
Abstract

These abstracts are published as supplied and have not been subject to editorial review or correction.
The effect of Remifentanil PCA vs Epidural in labour – maternal and neonatal outcomes
1Department of Anaesthesia, Northland DHB
2Department of Obstetrics and Gynaecology, Waikato DHB
3Department of Paediatrics, Waikato DHB
Background
Remifentanil is commonly used in obstetrics due to its fast metabolism time. Its effect on the neonate is unclear and studies are currently unable to correlate a negative effect of Remifentanil on the newborn.
Method
This project is registered with the clinical effectiveness, quality and patient safety department at Waikato Hospital (4086). Using a retrospective approach, we identified a total of 285 patients requiring Remifentanil patient controlled analgesia (PCA) presenting to Waikato delivery suite between the years 2017 to 2019. The primary outcome measured was an assessment of patients requiring further epidural analgesia post Remifentanil PCA. Secondary outcomes included number requiring caesarean section, instrumental use, number with a PPH or tear, apgars of neonates delivered, requirement for respiratory support after delivery, admission to the NICU, blood gas results of neonates and breastfeeding. This was compared to 285 patients requiring epidural analgesia.
Results
We found 24% (68 of 285) of Remifentanil patients required an epidural post PCA for further pain relief. Of the epidural patients, 1.75% (5 of 285) required a 2nd epidural after failing their first (RR 13.6, 95% CI 5.57–33.22, P = 0.0001, P < 0.05). 19% (53 of 285) of Remifentanil patients required caesarean section delivery compared to 31% (89 of 285) of epidural patients (RR 0.595, 95% CI 0.442–0.802, P = 0.0006, P < 0.05). 4% (12 of 285) of Remifentanil patients required instrument use compared to 11.2% (32 of 285) of epidural patients (RR 0.375, 95% CI 0.197–0.713, P = 0.0028, P < 0.05). 2.8% (8 of 285) of Remifentanil patients had a large PPH or tear compared to 3.5% (10 of 285) of epidural patients (RR 0.800, 95% CI 0.320-1.998, P = 0632, P > 0.05). NICU admission were less in the Remifentanil PCA group (48 neonates [17%] vs. 22 neonates [11%], p = 0.04), but when corrected for premature gestational age (a confounder for admission into NICU) this observation remains statistically significant (p = 0.04). Proportionately more babies were documented as requiring assistance breast feeding in the epidural group (103 women [37%] 29 women) [17%], p = 0.02). Cord gases showed no statistical significance in acid base status.
Conclusion
This data demonstrates advantages for both maternal and neonatal outcomes with remifentanil IV PCA but that a significant number of women will go on to require epidural analgesia after receiving remifentanil. More research is required before a causal relationship can be identified
References
Acute Renal Impairment in Elderly Patients after Hip Fracture Surgery (CHIEF Study)
1Department of Anaesthetics, Eastern Health
Background
Acute renal impairment (ARI), even minor impairment, is a significant risk factor in surgical patients.1 Elderly patients undergoing hip fracture surgery represent a high-risk patient group who are prone to postoperative complications. In this study, we examined the rate of ARI in this patient group and its association with mortality.
Methods
The CHIEF study was approved by the Eastern Health Human Research Ethics Committee (Ref: LR86-2015). Patients aged 70 years or over presenting to a metropolitan Australian hospital with a hip fracture requiring surgery between June 2011 and July 2015 were retrospectively analysed. Electronic medical records were used to collect patient data. Traditionally, acute kidney injury is defined by a 50% increase in creatinine2, but this may exclude patients who have smaller but still clinically significant impairment. Therefore, we defined ARI as a creatinine increase of 20% of the pre-operative value.1 Descriptive statistics were used to calculate rates of mortality and ARI. Statistical analysis was performed to examine ARI as a risk factor for 30-day mortality postoperatively.
Results
In the cohort of 825 patients, 805 had a recorded pre-operative and post-operative creatinine levels. 359 patients (45%) had pre-operative kidney impairment (estimated glomerular filtration rate <60 mL/min/1.73m2). 85 patients (11%) died within 30 days postoperatively. 111 patients (14%) developed ARI, 25 of whom (23%) died within 30 days postoperatively. The odds ratio for patients with ARI dying within 30 days is 3.07 (95% Confidence Interval 1.83–5.16, p < 0.001).
Conclusion
Our study has shown a significant risk of mortality even with a lower threshold of defining kidney impairment. This is consistent in previous studies using this definition for elderly patients undergoing other operations.1 ARI is a common complication for elderly patients undergoing hip fracture surgeries which poses a significant mortality risk. Using a lower threshold for ARI may alert clinicians to otherwise unrecognised kidney injury and ensure better postoperative outcomes.
