
Abstract
Robot-assisted laparoscopic prostatectomy requires a pneumoperitoneum combined with steep Trendelenburg positioning, and these conditions can be associated with impairment of cerebral autoregulation. The objective of this study was to determine if choice of anaesthetic agent affects the preservation of cerebral autoregulation during robot-assisted laparoscopic prostatectomy. We randomly assigned 30 patients to maintenance of general anaesthesia with either propofol or sevoflurane. Cerebral autoregulation was tested by administration of intravenous phenylephrine to increase mean arterial pressure from approximately 80 mmHg to 100 mmHg while assessing cerebral blood flow using transcranial Doppler ultrasonography. Autoregulation was first tested in the supine position and then approximately once every hour after Trendelenburg positioning. The main outcome measure was the result of the final autoregulation test prior to completion of surgery. At that time, we found cerebral autoregulation to be significantly impaired in six of the 15 patients receiving sevoflurane and none of the 15 patients receiving propofol (P = 0.02). However, it should be noted that some patients in the propofol group had impaired autoregulation on earlier tests. In conclusion, we found that autoregulation during robot-assisted laparoscopic prostatectomy is less likely to be impaired with propofol compared to sevoflurane anaesthesia, particularly towards the end of the surgery.
Introduction
Robot-assisted laparoscopic surgery is becoming increasingly common and robot-assisted laparoscopic prostatectomy (RALP) is one of the most commonly performed procedures for the treatment of localised prostate cancer in Australia. Optimal surgical access for robot-assisted surgery involving pelvic organs typically requires placing the patient in the steep Trendelenburg position. Robot-assisted procedures may be prolonged and there is concern that the prolonged steep Trendelenburg position, combined with potential hypercapnia from carbon dioxide pneumoperitoneum, could cause cerebral morbidity. This concern is highlighted by rare case reports of severe cerebral oedema after robot-assisted pelvic surgery.1,2
Several factors could contribute to the risk of cerebral oedema during robot-assisted laparoscopic surgery. The head-down positioning may increase both cerebral venous pressure and mean arterial pressure (MAP) at the height of the brain. Venous pressure may be further increased by raised intrathoracic pressure due to head-down positioning and mechanical effects of the pneumoperitoneum. Cerebral autoregulation can be impaired under general anaesthesia, which could also contribute to the risk of cerebral oedema. Cerebral autoregulation involves arteriolar vasoconstriction in response to increased MAP, and impairment of this process could expose the cerebral circulation to increased capillary hydrostatic pressure. Impairment of cerebral autoregulation has been reported in a series of patients in the steep Trendelenburg position for RALP under sevoflurane general anaesthesia. 3 In that study, impairment of cerebral autoregulation became progressively more likely over time.
It is known that, compared to anaesthesia with volatile anaesthetic agents, cerebral autoregulation is less likely to be impaired with propofol anaesthesia. In normal patients autoregulation is usually not impaired by sevoflurane; 4 however, under certain conditions, such as hypercapnia, autoregulation is better preserved by propofol than sevoflurane.5,6
The aim of this study was to compare cerebral autoregulation during RALP in patients anaesthetised with either propofol or sevoflurane. We hypothesised that autoregulation would be more likely to be impaired with longer duration of surgery and that propofol anaesthesia would be associated with a lower risk of impaired autoregulation compared to sevoflurane. In this study we randomly assigned patients to either propofol or sevoflurane anaesthesia and analysed autoregulation at multiple times, before and during Trendelenburg positioning, with the primary analysis focused on the last autoregulation test in each patient.
