
Abstract

Tracheostomies may be inserted to assist weaning from ventilation or to aid airway management. 1 Complications occur in up to 40% of patients, with tube displacement, tube obstruction, pneumothorax and haemorrhage most common.1–3 Prevention and management of tracheostomy emergencies requires multidisciplinary teamwork, a standardised approach, education, equipment, patient and carer involvement, and effective clinical governance.1,3,4 The use of clinical decision supports such as cognitive aids also improves performance, supports education, and guides quality improvement.1,5 The British National Tracheostomy Safety Project has developed extensive resources including emergency algorithms and bedhead signs. 6 We report on the development of an emergency tracheostomy management (ETM) cognitive aid at our institution (Figure 1). The aid is not intended to be used in laryngectomy emergencies.
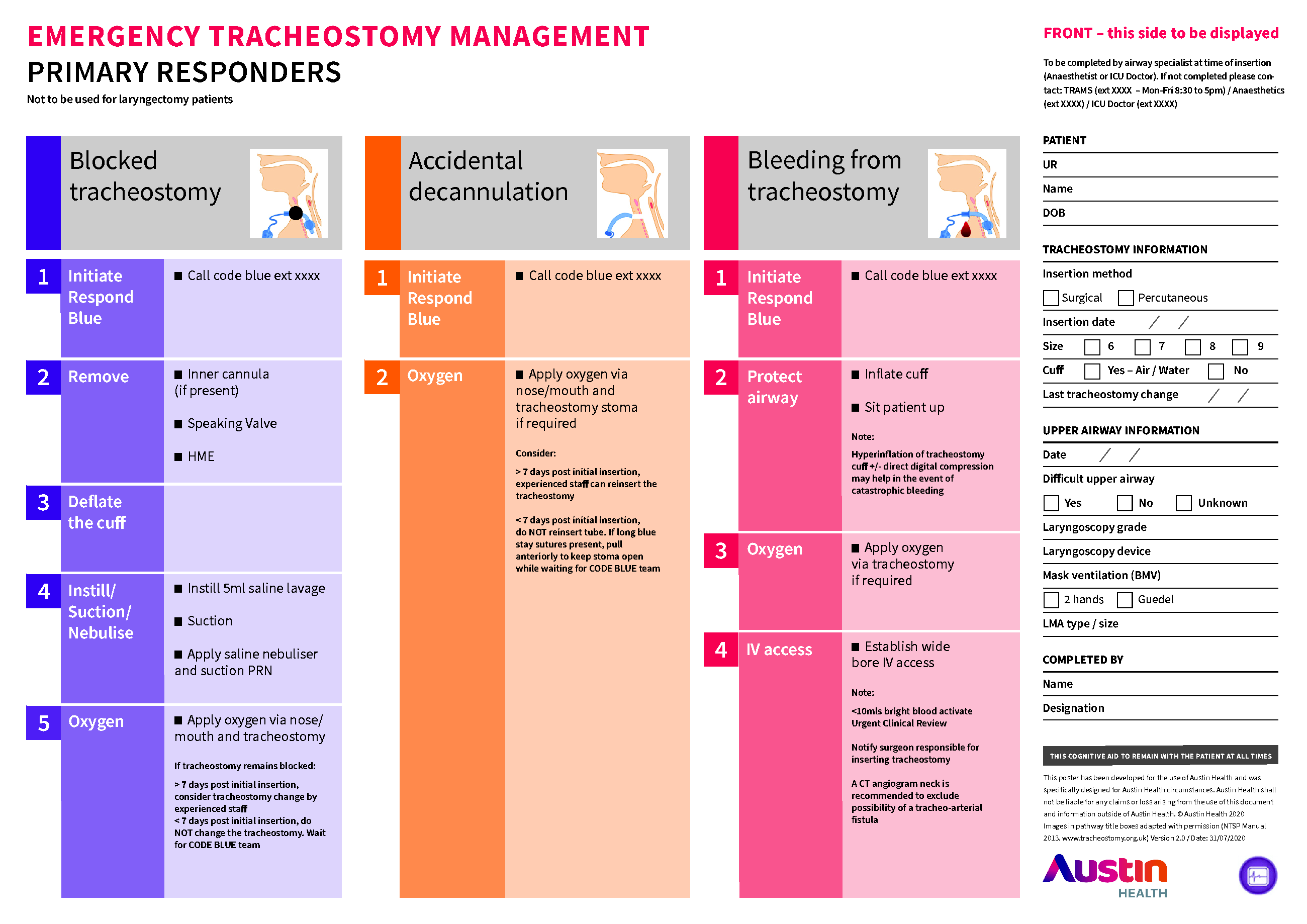
Emergency tracheostomy management cognitive aid.
