
Abstract
Summary
This retrospective study aimed to determine the incidence of and factors associated with peripheral intravenous extravasation in paediatric patients in the intraoperative setting. We conducted a retrospective study of 56,777 patients who underwent general anaesthesia and had peripheral intravenous catheter placement at Cincinnati Children’s Hospital between 1 January 2015 and 1 January 2017. Data collected included age, American Society of Anesthesiologists Physical Status Classification, catheter site, number of cannulation attempts, ultrasound use for cannulation, surgery duration, and surgery class. Primary outcome was peripheral intravenous extravasation using an extravasation assessment tool. Some 64,814 peripheral venous catheters were placed in patients undergoing general anaesthesia. Significant extravasation was documented in 40 catheters with an estimated incidence of 1 in 1620 venous catheters (0.06%). Of those 40 catheters, 47.5% (n = 19) were placed using ultrasound and 37.5% (n = 15) required more than one cannulation attempt. In multivariable analysis, peripheral intravenous catheter extravasation was associated with American Society of Anesthesiologists Physical Status Classification (3, 4, 5) versus (1, 2) (odds ratio 2.42 (95% CI 1.08 to 5.41)), inpatient versus outpatient surgeries (odds ratio 2.99 (95% CI 1.31 to 6.81)), and intravenous catheters placed with ultrasound guidance (odds ratio 8.01 (95% CI 4.12 to 15.57)). Our study identified factors associated with intraoperative peripheral intravenous extravasation, and will help develop mitigation strategies to minimise harm to patients.
Introduction
Reliable intravenous access is of paramount importance for delivery of anaesthetic agents and resuscitative medications during anaesthesia. Although use of peripheral intravenous catheters (PIV) is an everyday part of anaesthesia practice, they are not without complications. One of the most serious morbid complications of PIV is peripheral intravenous extravasation (PIVE). Extravasation is the unintended leakage of intravenous fluid or medication into the extravascular tissue surrounding the site of infusion and may or may not be associated with significant tissue injury.1,2
Although PIVE is reported in up to 6.5% of hospitalised patients,1,3,4 perioperative incidence is unclear. Rapid clinical identification of PIVE in the operating room can be difficult due to limited access to extremities and surgical draping. Unrecognised PIVE can lead to severe harm injuries such as tissue necrosis, limb deformity, and amputation, and has resulted in malpractice claims.5 –7 Despite the potential for severe and well-known harm, there is paucity of data regarding the overall incidence and risk factors associated with PIVE in the operating room. Proactive identification of risk factors associated with PIVE will enable risk mitigation.
With this background, we performed a retrospective study in paediatric patients undergoing general anaesthesia to evaluate the incidence of PIVE and factors associated with PIVE. In addition, we assessed the presence of PIVE-associated severe harm, as defined by absence of distal pulse, limb ischaemia, or injury requiring fasciotomy.
Methods
Institutional Review Board (IRB) approval was obtained from the Cincinnati Children's Hospital Medical Centre (CCHMC IRB #2017-0984), and the IRB waived the requirement for written consent for this retrospective study. Peripheral venous catheters in patients undergoing general anaesthesia or monitored anaesthesia care in the operating room during a two-year period (1 January 2015 to 1 January 2017) were assessed. This study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 8
The perioperative period for PIVE assessment was defined as anaesthesia start time to one hour after anaesthesia end time. PIVE was defined as limb swelling of 30% or more, and was assessed using a validated Peripheral Venous Infiltration and Extravasation Assessment Tool (Supplemental Figure 1) derived from the Pediatric PIV Infiltration Scale developed at Children’s Medical Center Dallas, TX, USA. 9 The PIV Assessment Tool incorporates relative size of extravasation and extravasated infusates to assess the extent of damage, consistent with recommendations for identification and management of PIVE. 10 Per institutional guidelines, trained personnel applied the measurement tool to patients with catheters found to have extravasation, and expert consultation from the vascular access team was activated for swelling greater than 30% to ensure proper measurement and determine the treatment plan for the affected limb. The standard length of venous catheters placed at our institution during the study period was as follows: 24 gauge – 19 mm, 22 gauge – 25 mm, 20 gauge – 25 mm, 18 gauge – 29.5 mm, and 16 gauge – 29.5 inches.