References
Discharge Destinations of Elderly Patients after Hip Fracture Surgery (CHIEF Study)
1Department of Anaesthetics, Maroondah Hospital, Eastern Health, Melbourne, Australia
Background
Previous studies have shown only half of patients are able to return home on discharge following surgical hip fracture repair 1 . In this study, we aim to analyse the discharge destinations of elderly patients who underwent surgical repair for hip fractures.
Methods
The CHIEF study was approved by the Eastern Health Human Research Ethics Committee (Ref: LR86-2015). A retrospective analysis was conducted on patients aged 65 years or over between June 2011 and July 2015, presenting to a metropolitan Australian hospital with a hip fracture requiring surgical management. Electronic medical records were used to collect demographics, perioperative data, and discharge destinations post-acute admission. We especially noted those patients who required an upgrade in their existing care needs. Descriptive statistics, statistical analyses and logistic regression were used to describe these discharge destinations and examine factors that are associated with each discharge setting.
Results
There were 864 patients included in the study; 6.7% of patients died during their hospitalisation. Of those who were alive, following discharge from acute admission, 4% returned directly home, 34% returned to their own residential age care facility (RACF), 1% went to a new RACF, and 56% required a subacute admission. Following final hospital discharge, 41% returned home, 35% returned to their original RACF, and 9% were placed at a new RACF (either from home or upgrade from their original facility). Patients with American Society of Anaesthesia (ASA) score of III or higher and older patients were more likely to require new placement at a RACF. There was no significant difference in terms of discharge location between sexes.
Conclusion
In elderly patients following surgical repair of hip fractures, most required at least a subacute admission, with a significant portion needing an escalation in their care needs on final discharge. Clinicians should be aware of the significance of this to ensure accurate postoperative discharge planning.
Reference
Perioperative thromboembolic events related to intraoperative application of topical gelatin and albumin-glutaraldehyde based haemostatic agents: a review of case reports and case series
1Central Adelaide Local Health Network
2The University of Adelaide
3The Queen Elizabeth Hospital Anaesthetic Department
4Discipline of Acute Care Medicine, University of Adelaide, Australia
Background
Recent work has highlighted the risk of intraoperative anaphylaxis from gelatin-based haemostatic agents 1 . However, an under-recognised complication of GBA and albumin-glutaraldehyde-based haemostat agents (AGA) is their potential to embolise. This review aims to collate and analyse cases reported in the literature of perioperative thromboembolic phenomena secondary to locally applied GBA and AGA agents.
Methods
An electronic search was performed on databases Embase, Ovid Medline, Proquest, Scopus and Pubmed. 8875 articles were reviewed from title and abstract. After exclusion, 13 articles with 18 cases were included for analysis. Data extracted from each of the articles included patient demographics, surgery type, haemostatic agent used, clinical features, radiology and pathological findings, and morbidity and mortality.
Results
Thromboembolic events included fourteen secondary to GBA and four from AGA. Cases included twelve pulmonary emboli, three peripheral emboli, two cerebral emboli and one coronary embolus. Embolic phenomena was most common following spinal orthopaedic surgery in GBA patients (43%), and Type A Aortic dissection repair in AGA patients (100%). The application of 10ml or more of GBA was frequently reported in cases (64%). Echocardiography was utilised in 80% of intraoperative PE’s. Postoperatively, computed tomography successfully identified GBA emboli through the ‘pseudo-air’ sign 2 . Six cases were fatal. The time course to each event ranged from occurring intraoperatively to 45 days post operation.
Conclusion
GBA and AGA agents are associated with venous and arterial embolisation, and high overall mortality. Spinal orthopaedic surgery may expose the valveless vertebral plexus, posing risk of migration to the pulmonary vasculature. Surgical fields should be dried before the application of AGA. Quantities of GBA > 10 mL were frequently reported. GBA and AGA embolisation can occur anywhere from immediate to 45 days post operatively. Communication between surgical and anaesthetic staff should occur at time of application of these agents.
References
Trends in Front of Neck Access – A bibliometric analysis
1Central Adelaide Local Health Network
2Adelaide University Medical School
Background
Front of Neck Access (FONA) is a critical skill Anaesthetists must be able to perform in the ‘Can’t Intubate, Can’t oxygenate’ (CICO) scenario, and is a core technical skill ANZCA registrars must develop during training (ANZCA 2020). However, since the Covid-19 pandemic, opportunities for first hand emergency airway experience have reduced. To gain an understanding of trends in the field of FONA and to guide future advancement, we conducted a bibliometric analysis of the 100 most cited papers for Front of Neck Access.