Austin Health is a tertiary referral hospital with multiple different services involved in tracheostomy care. The intensive care unit (ICU), Department of Anaesthesia, and several surgical units including maxillofacial, thoracic, and ear nose and throat (ENT) provide care for patients with tracheostomies. Two state services, the Victorian Respiratory Support Service (VRSS) and the Victorian Spinal Cord Service (VSCS), also based at Austin Health, provide care to tracheostomy patients with complex ventilation needs and spinal injuries, respectively. The Austin Tracheostomy Review and Management Service (TRAMS) was established in 2002 as a multidisciplinary consultative service. 1 TRAMS coordinates tracheostomy care, management guidelines and education across all disciplines at Austin Health and is a founding member of the Global Tracheostomy Collaborative (GTC). 1 In addition, the departments of anaesthesia and intensive care undertake specific airway education and co-ordination of airway emergencies.
Cognitive aids are tools that enable an experienced individual or team to perform reliably, avoiding both fixation and key omissions.7,8 They have been described as implementation tools intended to be used in real time and should be distinguished from foundation tools which contain more detailed background information targeting novices. 8 Cognitive aids must be aligned with current best practice and introduced with an education and training campaign so that they are familiar and useable in emergency situations.8,9 By developing a shared mental model, cognitive aids support team communication and facilitate transfer of leadership when required. 10 The key steps of cognitive aid development include staff familiarisation, implementation and long-term cultural change.7,8 Developing a cognitive aid for tracheostomy emergencies is particularly complex (see Table 1). 5
Considerations in the design of a tracheostomy emergency cognitive aid.
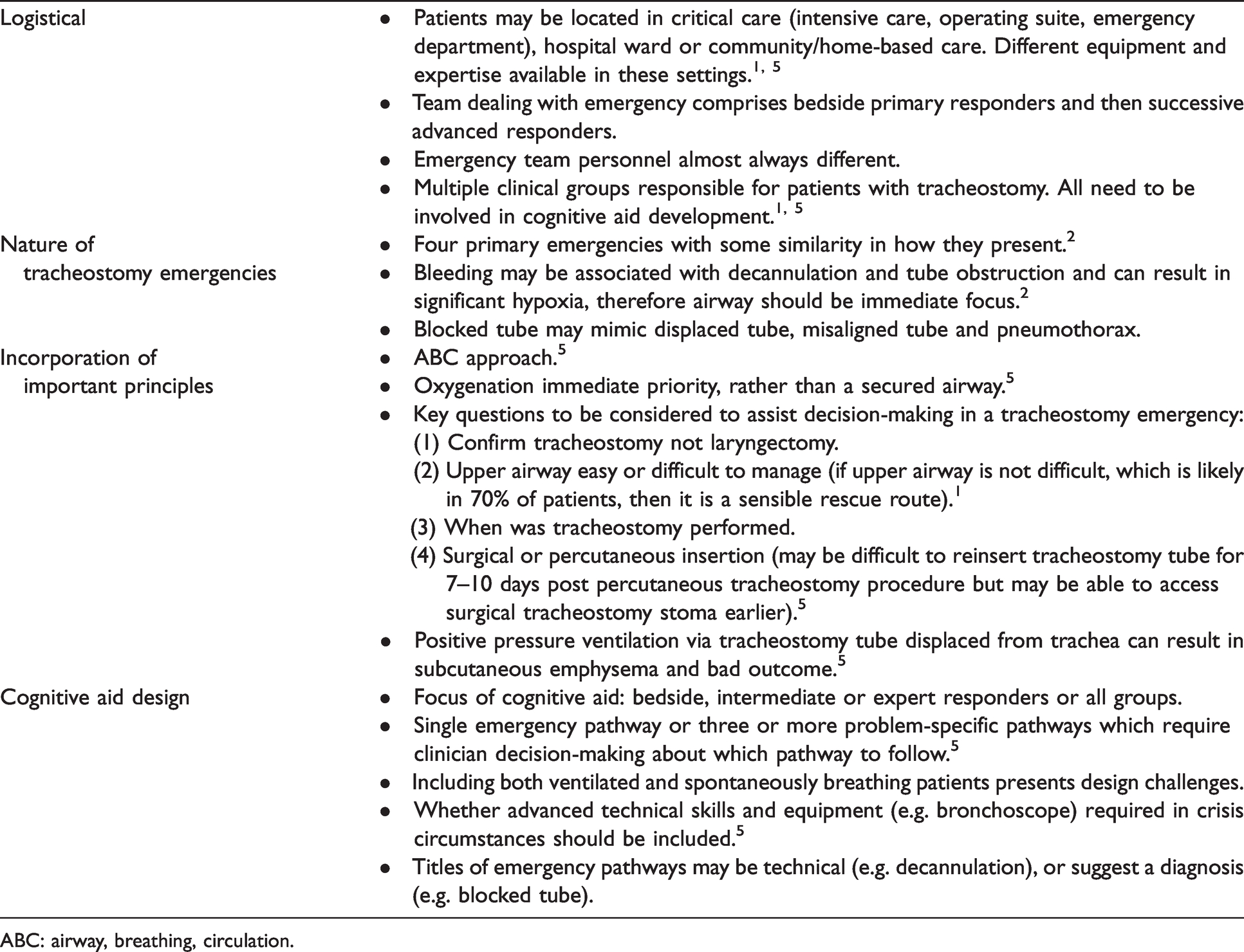
ABC: airway, breathing, circulation.
The Austin Health code blue team responds to all airway emergencies and includes an intensive care trainee, an anaesthetic trainee, a medical trainee and a senior ICU nurse. The amount of direct experience in managing tracheostomy emergencies may vary and while code blue team members are expected to have more advanced critical care skills than bedside staff, they are not necessarily tracheostomy experts. 5 A group was therefore formed to develop a cognitive aid for use by the code blue team in such situations. The task group decided to include three different emergency pathways in contrast to the single generic algorithm approach used in the British guideline. 