Methods
Patients scheduled for RALP were eligible for this study. Exclusion criteria included known intracranial pathology, known cerebrovascular disease, and morbid obesity (body mass index >40 kg/m2). Patients were randomly allocated to either propofol or sevoflurane as the primary anaesthetic agent. Permutated block randomisation was used and group allocation was concealed in consecutively numbered opaque envelopes opened by the treating anaesthetist immediately prior to induction of general anaesthesia. It was considered impractical to attempt to blind the treating anaesthetist or the investigators during intraoperative autoregulation testing, although investigators were not aware of patient allocation during subsequent offline analysis of autoregulation tests. The study protocol was approved by the Human Research Ethics Committee of the Sydney local health district and the trial was prospectively registered on the Australian New Zealand Clinical Trials Registry (ACTRN12619000548134). The trial was conducted at two sites: Royal Prince Alfred Hospital and Chris O’Brien Lifehouse in Sydney, Australia.
In the sevoflurane group, anaesthesia was induced with a single dose of propofol and maintained with inhaled sevoflurane. In the propofol group, anaesthesia was induced and maintained with propofol administered by a commercial microprocessor-controlled pump (Injectomat TIVA Agilia, Fresenius Kabi, Germany) running the Schnider pharmacokinetic model. All patients received an effect-site targeted infusion of remifentanil administered by the same commercial pump running the Minto pharmacokinetic model. In both groups, the anaesthetic dose was adjusted to aim for a bispectral index (BIS) of 45 ± 5. Blood pressure was supported with an intravenous infusion of phenylephrine, adjusted to manipulate MAP for the purpose of autoregulation testing (details below). Tracheal intubation was performed after administration of a non-depolarising muscle relaxant. Ventilation was adjusted to aim for an arterial partial pressure of carbon dioxide (CO2) (PaCO2) of 40 ± 4 mmHg at the times of autoregulation testing. The fractional inspired oxygen was standardised at 0.30–0.35 in an air–oxygen mix.
Arterial pressure was monitored via a radial artery catheter with the transducer referenced to the height of the external auditory meatus. Other standard monitoring included end-tidal CO2 and end-tidal sevoflurane concentration (in the sevoflurane group). Transcranial Doppler (TCD) assessment of cerebral artery blood velocity was used as an index of changes in cerebral blood flow (CBF) (Multidop-T; DWL, Sipplingen, Germany). A 2 MHz monitoring probe was situated over a temporal window and positioned to record middle cerebral artery blood velocity (Vmca). The probe was held in constant position by attachment to a head frame. An analog voltage signal from the TCD monitor was used to record the peak Vmca waveform. The Vmca signal and the analog signal from the arterial pressure transducer were converted to digital data (AD Instruments, Sydney, Australia) and recorded simultaneously on the hard drive of a personal computer.
Autoregulation testing was performed by recording Vmca while MAP was pharmacologically manipulated from around 80 mmHg to around 100mmHg over the period of a few minutes. First, the remifentanil target concentration was increased to achieve a MAP below 80 mmHg, and the remifentanil target was then left unchanged during the autoregulation test. In addition, a dose of intravenous labetalol was administered to five subjects (three in the propofol group and two in the sevoflurane group) to help achieve MAP around 80 mmHg at the height of the head. Phenylephrine was infused to aim for a steady MAP around 80 mmHg for at least two respiratory cycles, then the dose was increased, aiming to increase MAP over several minutes to achieve a steady MAP around 100 mmHg, again for at least two respiratory cycles.
The first autoregulation test was performed in the supine position, after induction of anaesthesia and prior to moving the patient to the head-down position. Due to time pressure in the operating theatre combined with difficulties locating the Vmca signal, we did not perform this initial autoregulation test in the supine position in four subjects (two in each group). Autoregulation testing was then repeated at approximately hourly intervals, commencing one hour after Trendelenburg positioning. Autoregulation testing was conducted at times of minimal surgical stimulation when haemodynamic parameters were judged stable.