If PIVE was identified, the severity was assessed with the tool as: severe (PIVE swelling ≥60% infiltrated), moderate (PIVE swelling 30%–59%), and mild (PIVE swelling <30%). PIVE cases with severe or moderate extravasation were classified as clinically significant and were included in this study. Infusates administered through catheters found to have extravasation were recorded and classified into four categories: Lower Risk (Green), Intermediate Risk (Yellow), and Higher Risk (Red), or Unlisted (Supplemental Figure 1). In addition, we explored the presence of severe harm resulting from the PIVE, such as absence of distal pulse, limb ischaemia, or injury requiring fasciotomy.
The following data were obtained from electronic health records: patient age, American Society of Anesthesiologists (ASA) Physical Status Classification, catheter placement location (pre-existing or placed in operating room), catheter site, number of attempts at cannulation, surgery class (inpatient or outpatient), duration of surgery (minutes), and utilisation of ultrasound for cannulation (a surrogate for difficult intravenous access).
Statistical analysis
PIVE was assessed as a binary ‘yes’ or ‘no’ outcome. Descriptive data, median and interquartile ranges for continuous variables and frequencies, and percentages for categorical variables, were analysed and the incidence of PIVE was calculated. The chi-square test was used to test association between extravasation and categorical variables. A normality test (Kolmogorov–Smirnov) was performed for continuous variables (age and duration of surgery). The Wilcoxon rank-sum test was applied to compare the difference in distribution of continuous variables of interest between two groups. A multivariable logistic regression model was developed with variables having a P value ≤0.10 in univariable associations using stepwise variable selection. Variables with an adjusted P value of ≤0.05 were retained in the final model. Analysis was performed using SAS 9.4 (SAS Institute, Cary, NC, USA).
Results
The study flow diagram is provided in Figure 1. During the 24-month study period 64,814 PIV catheters were placed in 56,777 patients. Out of these, 40 PIV catheters were associated with a clinically significant PIVE (≥30% swelling) with an incidence of one extravasation in approximately 1600 PIV. Demographic, patient and catheter characteristics are described in Table 1. A schematic representing the distribution of insertion sites for the extravasated intravenous catheters is shown in Supplemental Figure 2.
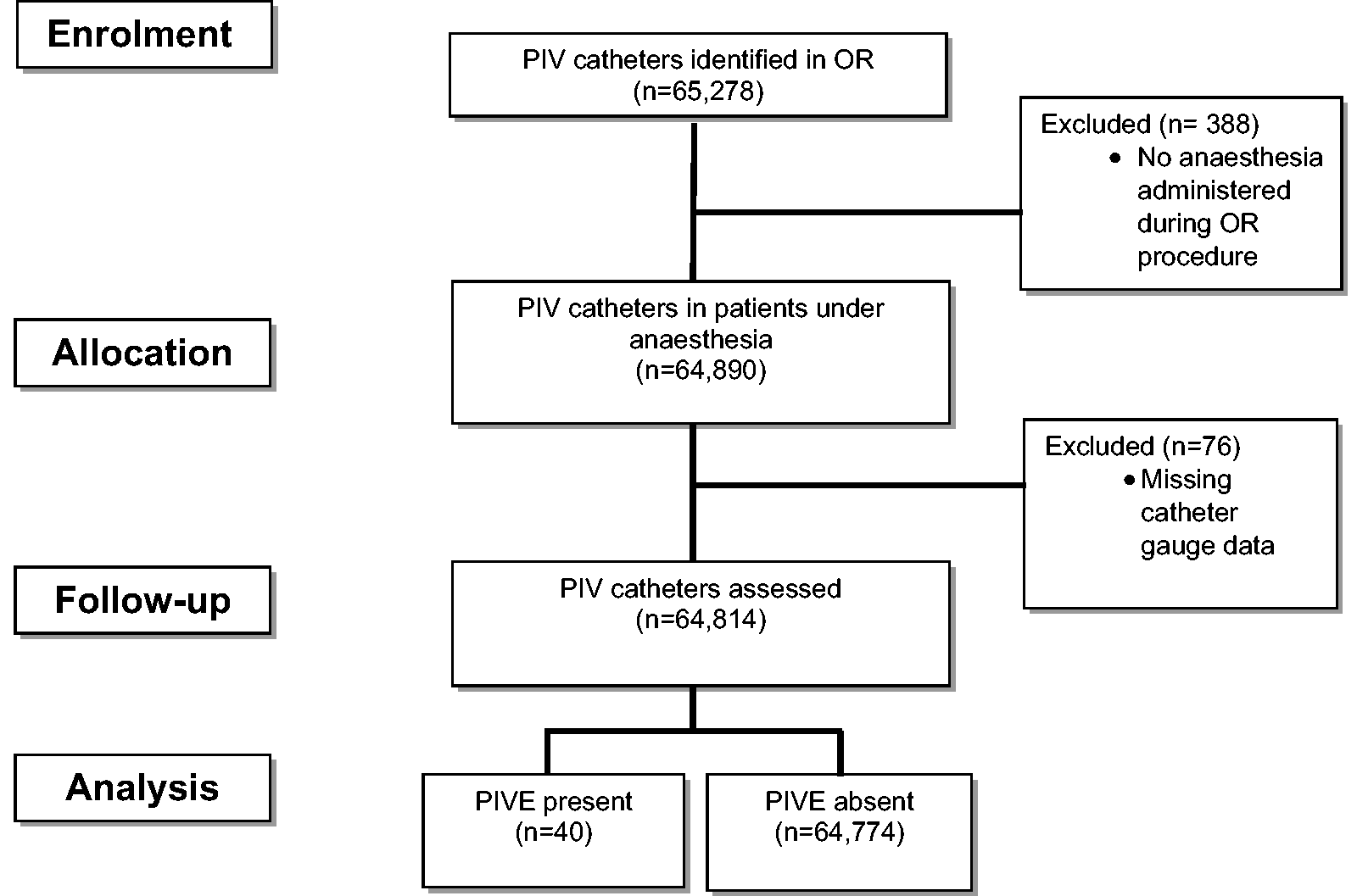
Flow diagram of patients in the study. PIV: peripheral intravenous catheter; OR: operating room; PIVE: peripheral intravenous extravasation.
Demographic characteristics of peripheral venous catheters with and without extravasation.
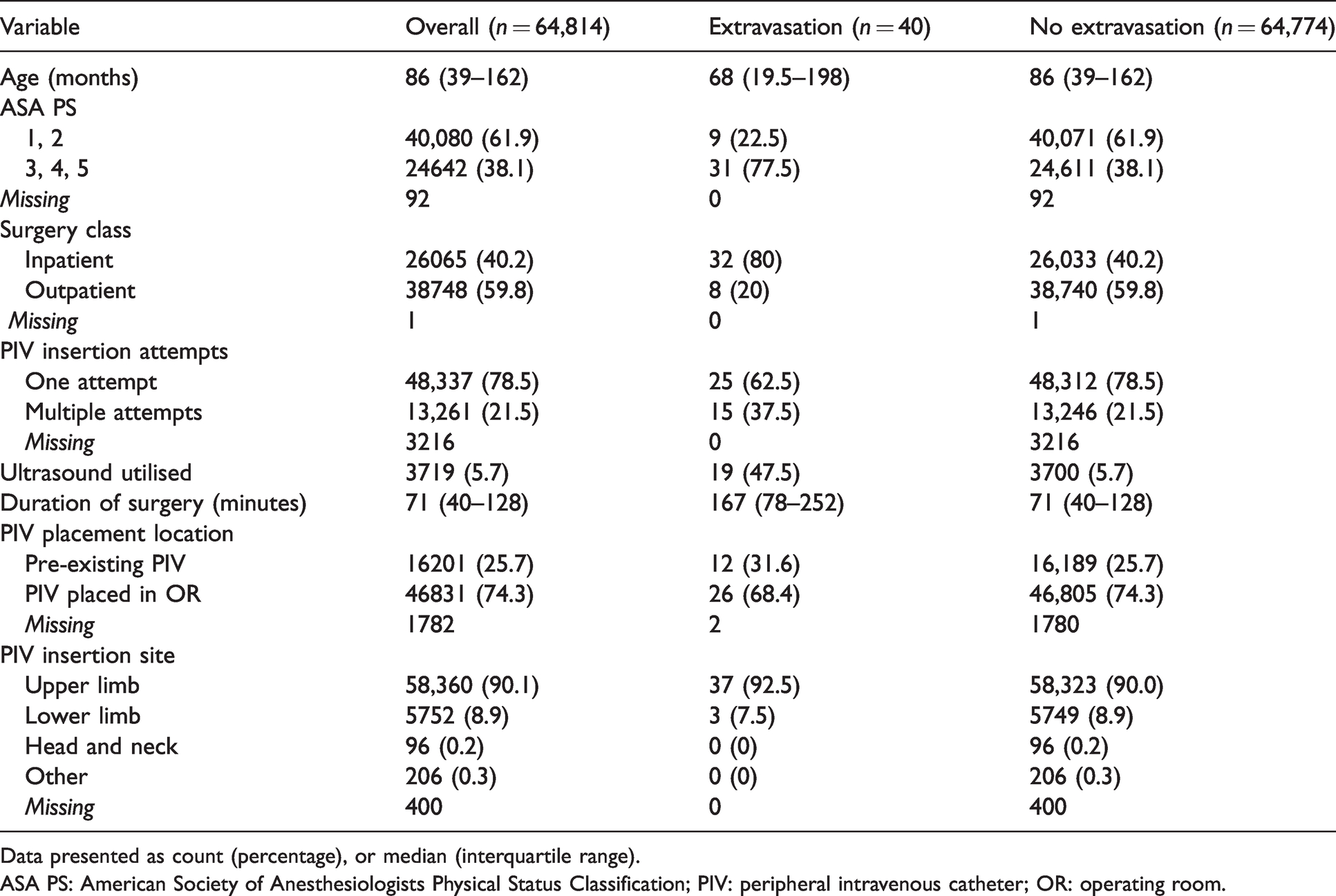
Data presented as count (percentage), or median (interquartile range).