Methods
The Thomas Reuters Web of Science database was searched on 13th of June 2021 using the terms; “Front of Neck Access”, “FONA”, “Cricothyroidotomy”, “Surgical cricothyroidotomy”, “Scalpel Cricothyroidotomy”, “Needle Cricothyroidotomy”. The 100 most cited papers relevant to FONA were analysed by design, topic, author, publication year and institution. The journal impact factor for the year 2019 along with Eigenfactor scores were recorded.
Results
A total of 787 papers were retrieved from our search. These were ranked by total number of citations. The median number of citations for the top 100 articles was 56.5 (IQR 28), with 44% of articles originating from the USA. The top five cited papers made up 37% of total citations. Anesthesia (n = 9) and The British Journal of Anesthesia (n = 9) had the greatest number of papers, whilst the greatest number of citations came from Academic Emergency Medicine (n = 2456). The years 2011 (n = 9) and 2015 (n = 9) had the greatest number of papers published. Technique for emergent FONA was the most common theme.
Conclusions
The most influential articles in the FONA literature have each been cited at least 35 times, reflecting considerable impact and quality. The USA has produced most research in this area, allowing the widespread dispersion of indications, technique and guidelines at a time when practical experience may be limited due to the pandemic.
References
Volatile anaesthetic use in the paediatric population at Christchurch Hospital
1Department of Anaesthesia, Christchurch Hospital
2University of Otago, Christchurch, New Zealand
Background
There is an increasing understanding of the overwhelming effects of climate change on human health. Healthcare itself makes a significant contribution, and inhalational anaesthetics have a high global warming potential. Our department has a long interest in reducing environmental impact by rationalising inhalational anaesthetic agent use. We repeated an audit 1 of the proportion of inhalational and intravenous (IV) anaesthetics in paediatric practice at our hospital, and the amount of sevoflurane being consumed. We expanded the audit to include nitrous oxide (N2O) and to investigate the hypothesis that inhalational induction in the anaesthetic room followed by a move to the operating theatre increases overall gas consumption.
Methods
Our study was approved by the New Zealand Health and Disability Ethics Committee (HDEC 21/CEN/35). We recorded demographics, consumption of inhaled anaesthetics during induction and maintenance, and the influence of the anaesthetic room on total usage.
Results
205 cases were available for analysis. 167 (81%) had inhalational inductions, 130 (63%) of these were maintained on sevoflurane while 37 (18%) were transitioned onto IV maintenance. Volatile anaesthetics used a median of 20mLs sevoflurane (IQR 16–29.25) and 12.41 L of N2O (IQR 8.3–19.9). If the patient was transitioned onto IV maintenance after an inhalational induction, then sevoflurane consumption was reduced about half to 10 mLs (IQR 8–13). There was no difference between the amount of sevoflurane or N2O used when the patient was induced in the anaesthetic room, compared to induction in theatre. N2O was not used for maintenance.
Conclusion
This study re-emphasised our previous observation that a large proportion of agent consumption occurs during induction of anaesthesia. Surprisingly we found that use of the anaesthetic room did not increase total gas consumption. This is thought to be due to a trend to reduce gas flows immediately after induction when the patient is moved to theatre.
References
Pharmacokinetics and pharmacodynamics of sevoflurane in adults during general anaesthesia
1Department of Pharmacology and Clinical Pharmacology, University of Auckland
2Department of Anaesthesiology, University of Auckland
3Department of Anaesthesia, Auckland City Hospital, Auckland, New Zealand
Background
The relationship between arterial sevoflurane concentration and depth of anaesthesia is poorly described. We aimed to quantify the relationships between inspired sevoflurane concentration, arterial blood concentration and bispectral index in adults using compartment models to describe sevoflurane disposition.
Methods
This study was approved by the New Zealand Northern Health and Disability Ethics Committee (HDEC 12/NTA/77) and registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12612001296820). Locality approval was granted from Auckland District Health Board (A+5741). All participants gave written informed consent. Participants were 64 adults (19–86 years, 44–160 kg, American Society of Anesthesiology Score 1–3) undergoing general anaesthesia with sevoflurane as the primary anaesthetic agent. Sevoflurane dose, arterial sevoflurane concentrations and bispectral index were analysed using nonlinear mixed effects models. The Greco response-surface model accounted for the additive effects of propofol, remifentanil and morphine with sevoflurane on bispectral index. Parameter estimates were scaled for size using theory-based allometry and standardised to a 70 kg individual.