For each autoregulation test, the cerebral autoregulation index (ARI) was calculated as previously described. 7 ARI = [(R2–R1)/R1]/[(MAP2–MAP1)/MAP1], where R = MAP/Vmca. R is an index of cerebral vascular resistance (ignoring the contribution of intracranial pressure to cerebral perfusion pressure). Subscripts 1 and 2 refer to measurements at the lower and higher MAP, respectively. An ARI of 1 indicates no increase in Vmca between MAP of 80 mmHg and 100 mmHg. An ARI of 0 indicates absent cerebral autoregulation across the 80 mmHg to 100 mmHg range of MAP, with Vmca increasing proportionally with MAP. As in previous studies, we defined significantly impaired cerebral autoregulation as an ARI of 0.4 or less. 5 Note that CBF can change independent of cerebral perfusion pressure (e.g. related to fluctuation in PaCO2 or changes in cerebral activity). Also, the ARI is based on proportional change in MAP which is not a true measure of change in cerebral perfusion pressure. For these reasons, the ARI is sometimes found to be greater than 1.0 when autoregulation is intact and less than 0.0 when autoregulation is markedly impaired.
Because we expected autoregulation to be more likely to be impaired with longer times in steep Trendelenburg, the pre-specified primary outcome was based on the last autoregulation test in each patient. We aimed to recruit 30 patients, 15 in each group based on a power calculation for detecting a difference in ARI of 0.3. However, prior to commencing recruitment and prior to registering the trial, we changed the primary outcome to be based on the number of patients in each group with significantly impaired autoregulation (ARI ≤0.4). Due to an oversight, we did not repeat the power calculation after changing the primary endpoint. Fisher’s exact test was used to compare proportions.
Results
We randomly assigned 30 patients, 15 to each group. Of 34 patients who were approached, two did not consent to participate and two others were not included because an adequate temporal window for TCD monitoring could not be found prior to induction of anaesthesia. There were no anaesthetic-related adverse outcomes identified.
