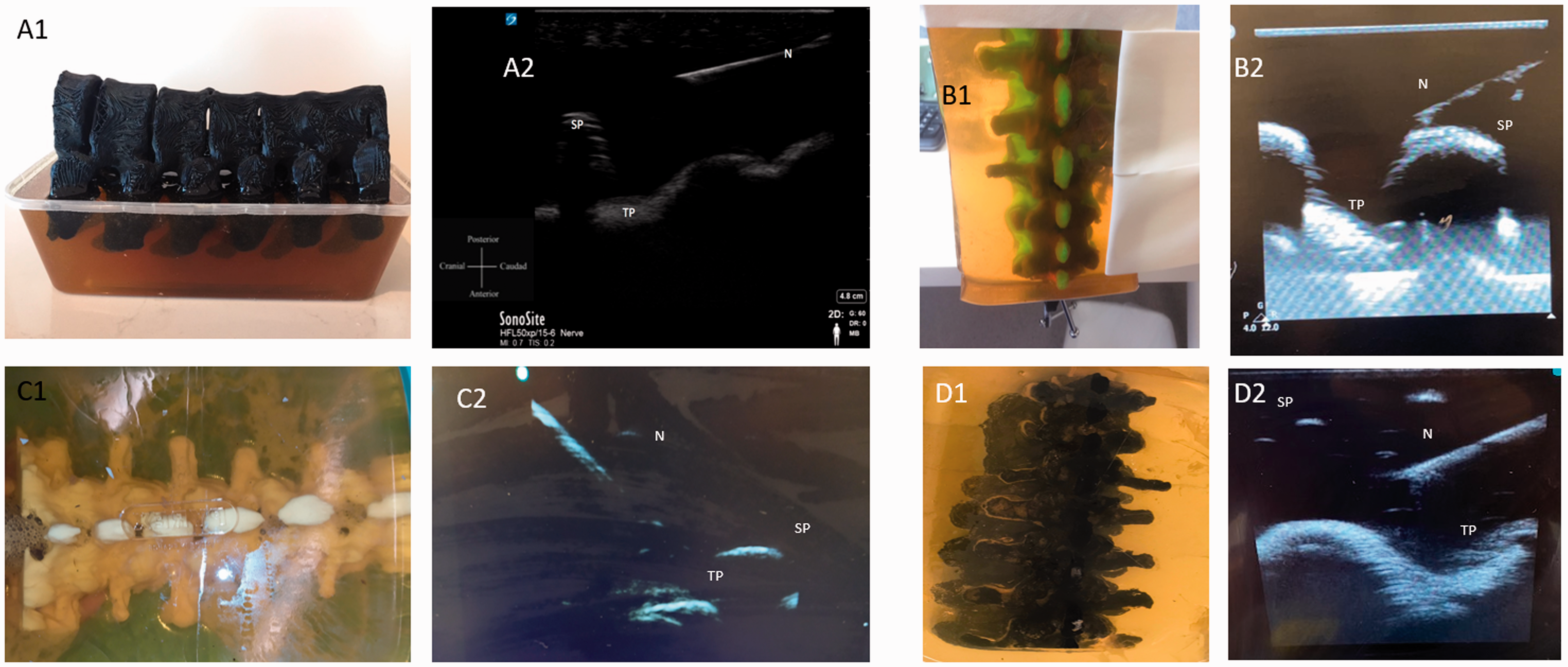
Footnotes
Author Contribution(s)
Acknowledgements
The authors would like to thank Austin Health 3D Med Lab for sharing the lumbar spine model file; Prof. Carolyn Weiniger and Dr Solomon Dadia for allowing access to the 3D laboratory at Tel Aviv Sourasky Medical Center; Esther Shaylor for sharing her expertise in using 3D printing in remote locations; and the Trustee for the Robert C. Bulley Charitable Fund for their research funding. The virtual 3D file of the ‘bones’ of the neuraxial trainer can be freely downloaded for use at ![]() . It has been made available under the terms of the Creative Commons Attribution Non-Commercial No Derivatives License which permits use without alteration for non-commercial clinical or educational purposes with proper citation of the author and copyright holder of the original work.
. It has been made available under the terms of the Creative Commons Attribution Non-Commercial No Derivatives License which permits use without alteration for non-commercial clinical or educational purposes with proper citation of the author and copyright holder of the original work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this work: Eastern Health printer and consumable materials were provided by the Robert Bulley Surgical Research Grant. The rest of this study was supported by departmental and institutional resources only.