ASA PS: American Society of Anesthesiologists Physical Status Classification; PIV: peripheral intravenous catheter; OR: operating room.
Among the 40 catheters with PIVE, 10 (25%) were severe and 30 (75%) were moderate. All catheters with PIVE were noted to have infusate extravasations: 21 (52.5%) were Lower Risk (Green), 14 (35%) were Intermediate Risk (Yellow), and five (13%) were unlisted medications. There were no catheters identified with extravasation of higher risk medications or vesicants. Approximately half of the 40 catheters with PIVE were placed with ultrasound and one-third required more than one attempt at placement. Extravasations were identified in the operating room (75%) and the remainder in the post-anaesthesia care unit. There were no occurrences of severe harm.
In the final multivariable model where only variables with a P value of ≤0.05 were retained, PIVE was associated with American Society of Anesthesiologists Physical Status Classification (3, 4, 5) versus (1, 2) (odds ratio 2.416; 95% confidence intervals (CI) 1.08 to 5.41; P = 0.0318), inpatient versus outpatient surgery (odds ratio [OR] 2.99; 95% CI 1.31 to 6.81; P = 0.0091), and difficult intravenous access measured by the utilisation of ultrasound (OR 8.01; 95% CI 4.12 to 15.57; P <0.0001) (Table 2). Results were similar when all variables with significant univariable association with PIVE were retained in the model.
Multivariable logistic regression model for peripheral intravenous extravasation.