Baseline and intraoperative characteristics are presented in Table 1. The ages of the two groups were similar, as was the number taking antihypertensive medications. There was no difference in the degree of Trendelenburg between groups and, at the time of the final autoregulation test, the groups had a similar range of PaCO2 and BIS values. The median remifentanil effect-site concentration in the propofol group was more than double that of the sevoflurane group (P<0.01, Mann–Whitney U-test).
Baseline and intraoperative characteristics of the patients.
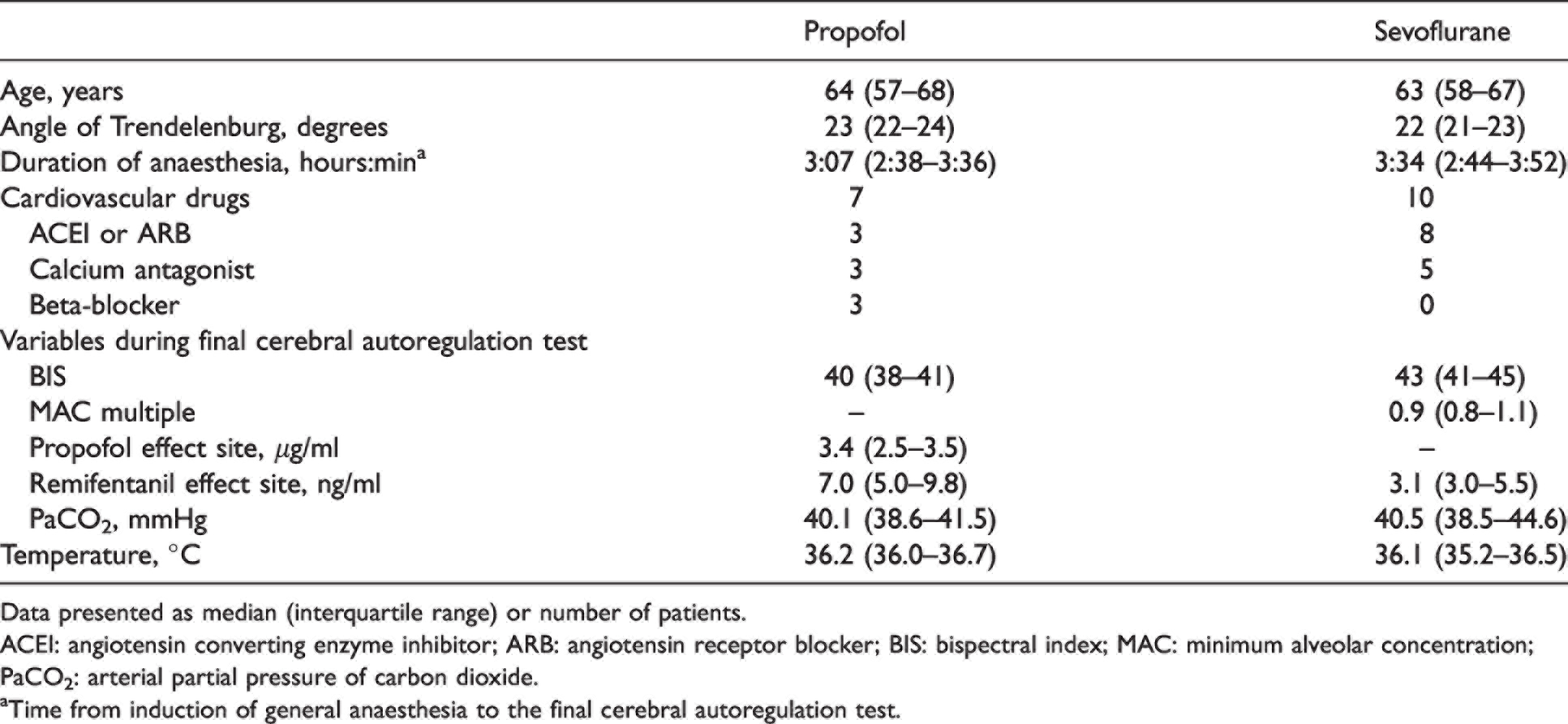
Data presented as median (interquartile range) or number of patients.
ACEI: angiotensin converting enzyme inhibitor; ARB: angiotensin receptor blocker; BIS: bispectral index; MAC: minimum alveolar concentration; PaCO2: arterial partial pressure of carbon dioxide.
aTime from induction of general anaesthesia to the final cerebral autoregulation test.
Autoregulation in the supine position, soon after induction of anaesthesia, was found to be significantly impaired in seven patients, three in the propofol group and four in the sevoflurane group. During Trendelenburg positioning, the ARI did not demonstrate a consistent change over time across the patient cohort (Figure 1 and Table 2). In some patients, autoregulation was initially within the intact range then became significantly impaired. In other patients, particularly in the propofol group, autoregulation was impaired on one or more tests then subsequently improved. Across all the autoregulation tests in the Trendelenburg position, the ARI indicated impaired autoregulation in 12 of 39 tests in the sevoflurane group and six of 39 tests in the propofol group (P>0.05). Comparing the final test in each patient, six patients in the sevoflurane group had an ARI of 0.4 or less compared to none in the propofol group (P = 0.02).