Results
Sevoflurane pharmacokinetics were described using a three-compartment model. An absorption half-time (TABS) was used to quantify the absorption of inspired sevoflurane from the lungs to blood. An effect-site compartment was used to relate sevoflurane concentrations to effect, linked using an equilibration half-time, T1/2 keo. The parameter estimates (%CV) were: TABS 19.8 (56.1%) seconds (56.1), CL 201 (91.9%) L/h/70 kg, Q2 591 (75.4%) L/h/70 kg, Q3 870 (61.4%) L/h/70 kg, V1 13.4 (84.9%) L/70 kg, V2 93.4 (63.6%) L/70 kg, V3 35500 (5.5%) L/70 kg. Bispectral index was described using a sigmoidal fractional maximal effect (EMAX) model. Baseline bispectral index (E0) was fixed at 98 (3.73%) and the maximal effect (EMAX) estimated at 0.636 (42.8%). The effect-site concentration producing half of EMAX (Ce50) 26.4 (67.9%) mg/L and the Hill exponent was 3.74. The T1/2 keo was 1.4 minutes.
Conclusions
Sevoflurane pharmacokinetics and pharmacodynamics were described using inhaled gas concentration, plasma concentration and a measure of drug effect. Response surface methods accounted for the combined effect of propofol, remifentanil, and morphine on bispectral index. The short T1/2 keo suggests rapid distribution of sevoflurane from the blood to the effect-site.
Coolsense® versus EMLA® for peripheral venous cannulation in adult volunteers: a randomised crossover trial
1Canterbury DHB, Christchurch, Canterbury, New Zealand
2Royal Papworth Hospital, Cambridge, United Kingdom
Background
Peripheral venous cannulation is a commonly performed invasive medical procedure. Topical treatments such as eutectic mixture of local anaesthetics (EMLA®) attenuate the associated pain 1 , but are limited by requiring up to one hour of application before becoming effective. The Coolsense® Pain Numbing Applicator is a new device using a cryoanalgesic means to anaesthetise skin within seconds. Coolsense is being increasingly used for cannulation, but comparative studies are lacking 2 .
Methods
This study was deemed to be outside the scope of review by the Health and Disability Ethics Committee of New Zealand after submission of the protocol because it involved a low-risk medical device (HDEC 18/STH/2). Local approval was granted by the University of Otago Research Office (RO#18115) and Māori consultation through Te Komiti Whakarite of Canterbury District Health Board. The RCT was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12618001354279). We recruited 64 healthy adult volunteers to this open-label two sequence, two period randomised crossover trial. Participants had two 20 gauge venous cannulae inserted, one on the dorsum of each hand. Each cannulation attempt was preceded by treatment with Coolsense or an EMLA patch containing 2.5% lignocaine and 2.5% prilocaine. The primary outcome was participant pain using the 0–10 Numerical Pain Rating Scale. Secondary outcomes were participant satisfaction scores on a 0–10 scale, treatment preference and failed cannulation attempts. Participants were randomised to either the Coolsense EMLA (n = 32) or EMLA Coolsense (n = 32) sequence.
Results
All participants completed the trial. The pooled mean paired difference of Numerical Pain Rating Scale was −1.84 (95%CI, −1.28 to −2.41; p < 0.001) in favour of EMLA. The pooled mean paired difference for satisfaction score was 2.26 (95%CI, 1.46 to 3.07; p < 0.001) higher with EMLA. Most participants preferred EMLA over Coolsense (p < 0.001). There was no significant difference regarding failed cannulation between the two treatments (p = 0.14).
Conclusions
Amongst healthy individuals undergoing elective peripheral venous cannulation, EMLA was associated with reduced pain, increased satisfaction and was the preferred treatment compared to Coolsense.
References
A multidisciplinary approach to rib fractures at Waikato Hospital
1Department of Anaesthesia, Waikato Hospital, New Zealand
Background
Rib fractures complicate trauma admissions in 10% of cases and increase patient morbidity and mortality. A multidisciplinary rib fracture analgesic protocol was developed at Waikato Hospital to improve patient outcomes. This study assessed the implementation and impact of the rib fracture analgesic protocol through comparison with a previous audit.