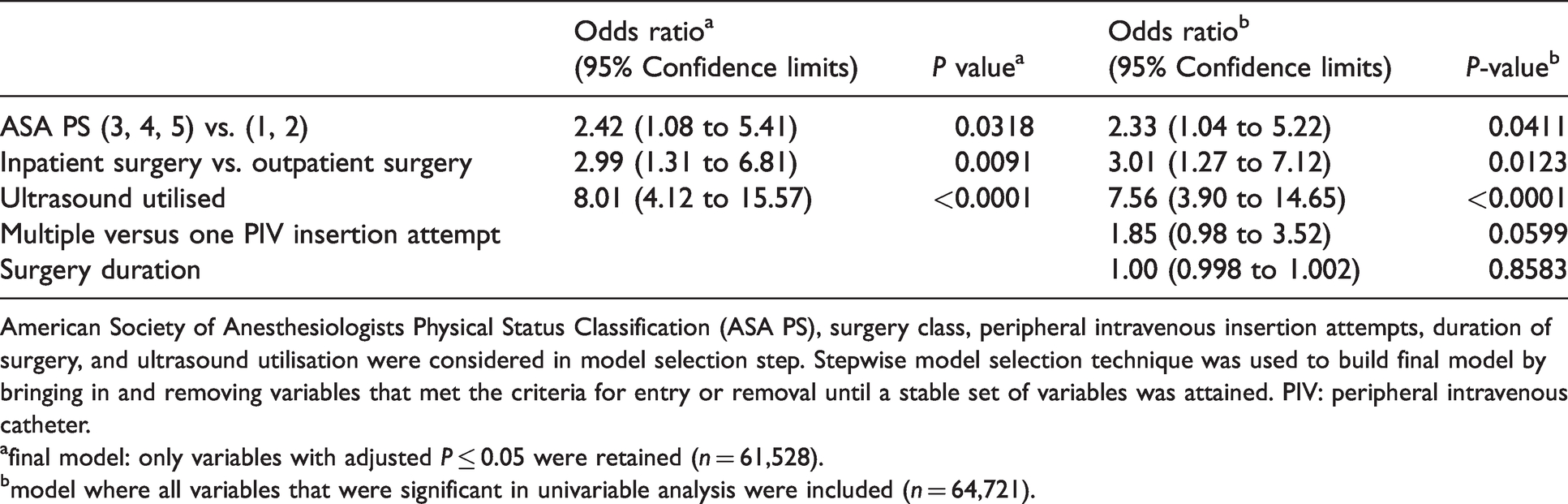
American Society of Anesthesiologists Physical Status Classification (ASA PS), surgery class, peripheral intravenous insertion attempts, duration of surgery, and ultrasound utilisation were considered in model selection step. Stepwise model selection technique was used to build final model by bringing in and removing variables that met the criteria for entry or removal until a stable set of variables was attained. PIV: peripheral intravenous catheter.
afinal model: only variables with adjusted P ≤ 0.05 were retained (n = 61,528).
bmodel where all variables that were significant in univariable analysis were included (n = 64,721).
Discussion
Although venous catheter extravasation is a relatively uncommon occurrence in the operating room, the potential for serious harm is significant. The ASA Closed Claims Project involving cases from paediatric and adult patients has demonstrated significant liability for anaesthesiologists for complications resulting from peripheral venous catheters. 11 These complications include skin slough (28%), swelling/infection (17%), nerve damage (17%), and fasciotomy scars (16%). Approximately half of these complications (55%) occurred after extravasation of drugs or fluids.
Despite these potentially serious consequences, there is no established standard of care for monitoring peripheral venous catheters in the operating room. Ball and colleagues 12 surveyed 266 anaesthesia providers and showed intravenous catheter assessment and documentation practices varied greatly among respondents. Overall, 68% of respondents felt it ‘best practice’ to assess catheters routinely during surgery; however, the intensity and frequency of assessment was varied. Multiple barriers to catheter assessment exist in the operating room. These include tucked arms, surgical draping, patient positioning, and the desire to avoid surgical interruption or a sterility breach.
There is no consistent or standard method for calculating rates of PIVE in hospitalised patients. Paquette and colleagues defined the incidence of PIVE as the number of extravasations per total patient days in hospitalised patients. 1 Our institution tracks PIVE as a quality metric using extravasations per total catheter dwell time (extravasations per line-days) and is consistent with recommendations by the Infusion Nursing Society. 10 However, due to the relatively short dwell time of a PIV during a typical anaesthetic, these definitions are less meaningful in perioperative patients. Our decision to calculate extravasations per catheter was clinically relevant to patients in the operating room and allowed for analysis of patient- and catheter-specific variables.