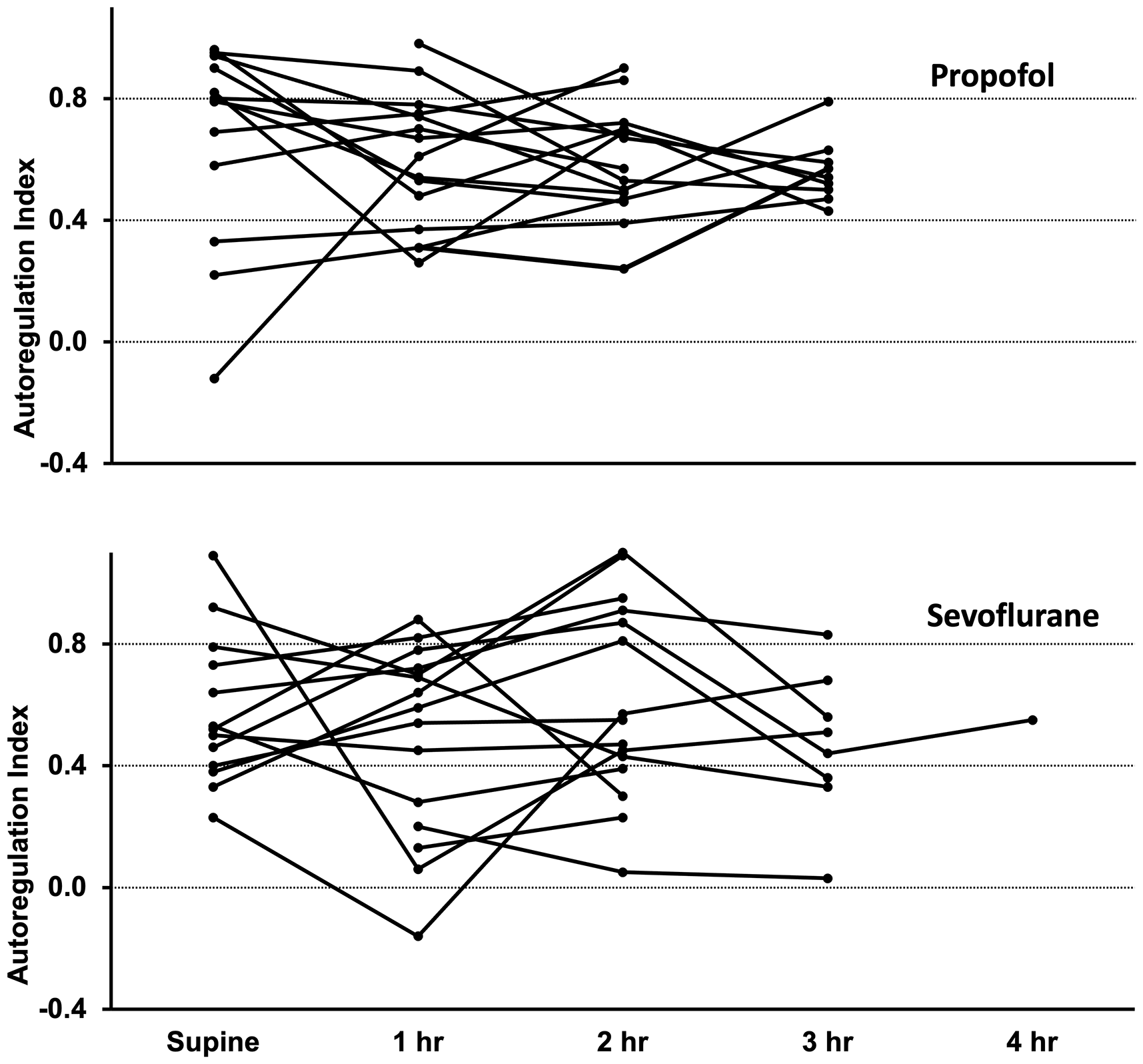
Individual cerebral autoregulation results supine (prior to Trendelenburg positioning) and one to four hours after Trendelenburg positioning, with lines connecting results from individual patients. Autoregulation index of 0.4 or less indicates significantly impaired cerebral autoregulation.
Individual cerebral autoregulation index results.