Methods
Approval for this study was obtained through the Waikato Clinical Audit Support Unit (#3877). Ethics approval was not required. 50 trauma patients presenting with rib fractures were prospectively assessed. The primary outcome was protocol compliance which was determined by inpatient pain service (IPS) referral, use of the analgesic protocol and physiotherapy involvement. Secondary outcomes included; 30-day mortality, respiratory complications, duration of admission, intensive care unit (ICU) admission, oxygen requirement and surgical interventions. Pain and functional activity scores were also measured.
Results
50 patients were assessed between March and June 2019. 5 were excluded due to incomplete or inaccessible records. 71% of the study population were male with an age range of 19 to 91 years. Motor vehicle accidents accounted for 73% of cases and half of patients (47%) had a severe rib fracture score. 98% were reviewed by the IPS within one day of referral and 100% received physiotherapy input. 98% of patients received intravenous opioid patient controlled analgesia and regional anaesthetic blocks were administered in 42%. 30-day mortality was 4% and pneumothoraces were the most common complication (62%). 24% of patients required ICU admission. Supplemental oxygen was required by 76% for a median of 5 days. Over the first three days of admission pain scores improved from 5.9 to 3.5 and severe functional limitation reduced from 62% of patients to 27%.
Conclusions
This study demonstrates excellent compliance with the rib fracture analgesic protocol and a marked improvement in patient outcomes compared with a previous audit.
References
A retrospective study on intra-operative cell salvage in patients undergoing total hip replacement or revision hip replacement surgery at the Royal Adelaide Hospital in 2020
1Central Adelaide Local Health Network
2The University of Adelaide Medical School, Australia
Background
Cell Salvage (CS) is a blood conservation technique, aimed at reducing allogeneic blood transfusion (ABT) and its associated complications1,2. CS has been demonstrated as beneficial to patients undergoing primary (pTHR) and revision total hip replacement (rTHR). This study aimed to determine how CS use has evolved, and evaluate the effect of CS on patient outcomes within the context of South Australia’s major orthopaedic trauma centre.
Methods
This study was approved by the Central Adelaide Local Health Network Human Research Ethics Committee (ref: 14344). Patients were identified through the Operating Room Management Information System. Data was extracted into the database RedCap including patient demographics, ABT administered, tranexamic acid (TXA) administration, CS volume delivered, post-operative haemoglobin (Hb) concentrations and length of stay (LOS).
Results
151 patients, undergoing 93 pTHR and 58 rTHR surgeries were identified. CS was used in 15 patients (9.9%), 14 of whom underwent rTHR, a significant increase since 2014 when it was utilised in 1.3% of patients (p = 0.0134). An average of 400ml [IQR 228 – 657] was collected across the whole cohort of CS patients, this was higher in those undergoing a procedure for a septic joint (792.3ml). 90 ABT units were transfused to patients intraoperatively or within 24 hours. Eight ABT’s were for patients undergoing pTHR, with the remainder 82 going to rTHR (p = <0.004). 88% of patients received intraoperative TXA, this did not reduce the risk of ABT (p = 0.76), however, did improve discharge Hb concentration (9.46 g/L 95% CI 2.80 to 16.12, p = 0.006).
Conclusions
CS use for patients undergoing THR has increased since 2014, most notably for rTHR. This is line with prior research demonstrating benefit1. There was no reduction in patients requiring at least one PRBC transfusion within 24 hours in patients who received CS or in those administered TXA. Increased use of CS for patients undergoing rTHR may be of benefit, given the significantly higher ABT requirement in this population.
Institutional ethics approval was gained for this project.
The Association between Quality of Recovery Metrics and Postoperative Opioid Use following Elective Total Knee Arthroplasty
1Faculty of Medical and Health Sciences, University of Auckland
2Department of Anaesthesia and Pain Medicine, Counties Manukau Health, New Zealand
Background
Opioid analgesics are commonly used following Total Knee Arthroplasty (TKA) to manage pain and improve patient recovery. Persistent opioid use following surgery can lead to short- and long-term adverse effects. We aimed to investigate whether patient-reported outcome metrics, such as the Quality of Recovery-15 (QoR-15), collected following TKA are associated with postoperative opioid use, and to determine predictors for the QoR-15.
Methods
Auckland Health Research Ethics Committee (AH21894) and Counties Manukau Health Research Office (1368) approvals were obtained. We retrospectively identified patients who underwent unilateral TKA at our institution between 1st January and 31st December 2018. QoR-15 scores collected from Post-Operative Day (POD) zero and one were summated. Patients were stratified into three groups by summated QoR-15 score: Low (<25th), Medium (25–75th), High (>75th percentile). The primary outcome was the proportion of patients dispensed strong opioids within 30-days following discharge. Secondary outcomes included inpatient opioid consumption and other recovery metrics. Regression models were developed for inpatient opioid consumption and QoR-15 respectively.