In our study, several clinical characteristics of patients and catheters were associated with PIVE. Markers of acutely ill patients, such as advanced ASA Physical Status and inpatient status, were found to be associated with increased extravasation in the operating room. These patients may be at greater risk for larger infusion volumes, need for caustic infusates, or underlying vasculopathy that increases likelihood of extravasations. We found that longer duration of surgery was associated with extravasation and may also be reflective of more complex surgical procedures or acutely ill patients. Previous studies have reported a higher incidence of extravasation in neonatal patients compared with children and adults; 13 however, patient age was not associated with extravasation in our study. Patients requiring multiple attempts at cannulation and the utilisation of ultrasound for catheter placement were associated with PIVE. These characteristics are surrogates for difficult intravenous access, which may be the underlying risk factor for extravasation. Difficult venous access, as defined by two or more attempts at cannulation, has previously been shown to be associated with increased extravasation in adult non–operating room patient populations. 14
Ultrasound is an increasingly important tool to assist in obtaining central, arterial, and peripheral venous access in patients undergoing anaesthesia.15,16 In a recent meta-analysis, ultrasound was shown to increase the success rate of peripheral venous cannulation in adult patients, especially in patients with known or predicted difficult venous access. 17 Because ultrasound allows the clinician to access deeper veins, a potential mechanism for extravasation in a difficult access situation is inadequate catheter length and subsequent inadvertent dislodgement.
Ensuring adequate catheter length is important, as catheter dislodgement can lead to extravasation.18,19 Based on our experience, placement by an experienced user, use of appropriate length catheters (long catheters for deep veins), targeting to place more than 50% of the catheter length in the vein, following the tip of the needle into the vein as distally as possible, and increased vigilance of venous catheters increases their safe use and potentially reduces PIVE. Although our data originated historically from a single paediatric tertiary care hospital, the variables studied are generalisable to all types of clinical care settings such as hospitals, clinics, and outpatient centres.
Our study has some limitations worth noting. First, the retrospective cohort study is prone to selection bias and information error. Although it is possible that extravasations in the operating room were inappropriately under-reported or incorrectly measured, our institution’s Departmental Safety Committee has a rigorous methodology for identifying, tracking, and reporting any PIVE which involves swelling of 30% or more of the affected limb. Furthermore, this study examined larger-volume extravasation as the primary outcome and did not identify mild (smaller volume) extravasations, as these were considered not clinically significant based on institutional guidelines. Another limitation is that we were not able to track the experience of the anaesthesia team or of the person placing the intravenous catheter. However, our PIVE perioperative incidence is comparable to the incidence of PIVE in hospitalised patients. 1
In conclusion, the overall incidence recorded in the database of clinically significant perioperative PIVE in children is 1 in 1620 PIVs. The factors associated with PIVE can be used to identify patients who may be at increased risk of extravasation.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X211062614 - Supplemental material for Factors associated with intraoperative intravenous catheter extravasation in children
Supplemental material, sj-pdf-1-aic-10.1177_0310057X211062614 for Factors associated with intraoperative intravenous catheter extravasation in children by Mecoli Marc D Conceptualization Data curation Formal analysis Investigation Methodology Writing original draft Writing review editing Ding Lili Formal analysis Investigation Writing review editing Yang Gang Formal analysis Investigation Software Writing review editing McSoley Joseph W Investigation Visualization Writing review editing Doellman Darcy A Conceptualization Investigation Writing review editing Rineair Sylvia A Conceptualization Investigation Writing review editingSubramanyam Rajeev Conceptualization Formal analysis Investigation Methodology Supervision Writing review editing in Anaesthesia and Intensive Care
Supplemental Material
sj-jpg-2-aic-10.1177_0310057X211062614 - Supplemental material for Factors associated with intraoperative intravenous catheter extravasation in children
Supplemental material, sj-jpg-2-aic-10.1177_0310057X211062614 for Factors associated with intraoperative intravenous catheter extravasation in children by Mecoli Marc D Conceptualization Data curation Formal analysis Investigation Methodology Writing original draft Writing review editing Ding Lili Formal analysis Investigation Writing review editing Yang Gang Formal analysis Investigation Software Writing review editing McSoley Joseph W Investigation Visualization Writing review editing Doellman Darcy A Conceptualization Investigation Writing review editing Rineair Sylvia A Conceptualization Investigation Writing review editing Subramanyam Rajeev Conceptualization Formal analysis Investigation Methodology Supervision Writing review editing in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Conflict of Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rajeev Subramanyam receives research funding from Masimo Foundation, Irvine, CA, USA, for a project unrelated to this publication. No conflicts of interest. Other authors do not declare any interests.
Funding Information
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: Departmental funding only.
Acknowledgements
The authors would like to thank Maria Ashton MS RPH MBA for editing the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.