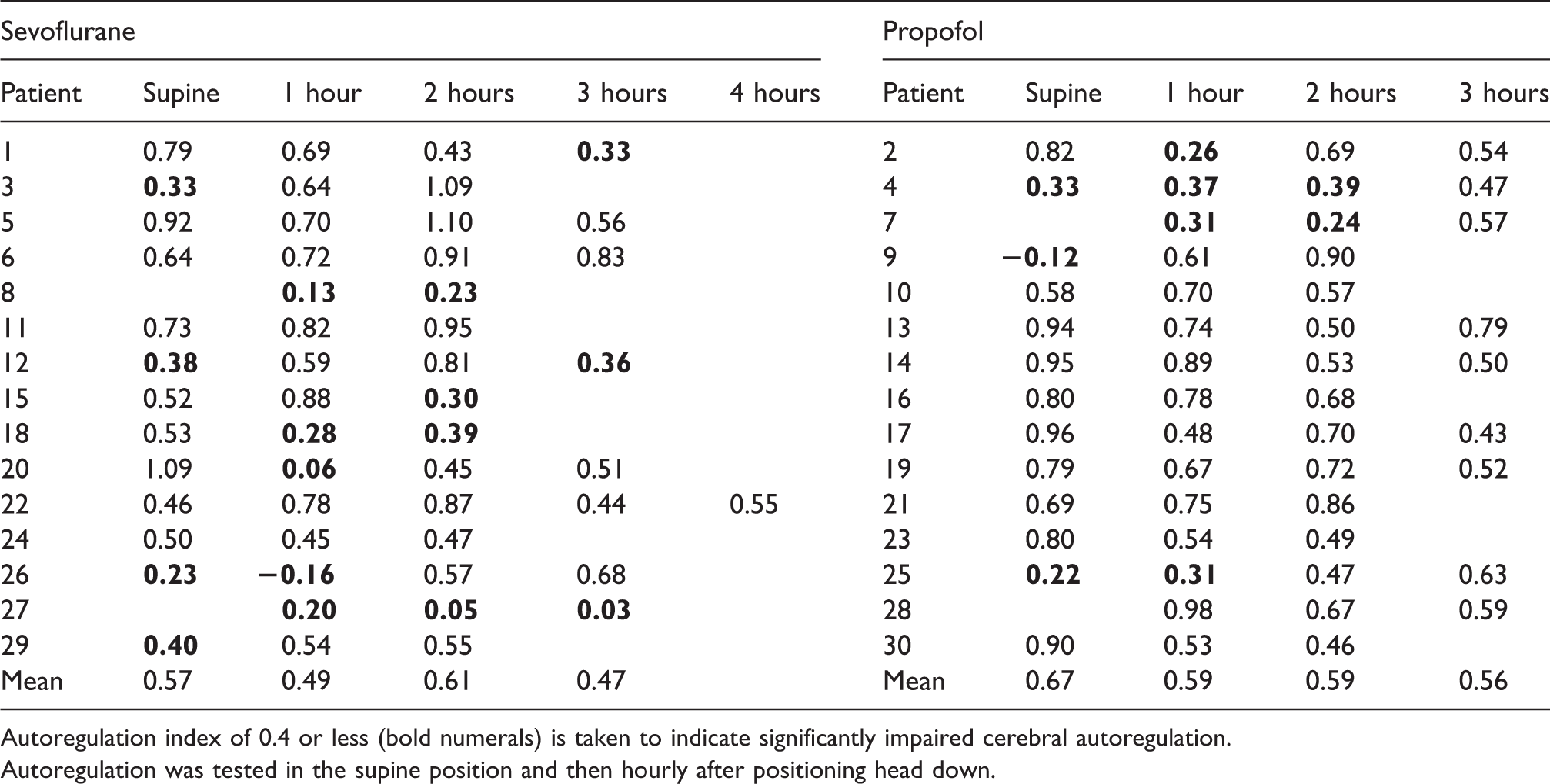
Autoregulation index of 0.4 or less (bold numerals) is taken to indicate significantly impaired cerebral autoregulation.
Autoregulation was tested in the supine position and then hourly after positioning head down.
