
Abstract

With the escalating global volume of surgery and an increasingly complex and comorbid patient population,1,2 optimisation of perioperative services is essential to reduce perioperative morbidity. In Australia and New Zealand, the Perioperative Medicine Special Interest Group (SIG) has held annual (2016–2018) strategic meetings on perioperative medicine. Knowledge gaps identified included areas of service priority, training and accreditation, and barriers to implementation.
We surveyed a population of anaesthetists and other specialists (surgeons, general medicine physicians and geriatricians) to inform the development of perioperative medicine systems in Australia and New Zealand. After institutional ethics approval (Peter MacCallum Cancer Centre HREC LNR/17/PMCC/213), a 26-item electronic survey (SurveyMonkey Inc., San Mateo, CA, USA; Supplementary Appendix 1, available as online supplementary material) was distributed via the Australian and New Zealand College of Anaesthetists (ANZCA) Clinical Trials Network to 1605 recipients.
This included 581 anaesthetist members of the ANZCA Perioperative SIG (group 1), 138 non-anaesthetist delegates attending the 2017 annual Perioperative Medicine SIG conference (group 2), and 886 Fellows of the Australian and New Zealand College of Anaesthetists (FANZCA) anaesthetists (group 3). Responses were anonymous. Results were analysed using Microsoft Excel version 15.33 (Microsoft Corp., Redmond, WA, USA, 2017). Questions with missing responses were included in the final results; the denominator of each question was the number of complete responses. The survey was conducted and reported in line with published recommendations on survey research methodology. 3
In total, 358 responses were received (response rate 22%), including 152/581 (26%) respondents from group 1, 71/138 (51%) respondents from group 2, and 135/886 (15%) respondents from group 3. Most respondents were specialists (325, 92%), predominantly based in public practice (259 working >50% public practice, 73%), and based in tertiary referral or teaching hospitals (191, 54%). Most anaesthetists (201, 76%) and non-anaesthetists (34, 58%) spent one or fewer days per week working in perioperative medicine. The current availability of perioperative services at respondents’ primary institutions is summarised in Table 1.
Perioperative services currently available at the respondent’s primary hospital.
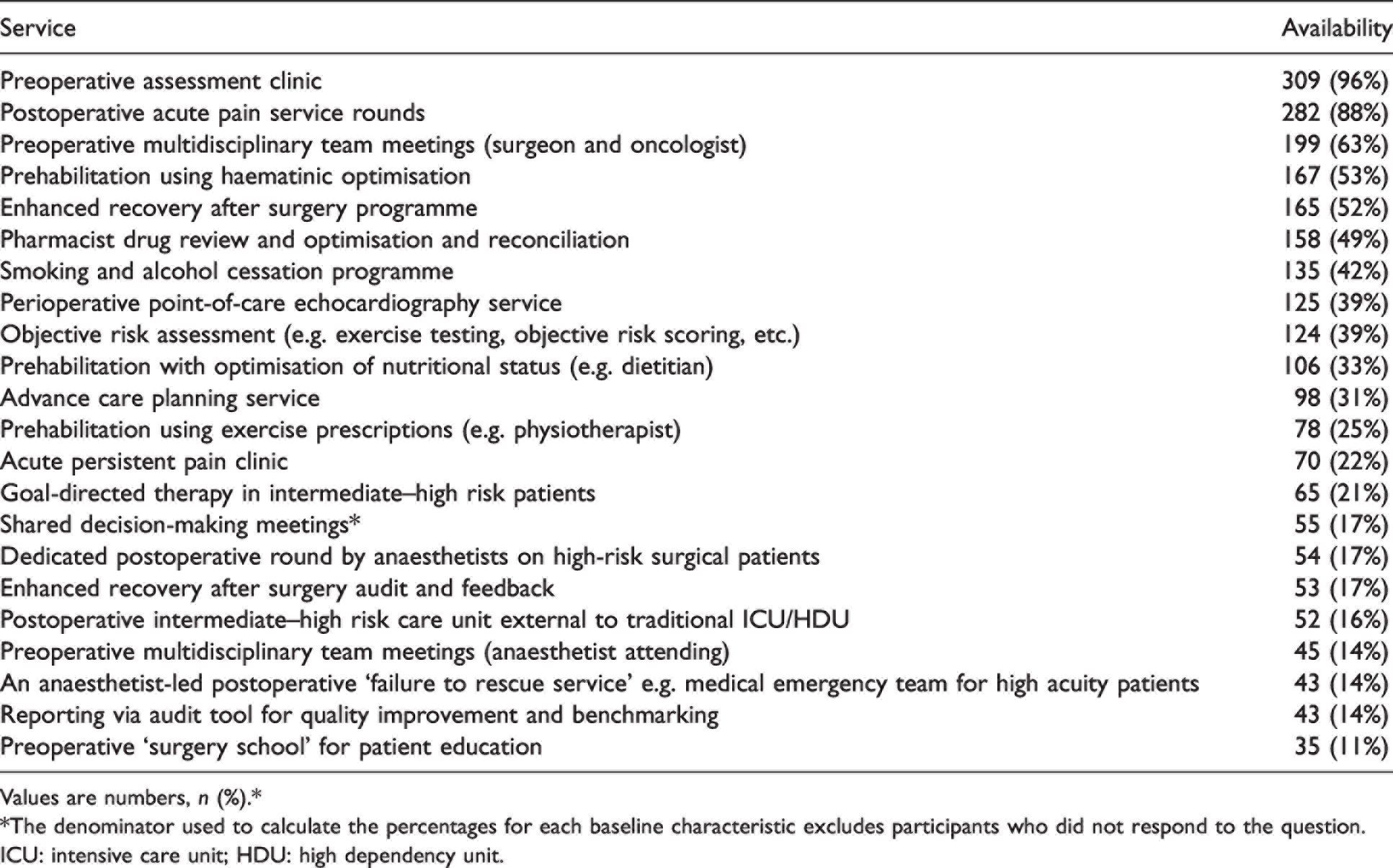
Values are numbers, n (%).*
*The denominator used to calculate the percentages for each baseline characteristic excludes participants who did not respond to the question.