Results
There were 362 patients eligible for inclusion, of whom 202 completed at least one QoR-15 survey. Baseline demographics between groups were similar except for gender (p = 0.01). In the low summated QoR-15 group, 87.9% were dispensed either morphine or oxycodone within 30-days following discharge, compared to 56.3% in the high group (p = 0.005). Inpatient opioid consumption on POD zero was significantly correlated with QoR-15 on POD zero (p = 0.009). This was also significant at POD one (p = 0.016). Correlation between summated QoR-15 and Days Alive and Out of Hospital at thirty-days, and Length of Stay revealed significant associations (p = 0.005; p < 0.001 respectively). Predictors of QoR-15 score included ethnicity, gender, and POD-one opioid consumption.
Conclusions
There is an association between QoR-15 and opioid dispensing after TKA, suggesting that patient-reported measures of early recovery may impact later trajectory and pain experience.
The Impact of Unilateral versus Bilateral Hip and Knee Arthroplasty on Haematological Parameters in the Perioperative Period: A Retrospective Cohort Study
1University of Auckland, Auckland, New Zealand
2Department of Anaesthesia and Pain Medicine, Counties Manukau Health, Auckland, New Zealand
3Department of Anaesthesiology, University of Auckland, Auckland, New Zealand
Background
Hip and knee arthroplasty (THA/TKA) are common procedures to reduce pain and improve quality of life. Patient Blood Management describes the optimization of haematological parameters to facilitate the surgical procedure. The purpose of this study is to determine the adequacy of optimization of these parameters and their impact on outcomes following unilateral or bilateral arthroplasty.
Methods
This project was approved by the Counties Manukau Health Research Office (number-1290). Patients undergoing either unilateral or bilateral THA and TKA between the 1st January 2017 and the 31st December 2018 were identified. Propensity score matching was used to produce two cohorts who had undergone unilateral or bilateral procedures. The primary outcome was the change in haemoglobin between the pre- and post-operative measurements. Secondary outcomes included haematological and patient centered measures. A two tailed p-value of <0.05 defined statistical significance.
Results
Overall, 1326 patients underwent surgery, with 58 (4.4%) bilateral procedures. Propensity score matching produced two cohorts with 46 (22.3%) bilateral and 160 (77.7%) unilateral procedures. There were no differences in baseline demographics (Table One). There was no difference in the incidence of preoperative anaemia (23.9% versus 17.5%, p = 0.39) or those with a baseline ferritin <100 ug/L (39.4% versus 46.8%, p = 0.67). Surgery in the bilateral group occurred more frequently at Middlemore Hospital (p < 0.001) and patients required critical care more frequently (p < 0.001). There was no difference in the number who had iron studies prior to surgery (10.9% versus 7.5%, p = 0.54) or who received IV iron (2.2% versus 1.3%, p = 0.53). The change in haemoglobin was greater in the bilateral group (28 (interquartile range: 20–34) versus 19 (13–25) g/L, p < 0.001) with more frequent allogenic transfusion (13.0% versus 1.3%, p = 0.002).
Conclusions
Bilateral arthroplasty is associated with greater change in haemoglobin and more transfusion. In this cohort, the rate of optimization of preoperative iron stores was low.