Discussion
Our results provide some support for the hypothesis that autoregulation is better preserved during robot-assisted laparoscopic surgery in the Trendelenburg position if anaesthesia is maintained with propofol rather than sevoflurane. Towards the end of Trendelenburg positioning, no patient in the propofol group had an ARI indicating significantly impaired autoregulation, whereas the ARI was in the significantly impaired range in 40% of the sevoflurane group. We chose the primary outcome of impaired autoregulation, on the last autoregulation test, based on the only other study of cerebral autoregulation during RALP, which reported progressive impairment of cerebral autoregulation with increased duration of Trendelenburg positioning. 3 However, we have not confirmed a progressive increase in the likelihood of impaired autoregulation and the opposite appeared to occur in our propofol group in which all patients who had impaired autoregulation subsequently improved. Our a priori decision to analyse the final test in each patient as the primary endpoint is problematic given that we did not find this test to be the most likely to be impaired. Comparing all of our autoregulation tests in the Trendelenburg position, twice the number of tests indicated impaired autoregulation with sevoflurane but this was not statistically significant.
When comparing our results with previous studies of cerebral pathophysiology during RALP surgery, it must be noted that the degree of Trendelenburg in our patients was significantly less than has often been reported. In the previous study of impaired cerebral autoregulation with sevoflurane anaesthesia, patients were positioned 40°–45° head down. 3 The same degree of Trendelenburg was also reported in a study that did not test cerebral autoregulation but found evidence for increasing intracranial pressure during RALP. 8 Our experience of current practice is to limit head-down tilt to 20°–30°. The median degree of Trendelenburg in our patients was 22° and our patients also spent less time in the Trendelenburg position compared to those previous studies. We speculate that the potential cerebral effects of positioning for RALP are mitigated as surgeons are now able to perform the operation with a shorter duration of less steep Trendelenburg positioning.
There is a plethora of methods for testing cerebral autoregulation. 9 The autoregulatory response is thought to comprise two separate mechanisms, with a rapid dynamic response and a slower static response. We used a method of testing static autoregulation whereby MAP changed over a period of several minutes and each Vmca–MAP data point was an average of multiple cardiac cycles over at least two complete respiratory cycles, thereby eliminating variability from short-term oscillations such as those due to intermittent positive pressure ventilation. In the previous study during RALP under sevoflurane anaesthesia, autoregulation was tested using a method of analysing correlation between Vmca and spontaneous fluctuations in MAP. 3 Methods of assessing autoregulation based on spontaneous fluctuations in MAP have the advantage of not requiring pharmacological interventions. However, spontaneous fluctuations in MAP are of a much smaller amplitude than the range of MAP used in our study, and the correlation is influenced by the dynamic rate of autoregulation. A possible advantage of the method we used is that the range of MAP over which autoregulation is tested could be considered a more rigorous test, with the range of arterial pressure arguably more representative of the full range commonly seen in clinical practice.
We found autoregulation prior to Trendelenburg positioning to be significantly impaired in several patients in the propofol group, despite normocapnia. Previous studies using the same method of autoregulation testing have reported no impairment of cerebral autoregulation in neurologically normal patients under propofol anaesthesia with normocapnia.5,7 This discrepancy between our current results and previous studies could be due to our older group of patients, many of whom would have been excluded from those previous studies as they were on medications for hypertension and other cardiovascular conditions. A recent study tested autoregulation in awake subjects with an age range comparable to our patients and with comorbidities comparable to our patients. 10 In that study, results were pooled and analysed using linear mixed modelling, in contrast to the approach in our study of characterising the autoregulation response in individual subjects. Nevertheless, it is apparent from their figures that autoregulation was significantly impaired in a proportion of awake subjects, particularly in subjects identified as having mild cognitive impairment. It is possible that some of the patients in our study who were found to have impaired autoregulation during general anaesthesia would have shown similarly impaired autoregulation if tested awake.
Autoregulation in some of our patients appeared to be surprisingly labile. For example, some patients had a high ARI on first testing, indicating intact autoregulation, then an ARI significantly below 0.4 one hour after Trendelenburg positioning, indicating impaired autoregulation, then subsequent tests after a longer time in the Trendelenburg position indicated a return to intact autoregulation. We are not aware of previous studies in which this form of autoregulation testing has been repeated several times during surgery, therefore we cannot comment on whether marked changes in cerebral autoregulation might be common in older patients undergoing major surgery or whether head-down positioning contributed to the instability of the autoregulatory response in our patients.