5 The use of three emergency pathways was already successfully established in the hospital in the TRAMS cognitive aid and existing education and training. A bleeding pathway was felt to be important due to its potential catastrophic significance.1,11 The task group also thought consideration of alternative causes for an apparently blocked tracheostomy tube was important. The use of a bronchoscope is advocated in tracheostomy emergency 5 and it was considered valuable to provide guidance on its appropriate use. A linear rather than a branched algorithm approach was used to try and more simply reproduce real-life workflow of the expert clinicians on the task group.8,10 A displaced or blocked tube may require removal, therefore it was considered logical for it to be placed prior to decannulation/completely removed tube. Bleeding may present as difficulty breathing or ventilating or a blocked tube so appropriate for it to follow the first two pathways. There was a determination to include only important and not excessive information; 8 however, this was challenging given the variable experience of the code blue responders. Use of a title (e.g. suction) for each step with an accompanying description of the implications or further actions required in that step was chosen as a method to address this expertise gradient. An academic communication designer (TGS) worked with an intensivist (CMF), an anaesthetist (JMG) and TRAMS to develop the overall appearance and to maximise clarity and impact with the aid of end-user feedback.8,9 The ETM cognitive aid is printed in A3 size. The development and implementation of this cognitive aid will allow us to continue to monitor the incidence and outcomes of tracheostomy emergencies and modify its design and tailor educational activities to optimise patient safety.
The ETM cognitive aid is placed at the bedhead of every patient with a tracheostomy alongside emergency equipment. While tracheostomy emergencies are infrequent, they are challenging to manage and have a high risk of poor outcomes. Multidisciplinary training and a cognitive aid such as we describe may improve patient outcomes.
Footnotes
Acknowledgements
Acknowledgements to the following clinicians who reviewed the cognitive aid and provided valuable feedback: Naomi Atkins, Renee Bartlett, Matthew Campbell, Teresa Ewart, Nova Gibson, Mark Howard, Dharshi Karalapillai, Simon Knight, Mary Larsen and Sam Radford.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RMIT University was contracted by Austin Health for Trevor Streader to provide communication design services. Trevor Streader and Jon Graham are members of the same extended family.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RMIT University was contracted by Austin Health for Trevor Streader to provide communication design services. All other authors received no financial support for authorship and publication of this article.