ICU: intensive care unit; HDU: high dependency unit.
Future priorities of perioperative medicine identified in our survey
Clinical services
The perioperative clinical services ranked most essential included preoperative assessment clinics (81%), shared decision-making meetings (68%), and postoperative rounds on high-risk patients (57%). Regarding postoperative rounds, respondents rated frailty, fractured neck of femur, and multiple comorbidities as key referral criteria (median (interquartile range, IQR) 4 (3–5), where 1 represents ‘never refer’ to 5 ‘definitely refer’). The most commonly selected duration of review was ‘until patients are haemodynamically stable, drinking, eating and mobilising (DrEaMing)’, 4 selected by 157 (41%) respondents (Figure 1).
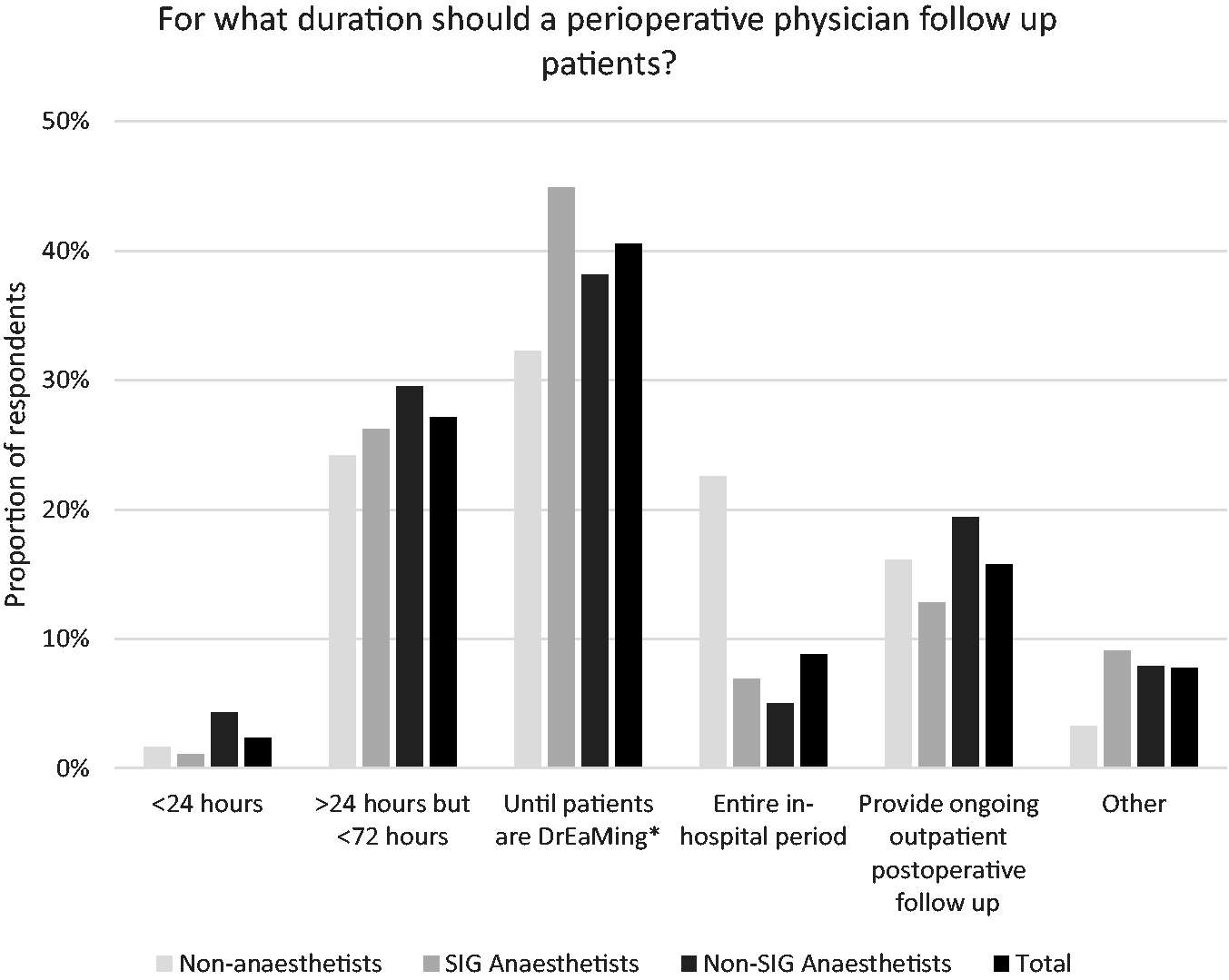
For what period of postoperative time should perioperative specialists follow up patients? (Participants may select more than one answer).