The tendency for sevoflurane to impair cerebral autoregulation, compared to propofol, is consistent with the known direct cerebral vasodilatory effect of sevoflurane.6,11 Cerebral oxygenation has been compared during propofol versus sevoflurane anaesthesia during RALP with 30° of Trendelenburg. 12 In that study, the vasodilatory effect of sevoflurane was associated with a higher jugular venous oxygen content compared to propofol. Interestingly, simultaneous near-infrared spectroscopy monitoring failed to detect this difference in cerebral oxygenation.
We dichotomised the results of autoregulation testing into either intact or significantly impaired, based on a threshold ARI of 0.4 or less. The clinical significance of impaired autoregulation under general anaesthesia for elective surgery is unknown. Therefore, the choice of a particular ARI threshold for dichotomising results is necessarily arbitrary, which is a potential weakness of our analysis. Another potential limitation of this study was the possibility of a residual effect of the propofol induction dose in the sevoflurane group at the time of the first autoregulation test. The median time between induction and the first autoregulation test in the sevoflurane group was 29 minutes, with a range of 21 to 122 minutes. Autoregulation testing in the Trendelenburg position did not commence until at least one hour after the initial testing, by which time we expect there would have been no residual effect of the propofol induction dose.
The patients randomly assigned to propofol in this study received a significantly higher remifentanil dose when aiming for a MAP of 80 mmHg. This could be because MAP tends to be higher with propofol anaesthesia compared to sevoflurane anaesthesia. Studies comparing sevoflurane with propofol have reported a higher MAP with propofol when both groups received similar doses of opioids.13,14 Comparable to our results, in a study involving cardiac surgical patients in which the dose of remifentanil was adjusted to haemodynamic variables, patients randomly assigned to propofol also received a remifentanil dose approximately twice that of patients randomly assigned to sevoflurane. 15
Autoregulation testing in our study could potentially have been confounded by the drugs used to manipulate MAP. However, cerebral autoregulation is not thought to be impaired by remifentanil 16 or labetalol 17 and, importantly for the validity of Vmca as an index of change in CBF, phenylephrine has a minimal effect on the diameter of the middle cerebral artery and is not thought to alter CBF directly.18,19
CO2 pneumoperitoneum, combined with potential effects of Trendelenburg positioning on ventilation, predisposes to hypercapnia during robot-assisted pelvic surgery. Because CO2 is a potent cerebral vasodilator, the treating anaesthetists in this study were asked to attempt to achieve normocapnia to avoid a confounding effect on autoregulation. It has previously been shown that autoregulation is more likely to be impaired by hypercapnia during sevoflurane anaesthesia compared to propofol anaesthesia. 5 However, that study was in healthy, younger patients in the supine position and no patient had impaired autoregulation when PaCO2 was less than 50 mmHg. In our patients, PaCO2 was always less than 50 mmHg. In routine clinical practice, more significant hypercapnia during RALP might be common, potentially causing cerebral autoregulation to be impaired by a combination of hypercapnia and a volatile anaesthetic agent. This could represent a potential benefit of propofol anaesthesia for RALP.
In conclusion, this study has confirmed that impaired cerebral autoregulation can occur in some patients during RALP with steep Trendelenburg positioning and CO2 pneumoperitoneum. We found evidence that autoregulation is less likely to be impaired with propofol compared to sevoflurane anaesthesia, particularly towards the end of the surgery.
Footnotes
Data sharing statement
Individual patient data will be made available on reasonable request.
Author Contribution(s)
Acknowledgements
The author(s) would like to acknowledge the contributions of Dr H Braithwaite and Dr H Drinkwater who assisted with patient recruitment and data collection.
Declaration of conflicting interests
John A Loadsman is the Chief Editor of Anaesthesia and Intensive Care. The authors have no other conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.