Table One
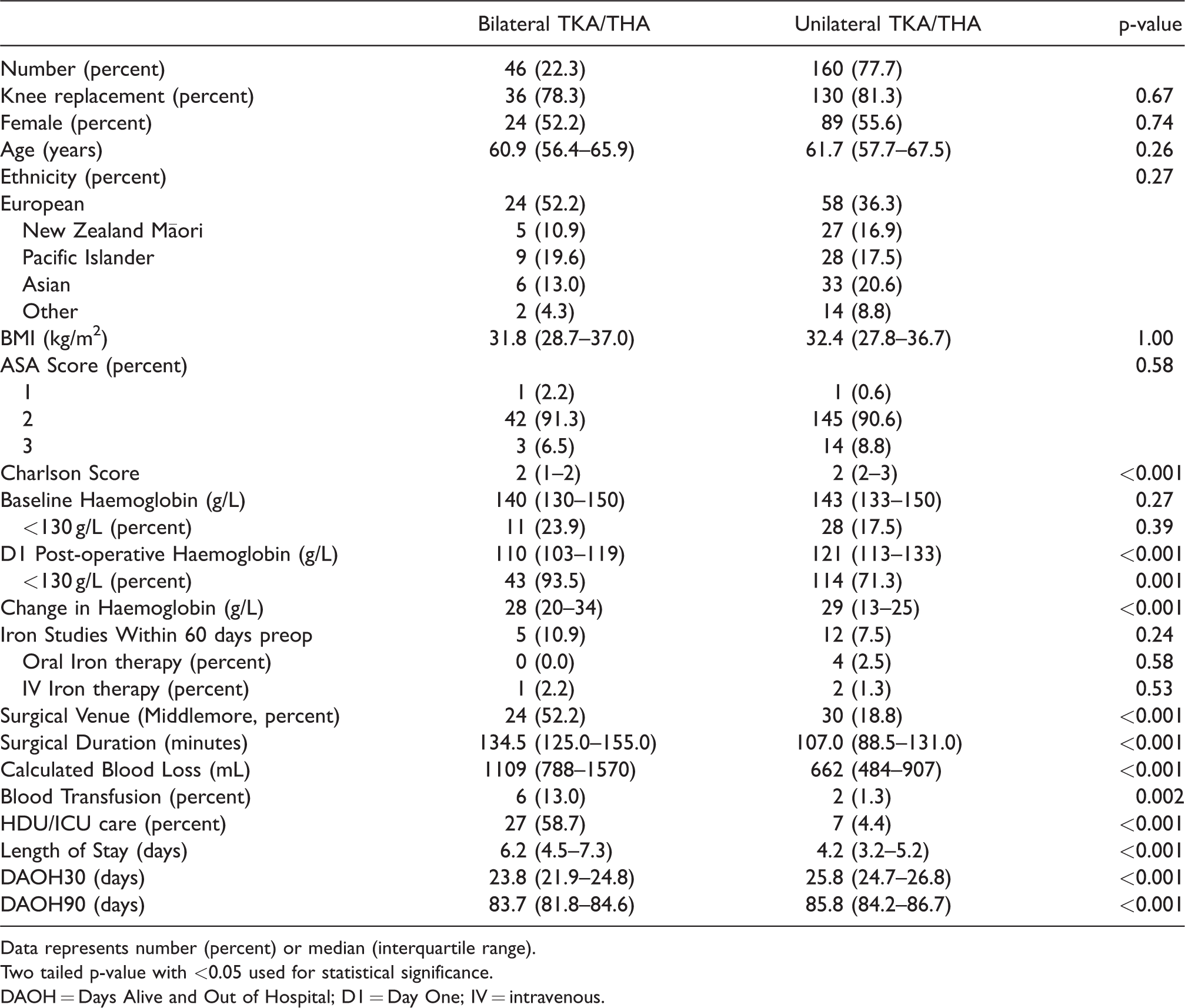
Data represents number (percent) or median (interquartile range).
Two tailed p-value with <0.05 used for statistical significance.
DAOH = Days Alive and Out of Hospital; D1 = Day One; IV = intravenous.
Functional Assessment in the Anaesthetic Assessment Clinic: Introduction of the Duke Activity Status Index (DASI) Questionnaire
1Department of Anaesthesia, Canterbury District Health Board, New Zealand
Background
The purpose of this study was to quantify and qualify the assessment of functional capacity recorded by anaesthetists in a pre-operative anaesthetic assessment clinic, before and after introduction of the Dukes Activity Status Index (DASI) 1 questionnaire. The DASI, an objective assessment of functional capacity, identifies patients at increased risk of post-operative death or myocardial infarction within 30 days of surgery more accurately than subjective assessments of functional capacity 2 .
Methods
Following ethics (HDEC ref: 21/STH/136) and locality approval (University of Otago Christchurch Reasearch Office #21105), a 12-week retrospective review was undertaken of the paper records completed by anaesthetists during the pre-operative assessment of patients scheduled for elective orthopaedic surgery, between September and December 2020. The quantitative and qualitative documentation of functional capacity was recorded. Following this a paper version of the DASI questionnaire was introduced to the clinic for patients to complete whilst waiting for their appointment. Anaesthetists were invited to review the completed questionnaires and calculate DASI scores and metabolic equivalents (METS). The review was then repeated for a second 12-week period between January and April 2021. The quantitative and qualitative assessments of functional capacity recorded by the anaesthetists in both groups were compared.
Results
Prior to introduction of the DASI questionnaire functional capacity was recorded in 207 (74%) of the 280 patients assessed at this clinic. 206 (99.5%) assessments were subjective, 1 (0.5%) assessment was objective. Following introduction of the DASI questionnaire functional capacity was recorded in 211 (85%) of the 247 patients assessed, 105 (49.7%) assessments were objective. The median DASI score was 18.95 (interquartile range 10.7 to 26.95); the median estimated METS was 5.07 (interquartile range 4.06 to 6.05).
