
Abstract

We report a case of asystole requiring cardiopulmonary resuscitation (CPR) five hours after a bilateral endoscopic thoracic sympathectomy (ETS). The reasons for the report are to alert clinicians to this rare but serious complication of bilateral ETS, and to recommend postoperative cardiac monitoring of patients undergoing this procedure.
A 55-year-old female was scheduled for bilateral ETS to manage lifelong excessive head and neck flushing and sweating. Her medical history included type 2 diabetes, for which she took metformin, sitagliptin and gliclazide, and hypertension, for which she took perindopril. She had no personal or family history of bradycardia or syncope, and no family history of sudden cardiac death. Her preoperative electrocardiogram (ECG) demonstrated sinus rhythm at 66 bpm with a corrected QT interval (QTc) of 420 ms. Her preoperative blood pressure was 146/75 mmHg.
Muscle relaxation was induced with rocuronium, and intubation was with a double-lumen endotracheal tube. Bilateral ETS of the second and third sympathetic ganglia was completed uneventfully, and sugammadex was used to reverse muscle relaxation. The patient remained in the post-anaesthesia care unit for 90 minutes due to a persistent oxygen requirement, where an ECG showed a normal sinus rhythm at 70/min, a chest X-ray demonstrated bibasal collapse and routine fentanyl protocol (total 200 µg) was commenced for pain. The patient was admitted to the high dependency unit (HDU) with bibasal atelectasis for high-flow nasal oxygen, with a heart rate of 75/min on arrival at 1630 hours.
In the HDU, the patient received a total of 400 µg sublingual buprenorphine and 50 mg intravenous tramadol for pain over three hours. After passing urine on the commode, the patient complained of nausea and lightheadedness—telemetry at this time demonstrated a sinus rhythm of 75/min with a QTc of 400 ms. She was transferred to bed whereupon she became unresponsive and pulseless. CPR was commenced at 1940 hours followed by return of spontaneous circulation after 45 seconds, and the patient regained consciousness. Telemetry demonstrated asystole, progressing to 2:1 Mobitz type II block, followed by a normal sinus rhythm at 57/min with a QTc of 430 ms (Figure 1).
Asystole followed by 2:1 Mobitz type II block.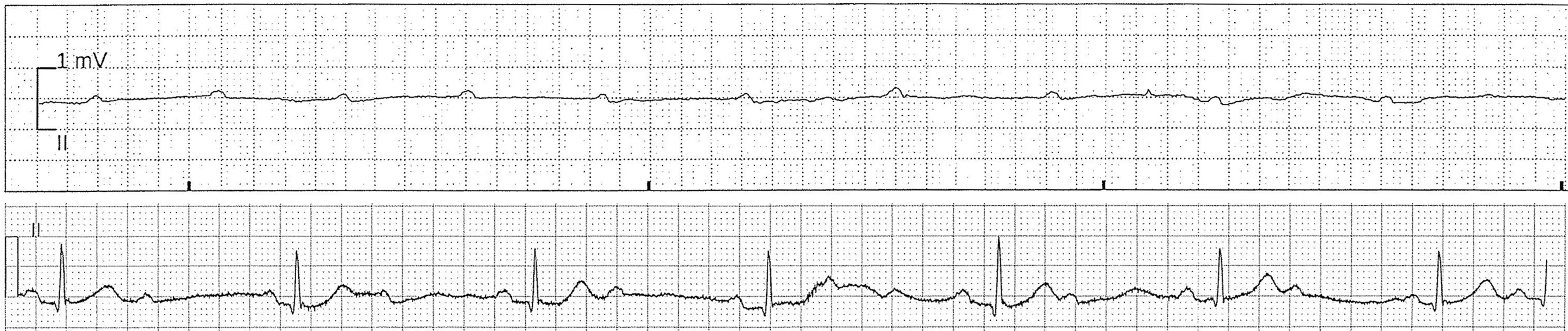
The patient remained cardiac monitored in the HDU without event for the next 72 hours, and computed tomography (CT) pulmonary angiography and transthoracic echocardiography performed during this time were unremarkable. After discussion with cardiology and cardiothoracic surgery, the patient underwent implantation of a loop recorder.
The patient remained asymptomatic, and at the six-month follow-up, there had been no further bradycardic episodes or prolonged pauses on interrogation of her loop recorder. CT coronary angiogram demonstrated a coronary calcium score of 0.
In the absence of pneumothorax, pulmonary embolism, structural heart defect, tamponade, electrolyte disturbance or toxins, the most likely cause of asystole in this case is unopposed overwhelming vagal tone from pain, nausea and micturition.
ETS is a procedure commonly performed for hyperhidrosis, a condition associated with wide-ranging social and professional impacts and significant psychological morbidity, including depression, anxiety and attention-deficit disorder. 1 Primary focal hyperhidrosis affects the palms, soles, axillae or face. Common risks include compensatory hyperhidrosis, bradycardia and Horner’s syndrome. 2 Rare risks include symptomatic bradycardia, 3 pneumothorax, pleural effusion, haemothorax, chylothorax and chronic pain. 2
Cardiac basal sympathetic tone originates from the premotor cells in the rostral ventrolateral medulla, which provides efferents via the sympathetic chain. Parasympathetic innervation is via the vagus nerve, which inhibits sympathetic tone beat-to-beat via reflex baroreceptor inhibition, primarily at the carotid sinus and aortic arch. Therefore, interruption of the thoracic chain in ETS may result in unopposed vagal impulses via reflex baroreceptor inhibition.
Bradycardia following ETS is fairly common, with one study demonstrating a decreased mean heart rate of 15% at 24 hours, persisting for six months. 4 Overall effect on heart rate is greater in bilateral ETS than unilateral ETS. However, there does not appear to be a consistent lateralising dominance of substellate fibres. 5 , 6 We must consider that those with primary hyperhidrosis may suffer from a pathological resting tachycardia in the context of autonomic dysfunction. Thus, a relative bradycardia post ETS may simply represent normalisation of the heart rate consistent with those without autonomic disorders. 4 Regardless, there has been one reported case of persistent symptomatic bradycardia secondary to unopposed vagotonia post-bilateral ETS, requiring pacemaker insertion. 7 There are also two reported cases of postoperative asystole: one during a second-stage (left then right) sympathectomy, 8 and one requiring pacemaker insertion following bilateral ETS. 9
Cardiovascular screening prior to ETS should include a baseline ECG, a targeted history of syncope or vagal symptoms and a review of all cardiovascular medications. Postoperative admission to a cardiac-monitored bed space should be strongly considered for high-risk patients, including those with bradycardia or a history of syncope or other vagal symptoms. We note that this was a case of asystole with no prior history of syncope, chronotropic medications or bradycardia. Thus, it may be difficult to risk stratify patients. For those with postoperative bradycardia or heart block, a long-acting parasympatholytic agent such as glycopyrrolate or a titratable beta-agonist such as isoprenaline may play a role in preventing asystole. For symptomatic bradycardia, first-line management is intravenous atropine 500 µg, followed by repeated doses up to 3 mg, transcutaneous pacing or adrenaline or isoprenaline infusion. 10 , 11
This is a case of asystole due to unopposed and overwhelming vagal tone secondary to pain, nausea and micturition. Cardiac arrest following ETS is an extremely rare complication. However, considering the potentially fatal consequences and reversibility of the condition, additional consideration must be given to postoperative monitoring of these patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.