Training and curriculum development
Overall, 208 (70%) respondents thought that perioperative medicine should be developed as a subspecialty of ANZCA, with 114 (55%) of these respondents recommending development as a joint faculty with other relevant medical colleges. Most respondents thought that anaesthetists should undergo additional training to be recognised as perioperative medicine specialists, including an additional subspecialty Fellowship (94, 32%), a diploma-level degree (97, 33%), or a masters/doctorate-level postgraduate degree (34, 11%). Only 59 respondents (20%) were interested in undertaking additional training in perioperative medicine.
Perceived barriers to advancing perioperative medicine as a subspecialty
Perceived major barriers included a lack of healthcare financing (178, 61% of respondents), lack of interest from health authorities (171, 59% of respondents), and lack of reimbursement by insurance companies (165, 57% of respondents). Limited access to high dependency unit (HDU) beds for patients at intermediate risk was thought to occur ‘always’ by 18 respondents (6%), ‘frequently’ by 125 (41%), and ‘sometimes’ by 91 (30%).
Our survey identified key perceived areas of service including preoperative assessment clinics, shared decision-making meetings and postoperative rounds. The latter two services were not available at many respondents’ hospitals, although these results should be interpreted as hypothesis-generating given that we did not survey a full cross-section of institutions. A recent survey of UK anaesthetists also identified preoperative assessment, identification of comorbidity and medical optimisation as key components of perioperative care. 5
The main perceived barrier to the advancement of perioperative medicine identified (aside from the common issue of funding) was a lack of engagement. In contrast, in a recent UK survey anaesthetists identified insufficient time, personnel and training as key barriers. 5 The low number of respondents (20%) in our survey indicating interest in undergoing additional training probably represents a real barrier. The finding that respondents perceived a relatively poor access to HDU beds for intermediate-risk patients is also important given that planned critical care admission may reduce postoperative complications in this cohort. 6
There was a range of opinions regarding perceived training requirements for perioperative medicine practitioners—from the primary specialty qualification (15%), a specific perioperative medicine Fellowship (32%), or a higher degree (44%). Similarly, in a recent survey of UK anaesthetists, 26% thought that perioperative medicine should be developed as a separate subspecialty, and 23% thought that a formal perioperative medicine qualification should be required. 5
While 356 respondents gave reasonably precise results, the main limitation of the survey was the low overall response rate (22%) and potential non-responder bias. The response rate was lower than the average response rate to ANZCA surveys (∼30%), and is far lower than the generally accepted threshold for a ‘good’ response rate of 60%. 3 However, our response rate is higher than a recently published survey on the attitudes of UK anaesthetists towards perioperative medicine (response rate 4.5%). 5 Our low response rate may indicate a lack of interest in perioperative medicine from clinicians; the FANZCA response rate (15%) was lower than that of delegates attending the perioperative medicine SIG meeting (31%). There is also the potential for non-responder bias given that most survey respondents were either members or conference delegates at the ANZCA Perioperative SIG meeting. In addition, the survey was conducted prior to the coronavirus 2019 (COVID-19) pandemic, and respondents’ perceptions about healthcare priorities may have subsequently changed. Finally, the survey responses represent the opinions of survey respondents, and these opinions may also be subject to error or bias. These factors may limit the generalisability of our results. However, there was a diverse group of respondents in terms of experience, place of practice and representation from anaesthetists working in both the public and private sectors.
There has been recent international interest in formalising systems for perioperative medicine, such as the US ‘perioperative surgical home’ and the UK ‘centre for perioperative care’. This survey provides some early data to guide policy decisions, such as expanding perioperative programmes to include initiatives such as shared decision-making and postoperative rounds of high-risk patients.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to thank Karen Goulding from the ANZCA Clinical Trials Network for her assistance with survey distribution.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.