Conclusions
Introduction of the DASI questionnaire into an anaesthetic clinic increased both the frequency of functional capacity assessments recorded, and the proportion of objective assessments compared to subjective assessments.
References
Academic Productivity of New Zealand Anaesthetists Versus General Surgeons from 2015 to 2019: Are Our Anaesthetists Publishing?
1Middlemore Hospital, Auckland, New Zealand
Background
Despite being the largest specialist group in New Zealand, Anaesthesia has one of the lowest academic outputs among all medical specialties. The aim of this study is to quantify the research outputs of New Zealand-based Anaesthetists and trainees from 2015 to 2019 and compare this with their General Surgical counterparts.
Methods
The names of practising New Zealand Anaesthetists and General Surgeons and their respective trainees as of March 2020 were searched on PubMed for papers published between 2015 and 2019. We included works as a primary or contributing author. Published errata and international multicentre studies under which the individual was not listed as an author were excluded. Other variables collected were: gender, postgraduate experience, country of medical qualification and academic status.
Results
We identified 1025 (14.5% trainees) doctors who identified as Anaesthetists and 382 (20.2% trainees) who were General Surgeons. During the study period, Anaesthetists collectively published 750 papers, compared with 1542 for General Surgeons (median 0 (interquartile range 0-0) versus 1 (0-3), p < 0.001). Specialist Anaesthetists were less likely to have published when compared with Specialist General Surgeons (17.7% versus 56.1%, p < 0.001). The same disparity existed for Anaesthesia versus General Surgical Trainees (15.4% versus 71.4%, p < 0.001). In those who published, the academic productivity was similar across all years asides from 2018 (2018: p = 0.03). In those who were Associate or Full Professors, there was no difference in academic productivity (p = 0.50).
Conclusions
New Zealand based Anaesthetists publish significantly less frequently when compared with General Surgeons. The disparity between trainee groups may reflect differences in training scheme requirements. Given the benefits of research for professional growth and contribution to the global literature base, efforts for change should be directed towards the pre-vocational and training stages, with the potential need to mandate research participation if these patterns are sustained.
EEG Power and Frailty - A Preliminary Investigation
1Christchurch Hospital
2University of Otago, Christchurch
3New Zealand Brain Research Institute
4University of Canterbury, New Zealand Christchurch, Aotearoa - New Zealand
Background
Monitoring the processed frontal electroencephalogram (pEEG) is used increasingly during anaesthesia to avoid awareness and for drug titration. With increasing age, EEG power – and anaesthetic requirement – decreases. This study aimed to explore the relationship between measures of general level of health and EEG characteristics, particularly power in the alpha band, during anaesthesia.
Methods
This study was approved by the Northern A Health and Disability Ethics Committee (ref: 18/NTA/140) and the University of Otago Christchurch Research Office (RO18171). Subjects aged 65 years or older. Exclusion criteria included cardiac, neurological, and hip procedures, and inability to complete the assessments. Consenting participants completed four assessments: WHO Disability Assessment Schedule (WHODAS), Edmonton Frail Scale, Timed Get Up and Go (TUG), and Montreal Cognitive Assessment (MoCA). During anaesthesia a Masimo Sedline pEEG monitor was used. Raw EEG data was analysed offline. Anaesthesia management was not standardized. The primary outcome measure was mean absolute alpha power over the 20-min period commencing 15 min after induction. WHODAS was repeated at one month.
Results
Data were from 42 of the 48 participants (26F, 16M; median 72 years (range 65–88). Primary anaesthetic: propofol in 22; sevoflurane in 20.
Assessment scores: MOCA median 26, [IQR 24 to 27.75], Edmonton Frailty Score 4.0 [2 to 6], TUG 10.3 [9.4 to 13.0], change in WHODAS 0.0 [−3 to 4], absolute alpha power 0.63 [0.43 to 1.22] μV2.
No significant correlations between absolute alpha power and age (r = 0.16), TUG (r = 0.30) or MoCA (r = 0.17).
A GLM, adjusting for age and anaesthetic agent, found an association between alpha power and MoCA (p = 0.034), and between alpha power and TUG (p = 0.028).
Conclusions
Our results suggest that both lower cognitive performance (MoCA) score and decreased physical ability (TUG) are associated with decreased alpha power. These patient characteristics may be markers of decreased anaesthetic requirement and increased risk of post-operative delirium.